
Exploring the Impact of Mining on Community Health and Health Service Delivery: Perceptions of Key Informants Involved in Gold Mining Communities in Burkina Faso
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Sites
2.2. Sampling and Recruitment of Study Participants
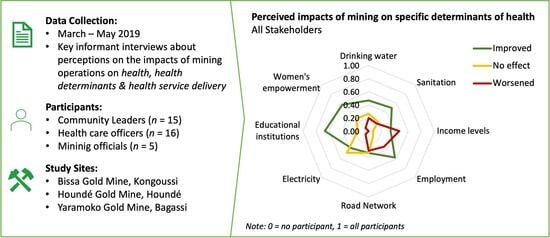
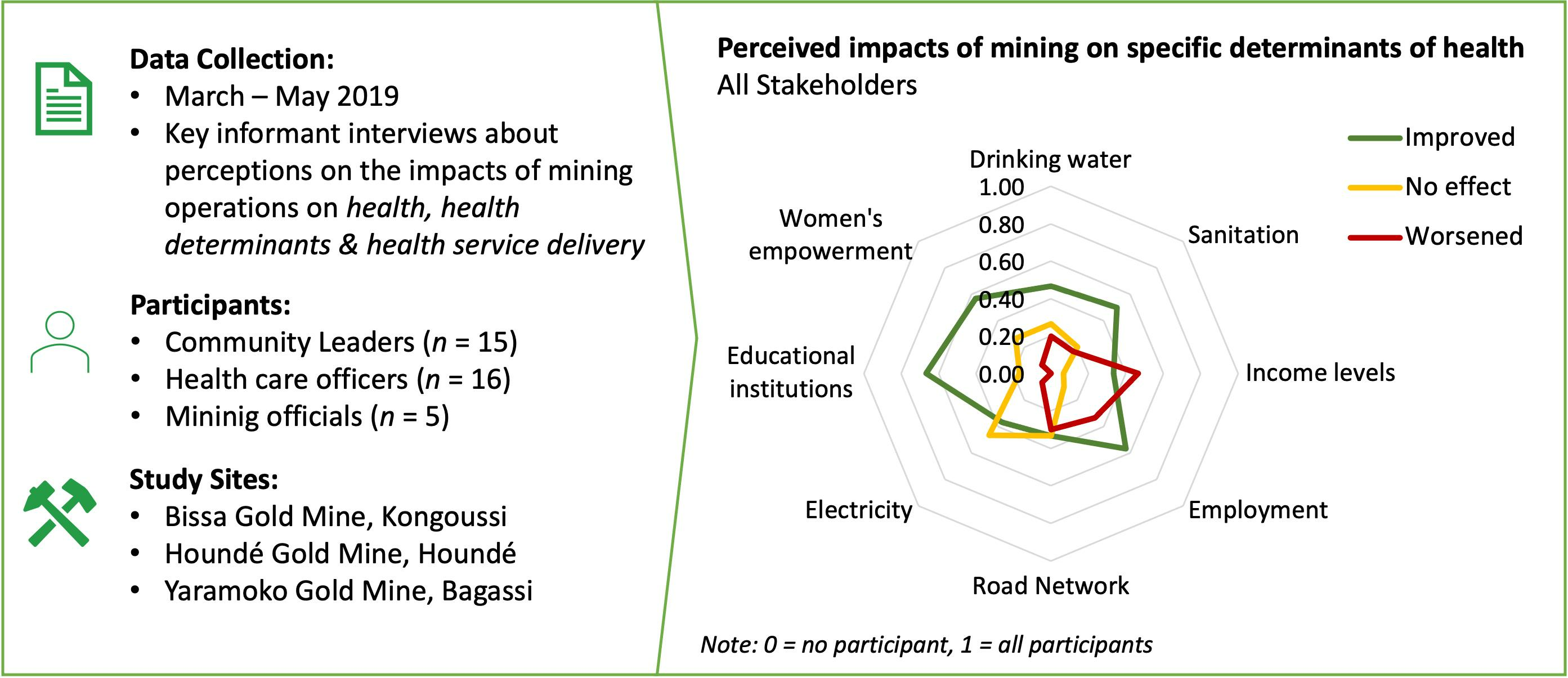
2.3. Data Collection
Quality Assurance
2.4. Data Management and Analysis
2.5. Ethical Considerations
3. Results
3.1. Study Population
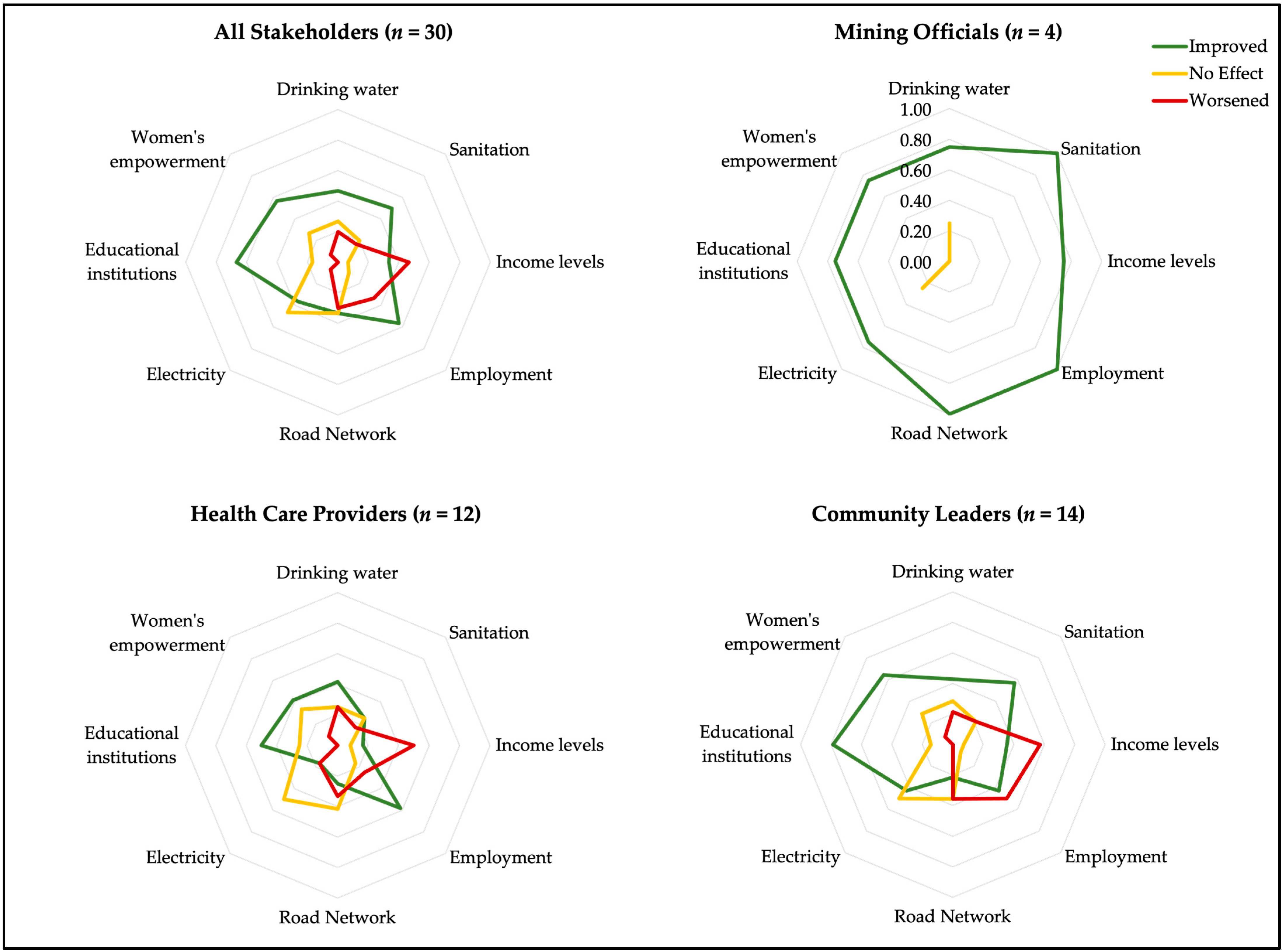
3.2. Perceived Impacts of Mining on Population Health and Health Determinants
3.2.1. Perceived Impacts of Mining on Education, Employment, Women’s Empowerment, and Income Levels
“It’s among our priorities, the women, the youth; so, health is among our priorities in terms of community investments”.(M1_mining official)
If you can’t make something with your hands, that doesn’t work. Before, we sold, and it was bought. But since these two years nothing is bought. They closed the artisanal site that existed and the people no longer have money to buy what they want. So, this is like a disease on us now. When you can’t get money for what you need, that’s a disease. So now it’s not okay.(M3_community leader)
3.2.2. Perceived Impact of Mining on Environmental Determinants of Health
“There are the tailings of the gold washing with the cyanide, and we are afraid because we do not know if there is infiltration of the subsurface. Will we be able to have clean water to drink in the future in this village. The odors that we smell in the open air, in the long run, what are the diseases that we could suffer from? That means we will die like chickens”.(M2_community leader)
3.2.3. Perceived Impact of Mining on Accidents and Associated Factors
“The main danger is not the mine itself, but the population! Advise people to drink a little less, to lead a less dangerous life. What we notice most often are accidents that are not the result of the mining company! But of individuals who abuse the alcohol”.(M1_healthcare provider)
3.3. Perceived Benefits and Challenges for Health Service Delivery Due to Mining
