
Who Let the Dogs Out? Unmasking the Neglected: A Semi-Systematic Review on the Enduring Impact of Toxocariasis, a Prevalent Zoonotic Infection
 , and
, and 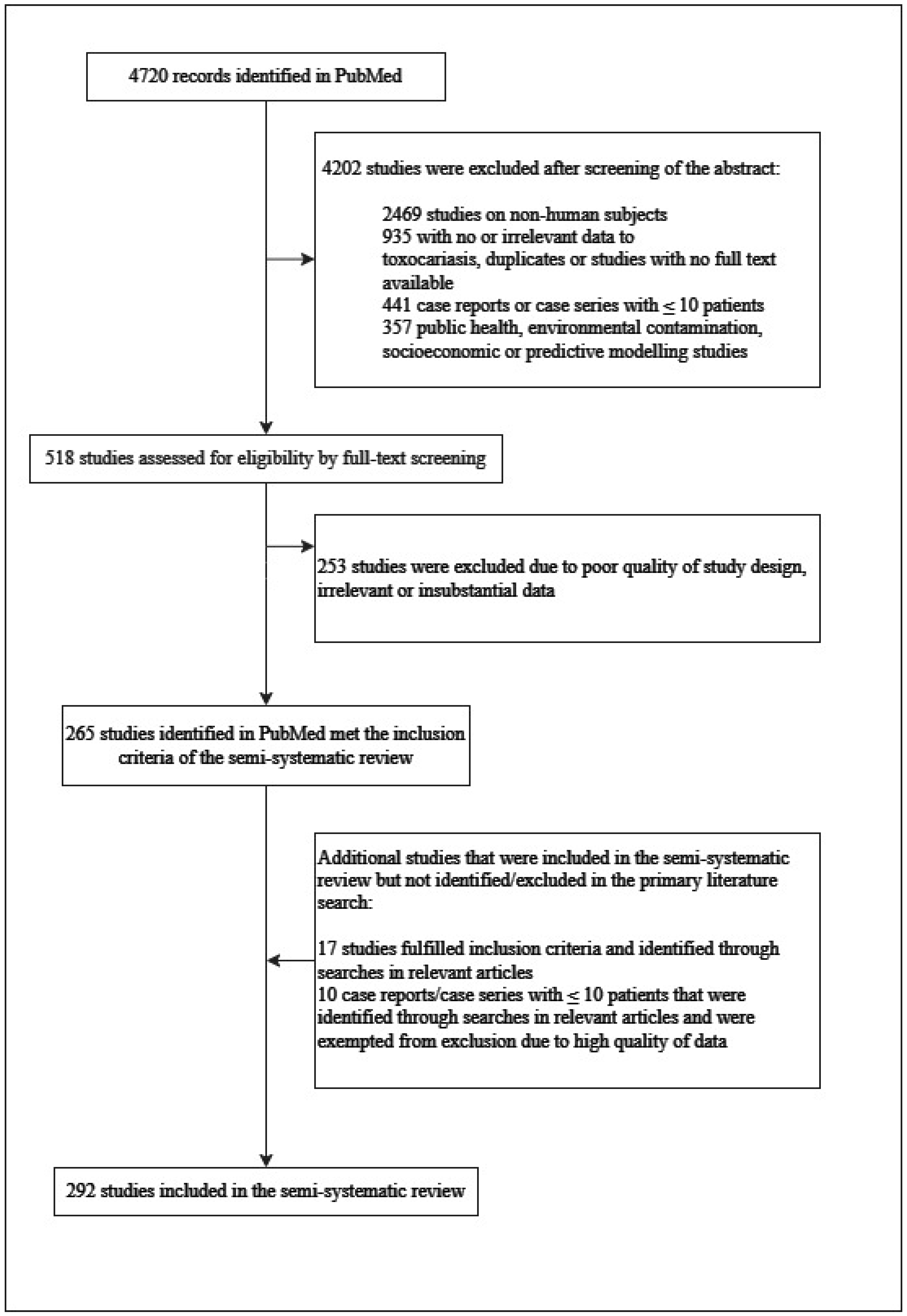{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology
Inclusion Criteria for Narrative Reviews
3. Epidemiology
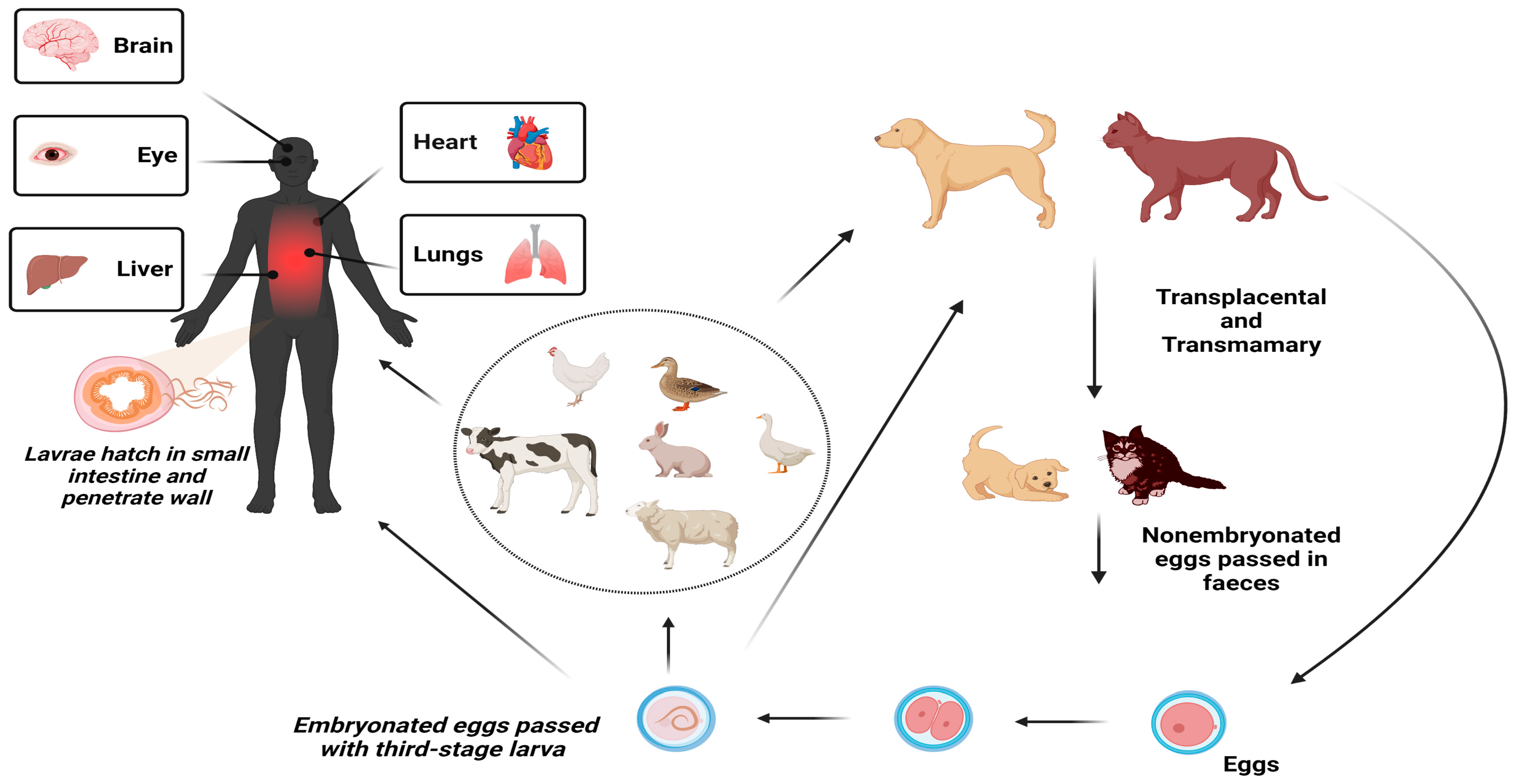
4. Pathophysiology
5. Clinical Presentations
5.1. Visceral Larva Migrans
5.2. Ocular Toxocarosis
5.3. Neurotoxocariasis or Cerebral Toxocariasis
5.4. Covert and Common Toxocarosis
6. Diagnosis of Toxocariasis in Humans
7. Treatment
7.1. Visceral Larval Migrans
7.2. Ocular Toxocarosis
7.3. Neurotoxocariasis
8. Prevention
9. Limitations
10. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bowman, D.D. History of Toxocara and the associated larva migrans. Adv. Parasitol. 2020, 109, 17–38. [Google Scholar] [CrossRef] [PubMed]
- Gasser, R.B.; Korhonen, P.K.; Zhu, X.Q.; Young, N.D. Harnessing the Toxocara Genome to Underpin Toxocariasis Research and New Interventions. Adv. Parasitol. 2016, 91, 87–110. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.Q.; Korhonen, P.K.; Cai, H.; Young, N.D.; Nejsum, P.; von Samson-Himmelstjerna, G.; Boag, P.R.; Tan, P.; Li, Q.; Min, J.; et al. Genetic blueprint of the zoonotic pathogen Toxocara canis. Nat. Commun. 2015, 6, 6145. [Google Scholar] [CrossRef] [PubMed]
- Li, M.W.; Lin, R.Q.; Song, H.Q.; Wu, X.Y.; Zhu, X.Q. The complete mitochondrial genomes for three Toxocara species of human and animal health significance. BMC Genom. 2008, 9, 224. [Google Scholar] [CrossRef] [PubMed]
- Mizgajska-Wiktor, H.; Jarosz, W. A comparison of soil contamination with Toxocara canis and Toxocara cati eggs in rural and urban areas of Wielkopolska district in 2000–2005. Wiadomości Parazytol. 2007, 53, 219–225. [Google Scholar]
- Gawor, J.; Borecka, A. The contamination of the environment with Toxocara eggs in Mazowieckie voivodship as a risk of toxocarosis in children. Wiadomości Parazytol. 2004, 50, 237–241. [Google Scholar]
- Fan, C.K.; Holland, C.V.; Loxton, K.; Barghouth, U. Cerebral Toxocariasis: Silent Progression to Neurodegenerative Disorders? Clin. Microbiol. Rev. 2015, 28, 663–686. [Google Scholar] [CrossRef]
- Beaver, P.C.; Snyder, C.H.; Carrera, G.M.; Dent, J.H.; Lafferty, J.W. Chronic eosinophilia due to visceral larva migrans; report of three cases. Pediatrics 1952, 9, 7–19. [Google Scholar] [CrossRef]
- Fan, C.K.; Liao, C.W.; Cheng, Y.C. Factors affecting disease manifestation of toxocarosis in humans: Genetics and environment. Vet. Parasitol. 2013, 193, 342–352. [Google Scholar] [CrossRef]
- Rostami, A.; Riahi, S.M.; Holland, C.V.; Taghipour, A.; Khalili-Fomeshi, M.; Fakhri, Y.; Omrani, V.F.; Hotez, P.J.; Gasser, R.B. Seroprevalence estimates for toxocariasis in people worldwide: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2019, 13, e0007809. [Google Scholar] [CrossRef]
- Abuseir, S. A systematic review of frequency and geographic distribution of water-borne parasites in the Middle East and North Africa. East. Mediterr. Health J. 2023, 29, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J. Toxocarosis in humans: How much of a problem is it in the UK? Drug Ther. Bull. 2023, 61, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Abbaszadeh Afshar, M.J.; Zahabiun, F.; Heydarian, P.; Mozafar Saadati, H.; Mohtasebi, S.; Khodamoradi, F.; Raissi, V. A Systematic Review and Meta-analysis of Toxocariasis in Iran: Is it Time to Take it Seriously? Acta Parasitol. 2020, 65, 569–584. [Google Scholar] [CrossRef]
- Hotez, P.J.; Wilkins, P.P. Toxocariasis: America’s most common neglected infection of poverty and a helminthiasis of global importance? PLoS Negl. Trop. Dis. 2009, 3, e400. [Google Scholar] [CrossRef]
- Van Den Broucke, S.; Kanobana, K.; Polman, K.; Soentjens, P.; Vekemans, M.; Theunissen, C.; Vlieghe, E.; Van Esbroeck, M.; Jacobs, J.; Van Den Enden, E.; et al. Toxocariasis diagnosed in international travelers at the Institute of Tropical Medicine, Antwerp, Belgium, from 2000 to 2013. PLoS Negl. Trop. Dis. 2015, 9, e0003559. [Google Scholar] [CrossRef] [PubMed]
- Moiyadi, A.; Mahadevan, A.; Anandh, B.; Shivashankar, R.S.; Chickabasavaiah, Y.T.; Shankar, S.K. Visceral larva migrans presenting as multiple intracranial and intraspinal abscesses. Neuropathology 2007, 27, 371–374. [Google Scholar] [CrossRef]
- Finsterer, J.; Auer, H. Neurotoxocarosis. Rev. Inst. Med. Trop. São Paulo 2007, 49, 279–287. [Google Scholar] [CrossRef]
- Kazek, B.; Jamroz, E.; Mandera, M.; Bierzynska-Macyszyn, G.; Kluczewska, E.; Marszal, E. The cerebral form of toxocarosis in a seven-year-old patient. Folia Neuropathol. 2006, 44, 72–76. [Google Scholar]
- Poulsen, C.S.; Skov, S.; Yoshida, A.; Skallerup, P.; Maruyama, H.; Thamsborg, S.M.; Nejsum, P. Differential serodiagnostics of Toxocara canis and Toxocara cati—Is it possible? Parasite Immunol. 2015, 37, 204–207. [Google Scholar] [CrossRef]
- Bachli, H.; Minet, J.C.; Gratzl, O. Cerebral toxocariasis: A possible cause of epileptic seizure in children. Child’s Nerv. Syst. 2004, 20, 468–472. [Google Scholar] [CrossRef]
- Lotsch, F.; Vingerling, R.; Spijker, R.; Grobusch, M.P. Toxocariasis in humans in Africa—A systematic review. Travel Med. Infect. Dis. 2017, 20, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Hernandez-Bustamante, E.A.; Alarcon-Braga, E.A.; Huayta-Cortez, M.; Carballo-Tello, X.L.; Seminario-Amez, R.A.; Rodriguez-Torres, A.; Casas-Patino, D.; Herrera-Anazco, P.; Benites-Zapata, V.A. Seroprevalence of human toxocariasis in Latin America and the Caribbean: A systematic review and meta-analysis. Front. Public Health 2023, 11, 1181230. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, R.; Rahimi, M.T.; Emameh, R.Z.; Mirzaei, M.; Perez-Cordon, G.; Ahmadpour, E. Status of human toxocariasis, a neglected parasitic zoonosis in Iran: A systematic review from past to current. Trop. Dr. 2020, 50, 285–291. [Google Scholar] [CrossRef]
- Eslahi, A.V.; Badri, M.; Khorshidi, A.; Majidiani, H.; Hooshmand, E.; Hosseini, H.; Taghipour, A.; Foroutan, M.; Pestehchian, N.; Firoozeh, F.; et al. Prevalence of Toxocara and Toxascaris infection among human and animals in Iran with meta-analysis approach. BMC Infect. Dis. 2020, 20, 20. [Google Scholar] [CrossRef] [PubMed]
- Korsholm, E. Toxocara canis as a cause of visceral larva migrans. Survival and development of eggs in the environment and potential ways of transmission to man: A review. Nord. Vet. Med. 1982, 34, 1–12. [Google Scholar]
- Marx, M.B. Parasites, pets, and people. Prim. Care 1991, 18, 153–165. [Google Scholar] [CrossRef]
- Choi, D.; Lim, J.H.; Choi, D.C.; Lee, K.S.; Paik, S.W.; Kim, S.H.; Choi, Y.H.; Huh, S. Transmission of Toxocara canis via ingestion of raw cow liver: A cross-sectional study in healthy adults. Korean J. Parasitol. 2012, 50, 23–27. [Google Scholar] [CrossRef]
- Choi, D.; Lim, J.H.; Choi, D.C.; Paik, S.W.; Kim, S.H.; Huh, S. Toxocariasis and ingestion of raw cow liver in patients with eosinophilia. Korean J. Parasitol. 2008, 46, 139–143. [Google Scholar] [CrossRef]
- Schantz, P.M.; Glickman, L.T. Toxocaral visceral larva migrans. N. Engl. J. Med. 1978, 298, 436–439. [Google Scholar] [CrossRef]
- Despommier, D. Toxocariasis: Clinical aspects, epidemiology, medical ecology, and molecular aspects. Clin. Microbiol. Rev. 2003, 16, 265–272. [Google Scholar] [CrossRef]
- Nicoletti, A. Toxocariasis. Handb. Clin. Neurol. 2013, 114, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, A. Neurotoxocariasis. Adv. Parasitol. 2020, 109, 219–231. [Google Scholar] [CrossRef]
- Cojocariu, I.E.; Bahnea, R.; Luca, C.; Leca, D.; Luca, M. Clinical and biological features of adult toxocariasis. Rev. Med. Chir. Soc. Medici Nat. Iasi 2012, 116, 1162–1165. [Google Scholar]
- Smith, H.; Holland, C.; Taylor, M.; Magnaval, J.F.; Schantz, P.; Maizels, R. How common is human toxocariasis? Towards standardizing our knowledge. Trends Parasitol. 2009, 25, 182–188. [Google Scholar] [CrossRef]
