
Test–Retest Reliability, Agreement and Criterion Validity of Three Questionnaires for the Assessment of Physical Activity and Sedentary Time in Patients with Myocardial Infarction
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedure
2.3. Physical Activity and Sedentary Time Questionnaire
2.3.1. Haskell-Q
- Haskell-Q MPA: “Number of days (0–7) with moderate-intensity physical activity accumulated towards the 30-min minimum by performing bouts each lasting 10 or more minutes during the last week”.
- Haskell-Q VPA: “Number of days (0–7) performing vigorous-intensity physical activity/exercise for a minimum of 20 min”.
- Haskell-Q MPAtot (supplementary question): “Number of days (0–7) with moderate-intensity physical activity accumulated toward the 30-min minimum during the last week”.
2.3.2. BHW-Q
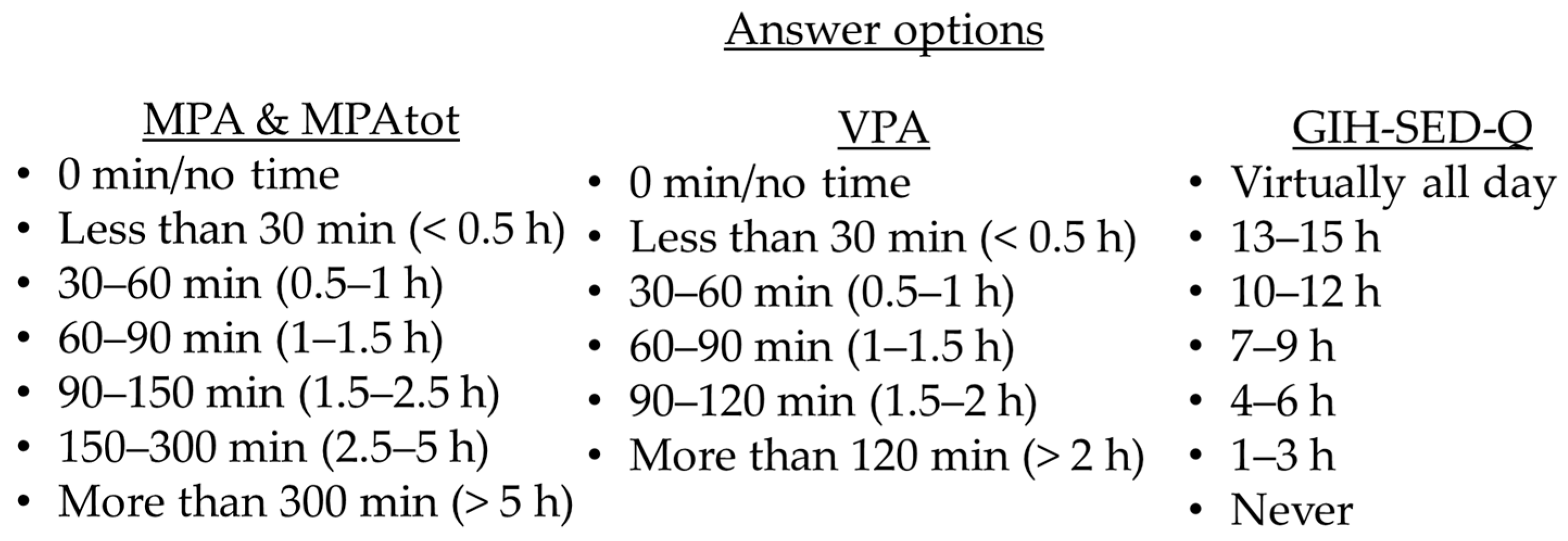
- BHW-Q VPA: “During a regular week, how much time do you spend exercising on a level that makes you short winded, for example running, fitness class, or ball games?”.
- BHW-Q MPA: “During a regular week, how much time are you physically active in ways that are not exercise, for example walks, bicycling, or gardening? Add together all activities lasting at least 10 min”.