4. Discussion
4.1. Role of Women in Mining Settings
4.2. Positive and Negative Impacts on Determinants of Health
4.3. Impacts of Mining on Healthcare Delivery
4.4. Untapped Potential of Health Impact Assessment
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Study Site Descriptions
Appendix B. Overview of SARA Indicators

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tracer Indicators, Items and Services for SARA | Perceived Positive Impacts Cited during KIIs | Perceived Negative Impacts Cited during KIIs |
|---|---|---|
| Service availability | ||
| 1. Health infrastructure |
| |
| 2. Health workforce |
|
|
| 3. Service utilization |
|
|
| General service readiness | ||
| 1. Basic amenities |
|
|
| 2. Basic equipment |
| |
| 3. Precautions for infection prevention | ||
| 4. Diagnostic capacity | ||
| 5. Essential medicines |
|
|
| Service-specific readiness | ||
| 1. Care related to maternal, child and adolescent health |
|
|
| 2. Malaria diagnosis or treatment |
| |
| 3. Tuberculosis services 4. All healthcare related to HIV/AIDS 5. Diagnosis or treatment of sexually transmitted infections (STIs) |
|
|
| 6. Noncommunicable diseases diagnosis or management: diabetes, cardiovascular disease, chronic respiratory disease, and cervical cancer screening 7. Basic and comprehensive surgical care 8. Blood transfusion 9. Laboratory capacity |
|
|
References
- Cole, M.J.; Broadhurst, J.L. Measuring the Sustainable Development Goals (SDGs) in Mining Host Communities: A South African Case Study. Extr. Ind. Soc. 2021, 8, 233–243. [Google Scholar] [CrossRef]
- Fraser, J. Creating Shared Value as a Business Strategy for Mining to Advance the United Nations Sustainable Development Goals. Extr. Ind. Soc. 2019, 6, 788–791. [Google Scholar] [CrossRef]
- Monteiro, N.B.R.; da Silva, E.A.; Moita Neto, J.M. Sustainable Development Goals in Mining. J. Clean. Prod. 2019, 228, 509–520. [Google Scholar] [CrossRef]
- UN General Assembly Transforming Our World: The 2030 Agenda For Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 4 April 2021).