- Chen, J.; Zhou, D.H.; Nisbet, A.J.; Xu, M.J.; Huang, S.Y.; Li, M.W.; Wang, C.R.; Zhu, X.Q. Advances in molecular identification, taxonomy, genetic variation and diagnosis of Toxocara spp. Infect. Genet. Evol. 2012, 12, 1344–1348. [Google Scholar] [CrossRef] [PubMed]
- Rubinsky-Elefant, G.; Hirata, C.E.; Yamamoto, J.H.; Ferreira, M.U. Human toxocariasis: Diagnosis, worldwide seroprevalences and clinical expression of the systemic and ocular forms. Ann. Trop. Med. Parasitol. 2010, 104, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Woodhall, D.M.; Fiore, A.E. Toxocariasis: A Review for Pediatricians. J. Pediatr. Infect. Dis. Soc. 2014, 3, 154–159. [Google Scholar] [CrossRef]
- Abd El Wahab, W.M.; Ali, M.I.; Ibrahim, S.S.; Mohamed, Y.A.; Hamdy, D.A. Toxocariasis: Potential association with bronchial asthma, and pneumonia among pediatric children. J. Parasit. Dis. 2023, 47, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Aghaei, S.; Riahi, S.M.; Rostami, A.; Mohammadzadeh, I.; Javanian, M.; Tohidi, E.; Foroutan, M.; Esmaeili Dooki, M. Toxocara spp. infection and risk of childhood asthma: A systematic review and meta-analysis. Acta Trop. 2018, 182, 298–304. [Google Scholar] [CrossRef]
- Gale, S.D.; Hedges, D.W. Neurocognitive and neuropsychiatric effects of toxocariasis. Adv. Parasitol. 2020, 109, 261–272. [Google Scholar] [CrossRef]
- Fan, C.K. Pathogenesis of cerebral toxocariasis and neurodegenerative diseases. Adv. Parasitol. 2020, 109, 233–259. [Google Scholar] [CrossRef] [PubMed]
- Luna, J.; Cicero, C.E.; Rateau, G.; Quattrocchi, G.; Marin, B.; Bruno, E.; Dalmay, F.; Druet-Cabanac, M.; Nicoletti, A.; Preux, P.M. Updated evidence of the association between toxocariasis and epilepsy: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006665. [Google Scholar] [CrossRef] [PubMed]
- Anisuzzaman; Hossain, M.S.; Hatta, T.; Labony, S.S.; Kwofie, K.D.; Kawada, H.; Tsuji, N.; Alim, M.A. Food- and vector-borne parasitic zoonoses: Global burden and impacts. Adv. Parasitol. 2023, 120, 87–136. [Google Scholar] [CrossRef] [PubMed]
- Anisuzzaman; Tsuji, N. Schistosomiasis and hookworm infection in humans: Disease burden, pathobiology and anthelmintic vaccines. Parasitol. Int. 2020, 75, 102051. [Google Scholar] [CrossRef]
- Devleesschauwer, B.; Ale, A.; Torgerson, P.; Praet, N.; Maertens de Noordhout, C.; Pandey, B.D.; Pun, S.B.; Lake, R.; Vercruysse, J.; Joshi, D.D.; et al. The burden of parasitic zoonoses in Nepal: A systematic review. PLoS Negl. Trop. Dis. 2014, 8, e2634. [Google Scholar] [CrossRef]
- Strube, C.; Raulf, M.K.; Springer, A.; Waindok, P.; Auer, H. Seroprevalence of human toxocarosis in Europe: A review and meta-analysis. Adv. Parasitol. 2020, 109, 375–418. [Google Scholar] [CrossRef]
- Fisher, M. Toxocara cati: An underestimated zoonotic agent. Trends Parasitol. 2003, 19, 167–170. [Google Scholar] [CrossRef]
- Maciag, L.; Morgan, E.R.; Holland, C. Toxocara: Time to let cati ‘out of the bag’. Trends Parasitol. 2022, 38, 280–289. [Google Scholar] [CrossRef]
- Rostami, A.; Ma, G.; Wang, T.; Koehler, A.V.; Hofmann, A.; Chang, B.C.H.; Macpherson, C.N.; Gasser, R.B. Human toxocariasis—A look at a neglected disease through an epidemiological ‘prism’. Infect. Genet. Evol. 2019, 74, 104002. [Google Scholar] [CrossRef]
- Sariego, I.; Kanobana, K.; Rojas, L.; Speybroeck, N.; Polman, K.; Nunez, F.A. Toxocariasis in Cuba: A literature review. PLoS Negl. Trop. Dis. 2012, 6, e1382. [Google Scholar] [CrossRef]
- Ma, G.; Rostami, A.; Wang, T.; Hofmann, A.; Hotez, P.J.; Gasser, R.B. Global and regional seroprevalence estimates for human toxocariasis: A call for action. Adv. Parasitol. 2020, 109, 275–290. [Google Scholar] [CrossRef] [PubMed]
- Fakhri, Y.; Gasser, R.B.; Rostami, A.; Fan, C.K.; Ghasemi, S.M.; Javanian, M.; Bayani, M.; Armoon, B.; Moradi, B. Toxocara eggs in public places worldwide—A systematic review and meta-analysis. Environ. Pollut. 2018, 242, 1467–1475. [Google Scholar] [CrossRef] [PubMed]
- Healy, S.R.; Morgan, E.R.; Prada, J.M.; Betson, M. Brain food: Rethinking food-borne toxocariasis. Parasitology 2022, 149, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zyoud, S.H. Global toxocariasis research trends from 1932 to 2015: A bibliometric analysis. Health Res. Policy Syst. 2017, 15, 14. [Google Scholar] [CrossRef] [PubMed]
- Pozio, E. How globalization and climate change could affect foodborne parasites. Exp. Parasitol. 2020, 208, 107807. [Google Scholar] [CrossRef]
- Macpherson, C.N. The epidemiology and public health importance of toxocariasis: A zoonosis of global importance. Int. J. Parasitol. 2013, 43, 999–1008. [Google Scholar] [CrossRef]
- Azam, D.; Ukpai, O.M.; Said, A.; Abd-Allah, G.A.; Morgan, E.R. Temperature and the development and survival of infective Toxocara canis larvae. Parasitol. Res. 2012, 110, 649–656. [Google Scholar] [CrossRef]
- Marmor, M.; Glickman, L.; Shofer, F.; Faich, L.A.; Rosenberg, C.; Cornblatt, B.; Friedman, S. Toxocara canis infection of children: Epidemiologic and neuropsychologic findings. Am. J. Public Health 1987, 77, 554–559. [Google Scholar] [CrossRef]
- Figueiredo, S.D.; Taddei, J.A.; Menezes, J.J.; Novo, N.F.; Silva, E.O.; Cristovao, H.L.; Cury, M.C. Clinical-epidemiological study of toxocariasis in a pediatric population. J. Pediatr. (Rio J.) 2005, 81, 126–132. [Google Scholar] [CrossRef]
- Bowman, D.D. Ascaris and Toxocara as foodborne and waterborne pathogens. Res. Vet. Sci. 2021, 135, 1–7. [Google Scholar] [CrossRef]
- Serrano-Moliner, M.; Morales-Suarez-Varela, M.; Valero, M.A. Epidemiology and management of foodborne nematodiasis in the European Union, systematic review 2000–2016. Pathog. Glob. Health 2018, 112, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Merigueti, Y.; Giuffrida, R.; da Silva, R.C.; Kmetiuk, L.B.; Santos, A.P.D.; Biondo, A.W.; Santarem, V.A. Dog and Cat Contact as Risk Factor for Human Toxocariasis: Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 854468. [Google Scholar] [CrossRef] [PubMed]
- Omonijo, A.O.; Kalinda, C.; Mukaratirwa, S. A systematic review and meta-analysis of canine, feline and human Toxocara infections in sub-Saharan Africa. J. Helminthol. 2019, 94, e96. [Google Scholar] [CrossRef]
- Gottstein, B.; Piarroux, R. Current trends in tissue-affecting helminths. Parasite 2008, 15, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Abou-El-Naga, I.F.; Mogahed, N. Potential roles of Toxocara canis larval excretory secretory molecules in immunomodulation and immune evasion. Acta Trop. 2023, 238, 106784. [Google Scholar] [CrossRef]
- Bowman, D.D. The anatomy of the third-stage larva of Toxocara canis and Toxocara cati. Adv. Parasitol. 2020, 109, 39–61. [Google Scholar] [CrossRef]
- Overgaauw, P.A.; van Knapen, F. Veterinary and public health aspects of Toxocara spp. Vet. Parasitol. 2013, 193, 398–403. [Google Scholar] [CrossRef]
- Roddie, G.; Stafford, P.; Holland, C.; Wolfe, A. Contamination of dog hair with eggs of Toxocara canis. Vet. Parasitol. 2008, 152, 85–93. [Google Scholar] [CrossRef]
- El-Tras, W.F.; Holt, H.R.; Tayel, A.A. Risk of Toxocara canis eggs in stray and domestic dog hair in Egypt. Vet. Parasitol. 2011, 178, 319–323. [Google Scholar] [CrossRef]
- Salem, G.; Schantz, P. Toxocaral visceral larva migrans after ingestion of raw lamb liver. Clin. Infect. Dis. 1992, 15, 743–744. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Nishiofuku, M.; Moriya, K.; Ouji, Y.; Ishizaka, S.; Kasahara, K.; Mikasa, K.; Hirai, T.; Mizuno, Y.; Ogawa, S.; et al. A familial case of visceral toxocariasis due to consumption of raw bovine liver. Parasitol. Int. 2008, 57, 525–529. [Google Scholar] [CrossRef]