- BHW-Q MPAtot (supplementary question): “During a regular week, how much time are you physically active in ways that are not exercise, for example walks, bicycling, or gardening? Add together all the time”.
2.3.3. GIH-SED-Q
- GIH-SED-Q sedentary time: “How much time do you sit during a usual day, excluding sleep?”.
2.4. Criterion Validity Instrument
2.5. Statistical Analyses
3. Results
3.1. Study Population
3.2. Test–Retest Reliability
3.3. Criterion Validity and Agreement
4. Discussion
Methodological Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. The Top 10 Causes of Death. Fact Sheet. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 2 March 2023).
- WHO. Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.-P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease: The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 42, 17–96. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientfic Report; U.S. Department of Health and Human Service: Washington, DC, USA, 2018. [Google Scholar]
- Ballin, M.; Nordström, P.; Niklasson, J.; Nordström, A. Associations of Objectively Measured Physical Activity and Sedentary Time with the Risk of Stroke, Myocardial Infarction or All-Cause Mortality in 70-Year-Old Men and Women: A Prospective Cohort Study. Sports Med. 2021, 51, 339–349. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, R.A.H.; Held, C.; Hadziosmanovic, N.; Armstrong, P.W.; Cannon, C.P.; Granger, C.B.; Hagström, E.; Hochman, J.S.; Koenig, W.; Lonn, E.; et al. Physical Activity and Mortality in Patients With Stable Coronary Heart Disease. J. Am. Coll. Cardiol. 2017, 70, 1689–1700. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, A.M.; Eaton, C.B.; LaMonte, M.J.; Manson, J.E.; Johnston, J.D.; Bidulescu, A.; Waring, M.E.; Manini, T.; Martin, L.W.; Stefanick, M.L.; et al. Change in Physical Activity and Sitting Time After Myocardial Infarction and Mortality Among Postmenopausal Women in the Women’s Health Initiative-Observational Study. J. Am. Heart Assoc. 2017, 6, e005354. [Google Scholar] [CrossRef]
- Ek, A.; Kallings, L.V.; Ekström, M.; Börjesson, M.; Ekblom, Ö. Subjective reports of physical activity levels and sedentary time prior to hospital admission can predict utilization of hospital care and all-cause mortality among patients with cardiovascular disease. Eur. J. Cardiovasc. Nurs. 2020, 19, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Washburn, R.A.; Schoeller, D.A. Measurement of Physical Activity. Quest 2001, 53, 295–309. [Google Scholar] [CrossRef]
- Brodin, N.; Swardh, E.; Biguet, G.; Opava, C.H. Understanding how to determine the intensity of physical activity--an interview study among individuals with rheumatoid arthritis. Disabil. Rehabil. 2009, 31, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Plasqui, G.; Westerterp, K.R. Physical activity assessment with accelerometers: An evaluation against doubly labeled water. Obesity 2007, 15, 2371–2379. [Google Scholar] [CrossRef]
- Van Remoortel, H.; Giavedoni, S.; Raste, Y.; Burtin, C.; Louvaris, Z.; Gimeno-Santos, E.; Langer, D.; Glendenning, A.; Hopkinson, N.S.; Vogiatzis, I.; et al. Validity of activity monitors in health and chronic disease: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 84. [Google Scholar] [CrossRef] [Green Version]
- Terwee, C.B.; Mokkink, L.B.; van Poppel, M.N.; Chinapaw, M.J.; van Mechelen, W.; de Vet, H.C. Qualitative attributes and measurement properties of physical activity questionnaires: A checklist. Sports Med. 2010, 40, 525–537. [Google Scholar] [CrossRef] [PubMed]