- Winkler, M.S.; Adongo, P.B.; Binka, F.; Brugger, F.; Diagbouga, S.; Macete, E.; Munguambe, K.; Okumu, F. Health Impact Assessment for Promoting Sustainable Development: The HIA4SD Project. Impact Assess. Proj. Apprais. 2020, 38, 225–232. [Google Scholar] [CrossRef]
- Carney, J.G.; Gushulak, B.D. A Review of Research on Health Outcomes for Workers, Home and Host Communities of Population Mobility Associated with Extractive Industries. J. Immigr. Minor. Health 2016, 18, 673–686. [Google Scholar] [CrossRef]
- Winkler, M.; Krieger, G.; Divall, M.; Wielga, M.; Singer, B.; Tanner, M.; Utzinger, J. Untapped Potential of Health Impact Assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Dietler, D.; Lewinski, R.; Azevedo, S.; Engebretsen, R.; Brugger, F.; Utzinger, J.; Winkler, M.S. Inclusion of Health in Impact Assessment: A Review of Current Practice in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2020, 17, 4155. [Google Scholar] [CrossRef]
- Engebretsen, R.E.H.; Brugger, F. Divergent Corporates: Explaining Mining Companies Divergent Performance in Health Impact Assessments. Resour. Policy 2021, 74, 102355. [Google Scholar] [CrossRef]
- Hermanus, M.A. Occupational Health and Safety in Mining—Status, New Developments, and Concerns. J. South. Afr. Inst. Min. Metall. 2007, 107, 531–538. [Google Scholar]
- Knoblauch, A.M.; Farnham, A.; Zabré, H.R.; Owuor, M.; Archer, C.; Nduna, K.; Chisanga, M.; Zulu, L.; Musunka, G.; Utzinger, J.; et al. Community Health Impacts of the Trident Copper Mine Project in Northwestern Zambia: Results from Repeated Cross-Sectional Surveys. Int. J. Environ. Res. Public Health 2020, 17, 3633. [Google Scholar] [CrossRef]
- Entwistle, J.A.; Hursthouse, A.S.; Marinho Reis, P.A.; Stewart, A.G. Metalliferous Mine Dust: Human Health Impacts and the Potential Determinants of Disease in Mining Communities. Curr. Pollut. Rep. 2019, 5, 67–83. [Google Scholar] [CrossRef]
- Leuenberger, A.; Winkler, M.S.; Cambaco, O.; Cossa, H.; Kihwele, F.; Lyatuu, I.; Zabré, H.R.; Farnham, A.; Macete, E.; Munguambe, K. Health Impacts of Industrial Mining on Surrounding Communities: Local Perspectives from Three Sub-Saharan African Countries. PLoS ONE 2021, 16, e0252433. [Google Scholar] [CrossRef]
- Dietler, D.; Farnham, A.; Lyatuu, I.; Fink, G.; Winkler, M.S. Industrial Mining and HIV Risk: Evidence from 39 Mine Openings across 16 Countries in Sub-Saharan Africa. AIDS 2022, 36, 1573–1581. [Google Scholar] [CrossRef]
- Castro, M.C.; Peterka, C. Malaria Is Increasing in Indigenous and Artisanal Mining Areas in the Brazilian Amazon. Nat. Med. 2023, 29, 762–764. [Google Scholar] [CrossRef]
- Shandro, J.A.; Veiga, M.M.; Shoveller, J.; Scoble, M.; Koehoorn, M. Perspectives on Community Health Issues and the Mining Boom–Bust Cycle. Resour. Policy 2011, 36, 178–186. [Google Scholar] [CrossRef]
- Sharma, S.; Rees, S. Consideration of the Determinants of Women’s Mental Health in Remote Australian Mining Towns. Aust. J. Rural. Health 2007, 15, 1–7. [Google Scholar] [CrossRef]
- Donato, D.B.; Nichols, O.; Possingham, H.; Moore, M.; Ricci, P.F.; Noller, B.N. A Critical Review of the Effects of Gold Cyanide-Bearing Tailings Solutions on Wildlife. Environ. Int. 2007, 33, 974–984. [Google Scholar] [CrossRef]
- Hassan, N.A.; Sahani, M.; Hod, R.; Yahya, N.A. A Study on Exposure to Cyanide Among a Community Living Near a Gold Mine in Malaysia. J. Environ. Health 2015, 77, 42–49. [Google Scholar]
- Kwaansa-Ansah, E.E.; Amenorfe, L.P.; Armah, E.K.; Opoku, F. Human Health Risk Assessment of Cyanide Levels in Water and Tuber Crops from Kenyasi, a Mining Community in the Brong Ahafo Region of Ghana. Int. J. Food Contam. 2017, 4, 16. [Google Scholar] [CrossRef]
- Martin, A.; Arias, J.; Lopez, J.; Santos, L.; Venegas, C.; Duarte, M.; Ortiz-Ardila, A.; de Parra, N.; Campos, C.; Celis Zambrano, C. Evaluation of the Effect of Gold Mining on the Water Quality in Monterrey, Bolivar (Colombia). Water 2020, 12, 2523. [Google Scholar] [CrossRef]