- Epe, C.; Sabel, T.; Schnieder, T.; Stoye, M. The behavior and pathogenicity of Toxacara canis larvae in mice of different strains. Parasitol. Res. 1994, 80, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Gavignet, B.; Piarroux, R.; Aubin, F.; Millon, L.; Humbert, P. Cutaneous manifestations of human toxocariasis. J. Am. Acad. Dermatol. 2008, 59, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Zibaei, M.; Shayesteh, Z.; Moradi, N.; Bahadory, S. Human Toxocara Infection: Allergy and Immune Responses. Antiinflamm. Antiallergy Agents Med. Chem. 2019, 18, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Holland, C.V.; Hamilton, C.M. The significance of cerebral toxocariasis: A model system for exploring the link between brain involvement, behaviour and the immune response. J. Exp. Biol. 2013, 216, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Obwaller, A.; Jensen-Jarolim, E.; Auer, H.; Huber, A.; Kraft, D.; Aspock, H. Toxocara infestations in humans: Symptomatic course of toxocarosis correlates significantly with levels of IgE/anti-IgE immune complexes. Parasite Immunol. 1998, 20, 311–317. [Google Scholar] [CrossRef]
- Maizels, R.M. Toxocara canis: Molecular basis of immune recognition and evasion. Vet. Parasitol. 2013, 193, 365–374. [Google Scholar] [CrossRef]
- Waindok, P.; Janecek-Erfurth, E.; Lindenwald, D.; Wilk, E.; Schughart, K.; Geffers, R.; Balas, L.; Durand, T.; Rund, K.M.; Schebb, N.H.; et al. Multiplex profiling of inflammation-related bioactive lipid mediators in Toxocara canis- and Toxocara cati-induced neurotoxocarosis. PLoS Negl. Trop. Dis. 2019, 13, e0007706. [Google Scholar] [CrossRef]
- Mitre, E.; Klion, A.D. Eosinophils and helminth infection: Protective or pathogenic? Semin. Immunopathol. 2021, 43, 363–381. [Google Scholar] [CrossRef]
- Anisuzzaman; Hatta, T.; Miyoshi, T.; Matsubayashi, M.; Islam, M.K.; Alim, M.A.; Anas, M.A.; Hasan, M.M.; Matsumoto, Y.; Yamamoto, Y.; et al. Longistatin in tick saliva blocks advanced glycation end-product receptor activation. J. Clin. Investig. 2014, 124, 4429–4444. [Google Scholar] [CrossRef]
- Ushio, H.; Hirota, S.; Jippo, T.; Higuchi, S.; Kawamoto, K.; Kitamura, Y.; Matsuda, H. Mechanisms of eosinophilia in mice infested with larval Haemaphysalis longicornis ticks. Immunology 1995, 84, 469–475. [Google Scholar] [PubMed]
- Masure, D.; Vlaminck, J.; Wang, T.; Chiers, K.; Van den Broeck, W.; Vercruysse, J.; Geldhof, P. A role for eosinophils in the intestinal immunity against infective Ascaris suum larvae. PLoS Negl. Trop. Dis. 2013, 7, e2138. [Google Scholar] [CrossRef] [PubMed]
- Balla, K.M.; Lugo-Villarino, G.; Spitsbergen, J.M.; Stachura, D.L.; Hu, Y.; Banuelos, K.; Romo-Fewell, O.; Aroian, R.V.; Traver, D. Eosinophils in the zebrafish: Prospective isolation, characterization, and eosinophilia induction by helminth determinants. Blood 2010, 116, 3944–3954. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.J.; Askenase, P.W. Blood eosinophil and basophil responses in guinea pigs parasitized by Amblyomma americanum ticks. Am. J. Trop. Med. Hyg. 1982, 31, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.R.; Keane, C.T.; O’Connor, P.; Mulvihill, E.; Holland, C. The expanded spectrum of toxocaral disease. Lancet 1988, 1, 692–695. [Google Scholar] [CrossRef]
- Pawlowski, Z. Toxocariasis in humans: Clinical expression and treatment dilemma. J. Helminthol. 2001, 75, 299–305. [Google Scholar] [CrossRef]
- Del Prete, G.F.; De Carli, M.; Mastromauro, C.; Biagiotti, R.; Macchia, D.; Falagiani, P.; Ricci, M.; Romagnani, S. Purified protein derivative of Mycobacterium tuberculosis and excretory-secretory antigen(s) of Toxocara canis expand in vitro human T cells with stable and opposite (type 1 T helper or type 2 T helper) profile of cytokine production. J. Clin. Investig. 1991, 88, 346–350. [Google Scholar] [CrossRef]
- Kayes, S.G. Human toxocariasis and the visceral larva migrans syndrome: Correlative immunopathology. Chem. Immunol. 1997, 66, 99–124. [Google Scholar] [CrossRef]
- Fauser, S.; Kern, P. T-lymphocyte cytokine mRNA expression in cystic echinococcosis. Acta Trop. 1997, 64, 35–51. [Google Scholar] [CrossRef]
- Mazur-Melewska, K.; Jonczyk, K.; Modlinska-Cwalinska, A.; Figlerowicz, M.; Sluzewski, W. Visceral larva migrans syndrome: Analysis of serum cytokine levels in children with hepatic lesions confirmed in radiological findings. Parasite Immunol. 2014, 36, 668–673. [Google Scholar] [CrossRef]
- Nagy, D.; Bede, O.; Danka, J.; Szenasi, Z.; Sipka, S. Analysis of serum cytokine levels in children with chronic cough associated with Toxocara canis infection. Parasite Immunol. 2012, 34, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Takamoto, M.; Kusama, Y.; Takatsu, K.; Nariuchi, H.; Sugane, K. Occurrence of interleukin-5 production by CD4- CD8- (double-negative) T cells in lungs of both normal and congenitally athymic nude mice infected with Toxocara canis. Immunology 1995, 85, 285–291. [Google Scholar] [PubMed]
- Anisuzzaman, M.; Khyrul Islam, M.; Abdul Alim, M.; Miyoshi, T.; Hatta, T.; Yamaji, K.; Matsumoto, Y.; Fujisaki, K.; Tsuji, N. Longistatin, a plasminogen activator, is key to the availability of blood-meals for ixodid ticks. PLoS Pathog. 2011, 7, e1001312. [Google Scholar] [CrossRef] [PubMed]
- Anisuzzaman, M.; Khyrul Islam, M.; Abdul Alim, M.; Miyoshi, T.; Hatta, T.; Yamaji, K.; Matsumoto, Y.; Fujisaki, K.; Tsuji, N. Longistatin, a novel plasminogen activator from vector ticks, is resistant to plasminogen activator inhibitor-1. Biochem. Biophys. Res. Commun. 2011, 413, 599–604. [Google Scholar] [CrossRef]
- Ackerman, S.J.; Bochner, B.S. Mechanisms of eosinophilia in the pathogenesis of hypereosinophilic disorders. Immunol. Allergy Clin. N. Am. 2007, 27, 357–375. [Google Scholar] [CrossRef]
- Dent, L.A.; Daly, C.M.; Mayrhofer, G.; Zimmerman, T.; Hallett, A.; Bignold, L.P.; Creaney, J.; Parsons, J.C. Interleukin-5 transgenic mice show enhanced resistance to primary infections with Nippostrongylus brasiliensis but not primary infections with Toxocara canis. Infect. Immun. 1999, 67, 989–993. [Google Scholar] [CrossRef]
- Abdala-Valencia, H.; Coden, M.E.; Chiarella, S.E.; Jacobsen, E.A.; Bochner, B.S.; Lee, J.J.; Berdnikovs, S. Shaping eosinophil identity in the tissue contexts of development, homeostasis, and disease. J. Leukoc. Biol. 2018, 104, 95–108. [Google Scholar] [CrossRef]
- Kay, A.B. The role of eosinophils in the pathogenesis of asthma. Trends Mol. Med. 2005, 11, 148–152. [Google Scholar] [CrossRef]
- Kay, A.B.; Phipps, S.; Robinson, D.S. A role for eosinophils in airway remodelling in asthma. Trends Immunol. 2004, 25, 477–482. [Google Scholar] [CrossRef]
- Gomes, I.; Mathur, S.K.; Espenshade, B.M.; Mori, Y.; Varga, J.; Ackerman, S.J. Eosinophil-fibroblast interactions induce fibroblast IL-6 secretion and extracellular matrix gene expression: Implications in fibrogenesis. J. Allergy Clin. Immunol. 2005, 116, 796–804. [Google Scholar] [CrossRef]
- Valent, P.; Klion, A.D.; Horny, H.P.; Roufosse, F.; Gotlib, J.; Weller, P.F.; Hellmann, A.; Metzgeroth, G.; Leiferman, K.M.; Arock, M.; et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J. Allergy Clin. Immunol. 2012, 130, 607–612.e609. [Google Scholar] [CrossRef] [PubMed]
- van Balkum, M.; Kluin-Nelemans, H.; van Hellemond, J.J.; van Genderen, P.J.J.; Wismans, P.J. Hypereosinophilia: A diagnostic challenge. Neth. J. Med. 2018, 76, 431–436. [Google Scholar] [PubMed]
- Gillespie, S.H. Human toxocariasis. J. Appl. Bacteriol. 1987, 63, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Sugane, K.; Kusama, Y.; Takamoto, M.; Tominaga, A.; Takatsu, K. Eosinophilia, IL-5 level and recovery of larvae in IL-5 transgenic mice infected with Toxocara canis. J. Helminthol. 1996, 70, 153–158. [Google Scholar] [CrossRef]
- Takamoto, M.; Ovington, K.S.; Behm, C.A.; Sugane, K.; Young, I.G.; Matthaei, K.I. Eosinophilia, parasite burden and lung damage in Toxocara canis infection in C57Bl/6 mice genetically deficient in IL-5. Immunology 1997, 90, 511–517. [Google Scholar] [CrossRef]
- Parsons, J.C.; Coffman, R.L.; Grieve, R.B. Antibody to interleukin 5 prevents blood and tissue eosinophilia but not liver trapping in murine larval toxocariasis. Parasite Immunol. 1993, 15, 501–508. [Google Scholar] [CrossRef]