- Bäck, M.; Leosdottir, M.; Hagström, E.; Norhammar, A.; Hag, E.; Jernberg, T.; Wallentin, L.; Lindahl, B.; Hambraeus, K. The SWEDEHEART secondary prevention and cardiac rehabilitation registry (SWEDEHEART CR registry). Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health: Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, S.J.; Ekblom, O.; Andersson, E.; Borjesson, M.; Kallings, L.V. Categorical answer modes provide superior validity to open answers when asking for level of physical activity: A cross-sectional study. Scand. J. Public Health 2016, 44, 70–76. [Google Scholar] [CrossRef]
- Kallings, L.V.; Olsson, S.J.G.; Ekblom, Ö.; Ekblom-Bak, E.; Börjesson, M. The SED-GIH: A Single-Item Question for Assessment of Stationary Behavior-A Study of Concurrent and Convergent Validity. Int. J. Environ. Res. Public Health 2019, 16, 4766. [Google Scholar] [CrossRef] [Green Version]
- Larsson, K.; Kallings, L.V.; Ekblom, Ö.; Blom, V.; Andersson, E.; Ekblom, M.M. Criterion validity and test-retest reliability of SED-GIH, a single item question for assessment of daily sitting time. BMC Public Health 2019, 19, 17. [Google Scholar] [CrossRef] [Green Version]
- Lönn, A.; Kallings, L.V.; Börjesson, M.; Ekblom, Ö.; Ekström, M. Convergent validity of commonly used questions assessing physical activity and sedentary time in Swedish patients after myocardial infarction. BMC Sports Sci. Med. Rehabil. 2022, 14, 117. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport. 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Chan, Y.H. Biostatistics 104: Correlational analysis. Singap. Med. J. 2003, 44, 614–619. [Google Scholar]
- Freene, N.; McManus, M.; Mair, T.; Tan, R.; Davey, R. Objectively Measured Changes in Physical Activity and Sedentary Behavior in Cardiac Rehabilitation: A PROSPECTIVE COHORT STUDY. J. Cardiopulm. Rehabil. Prev. 2018, 38, E5–E8. [Google Scholar] [CrossRef] [PubMed]
- Dowd, K.P.; Szeklicki, R.; Minetto, M.A.; Murphy, M.H.; Polito, A.; Ghigo, E.; van der Ploeg, H.; Ekelund, U.; Maciaszek, J.; Stemplewski, R.; et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 15. [Google Scholar] [CrossRef]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Alter, D.A. A prospective study examining the influence of cardiac rehabilitation on the sedentary time of highly sedentary, physically inactive patients. Ann. Phys. Rehabil. Med. 2018, 61, 207–214. [Google Scholar] [CrossRef]
- Kambič, T.; Sarabon, N.; Hadzic, V.; Lainscak, M. Objectively Measured Physical Activity in Patients with Coronary Artery Disease: A Cross-Validation Study. Biosensors 2021, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Orrell, A.; Doherty, P.; Coulton, S.; Miles, J.; Stamatakis, E.; Lewin, R. Failure to validate the Health Survey for England physical activity module in a cardiac population. Health Policy 2007, 84, 262–268. [Google Scholar] [CrossRef]
- Freene, N.; McManus, M.; Mair, T.; Tan, R.; Clark, B.; Davey, R. Validity of the Past-day Adults’ Sedentary Time Questionnaire in a Cardiac Rehabilitation Population. J. Cardiopulm. Rehabil. Prev. 2020, 40, 325–329. [Google Scholar] [CrossRef]
- Gardner, B.; Flint, S.; Rebar, A.L.; Dewitt, S.; Quail, S.K.; Whall, H.; Smith, L. Is sitting invisible? Exploring how people mentally represent sitting. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 85. [Google Scholar] [CrossRef] [PubMed]
- Bakker, E.A.; Hartman, Y.A.W.; Hopman, M.T.E.; Hopkins, N.D.; Graves, L.E.F.; Dunstan, D.W.; Healy, G.N.; Eijsvogels, T.M.H.; Thijssen, D.H.J. Validity and reliability of subjective methods to assess sedentary behaviour in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 75. [Google Scholar] [CrossRef]
- SWEDEHEART. SWEDEHEART Annual Report 2021. 2022. Available online: https://www.ucr.uu.se/swedeheart/dokument-sh/arsrapporter-sh/1-swedeheart-annual-report-2021-english/viewdocument/3384 (accessed on 25 July 2023).