- Harington, J.S.; McGlashan, N.D.; Chelkowska, E.Z. A Century of Migrant Labour in the Gold Mines of South Africa. J. South. Afr. Inst. Min. Metall. 2004, 104, 65–71. [Google Scholar]
- Ouoba, Y. Artisanal versus Industrial Mining: Impacts on Poverty in Regions of Burkina Faso. Miner. Econ. 2017, 30, 181–191. [Google Scholar] [CrossRef]
- Kleinschmidt, I.; Schwabe, C.; Benavente, L.; Torrez, M.; Ridl, F.C.; Segura, J.L.; Ehmer, P.; Nchama, G.N. Marked Increase in Child Survival after Four Years of Intensive Malaria Control. Am. J. Trop. Med. Hyg. 2009, 80, 882–888. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Musunka, G.; Pascall, A.; Nduna, K.; Ng’uni, H.; Utzinger, J.; Winkler, M.S. Selected Indicators and Determinants of Women’s Health in the Vicinity of a Copper Mine Development in Northwestern Zambia. BMC Women’s Health 2018, 18, 62. [Google Scholar] [CrossRef]
- Lange, S.; Kolstad, I. Corporate Community Involvement and Local Institutions: Two Case Studies From the Mining Industry in Tanzania. J. Afr. Bus. 2012, 13, 134–144. [Google Scholar] [CrossRef]
- Winkler, M.; Viliani, F.; Knoblauch, A.; Cave, B.; Divall, M.; Ramesh, G.; Harris-Roxas, B.; Furu, P. Health Impact Assessment International Best Practice Principles; Special Publication Series No. 5; International Association for Impact Assessment: Fargo, ND, USA, 2021. [Google Scholar]
- Zabré, H.R.; Knoblauch, A.M.; Diagbouga, S.P.; Fink, G.; Owuor, M.; Nduna, K.; Chisanga, M.; Musunka, G.; Divall, M.J.; Winkler, M.S.; et al. Changes in Socioeconomic Determinants of Health in a Copper Mine Development Area, Northwestern Zambia. Extr. Ind. Soc. 2021, 8, 100985. [Google Scholar] [CrossRef]
- Hilson, A.; Hilson, G.; Dauda, S. Corporate Social Responsibility at African Mines: Linking the Past to the Present. J. Environ. Manag. 2019, 241, 340–352. [Google Scholar] [CrossRef]
- Hilson, G. Corporate Social Responsibility in the Extractive Industries: Experiences from Developing Countries. Resour. Policy 2012, 37, 131–137. [Google Scholar] [CrossRef]
- Kapelus, P. Mining, Corporate Social Responsibility and the “Community”: The Case of Rio Tinto, Richards Bay Minerals and the Mbonambi. J. Bus. Ethics 2002, 39, 275–296. [Google Scholar] [CrossRef]
- Rodrigues, M.; Mendes, L. Mapping of the Literature on Social Responsibility in the Mining Industry: A Systematic Literature Review. J. Clean. Prod. 2018, 181, 88–101. [Google Scholar] [CrossRef]
- Bezzola, S.; Günther, I.; Brugger, F.; Lefoll, E. CSR and Local Conflicts in African Mining Communities. World Dev. 2022, 158, 105968. [Google Scholar] [CrossRef]
- Brugger, F. Getting a Social License: Enough to Catch the Elusive Ghost in Town? Oil Gas Energy Law 2020, 18, 1–15. [Google Scholar]
- Garvin, T.; McGee, T.K.; Smoyer-Tomic, K.E.; Aubynn, E.A. Community–Company Relations in Gold Mining in Ghana. J. Environ. Manag. 2009, 90, 571–586. [Google Scholar] [CrossRef]
- Agyemang-Duah, W.; Arthur-Holmes, F.; Sobeng, A.K.; Peprah, P.; Dokbila, J.M.; Asare, E.; Okyere, J. Corporate Social Responsibility in Public Health Provision: Community Members’ Assessment. Cogent Med. 2019, 6, 1622999. [Google Scholar] [CrossRef]
- Ololade, O.O.; Annegarn, H.J. Contrasting Community and Corporate Perceptions of Sustainability: A Case Study within the Platinum Mining Region of South Africa. Resour. Policy 2013, 38, 568–576. [Google Scholar] [CrossRef]
- Mabey, P.T.; Li, W.; Sundufu, A.J.; Lashari, A.H. Environmental Impacts: Local Perspectives of Selected Mining Edge Communities in Sierra Leone. Sustainability 2020, 12, 5525. [Google Scholar] [CrossRef]
- Brisbois, B.W.; Reschny, J.; Fyfe, T.M.; Harder, H.G.; Parkes, M.W.; Allison, S.; Buse, C.G.; Fumerton, R.; Oke, B. Mapping Research on Resource Extraction and Health: A Scoping Review. Extr. Ind. Soc. 2019, 6, 250–259. [Google Scholar] [CrossRef]