- Amor, D.; Santos, L.N.; Silva, E.S.; de Santana, M.B.R.; Belitardo, E.; Sena, F.A.; Pontes-de-Carvalho, L.; Figueiredo, C.A.; Alcantara-Neves, N.M. Toxocara canis extract fractions promote mainly the production of Th1 and regulatory cytokines by human leukocytes in vitro. Acta Trop. 2022, 234, 106579. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Baek, S.; Park, S.Y.; Shin, B.; Kwon, H.S.; Cho, Y.S.; Moon, H.B.; Kim, T.B. Clinical course and treatment outcomes of toxocariasis-related eosinophilic disorder. Medicine 2018, 97, e12361. [Google Scholar] [CrossRef]
- Lamina, J. Visceral larva migrans infections caused by toxocara species (author’s transl). Dtsch. Med. Wochenschr. 1980, 105, 796–799. [Google Scholar] [CrossRef]
- Pivetti-Pezzi, P. Ocular toxocariasis. Int. J. Med. Sci. 2009, 6, 129–130. [Google Scholar] [CrossRef]
- Katz, M. Anthelmintics. Drugs 1977, 13, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Kuenzli, E.; Neumayr, A.; Chaney, M.; Blum, J. Toxocariasis-associated cardiac diseases—A systematic review of the literature. Acta Trop. 2016, 154, 107–120. [Google Scholar] [CrossRef]
- Barisani-Asenbauer, T.; Maca, S.M.; Hauff, W.; Kaminski, S.L.; Domanovits, H.; Theyer, I.; Auer, H. Treatment of ocular toxocariasis with albendazole. J. Ocul. Pharmacol. Ther. 2001, 17, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Meliou, M.; Mavridis, I.N.; Pyrgelis, E.S.; Agapiou, E. Toxocariasis of the Nervous System. Acta Parasitol. 2020, 65, 291–299. [Google Scholar] [CrossRef]
- Hoffmeister, B.; Glaeser, S.; Flick, H.; Pornschlegel, S.; Suttorp, N.; Bergmann, F. Cerebral toxocariasis after consumption of raw duck liver. Am. J. Trop Med. Hyg. 2007, 76, 600–602. [Google Scholar] [CrossRef]
- Springer, A.; Heuer, L.; Janecek-Erfurth, E.; Beineke, A.; Strube, C. Histopathological characterization of Toxocara canis- and T. cati-induced neurotoxocarosis in the mouse model. Parasitol. Res. 2019, 118, 2591–2600. [Google Scholar] [CrossRef] [PubMed]
- Dousset, V.; Sibon, I.; Menegon, P. Case no 6. Cerebral vasculitis due to Toxocara canis (or catis) origin. J. Radiol. 2003, 84, 89–91. [Google Scholar] [PubMed]
- Lompo, L.D.; Kamdem, F.K.; Revenco, E.; Allibert, R.; Medeiros, E.; Vuillier, F.; Moulin, T. Toxocara canis cerebral vasculitis revealed by iterative strokes. Rev. Neurol. 2012, 168, 533–537. [Google Scholar] [CrossRef]
- Fellrath, J.M.; Magnaval, J.F. Toxocariasis after slug ingestion characterized by severe neurologic, ocular, and pulmonary involvement. Open Forum Infect. Dis. 2014, 1, ofu063. [Google Scholar] [CrossRef]
- Hamidou, M.A.; Fradet, G.; Kadi, A.M.; Robin, A.; Moreau, A.; Magnaval, J.F. Systemic vasculitis with lymphocytic temporal arteritis and Toxocara canis infection. Arch. Intern. Med. 2002, 162, 1521–1524. [Google Scholar] [CrossRef]
- de Boysson, H.; Martin Silva, N.; Comoz, F.; Boutemy, J.; Bienvenu, B. Vasculitis secondary to anti-C1q antibodies induced by Toxocariasis. Infection 2015, 43, 755–758. [Google Scholar] [CrossRef] [PubMed]
- Maiga, Y.; Wiertlewski, S.; Desal, H.; Marjolet, M.; Damier, P. Presentation of cerebral toxocariasis with mental confusion in an adult: Case report and review of the literature. Bull. Soc. Pathol. Exot. 2007, 100, 101–104. [Google Scholar] [PubMed]
- Ardiles, A.; Chanqueo, L.; Reyes, V.; Araya, L. Toxocariasis in an adult manifested as hypereosinophilic syndrome with predominant neurological involvement. Clinical case. Rev. Med. Chile 2001, 129, 780–785. [Google Scholar] [PubMed]
- Oujamaa, L.; Sibon, I.; Vital, A.; Menegon, P. Cerebral vasculitis secondary to Toxocara canis and Fasciola hepatica co-infestation. Rev. Neurol. 2003, 159, 447–450. [Google Scholar]
- Stiles, C.W. The determination of generic types, and a list of roundworm genera with their original and type species. In Bulletin 79; Stiles, C.W., Hassall, A., Eds.; Bureau of Animal Industry, United States Department of Agriculture: Washington, DC, USA, 1905; pp. 1–150. [Google Scholar]
- Wilder, H.C. Nematode endophthalmitis. Trans. Am. Acad. Ophthalmol. Otolaryngol. 1950, 55, 99–109. [Google Scholar]
- Chandler, A.C. The helminthic parasites of cats in Calcutta and the relation of cats to human helminthic infections. Indian J. Med. Res. 1925, 23, 213–227. [Google Scholar]
- Fülleborn, F. Askarisinfektion durch Verzehren eingekapselter Larven und übergelungene intrauterine Askarisinfektion. Arch. Schiffs-u. Tropen-Hyg. 1921, 25, 367–375. [Google Scholar]
- Schwartz, B. Some parasites of dogs and cats transmissible to human beings and domesticated animals. Vet. Alumni Quart. Ohio State Univ. 1932, 20, 5. [Google Scholar]
- Nichols, R.L. The etiology of visceral larva migrans. I. Diagnostic morphology of infective second-stage Toxocara larvae. J. Parasitol. 1956, 42, 349–362. [Google Scholar] [CrossRef]
- Strube, C.; Heuer, L.; Janecek, E. Toxocara spp. infections in paratenic hosts. Vet. Parasitol. 2013, 193, 375–389. [Google Scholar] [CrossRef]
- Magnaval, J.F.; Glickman, L.T.; Dorchies, P.; Morassin, B. Highlights of human toxocariasis. Korean J. Parasitol. 2001, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Moreira, G.M.; Telmo, P.d.L.; Mendonca, M.; Moreira, A.N.; McBride, A.J.; Scaini, C.J.; Conceicao, F.R. Human toxocariasis: Current advances in diagnostics, treatment, and interventions. Trends Parasitol. 2014, 30, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Akao, N.; Ohta, N. Toxocariasis in Japan. Parasitol. Int. 2007, 56, 87–93. [Google Scholar] [CrossRef]
- Raistrick, E.R.; Hart, J.C. Ocular toxocariasis in adults. Br. J. Ophthalmol. 1976, 60, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Fillaux, J.; Cassaing, S.; Valentin, A.; Iriart, X.; Berry, A. Human toxocariasis and atopy. Parasite 2020, 27, 32. [Google Scholar] [CrossRef] [PubMed]
- Juarez, X.S.; Delgado, M.; Matteucci, E.D.; Schiavino, S.; Pasinovich, M.E.; Garcia-Franco, L.; Cancellara, A.D. Toxocariasis in children: Analysis of 85 cases in a paediatric hospital in Argentina. Rev. Chilena Infectol. 2021, 38, 761–767. [Google Scholar] [CrossRef]
- Lee, K.H.; Kim, T.J.; Lee, K.W. Pulmonary Toxocariasis: Initial and Follow-up CT Findings in 63 Patients. AJR Am. J. Roentgenol. 2015, 204, 1203–1211. [Google Scholar] [CrossRef]
- Bolivar-Mejia, A.; Rodriguez-Morales, A.J.; Paniz-Mondolfi, A.E.; Delgado, O. Cardiovascular manifestations of human toxocariasis. Arch. Cardiol. Mex. 2013, 83, 120–129. [Google Scholar] [CrossRef]
- Stoicescu, R.M.; Mihai, C.M.; Giannakopoulou, A.D. Marked hypereosinophilia in a toddler: A case report. J. Med. Life 2011, 4, 105–108. [Google Scholar]
- Musso, C.; Castelo, J.S.; Tsanaclis, A.M.; Pereira, F.E. Prevalence of Toxocara-induced liver granulomas, detected by immunohistochemistry, in a series of autopsies at a Children’s Reference Hospital in Vitoria, ES, Brazil. Virchows Arch. 2007, 450, 411–417. [Google Scholar] [CrossRef]
- Hartleb, M.; Januszewski, K. Severe hepatic involvement in visceral larva migrans. Eur. J. Gastroenterol. Hepatol. 2001, 13, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Shimokawa, H.; Kubota, T.; Nawa, Y.; Takeshita, A. Myocarditis associated with visceral larva migrans due to Toxocara canis. Intern. Med. 2002, 41, 706–708. [Google Scholar] [CrossRef] [PubMed]
- Enko, K.; Tada, T.; Ohgo, K.O.; Nagase, S.; Nakamura, K.; Ohta, K.; Ichiba, S.; Ujike, Y.; Nawa, Y.; Maruyama, H.; et al. Fulminant eosinophilic myocarditis associated with visceral larva migrans caused by Toxocara canis infection. Circ. J. 2009, 73, 1344–1348. [Google Scholar] [CrossRef] [PubMed]
- Humbert, P.; Niezborala, M.; Salembier, R.; Aubin, F.; Piarroux, R.; Buchet, S.; Barale, T. Skin manifestations associated with toxocariasis: A case-control study. Dermatology 2000, 201, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Minciullo, P.L.; Cascio, A.; Gangemi, S. Association between urticaria and nematode infections. Allergy Asthma Proc. 2018, 39, 86–95. [Google Scholar] [CrossRef]
- Kabaalioglu, A.; Ceken, K.; Alimoglu, E.; Saba, R.; Apaydin, A. Hepatic toxocariasis: US, CT and MRI findings. Ultraschall Med. 2005, 26, 329–332. [Google Scholar] [CrossRef]
- Lim, J.H. Toxocariasis of the liver: Visceral larva migrans. Abdom. Imaging 2008, 33, 151–156. [Google Scholar] [CrossRef]