- Hagströmer, M.; Ainsworth, B.E.; Kwak, L.; Bowles, H.R. A checklist for evaluating the methodological quality of validation studies on self-report instruments for physical activity and sedentary behavior. J. Phys. Act. Health 2012, 9, S29–S36. [Google Scholar] [CrossRef] [PubMed]
- Welk, G. Physical Activity Assessments for Health-Related Research; Human Kinetics: Champaign, IL, USA, 2002. [Google Scholar]
- FAO; WHO; UNU. Human energy requirements: Report of a joint FAO/WHO/UNU Expert Consultation. Food Nutr. Bull. 2005, 26, 166. [Google Scholar]
- Prince, S.A.; Blanchard, C.M.; Grace, S.L.; Reid, R.D. Objectively-measured sedentary time and its association with markers of cardiometabolic health and fitness among cardiac rehabilitation graduates. Eur. J. Prev. Cardiol. 2016, 23, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.J.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski, K.; Rhodes, R.; Naylor, P.J.; Tuokko, H.; MacDonald, S. Direct and indirect measurement of physical activity in older adults: A systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 148. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.; Green, A.; Hall, H.; Yoward, S. Criterion validity of an ankle or waist mounted Actigraph GT3X accelerometer in measurement of body position and step count. Physiotherapy 2016, 102, e79–e80. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Gender, female, n (%) | 15 (26) |
| Age, years, mean (SD) | 66 (9.2) |
| Age, years, median (IQR) | 69 (60, 72) |
| Height, cm (SD) | 175 (10) |
| Weight, kg (SD) | 84 (15.4) |
| BMI, kg/m2 (SD) | 27.6 (5.3) |
| Current smoking | 5 (9) |
| Previous smoker > 1 month | 23 (41) |
| DM | 4 (7) |
| Hypertension | 23 (40) |
| Previous MI | 8 (14) |
| Heart failure | 5 (9) |
| Angina pectoris | 4 (7) |
| Atrial fibrillation | 4 (7) |
| Disease in the musculoskeletal system | 6 (11) |
| Other | 13 (23) |
| Variable | Test 1 | Test 2 |
|---|---|---|
| Haskell-Q MPA (days/w) | 5 (4–7) | 5 (3–7) |
| Haskell-Q VPA (days/w) | 1 (0–3) | 2 (1–5) |
| Haskell-Q MPAtot * (days/w) | 5 (3–7) | 5 (2–6) |
| BHW-Q VPA (min/w) | 45 (0–105) | 45 (0–105) |
| BHW-Q MPA (min/w) | 225 (75–300) | 225 (45–300) |
| BHW-Q MPAtot * (min/w) | 225 (120–300) | 225 (120–300) |
| GIH-SED-Q (hours/day) | 5 (5–8) | 5 (5–8) |
| BHW activity minutes ** | 300 (143–435) | 285 (139–386) |
| BHW activity minutes *** | 300 (188–435) | 300 (225–450) |
| Variable | Mean (SD) | Median (IQR) |
|---|---|---|
| Total wear time (min/day) | 845 (66) | 847 (794–878) |
| VM CPM | 558 (201) | 512 (408–681) |
| LPA (min/w) | 2238 (583) | 2303 (1873–2605) |
| MPA (min/w) | 301 (191) | 256 (135–402) |
| VPA (min/w) | 21 (56) | 1 (0–10) |
| MVPA ≥ 10 min bouts (min/w) | 162 (178) | 115 (18–237) |
| Accelerometer activity minutes 1 | 342 (248) | 299 (143–464) |
| Accelerometer activity minutes 2 | 204 (253) | 143 (25–288) |