- Karakaya, E.; Nuur, C. Social Sciences and the Mining Sector: Some Insights into Recent Research Trends. Resour. Policy 2018, 58, 257–267. [Google Scholar] [CrossRef]
- Leuenberger, A.; Farnham, A.; Azevedo, S.; Cossa, H.; Dietler, D.; Nimako, B.; Adongo, P.B.; Merten, S.; Utzinger, J.; Winkler, M.S. Health Impact Assessment and Health Equity in Sub-Saharan Africa: A Scoping Review. Environ. Impact Assess. Rev. 2019, 79, 106288. [Google Scholar] [CrossRef]
- Farnham, A.; Cossa, H.; Dietler, D.; Engebretsen, R.; Leuenberger, A.; Lyatuu, I.; Nimako, B.; Zabre, H.R.; Brugger, F.; Winkler, M.S. Investigating Health Impacts of Natural Resource Extraction Projects in Burkina Faso, Ghana, Mozambique, and Tanzania: Protocol for a Mixed Methods Study. JMIR Res. Protoc. 2020, 9, e17138. [Google Scholar] [CrossRef]
- Sofaer, S. Qualitative Methods: What Are They and Why Use Them? Health Serv. Res. 1999, 34, 1101–1118. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Endeavour Mining Houndé Mine. Available online: https://www.endeavourmining.com/our-business/our-assets/hound%C3%A9-mine (accessed on 7 April 2021).
- Mining Data Online Bissa Mine (Bissa-Bouly Operation). Available online: https://miningdataonline.com/property/555/Bissa-Mine.aspx (accessed on 11 January 2021).
- Mining Data Online Yaramoko Mine (Bagassi South Mine). Available online: https://miningdataonline.com/property/561/Yaramoko.aspx (accessed on 11 January 2021).
- Kanstrup, A.M.; Bertelsen, P.; Madsen, J.Ø. Design with the Feet: Walking Methods and Participatory Design. In Proceedings of the 13th Participatory Design Conference, Windhoek, Namibia, 6–10 October 2014: Research Papers—Volume 1; Association for Computing Machinery: New York, NY, USA, 2014; pp. 51–60. [Google Scholar] [CrossRef]
- Maman, S.; Lane, T.; Ntogwisangu, J.; Modiba, P.; Vanrooyen, H.; Timbe, A.; Visrutaratna, S.; Fritz, K. Using Participatory Mapping to Inform a Community-Randomized Trial of HIV Counseling and Testing. Field Methods 2009, 21, 368–387. [Google Scholar] [CrossRef]
- Mulopo, C.; Mbereko, A.; Chimbari, M. Community Mapping and Transect Walks to Determine Schistosomiasis Risk Factors Related to WASH Practices in KwaZulu-Natal. Waterlines 2020, 39, 253–276. [Google Scholar] [CrossRef]
- Rutta, E.; Williams, H.; Mwansasu, A.; Mung’ong’o, F.; Burke, H.; Gongo, R.; Veneranda, R.; Qassim, M. Refugee Perceptions of the Quality of Healthcare: Findings from a Participatory Assessment in Ngara, Tanzania. Disasters 2005, 29, 291–309. [Google Scholar] [CrossRef]
- Leuenberger, A.; Winkler, M.S.; Lyatuu, I.; Cossa, H.; Zabré, H.R.; Dietler, D.; Farnham, A. Incorporating Community Perspectives in Health Impact Assessment: A Toolbox. Environ. Impact Assess. Rev. 2022, 95, 106788. [Google Scholar] [CrossRef]
- Anderson, C. Presenting and Evaluating Qualitative Research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef]
- Verma, S.; Gautam, R.; Pandey, S.; Mishra, A.; Shukla, S. Sampling Typology and Techniques. Int. J. Sci. Res. 2017, 5, 2321-0613. [Google Scholar]
- Leuenberger, A.; Kihwele, F.; Lyatuu, I.; Kengia, J.T.; Farnham, A.; Winkler, M.S.; Merten, S. Gendered Health Impacts of Industrial Gold Mining in Northwestern Tanzania: Perceptions of Local Communities. Impact Assess. Proj. Apprais. 2021, 39, 183–195. [Google Scholar] [CrossRef]
- Ploughman, M.; Austin, M.; Stefanelli, M.; Godwin, M. Applying Cognitive Debriefing to Pre-Test Patient-Reported Outcomes in Older People with Multiple Sclerosis. Qual. Life Res. 2010, 19, 483–487. [Google Scholar] [CrossRef]
- Responsive Translation What Is Cognitive Debriefing and How Does It Improve Instrument Validity?|Responsive Translation. 2015. Available online: https://www.responsivetranslation.com/blog/cognitive-debriefing/ (accessed on 13 April 2021).