- Hrusovsky, S.; Krcmery, V.; Sobota, K.; Cermak, P.; Andre, I.; Sobotova, O.; Dubrava, M.; Kovac, A.; Gocar, E. Ultrasonography of echinococcosis, toxocariasis and cysticercosis of the liver. Ceskoslovenska Radiol. 1989, 43, 318–324. [Google Scholar]
- Mukund, A.; Arora, A.; Patidar, Y.; Mangla, V.; Bihari, C.; Rastogi, A.; Sarin, S.K. Eosinophilic abscesses: A new facet of hepatic visceral larva migrans. Abdom. Imaging 2013, 38, 774–777. [Google Scholar] [CrossRef]
- Raffray, L.; Le Bail, B.; Malvy, D. Hepatic visceral larva migrans presenting as a pseudotumor. Clin. Gastroenterol. Hepatol. 2013, 11, e42. [Google Scholar] [CrossRef]
- Woodhall, D.; Starr, M.C.; Montgomery, S.P.; Jones, J.L.; Lum, F.; Read, R.W.; Moorthy, R.S. Ocular toxocariasis: Epidemiologic, anatomic, and therapeutic variations based on a survey of ophthalmic subspecialists. Ophthalmology 2012, 119, 1211–1217. [Google Scholar] [CrossRef]
- Sil, A.; Bhanja, D.B.; Chandra, A.; Biswas, S.K. Loeffler’s Syndrome and Multifocal Cutaneous Larva Migrans: Case report of an uncommon occurrence and review of the literature. Sultan Qaboos Univ. Med J. 2023, 23, 104–108. [Google Scholar] [CrossRef]
- Sharghi, N.; Schantz, P.M.; Caramico, L.; Ballas, K.; Teague, B.A.; Hotez, P.J. Environmental exposure to Toxocara as a possible risk factor for asthma: A clinic-based case-control study. Clin. Infect. Dis. 2001, 32, E111–E116. [Google Scholar] [CrossRef]
- Buijs, J.; Egbers, M.W.; Nijkamp, F.P. Toxocara canis-induced airway eosinophilia and tracheal hyporeactivity in guinea pigs and mice. Eur. J. Pharmacol. 1995, 293, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Pinelli, E.; Aranzamendi, C. Toxocara infection and its association with allergic manifestations. Endocr. Metab. Immune Disord. Drug Targets 2012, 12, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Desowitz, R.S.; Rudoy, R.; Barnwell, J.W. Antibodies to canine helminth parasites in asthmatic and nonasthmatic children. Int. Arch. Allergy Appl. Immunol. 1981, 65, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Sandra Guadalupe, B.G.; Mario Noe, M.G.; Gustavo Esteban, P.A.; Norma Yvett, G.B.; Karina, C.S.; Alma Leticia, C.Z.; Alan Eduardo, H.S.; Jose Guadalupe, H.L.; Alvaro, P.M.; Alejandro Gabriel, G.G.; et al. Detection of antigens and anti-Toxocara canis antibodies in children with different asthma severities. Immun. Inflamm. Dis. 2021, 9, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Darvish, S.; Mohammadzadeh, I.; Mehravar, S.; Spotin, A.; Rostami, A. The association between seropositivity to human toxocariasis and childhood asthma in northern Iran: A case-control study. Allergol. Immunopathol. 2021, 49, 25–31. [Google Scholar] [CrossRef]
- Fialho, P.M.M.; Correa, C.R.S.; Lescano, S.Z. Asthma and Seroconversion from Toxocara spp. Infection: Which Comes First? BioMed Res. Int. 2018, 2018, 4280792. [Google Scholar] [CrossRef]
- Cadore, P.S.; Zhang, L.; Lemos, L.d.L.; Lorenzi, C.; Telmo, P.d.L.; Dos Santos, P.C.; Mattos, G.T.; Vignol, F.S.; Prietsch, S.O.; Berne, M.E.; et al. Toxocariasis and childhood asthma: A case-control study. J. Asthma 2016, 53, 601–606. [Google Scholar] [CrossRef]
- Li, L.; Gao, W.; Yang, X.; Wu, D.; Bi, H.; Zhang, S.; Huang, M.; Yao, X. Asthma and toxocariasis. Ann. Allergy Asthma Immunol. 2014, 113, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Bahnea, R.G.; Cardei, E.; Luca, M.C.; Cojocaru, I.; Ripa, C.; Luca, M. Cutaneous manifestations on toxocariasis cases hospitalized in the Paediatric Diseases Clinic of Iasi, between 2005–2008. Rev. Med. Chir. Soc. Med. Nat. Iasi 2009, 113, 428–431. [Google Scholar] [PubMed]
- Doury, P. Is there a role for parasites in the etiology of inflammatory rheumatism? Bull. Acad. Natl. Med. 1990, 174, 743–751; discussion 751–754. [Google Scholar]
- Auer, H.; Walochnik, J. Toxocariasis and the clinical spectrum. Adv. Parasitol. 2020, 109, 111–130. [Google Scholar] [CrossRef] [PubMed]
- Rayes, A.A.; Teixeira, D.; Serufo, J.C.; Nobre, V.; Antunes, C.M.; Lambertucci, J.R. Human toxocariasis and pyogenic liver abscess: A possible association. Am. J. Gastroenterol. 2001, 96, 563–566. [Google Scholar] [CrossRef]
- Smith, H.V. Antibody reactivity in human toxocariasis. In Toxocara and Toxocariasis: Clinical, Epidemiological, and Molecular Perspectives; Lewis, J.W., Maizels, R.M., Eds.; Institute of Biology and the British Society for Parasitology: London, UK, 1993; pp. 91–109. [Google Scholar]
- Dinning, W.J.; Gillespie, S.H.; Cooling, R.J.; Maizels, R.M. Toxocariasis: A practical approach to management of ocular disease. Eye 1988, 2 Pt 5, 580–582. [Google Scholar] [CrossRef]
- Stewart, J.M.; Cubillan, L.D.; Cunningham, E.T., Jr. Prevalence, clinical features, and causes of vision loss among patients with ocular toxocariasis. Retina 2005, 25, 1005–1013. [Google Scholar] [CrossRef]
- Krasny, J.; Sach, J. Forms of Ocular Larval Toxocariasis in Childhood. A Review. Ceska Slov. Oftalmol. 2022, 2, 1001–1009. [Google Scholar] [CrossRef]
- Badri, M.; Eslahi, A.V.; Olfatifar, M.; Dalvand, S.; Houshmand, E.; Abdoli, A.; Majidiani, H.; Eslami, A.; Zibaei, M.; Johkool, M.G.; et al. Keys to Unlock the Enigma of Ocular Toxocariasis: A Systematic Review and Meta-analysis. Ocul. Immunol. Inflamm. 2021, 29, 1265–1276. [Google Scholar] [CrossRef]
- Urban, B.; Bakunowicz-Lazarczyk, A.; Michal, S. Clinical features, the effectiveness of treatment and function of vision organ in children and adolescents with ocular toxocariasis. Klin. Ocz. 2008, 110, 364–366. [Google Scholar]
- Sanchez, T.J.; Lopez, G.J.; Gonzalez, N.M.; Villaseca, D.E.; Manieu, M.D.; Roizen, B.A.; Noemi, H.I.; Viovy, A.A. Prevalence of ocular lesions in children seropositive to Toxocara canis. Rev. Chil. Infectología 2011, 28, 431–434. [Google Scholar] [CrossRef]
- Kwon, S.I.; Lee, J.P.; Park, S.P.; Lee, E.K.; Huh, S.; Park, I.W. Ocular toxocariasis in Korea. Jpn. J. Ophthalmol. 2011, 55, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Chang, Q.; Gonzales, J.A.; Chen, Q.; Zhang, Y.; Huang, X.; Xu, G.; Wang, W.; Jiang, R. Clinical characteristics of ocular toxocariasis in Eastern China. Graefe’s Arch. Clin. Exp. Ophthalmol. 2012, 250, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Woo, S.J.; Hyon, J.Y.; Park, K.H. Cataract formation associated with ocular toxocariasis. J. Cataract. Refract. Surg. 2013, 39, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Despreaux, R.; Fardeau, C.; Touhami, S.; Brasnu, E.; Champion, E.; Paris, L.; Touitou, V.; Bodaghi, B.; Lehoang, P. Ocular Toxocariasis: Clinical Features and Long-term Visual Outcomes in Adult Patients. Am. J. Ophthalmol. 2016, 166, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, Q.; Li, J.; Ji, X.; Xu, Y.; Zhao, P. Clinical Characteristics of Pediatric Patients with Ocular Toxocariasis in China. Ophthalmologica 2016, 235, 97–105. [Google Scholar] [CrossRef]
- Sahu, E.S.; Pal, B.; Sharma, T.; Biswas, J. Clinical Profile, Treatment, and Visual Outcome of Ocular Toxocara in a Tertiary Eye Care Centre. Ocul. Immunol. Inflamm. 2018, 26, 753–759. [Google Scholar] [CrossRef]
- Morocoima, A.; Herrera, L.; Ruiz, E.; Cordova, M.; Ferrer, E. Ocular manifestations of toxocariasis in schoolchildren from the state from the Anzoategui state in Venezuela. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 621–626. [Google Scholar] [CrossRef]
- Wang, H.; Tao, Y. Clinical Features and Prognostic Factors in Northern Chinese Patients with Peripheral Granuloma Type of Ocular Toxocariasis: A Retrospective Cohort Study. Ocul. Immunol. Inflamm. 2021, 29, 1259–1264. [Google Scholar] [CrossRef]
- Good, B.; Holland, C.V.; Taylor, M.R.; Larragy, J.; Moriarty, P.; O’Regan, M. Ocular toxocariasis in schoolchildren. Clin. Infect. Dis. 2004, 39, 173–178. [Google Scholar] [CrossRef]
- Shields, J.A. Ocular toxocariasis. A review. Surv. Ophthalmol. 1984, 28, 361–381. [Google Scholar] [CrossRef] [PubMed]