| SED (min/day) | 479 (88) | 486 (43–543) |
| Question | n | Kappa (95% CI) | p (k) | Spearman’s rho | p (rho) |
|---|---|---|---|---|---|
| Haskell-Q MPA | 56 | 0.434 (0.284–0.585) | <0.001 | 0.573 * | <0.001 |
| Haskell-Q VPA | 56 | 0.317 (0.152–0.482) | <0.001 | 0.409 * | 0.002 |
| Haskell-Q MPAtot 1 | 55 | 0.375 (0.220–0.530) | <0.001 | 0.532 * | <0.001 |
| BHW-Q VPA | 56 | 0.521 (0.359–0.684) | <0.001 | 0.633 * | <0.001 |
| BHW-Q MPA | 56 | 0.295 (0.104–0.485) | 0.007 | 0.345 * | 0.009 |
| BHW-Q MPAtot 1 | 55 | 0.337 (0.139–0.535) | <0.001 | 0.383 * | 0.004 |
| BHW activity minutes 2 | 55 | 0.354 (0.197–0.512) | <0.001 | 0.542 * | <0.001 |
| BHW activity minutes 3 | 54 | 0.422 (0.268–0.575) | <0.001 | 0.619 * | <0.001 |
| GIH-SED-Q | 57 | 0.535 (0.360–0.711) | <0.001 | 0.602 * | <0.001 |
| Question | n | Kappa (95% CI) | p (k) | Spearman’s rho | p (rho) |
|---|---|---|---|---|---|
| Haskell-Q MPA | 56 | 0.129 (−0.029–0.251) | 0.029 | 0.407 * | 0.002 |
| Haskell-Q VPA | 57 | 0.047 (−0.015–0.109) | 0.146 | 0.139 | 0.301 |
| Haskell-Q MPAtot 1 | 55 | 0.218 (0.038–0.398) | 0.013 | 0.282 ** | 0.037 |
| BHW-Q VPA | 56 | 0.080 (−0.073–0.234) | 0.243 | 0.256 | 0.057 |
| BHW-Q MPA | 56 | 0.341 (0.185–0.496) | <0.001 | 0.578 * | <0.001 |
| BHW-Q MPAtot 1 | 55 | 0.237 (0.099–0.376) | <0.001 | 0.501 * | <0.001 |
| Activity minutes 2 | 56 | 0.276 (0.141–0.411) | <0.001 | 0.429 * | <0.001 |
| Activity minutes 3 | 54 | 0.254 (0.086–0.421) | 0.002 | 0.385 * | 0.004 |
| GIH-SED-Q | 57 | 0.116 (−0.022–0.254) | 0.061 | 0.291 ** | 0.028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bargholtz, M.; Brosved, M.; Heimburg, K.; Hellmark, M.; Leosdottir, M.; Hagströmer, M.; Bäck, M. Test–Retest Reliability, Agreement and Criterion Validity of Three Questionnaires for the Assessment of Physical Activity and Sedentary Time in Patients with Myocardial Infarction. Int. J. Environ. Res. Public Health 2023, 20, 6579. https://doi.org/10.3390/ijerph20166579
Bargholtz M, Brosved M, Heimburg K, Hellmark M, Leosdottir M, Hagströmer M, Bäck M. Test–Retest Reliability, Agreement and Criterion Validity of Three Questionnaires for the Assessment of Physical Activity and Sedentary Time in Patients with Myocardial Infarction. International Journal of Environmental Research and Public Health. 2023; 20(16):6579. https://doi.org/10.3390/ijerph20166579
Chicago/Turabian StyleBargholtz, Marcus, Madeleine Brosved, Katarina Heimburg, Marie Hellmark, Margret Leosdottir, Maria Hagströmer, and Maria Bäck. 2023. "Test–Retest Reliability, Agreement and Criterion Validity of Three Questionnaires for the Assessment of Physical Activity and Sedentary Time in Patients with Myocardial Infarction" International Journal of Environmental Research and Public Health 20, no. 16: 6579. https://doi.org/10.3390/ijerph20166579