- Health Statistics and Information Systems, World Health Organization. Service Availability and Readiness Assessment (SARA): An Annual Monitoring System for Service Delivery. Available online: https://www.who.int/data/data-collection-tools/service-availability-and-readiness-assessment-(sara) (accessed on 6 December 2023).
- Cronjé, F.; Reyneke, S.; Wyk, D. van Local Communities and Health Disaster Management in the Mining Sector. Jàmbá J. Disaster Risk Stud. 2013, 5, 12. [Google Scholar] [CrossRef]
- Benshaul-Tolonen, A.; Chuhan-Pole, P.; Dabalen, A.; Kotsadam, A.; Sanoh, A. The Local Socioeconomic Effects of Gold Mining: Evidence from Ghana. Extr. Ind. Soc. 2019, 6, 1234–1255. [Google Scholar] [CrossRef]
- Gamu, J.; Le Billon, P.; Spiegel, S. Extractive Industries and Poverty: A Review of Recent Findings and Linkage Mechanisms. Extr. Ind. Soc. 2015, 2, 162–176. [Google Scholar] [CrossRef]
- Antabe, R.; Atuoye, K.N.; Kuuire, V.Z.; Sano, Y.; Arku, G.; Luginaah, I. Community Health Impacts of Surface Mining in the Upper West Region of Ghana: The Roles of Mining Odors and Dust. Hum. Ecol. Risk Assess. Int. J. 2017, 23, 798–813. [Google Scholar] [CrossRef]
- Porgo, M.; Gokyay, O. Environmental Impacts of Gold Mining in Essakane Site of Burkina Faso. Hum. Ecol. Risk Assess. Int. J. 2017, 23, 641–654. [Google Scholar] [CrossRef]
- Sharp, B.; van Wyk, P.; Sikasote, J.B.; Banda, P.; Kleinschmidt, I. Malaria Control by Residual Insecticide Spraying in Chingola and Chililabombwe, Copperbelt Province, Zambia. Trop. Med. Int. Health 2002, 7, 732–736. [Google Scholar] [CrossRef]
- White, L.; Noble, B.F. Strategic Environmental Assessment for Sustainability: A Review of a Decade of Academic Research. Environ. Impact Assess. Rev. 2013, 42, 60–66. [Google Scholar] [CrossRef]
- Lokuwaduge, C.S.D.S.; Heenetigala, K. Integrating Environmental, Social and Governance (ESG) Disclosure for a Sustainable Development: An Australian Study. Bus. Strategy Environ. 2017, 26, 438–450. [Google Scholar] [CrossRef]
- Muhirwa, F.; Shen, L.; Elshkaki, A.; Hirwa, H.; Umuziranenge, G.; Velempini, K. Linking Large Extractive Industries to Sustainable Development of Rural Communities at Mining Sites in Africa: Challenges and Pathways. Resour. Policy 2023, 81, 103322. [Google Scholar] [CrossRef]
- Ribeiro-Duthie, A.C.; Domingos, L.M.B.; Oliveira, M.F.; Araujo, P.C.; Alamino, R.C.J.; Silva, R.S.V.; Ribeiro-Duthie, J.M.; Castilhos, Z.C. Sustainable Development Opportunities within Corporate Social Responsibility Practices from LSM to ASM in the Gold Mining Industry. Miner. Econ. 2017, 30, 141–152. [Google Scholar] [CrossRef]
- Langston, J.D.; Lubis, M.I.; Sayer, J.A.; Margules, C.; Boedhihartono, A.K.; Dirks, P.H.G.M. Comparative Development Benefits from Small and Large Scale Mines in North Sulawesi, Indonesia. Extr. Ind. Soc. 2015, 2, 434–444. [Google Scholar] [CrossRef]
- Zvarivadza, T. Large Scale Miners—Communities Partnerships: A Plausible Option for Communities Survival beyond Mine Closure. Available online: https://reader.elsevier.com/reader/sd/pii/S0301420717303719?token=4E4391B5980F3BDEDACBF0924C4EC5EBD955DF0740656B951C71A78D7CD3E99B6C2BBD324A3717A410038EB34B9755F8&originRegion=eu-west-1&originCreation=20210405203320 (accessed on 5 April 2021).
- Adusah-Karikari, A. Black Gold in Ghana: Changing Livelihoods for Women in Communities Affected by Oil Production. Extr. Ind. Soc. 2015, 2, 24–32. [Google Scholar] [CrossRef]
- Doso Jnr, S.; Ayensu-Ntim, A.; Twumasi-Ankrah, B.; Twum Barimah, P. Effects of Loss of Agricultural Land Due to Large-Scale Gold Mining on Agriculture in Ghana: The Case of the Western Region. Br. J. Res. 2015, 2, 196–221. [Google Scholar]
- Omorodion, F.I. The Impact of Petroleum Refinery on the Economic Livelihoods of Women in the Niger Delta Region of Nigeria. A J. Cult. Afr. Women Stud. 2004, 6, 1–15. [Google Scholar]
- Whitehead, A.; Kabeer, N. Living with Unvertainty: Gender, Livelihods and Pro-Poor Growth in Rural Sub-Saharan Africa. Working Paper No. 134. Institute of Development Studies. 2001. Available online: https://www.ids.ac.uk/download.php?file=files/Wp134.pdf (accessed on 25 November 2023).