- Small, K.W.; McCuen, B.W., II; de Juan, E., Jr.; Machemer, R. Surgical management of retinal traction caused by toxocariasis. Am. J. Ophthalmol. 1989, 108, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Galindo, V.; Glickman, L.T.; Clanet, M. Human Toxocara infection of the central nervous system and neurological disorders: A case-control study. Parasitology 1997, 115 Pt 5, 537–543. [Google Scholar] [CrossRef]
- Deshayes, S.; Bonhomme, J.; de La Blanchardiere, A. Neurotoxocariasis: A systematic literature review. Infection 2016, 44, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, S.S.; Garcia, H.H.; Nicoletti, A. Clinical and Magnetic Resonance Imaging Findings of Neurotoxocariasis. Front. Neurol. 2018, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Vidal, J.E.; Sztajnbok, J.; Seguro, A.C. Eosinophilic meningoencephalitis due to Toxocara canis: Case report and review of the literature. Am. J. Trop. Med. Hyg. 2003, 69, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Caldera, F.; Burlone, M.E.; Genchi, C.; Pirisi, M.; Bartoli, E. Toxocara encephalitis presenting with autonomous nervous system involvement. Infection 2013, 41, 691–694. [Google Scholar] [CrossRef]
- Ruttinger, P.; Hadidi, H. MRI in cerebral toxocaral disease. J. Neurol. Neurosurg. Psychiatry 1991, 54, 361–362. [Google Scholar] [CrossRef]
- Singer, O.C.; Conrad, F.; Jahnke, K.; Hattingen, E.; Auer, H.; Steinmetz, H. Severe meningoencephalomyelitis due to CNS-Toxocarosis. J. Neurol. 2011, 258, 696–698. [Google Scholar] [CrossRef]
- Quinnell, R.J. Genetics of susceptibility to human helminth infection. Int. J. Parasitol. 2003, 33, 1219–1231. [Google Scholar] [CrossRef]
- Ota, K.V.; Dimaras, H.; Heon, E.; Gallie, B.L.; Chan, H.S. Radiologic surveillance for retinoblastoma metastases unexpectedly showed disseminated toxocariasis in liver, lung, and spinal cord. Can. J. Ophthalmol. 2010, 45, 185–186. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, B.J.; Lee, S.P.; Jeung, Y.J.; Oh, M.J.; Park, M.S.; Paeng, J.W.; Lee, B.J.; Choi, D.C. Toxocariasis might be an important cause of atopic myelitis in Korea. J. Korean Med. Sci. 2009, 24, 1024–1030. [Google Scholar] [CrossRef]
- Kamuyu, G.; Bottomley, C.; Mageto, J.; Lowe, B.; Wilkins, P.P.; Noh, J.C.; Nutman, T.B.; Ngugi, A.K.; Odhiambo, R.; Wagner, R.G.; et al. Exposure to multiple parasites is associated with the prevalence of active convulsive epilepsy in sub-Saharan Africa. PLoS Negl. Trop. Dis. 2014, 8, e2908. [Google Scholar] [CrossRef] [PubMed]
- Akyol, A.; Bicerol, B.; Ertug, S.; Ertabaklar, H.; Kiylioglu, N. Epilepsy and seropositivity rates of Toxocara canis and Toxoplasma gondii. Seizure 2007, 16, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Caballero-Garcia, M.D.L.; Simon-Salvador, J.; Hernandez-Aguilar, J.C.; Reyes-Lopez, A.; Nogueda-Torres, B.; Jimenez-Cardoso, E. Frequency of Toxocara canis antibodies in Mexican paediatric patients with epilepsy. J. Helminthol. 2019, 94, e89. [Google Scholar] [CrossRef] [PubMed]
- Rishi, V.; Singh, R.; Goyal, M.K.; Modi, M.; Garg, V.; Thakur, J.S.; Sehgal, R.K.; Khandelwal, N.; Jain, G.; Kumar, A.S.; et al. Exposure to Toxocara Canis is not Associated with New-Onset Epilepsy. Neurol India 2022, 70, 2383–2387. [Google Scholar] [CrossRef] [PubMed]
- Critchley, E.M.; Vakil, S.D.; Hutchinson, D.N.; Taylor, P. Toxoplasma, Toxocara, and epilepsy. Epilepsia 1982, 23, 315–321. [Google Scholar] [CrossRef]
- Quattrocchi, G.; Nicoletti, A.; Marin, B.; Bruno, E.; Druet-Cabanac, M.; Preux, P.M. Toxocariasis and epilepsy: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2012, 6, e1775. [Google Scholar] [CrossRef]
- Moshe, S.L.; Perucca, E.; Ryvlin, P.; Tomson, T. Epilepsy: New advances. Lancet 2015, 385, 884–898. [Google Scholar] [CrossRef]
- Noormahomed, E.V.; Nhacupe, N.; Mascaro-Lazcano, C.; Mauaie, M.N.; Buene, T.; Funzamo, C.A.; Benson, C.A. A cross-sectional serological study of cysticercosis, schistosomiasis, toxocariasis and echinococcosis in HIV-1 infected people in Beira, Mozambique. PLoS Negl. Trop. Dis. 2014, 8, e3121. [Google Scholar] [CrossRef]
- Dare, L.O.; Bruand, P.E.; Gerard, D.; Marin, B.; Lameyre, V.; Boumediene, F.; Preux, P.M. Associations of mental disorders and neurotropic parasitic diseases: A meta-analysis in developing and emerging countries. BMC Public Health 2019, 19, 1645. [Google Scholar] [CrossRef] [PubMed]
- Taghipour, A.; Habibpour, H.; Mirzapour, A.; Rostami, A. Toxocara infection/exposure and the risk of schizophrenia: A systematic review and meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Sack, U.; Scheibe, R.; Wotzel, M.; Hammerschmidt, S.; Kuhn, H.; Emmrich, F.; Hoheisel, G.; Wirtz, H.; Gessner, C. Multiplex analysis of cytokines in exhaled breath condensate. Cytom. Part A 2006, 69, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Zachariah, S.B.; Zachariah, B.; Varghese, R. Neuroimaging studies of cerebral “visceral larva migrans” syndrome. J. Neuroimaging 1994, 4, 39–40. [Google Scholar] [CrossRef] [PubMed]
- Xinou, E.; Lefkopoulos, A.; Gelagoti, M.; Drevelegas, A.; Diakou, A.; Milonas, I.; Dimitriadis, A.S. CT and MR imaging findings in cerebral toxocaral disease. AJNR Am. J. Neuroradiol. 2003, 24, 714–718. [Google Scholar]
- Lee, I.H.; Kim, S.T.; Oh, D.K.; Kim, H.J.; Kim, K.H.; Jeon, P.; Byun, H.S. MRI findings of spinal visceral larva migrans of Toxocara canis. Eur. J. Radiol. 2010, 75, 236–240. [Google Scholar] [CrossRef]
- Umehara, F.; Ookatsu, H.; Hayashi, D.; Uchida, A.; Douchi, Y.; Kawabata, H.; Goto, R.; Hashiguchi, A.; Matsuura, E.; Okubo, R.; et al. MRI studies of spinal visceral larva migrans syndrome. J. Neurol. Sci. 2006, 249, 7–12. [Google Scholar] [CrossRef]
- Jabbour, R.A.; Kanj, S.S.; Sawaya, R.A.; Awar, G.N.; Hourani, M.H.; Atweh, S.F. Toxocara canis myelitis: Clinical features, magnetic resonance imaging (MRI) findings, and treatment outcome in 17 patients. Medicine 2011, 90, 337–343. [Google Scholar] [CrossRef]
- Taylor, M.R.; Keane, C.T.; O’Connor, P.; Girdwood, R.W.; Smith, H. Clinical features of covert toxocariasis. Scand. J. Infect. Dis. 1987, 19, 693–696. [Google Scholar] [CrossRef]
- Wendler, H. The visceral larva migrans syndrome due to Toxocara canis. Munch. Med. Wochenschr. 1972, 114, 1634–1640. [Google Scholar]
- Chen, J.; Liu, Q.; Liu, G.H.; Zheng, W.B.; Hong, S.J.; Sugiyama, H.; Zhu, X.Q.; Elsheikha, H.M. Toxocariasis: A silent threat with a progressive public health impact. Infect. Dis. Poverty 2018, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Fogt, R. Molecular techniques applied in species identification of Toxocara. Wiadomosci Parazytol. 2006, 52, 31–35. [Google Scholar]
- Roldan, W.H.; Espinoza, Y.A.; Huapaya, P.E.; Jimenez, S. Diagnosis of human toxocarosis. Rev. Peru. Med. Exp. Salud Publica 2010, 27, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Noordin, R.; Yunus, M.H.; Tan Farrizam, S.N.; Arifin, N. Serodiagnostic methods for diagnosing larval toxocariasis. Adv. Parasitol. 2020, 109, 131–152. [Google Scholar] [CrossRef]
- Jones, J.L.; Kruszon-Moran, D.; Won, K.; Wilson, M.; Schantz, P.M. Toxoplasma gondii and Toxocara spp. co-infection. Am. J. Trop. Med. Hyg. 2008, 78, 35–39. [Google Scholar] [CrossRef]
- Rudzinska, M.; Kowalewska, B.; Sikorska, K. Clinical usefulness of Western blotting and ELISA avidity for the diagnosis of human toxocariasis. Parasite Immunol. 2017, 39, 12400. [Google Scholar] [CrossRef]
- Huang, L.; Sun, L.; Liu, C.; Li, S.; Zhang, T.; Luo, X.; Ding, X. Diagnosis of Ocular Toxocariasis by Serum and Aqueous Humor IgG ELISA. Transl. Vis. Sci. Technol. 2021, 10, 33. [Google Scholar] [CrossRef]
- Wickramasinghe, S.; Yatawara, L.; Nagataki, M.; Takamoto, M.; Watanabe, Y.; Rajapakse, R.P.; Uda, K.; Suzuki, T.; Agatsuma, T. Development of a highly sensitive IgG-ELISA based on recombinant arginine kinase of Toxocara canis for serodiagnosis of visceral larva migrans in the murine model. Parasitol. Res. 2008, 103, 853–858. [Google Scholar] [CrossRef]
- Jin, Y.; Shen, C.; Huh, S.; Sohn, W.M.; Choi, M.H.; Hong, S.T. Serodiagnosis of toxocariasis by ELISA using crude antigen of Toxocara canis larvae. Korean J. Parasitol. 2013, 51, 433–439. [Google Scholar] [CrossRef]
- Noordin, R.; Smith, H.V.; Mohamad, S.; Maizels, R.M.; Fong, M.Y. Comparison of IgG-ELISA and IgG4-ELISA for Toxocara serodiagnosis. Acta Trop. 2005, 93, 57–62. [Google Scholar] [CrossRef]
- Fillaux, J.; Magnaval, J.F. Laboratory diagnosis of human toxocariasis. Vet. Parasitol. 2013, 193, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Fabre, R.; Maurieres, P.; Charlet, J.P.; de Larrard, B. Application of the western blotting procedure for the immunodiagnosis of human toxocariasis. Parasitol. Res. 1991, 77, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Skulinova, K.; Novak, J.; Kolarova, L.; Kasny, M. Antigenic Proteins from the Excretory-Secretory Products of Toxocara canis Larvae and Evaluation of Their Potential for Immunodiagnostics of Larval Toxocarosis. Acta Parasitol. 2022, 67, 705–713. [Google Scholar] [CrossRef]
- Roig, J.; Romeu, J.; Riera, C.; Texido, A.; Domingo, C.; Morera, J. Acute eosinophilic pneumonia due to toxocariasis with bronchoalveolar lavage findings. Chest 1992, 102, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Kaneva, E.; Rainova, I.; Harizanov, R.; Kaftandjiev, I. Study of IgG avidity and the level of specific IgA antibodies and their significance in the diagnosis of human toxocarosis. Exp. Parasitol. 2022, 236–237, 108236. [Google Scholar] [CrossRef] [PubMed]
- Watthanakulpanich, D.; Smith, H.V.; Hobbs, G.; Whalley, A.J.; Billington, D. Application of Toxocara canis excretory-secretory antigens and IgG subclass antibodies (IgG1-4) in serodiagnostic assays of human toxocariasis. Acta Trop. 2008, 106, 90–95. [Google Scholar] [CrossRef]
- Roldan, W.H.; Elefant, G.R.; Ferreira, A.W. Immunoglobulin M antibodies are not specific for serodiagnosis of human toxocariasis. Parasite Immunol. 2017, 39, e12447. [Google Scholar] [CrossRef]
- Boldis, V.; Ondriska, F.; Spitalska, E.; Reiterova, K. Immunodiagnostic approaches for the detection of human toxocarosis. Exp. Parasitol. 2015, 159, 252–258. [Google Scholar] [CrossRef]
- Li, M.W.; Lin, R.Q.; Chen, H.H.; Sani, R.A.; Song, H.Q.; Zhu, X.Q. PCR tools for the verification of the specific identity of ascaridoid nematodes from dogs and cats. Mol. Cell. Probes 2007, 21, 349–354. [Google Scholar] [CrossRef]
- Norhaida, A.; Suharni, M.; Liza Sharmini, A.T.; Tuda, J.; Rahmah, N. rTES-30USM: Cloning via assembly PCR, expression, and evaluation of usefulness in the detection of toxocariasis. Ann. Trop. Med. Parasitol. 2008, 102, 151–160. [Google Scholar] [CrossRef]
- Olave, A.M.; Mesa, J.A.; Botero, J.H.; Patino, E.B.; Garcia, G.M.; Alzate, J.F. Production and evaluation of the recombinant antigen TES-30 of Toxocara canis for the immunodiagnosis of toxocariasis. Biomedica 2016, 36, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Knapp, J.; Lallemand, S.; Monnien, F.; Felix, S.; Courquet, S.; Umhang, G.; Millon, L. Real-time multiplex PCR for human echinococcosis and differential diagnosis. Parasite 2023, 30, 3. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.H.; Ma, G.X.; Luo, Y.F.; Luo, Y.L.; Yin, S.S.; Xiong, Y.; Zhou, R.Q. Tissue distribution and functional analysis of vitellogenin-6 of Toxocara canis. Exp. Parasitol. 2017, 177, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Othman, A.A. Therapeutic battle against larval toxocariasis: Are we still far behind? Acta Trop. 2012, 124, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Caumes, E. Treatment of cutaneous larva migrans and Toxocara infection. Fundam. Clin. Pharmacol. 2003, 17, 213–216. [Google Scholar] [CrossRef]
- Ortiz-Perez, E.; Rivera, G.; Salas, C.O.; Zarate-Ramos, J.J.; Trofymchuk, O.S.; Hernandez-Soberanis, L.; Perales-Flores, J.D.; Vazquez, K. Natural and Synthetic Naphthoquinones as Potential Anti-Infective Agents. Curr. Top Med. Chem. 2021, 21, 2046–2069. [Google Scholar] [CrossRef]
- Xiao, S.H.; Wu, H.-M.; Tanner, M.; Utzinger, J.; Wang, C. Tribendimidine: A promising, safe and broad-spectrum anthelmintic agent from China. Acta Trop. 2005, 94, 1–14. [Google Scholar] [CrossRef]
- Lam, N.S.; Long, X.; Su, X.Z.; Lu, F. Artemisinin and its derivatives in treating helminthic infections beyond schistosomiasis. Pharmacol. Res. 2018, 133, 77–100. [Google Scholar] [CrossRef]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; Bethesda: Rockville, MD, USA, 2012. Available online: https://pubmed.ncbi.nlm.nih.gov/31643176/ (accessed on 16 October 2023).
- Silva, T.C.; Mengarda, A.C.; Lemes, B.L.; Lescano, S.A.Z.; Souza, D.C.S.; Lago, J.H.G.; de Moraes, J. N-(4-Methoxyphenyl)Pentanamide, a Simplified Derivative of Albendazole, Displays Anthelmintic Properties against the Nematode Toxocara canis. Microbiol. Spectr. 2022, 10, e0180722. [Google Scholar] [CrossRef]
- Magnaval, J.F. Apparent weak efficacy of ivermectin for treatment of human toxocariasis. Antimicrob. Agents Chemother. 1998, 42, 2770. [Google Scholar] [CrossRef]
- Magnaval, J.F. Comparative efficacy of diethylcarbamazine and mebendazole for the treatment of human toxocariasis. Parasitology 1995, 110 Pt 5, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Charlet, J.P. Comparative efficacy of thiabendazole and mebendazole in the treatment of toxocariasis. Therapie 1987, 42, 541–544. [Google Scholar] [PubMed]
- Sturchler, D.; Schubarth, P.; Gualzata, M.; Gottstein, B.; Oettli, A. Thiabendazole vs. albendazole in treatment of toxocariasis: A clinical trial. Ann. Trop. Med. Parasitol. 1989, 83, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Gyorkos, T.W.; St-Denis, K. Systematic review of exposure to albendazole or mebendazole during pregnancy and effects on maternal and child outcomes, with particular reference to exposure in the first trimester. Int. J. Parasitol. 2019, 49, 541–554. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Han, J.Y.; Ahn, H.K.; Ryu, H.M.; Koren, G. Foetal outcomes after exposure to albendazole in early pregnancy. J. Obstet. Gynaecol. 2017, 37, 1108–1111. [Google Scholar] [CrossRef]
- Salam, R.A.; Haider, B.A.; Humayun, Q.; Bhutta, Z.A. Effect of administration of antihelminthics for soil-transmitted helminths during pregnancy. Cochrane Database Syst. Rev. 2015, 6, CD005547. [Google Scholar] [CrossRef]
- Horton, J. Albendazole: A review of anthelmintic efficacy and safety in humans. Parasitology 2000, 121 (Suppl. S1), S113–S132. [Google Scholar] [CrossRef]
- Morris, D.L.; Smith, P.G. Albendazole in hydatid disease—Hepatocellular toxicity. Trans. R. Soc. Trop. Med. Hyg. 1987, 81, 343–344. [Google Scholar] [CrossRef]
- Ben Fredj, N.; Chaabane, A.; Chadly, Z.; Ben Fadhel, N.; Boughattas, N.A.; Aouam, K. Albendazole-induced associated acute hepatitis and bicytopenia. Scand. J. Infect. Dis. 2014, 46, 149–151. [Google Scholar] [CrossRef]
- Yildiz, B.O.; Haznedaroglu, I.C.; Coplu, L. Albendazole-induced amegakaryocytic thrombocytopenic purpura. Ann. Pharmacother. 1998, 32, 842. [Google Scholar] [CrossRef]
- Polat, C.; Dervisoglu, A.; Hokelek, M.; Yetim, I.; Buyukkarabacak, Y.; Ozkutuk, Y.; Erzurumlu, K. Dual treatment of albendazole in hepatic hydatidosis: New therapeutic modality in 52 cases. J. Gastroenterol. Hepatol. 2005, 20, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, Y.; Yilmaz, C.; Cagin, Y.F.; Atayan, Y.; Karadag, N.; Harputluoglu, M.M.M. Albendazole Induced Recurrent Acute Toxic Hepatitis: A Case Report. Acta Gastroenterol. Belg 2017, 80, 309–311. [Google Scholar]
- Marin Zuluaga, J.I.; Marin Castro, A.E.; Perez Cadavid, J.C.; Restrepo Gutierrez, J.C. Albendazole-induced granulomatous hepatitis: A case report. J. Med. Case Rep. 2013, 7, 201. [Google Scholar] [CrossRef] [PubMed]
- Dayan, A.D. Albendazole, mebendazole and praziquantel. Review of non-clinical toxicity and pharmacokinetics. Acta Trop. 2003, 86, 141–159. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Charlet, J.P. Etude double aveugle de l’efficacité du mébendazole dans le traitement de la toxocarose humaine. Therapie 1992, 47, 145–148. [Google Scholar]
- Braithwaite, P.A.; Thomas, R.J.; Thompson, R.C. Hydatid disease: The alveolar variety in Australia. A case report with comment on the toxicity of mebendazole. Aust. N. Z. J. Surg. 1985, 55, 519–523. [Google Scholar] [CrossRef]