- Muchadenyika, D. Women Struggles and Large-Scale Diamond Mining in Marange, Zimbabwe. Extr. Ind. Soc. 2015, 2, 714–721. [Google Scholar] [CrossRef]
- Tolonen, A. Local Industrial Shocks, Female Empowerment and Infant Health: Evidence from Africa’s Gold Mining Industry. Job Mark. Paper. 2014, Volume 72. Available online: https://www.worldbank.org/content/dam/Worldbank/document/Gender/JMP_Tolonen.pdf (accessed on 25 November 2023).
- Jenkins, K. Women, Mining and Development: An Emerging Research Agenda. Extr. Ind. Soc. 2014, 1, 329–339. [Google Scholar] [CrossRef]
- Duflo, E. Women Empowerment and Economic Development. J. Econ. Lit. 2012, 50, 1051–1079. [Google Scholar] [CrossRef]
- Kabeer, N. Gender, Poverty, and Inequality: A Brief History of Feminist Contributions in the Field of International Development. Gend. Dev. 2015, 23, 189–205. [Google Scholar] [CrossRef]
- Kabeer, N.; Natali, L. Gender Equality and Economic Growth: Is There a Win-Win? IDS Work. Pap. 2013, 2013, 1–58. [Google Scholar] [CrossRef]
- IFC. Women in Mining; International Finance Corporation: Washington, DC, USA, 2009. [Google Scholar]
- Eftimie, A.; Heller, K.; Strongman, J. Gender Dimensions of the Extractive Industries: Mining for Equity; The World Bank: Washington, DC, USA, 2009. [Google Scholar]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an Equity Lens to Interventions: Using PROGRESS Ensures Consideration of Socially Stratifying Factors to Illuminate Inequities in Health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef]
- Caxaj, C.S.; Berman, H.; Varcoe, C.; Ray, S.L.; Restoulec, J.-P. Gold Mining on Mayan-Mam Territory: Social Unravelling, Discord and Distress in the Western Highlands of Guatemala. Soc. Sci. Med. 2014, 111, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Curtis, M.; Lissu, T. A Golden Opportunity? How Tanzania Is Failing to Benefit from Gold Mining, 2nd ed.; Christian Council of Tanzania, National Council of Muslims in Tanzania and Tanzania Episcopal Conference: Dar es Salaam, Tanzania, 2008. [Google Scholar]
- Marmot, M. Social Determinants of Health Inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Leuenberger, A.; Cambaco, O.; Zabré, H.R.; Lyatuu, I.; Utzinger, J.; Munguambe, K.; Merten, S.; Winkler, M.S. “It Is Like We Are Living in a Different World”: Health Inequity in Communities Surrounding Industrial Mining Sites in Burkina Faso, Mozambique, and Tanzania. Int. J. Environ. Res. Public Health 2021, 18, 11015. [Google Scholar] [CrossRef] [PubMed]
- Farnham, A.; Loss, G.; Lyatuu, I.; Cossa, H.; Kulinkina, A.V.; Winkler, M.S. A Roadmap for Using DHIS2 Data to Track Progress in Key Health Indicators in the Global South: Experience from Sub-Saharan Africa. BMC Public Health 2023, 23, 1030. [Google Scholar] [CrossRef] [PubMed]
- Gesicho, M.B.; Babic, A. Identifying Barriers and Facilitators in HIV-Indicator Reporting for Different Health Facility Performances: A Qualitative Case Study. PLoS ONE 2021, 16, e0247525. [Google Scholar] [CrossRef]
- Njomo, D.W.; Mukoko, D.A.; Nyamongo, N.K.; Karanja, J. Increasing Coverage in Mass Drug Administration for Lymphatic Filariasis Elimination in an Urban Setting: A Study of Malindi Town, Kenya. PLoS ONE 2014, 9, e83413. [Google Scholar] [CrossRef]
- Pluye, P.; Hong, Q.N. Combining the Power of Stories and the Power of Numbers: Mixed Methods Research and Mixed Studies Reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef]
- Razum, O.; Gerhardus, A. Editorial: Methodological Triangulation in Public Health Research—Advancement or Mirage? Trop. Med. Int. Health 1999, 4, 243–244. [Google Scholar] [CrossRef]
- Beier, J.C.; Keating, J.; Githure, J.I.; Macdonald, M.B.; Impoinvil, D.E.; Novak, R.J. Integrated Vector Management for Malaria Control. Malar. J. 2008, 7, S4. [Google Scholar] [CrossRef]
- Espino, F.E.; Koops, V.; Manderson, L. Community Participation and Tropical Disease Control in Resource-Poor Settings; Social, Economic and Behavioural Research Special Topics No. 2; WHO Special Programme for Research and Training in Tropical Diseases (TDR): Geneva, Switzerland, 2004. [Google Scholar]
- Rifkin, S.B. Community Participation in Maternal and Child Health/Family Planning Programmes: An Analysis Based on Case Study Materials; World Health Organization: Geneva, Switzerland, 1990; ISBN 978-92-4-156135-8. [Google Scholar]
- WHO. Declaration of Alma-Ata: International Conference on Primary Health Care. Available online: https://www.who.int/teams/social-determinants-of-health/declaration-of-alma-ata (accessed on 20 April 2021).