- Miskovitz, P.F.; Javitt, N.B. Leukopenia associated with mebendazole therapy of hydatid disease. Am. J. Trop. Med. Hyg. 1980, 29, 1356–1358. [Google Scholar] [CrossRef]
- Puente, S.; Lago, M.; Subirats, M.; Sanz-Esteban, I.; Arsuaga, M.; Vicente, B.; Alonso-Sardon, M.; Belhassen-Garcia, M.; Muro, A. Imported Mansonella perstans infection in Spain. Infect. Dis. Poverty 2020, 9, 105. [Google Scholar] [CrossRef]
- Boussinesq, M.; Prod’hon, J.; Chippaux, J.P. Onchocerca volvulus: Striking decrease in transmission in the Vina valley (Cameroon) after eight annual large scale ivermectin treatments. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 82–86. [Google Scholar] [CrossRef]
- Marti, H.; Haji, H.J.; Savioli, L.; Chwaya, H.M.; Mgeni, A.F.; Ameir, J.S.; Hatz, C. A comparative trial of a single-dose ivermectin versus three days of albendazole for treatment of Strongyloides stercoralis and other soil-transmitted helminth infections in children. Am. J. Trop. Med. Hyg. 1996, 55, 477–481. [Google Scholar] [CrossRef]
- Ahn, S.J.; Ryoo, N.K.; Woo, S.J. Ocular toxocariasis: Clinical features, diagnosis, treatment, and prevention. Asia Pac. Allergy 2014, 4, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, K.; Kirmse, B.; Bradbury, R.S.; Moorthy, R.S.; Arguello, I.; McGuffey, C.D.; Tieu, B.; Hobbs, C.V. Case Report: Ocular Toxocariasis: A Report of Three Cases from the Mississippi Delta. Am. J. Trop. Med. Hyg. 2019, 100, 1223–1226. [Google Scholar] [CrossRef] [PubMed]
- Rubin, M.L.; Kaufman, H.E.; Tierney, J.P.; Lucas, H.C. An intraretinal nematode (a case report). Trans. Am. Acad. Ophthalmol. Otolaryngol. 1968, 72, 855–866. [Google Scholar] [PubMed]
- Seong, S.; Moon, D.; Lee, D.K.; Kim, H.E.; Oh, H.S.; Kim, S.H.; Kwon, O.W.; You, Y.S. A case of ocular toxocariasis successfully treated with albendazole and triamcinolon. Korean J. Parasitol. 2014, 52, 537–540. [Google Scholar] [CrossRef]
- Hřckova, G. Novel approaches to immunoprophylaxis in toxocariasis. In Toxocara: The Enigmatic Parasite; Holland, C.V., Smith, H.V., Eds.; CAB International: Oxford, UK, 2006; pp. 174–194. [Google Scholar]
- Martinez-Pulgarin, D.F.; Munoz-Urbano, M.; Gomez-Suta, L.D.; Delgado, O.M.; Rodriguez-Morales, A.J. Ocular toxocariasis: New diagnostic and therapeutic perspectives. Recent Pat. Anti-Infect. Drug Discov. 2015, 10, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Frazier, M.; Anderson, M.L.; Sophocleous, S. Treatment of ocular toxocariasis with albendezole: A case report. Optometry 2009, 80, 175–180. [Google Scholar] [CrossRef]
- Zhang, T.; Guo, D.; Xu, G.; Jiang, R. Ocular Toxocariasis: Long-Term Follow-up and Prognosis of Patients following Vitrectomy. Ocul. Immunol. Inflamm. 2020, 28, 517–523. [Google Scholar] [CrossRef]
- Giuliari, G.P.; Ramirez, G.; Cortez, R.T. Surgical treatment of ocular toxocariasis: Anatomic and functional results in 45 patients. Eur. J. Ophthalmol. 2011, 21, 490–494. [Google Scholar] [CrossRef]
- Ahn, S.J.; Woo, S.J.; Jin, Y.; Chang, Y.S.; Kim, T.W.; Ahn, J.; Heo, J.W.; Yu, H.G.; Chung, H.; Park, K.H.; et al. Clinical features and course of ocular toxocariasis in adults. PLoS Negl. Trop. Dis. 2014, 8, e2938. [Google Scholar] [CrossRef]
- el Matri, L.; Ghorbal, M.; Ayadi, A.; Ben Naceur, B.; Triki, M.F. Toxocara canis in apparently bilateral ocular site. J. Fr. Ophtalmol. 1990, 13, 303–308. [Google Scholar]
- Choi, K.D.; Choi, J.H.; Choi, S.Y.; Jung, J.H. Toxocara optic neuropathy: Clinical features and ocular findings. Int. J. Ophthalmol. 2018, 11, 520–523. [Google Scholar] [CrossRef] [PubMed]
- Gass, J.D.; Braunstein, R.A. Further observations concerning the diffuse unilateral subacute neuroretinitis syndrome. Arch. Ophthalmol. 1983, 101, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Zygulska-Machowa, H.; Ziobrowski, S. A case of ocular toxocariasis treated by xenon photocoagulation. Klin. Ocz. 1987, 89, 213–214. [Google Scholar]
- Garcia, H.H. Neurocysticercosis. Neurol. Clin. 2018, 36, 851–864. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, O.; Bialek, R.; Nagele, T.; Dichgans, J. Eosinophilic meningomyelitis in toxocariasis: Case report and review of the literature. Clin. Neurol. Neurosurg. 2005, 107, 432–438. [Google Scholar] [CrossRef]
- Graeff-Teixeira, C.; da Silva, A.C.; Yoshimura, K. Update on eosinophilic meningoencephalitis and its clinical relevance. Clin. Microbiol. Rev. 2009, 22, 322–348. [Google Scholar] [CrossRef]
- Sotelo, J.; Jung, H. Pharmacokinetic optimisation of the treatment of neurocysticercosis. Clin. Pharmacokinet. 1998, 34, 503–515. [Google Scholar] [CrossRef]
- Hombu, A.; Yoshida, A.; Kikuchi, T.; Nagayasu, E.; Kuroki, M.; Maruyama, H. Treatment of larva migrans syndrome with long-term administration of albendazole. J. Microbiol. Immunol. Infect. 2019, 52, 100–105. [Google Scholar] [CrossRef]
- Jabbour, R.; Atweh, L.A.; Atweh, S. Migration of Toxocara canis into the spinal cord in poorly treated patients. Neurology 2015, 84 (Suppl. S14), P6.327. Available online: https://n.neurology.org/content/84/14_Supplement/P6.327.short (accessed on 16 October 2023).
- Goffette, S.; Jeanjean, A.P.; Duprez, T.P.; Bigaignon, G.; Sindic, C.J. Eosinophilic pleocytosis and myelitis related to Toxocara canis infection. Eur. J. Neurol. 2000, 7, 703–706. [Google Scholar] [CrossRef]
- Wang, J.L.; Li, T.T.; Huang, S.Y.; Cong, W.; Zhu, X.Q. Major parasitic diseases of poverty in mainland China: Perspectives for better control. Infect. Dis. Poverty 2016, 5, 67. [Google Scholar] [CrossRef] [PubMed]
- Matsangos, M.; Ziaka, L.; Exadaktylos, A.K.; Klukowska-Rotzler, J.; Ziaka, M. Health Status of Afghan Refugees in Europe: Policy and Practice Implications for an Optimised Healthcare. Int. J. Environ. Res. Public Health 2022, 19, 9157. [Google Scholar] [CrossRef] [PubMed]
- Deplazes, P.; van Knapen, F.; Schweiger, A.; Overgaauw, P.A. Role of pet dogs and cats in the transmission of helminthic zoonoses in Europe, with a focus on echinococcosis and toxocarosis. Vet. Parasitol. 2011, 182, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; King, L.; Carlin, E.P. Zoonoses of people and their pets: A US perspective on significant pet-associated parasitic diseases. Trends Parasitol. 2010, 26, 153–154. [Google Scholar] [CrossRef]
- Parsons, J.C. Ascarid infections of cats and dogs. Vet. Clin. N. Am. Small Anim. Pr. 1987, 17, 1307–1339. [Google Scholar] [CrossRef]
- Nguyen, H.M.; Do, D.T.; Greiman, S.E.; Nguyen, H.V.; Hoang, H.V.; Phan, T.Q.; Pham-Duc, P.; Madsen, H. An overview of human helminthioses in Vietnam: Their prevention, control and lessons learnt. Acta Trop. 2023, 238, 106753. [Google Scholar] [CrossRef]
- Carlin, E.P.; Tyungu, D.L. Toxocara: Protecting pets and improving the lives of people. Adv. Parasitol. 2020, 109, 3–16. [Google Scholar] [CrossRef]
- Action to reduce human health hazards arising from animals. WHO Chron. 1978, 32, 307–310.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henke, K.; Ntovas, S.; Xourgia, E.; Exadaktylos, A.K.; Klukowska-Rötzler, J.; Ziaka, M. Who Let the Dogs Out? Unmasking the Neglected: A Semi-Systematic Review on the Enduring Impact of Toxocariasis, a Prevalent Zoonotic Infection. Int. J. Environ. Res. Public Health 2023, 20, 6972. https://doi.org/10.3390/ijerph20216972
Henke K, Ntovas S, Xourgia E, Exadaktylos AK, Klukowska-Rötzler J, Ziaka M. Who Let the Dogs Out? Unmasking the Neglected: A Semi-Systematic Review on the Enduring Impact of Toxocariasis, a Prevalent Zoonotic Infection. International Journal of Environmental Research and Public Health. 2023; 20(21):6972. https://doi.org/10.3390/ijerph20216972
Chicago/Turabian StyleHenke, Katrin, Sotirios Ntovas, Eleni Xourgia, Aristomenis K. Exadaktylos, Jolanta Klukowska-Rötzler, and Mairi Ziaka. 2023. "Who Let the Dogs Out? Unmasking the Neglected: A Semi-Systematic Review on the Enduring Impact of Toxocariasis, a Prevalent Zoonotic Infection" International Journal of Environmental Research and Public Health 20, no. 21: 6972. https://doi.org/10.3390/ijerph20216972