- Coelho, P.; Silva, S.; Roma-Torres, J.; Costa, C.; Henriques, A.; Teixeira, J.; Gomes, M.; Mayan, O. Health Impact of Living near an Abandoned Mine—Case Study: Jales Mines. Int. J. Hyg. Environ. Health 2007, 210, 399–402. [Google Scholar] [CrossRef]
- Kakudji Kyungu, A. Exacerbation of Vulnerability in a Hospital Setting in Lubumbashi (Democratic Republic of Congo). Glob. Health Promot. 2013, 20, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Paoliello, M.M.B.; De Capitani, E.M.; da Cunha, F.G.; Matsuo, T.; de Carvalho, M.F.; Sakuma, A.; Figueiredo, B.R. Exposure of Children to Lead and Cadmium from a Mining Area of Brazil. Environ. Res. 2002, 88, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.; Nyanza, E.C.; Condon, M.; Fisher, J.; Maduka, T.; Benshaul-Tolonen, A. Understanding Environmental, Health and Economic Activity Interactions Following Transition of Ownership in Gold Mining Areas in Tanzania: A Case of Private to Public. Land Use Policy 2018, 79, 650–658. [Google Scholar] [CrossRef]
- Hilson, G. An Overview of Land Use Conflicts in Mining Communities. Land Use Policy 2002, 19, 65–73. [Google Scholar] [CrossRef]
- Wilson, S.A. Company–Community Conflicts Over Diamond Resources in Kono District, Sierra Leone. Soc. Nat. Resour. 2013, 26, 254–269. [Google Scholar] [CrossRef]
- Cernea, M.M. Compensation and Benefit Sharing: Why Resettlement Policies and Practices Must Be Reformed. Water Sci. Eng. 2008, 1, 89–120. [Google Scholar] [CrossRef]
- Lawson, E.T.; Bentil, G. Shifting Sands: Changes in Community Perceptions of Mining in Ghana. Available online: https://link.springer.com/article/10.1007/s10668-013-9472-y (accessed on 13 April 2021).
- Althubaiti, A. Information Bias in Health Research: Definition, Pitfalls, and Adjustment Methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef]
- Newing, H.; Eagle, C.M.; Puri, R.; Watson, C.W. Conducting Research in Conservation: Social Science Methods and Practice; Routledge: Milton Park, UK, 2010; p. 376. ISBN 978-1-136-93440-7. [Google Scholar]




| Health District | Kongoussi | Houndé | Bagassi |
|---|---|---|---|
| Mining project | Bissa Gold Mine | Houndé Gold Mine | Yaramoko Gold Mine |
| Operator (location of corporate office) | Nord Gold SE (Russia) | Endeavour Mining (UK) | Roxgold Inc (Canada) |
| Commodity | Gold | Gold | Gold |
| Operational since | 2013 | 2017 | 2016 |
| Type of mine | Open pit | Open pit | Underground |
| Population Size (2006) | 71,000 | 77,000 | 33,000 |
| Data collection | May 2019 | March 2019 | April/May 2019 |
| Expected mine life | Until 2034 | Until 2027 | Until 2027 |
| Mine | Gender | Mining Officials (n = 5) | Community Leaders (n = 15) | Healthcare Providers (n = 16) | Total n = 36 (%) | |
|---|---|---|---|---|---|---|
| Bissa Gold Mine | Male | 0 | 4 | 3 | 7 | 10 |
| Female | 0 | 1 | 2 | 3 | ||
| Houndé Gold Mine | Male | 1 | 4 | 5 | 10 | 11 |
| Female | 0 | 1 | 0 | 1 | ||
| Yaramoko Gold Mine | Male | 4 | 4 | 6 | 14 | 15 |
| Female | 0 | 1 | 0 | 1 | ||
| Total | Male | 5 | 12 | 14 | 31 (86%) | 36 (100%) |
| Female | 0 | 3 | 2 | 5 (14%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Himmelsbach, G.S.; Zabré, H.R.; Leuenberger, A.; Knoblauch, A.M.; Brugger, F.; Winkler, M.S. Exploring the Impact of Mining on Community Health and Health Service Delivery: Perceptions of Key Informants Involved in Gold Mining Communities in Burkina Faso. Int. J. Environ. Res. Public Health 2023, 20, 7167. https://doi.org/10.3390/ijerph20247167
Himmelsbach GS, Zabré HR, Leuenberger A, Knoblauch AM, Brugger F, Winkler MS. Exploring the Impact of Mining on Community Health and Health Service Delivery: Perceptions of Key Informants Involved in Gold Mining Communities in Burkina Faso. International Journal of Environmental Research and Public Health. 2023; 20(24):7167. https://doi.org/10.3390/ijerph20247167
Chicago/Turabian StyleHimmelsbach, Gianna S., Hyacinthe R. Zabré, Andrea Leuenberger, Astrid M. Knoblauch, Fritz Brugger, and Mirko S. Winkler. 2023. "Exploring the Impact of Mining on Community Health and Health Service Delivery: Perceptions of Key Informants Involved in Gold Mining Communities in Burkina Faso" International Journal of Environmental Research and Public Health 20, no. 24: 7167. https://doi.org/10.3390/ijerph20247167