
Measuring the Impact of Bedroom Privacy on Social Networks in a Long-Term Care Facility for Hong Kong Older Adults: A Spatio-Social Network Analysis Approach

Abstract
:1. Introduction
1.1. Bedroom Privacy
1.2. Social Life in LTC Facilities
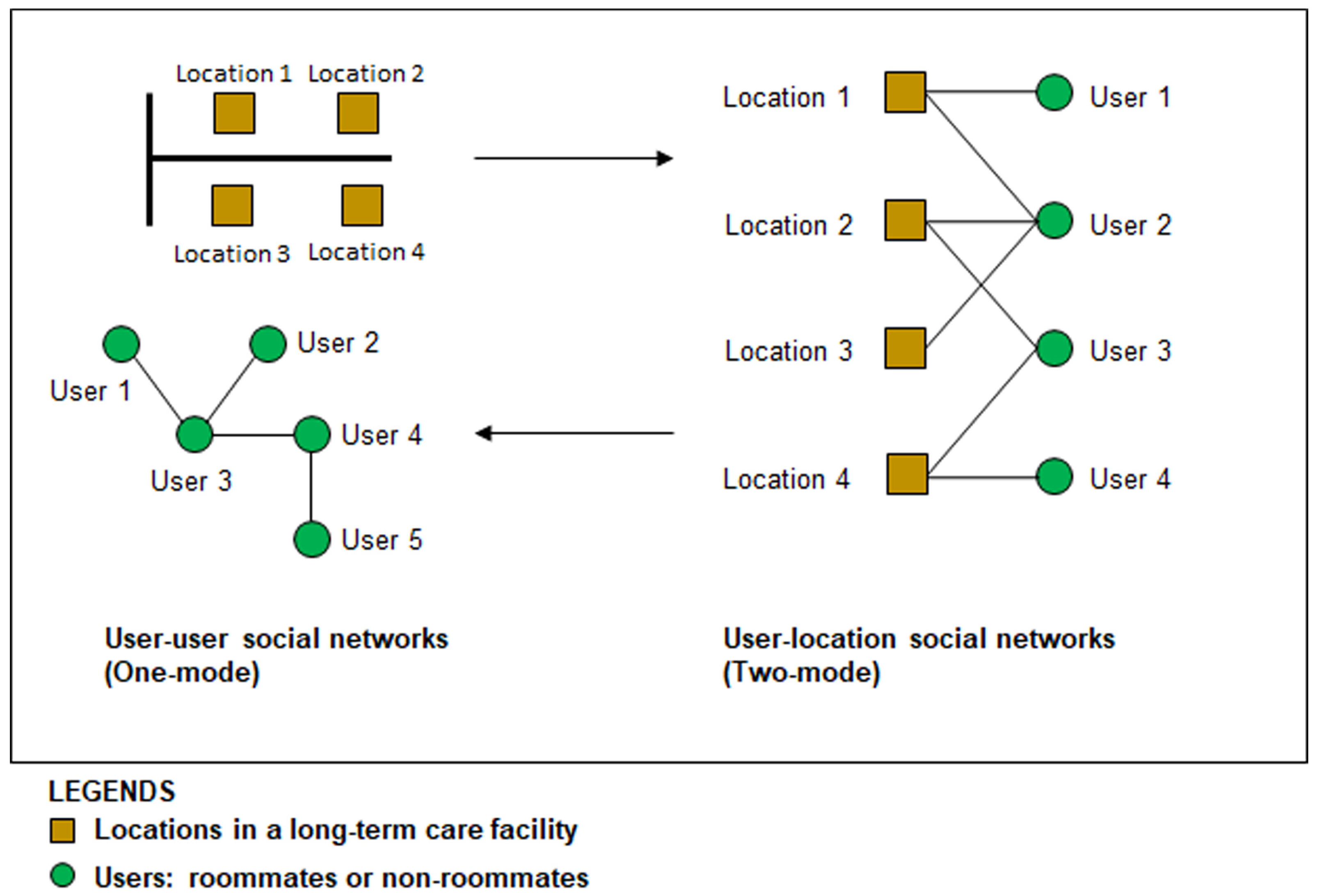
1.3. A Spatio-Social Network Analysis Approach
2. Materials and Methods
2.1. Settings
2.2. Assessing Bedroom Privacy
2.3. Measuring Social Networks
2.4. Data Collection
2.5. Analysis
3. Results
3.1. Bedroom Privacy
3.2. Feasibility of the Spatio-Social Network Analysis Approach
3.3. Residents’ Social Networks
3.3.1. Social Network Structure
3.3.2. Social Network Types
3.4. The Associations between Bedroom Privacy and Social Life
4. Discussion
4.1. Bedroom Occupancy
4.2. Visual Privacy
4.3. Visibility
4.4. Bedroom Adjacency
4.5. Transitional Spaces
5. Conclusions
6. Future Areas of Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campo, M.; Chaudhury, H. Informal Social Interaction among Residents with Dementia in Special Care Units: Exploring the Role of the Physical and Social Environments. Dementia 2012, 11, 401–423. [Google Scholar] [CrossRef]
- Ferdous, F.; Diaz Moore, K. Field Observations into the Environmental Soul: Spatial Configuration and Social Life for People Experiencing Dementia. Am. J. Alzheimer’s Dis. Other Dement. 2015, 30, 209–218. [Google Scholar] [CrossRef]
- Jang, M. The Relationship between Spatial Characteristics and Social Interaction of Older Adults with Dementia in Nursing Homes. J. Asian Archit. Build. Eng. 2023, 22, 175–187. [Google Scholar] [CrossRef]
- Kane, R.A. Long-Term Care and a Good Quality of Life: Bringing Them Closer Together. Gerontologist 2001, 41, 293–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regnier, V. Design for Assisted Living: Guidelines for Housing the Physically and Mentally Frail, 1st ed.; John Wiley & Sons: Hoboken, NJ, USA, 2002. [Google Scholar]
- Zeisel, J.; Silverstein, N.M.; Hyde, J.; Levkoff, S.; Lawton, M.P.; Holmes, W. Environmental Correlates to Behavioral Health Outcomes in Alzheimer’s Special Care Units. Gerontologist 2003, 43, 697–711. [Google Scholar] [CrossRef] [Green Version]
- Calkins, M.; Cassella, C. Exploring the Cost and Value of Private versus Shared Bedrooms in Nursing Homes. Gerontologist 2007, 47, 169–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, M.P.; Bader, J. Wish for Privacy by Young and Old. J. Gerontol. 1970, 25, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Altman, I. The Environment and Social Behavior: Privacy, Personal Space, Territory, and Crowding; Brooks/Cole Publishing Company: Monterey, CA, USA, 1975. [Google Scholar]
- Tao, Y.; Lau, S.S.Y.; Gou, Z.; Fu, J.; Jiang, B.; Chen, X. Privacy and Well-Being in Aged Care Facilities with a Crowded Living Environment: Case Study of Hong Kong Care and Attention Homes. Int. J. Environ. Res. Public Health 2018, 15, 2157. [Google Scholar] [CrossRef] [Green Version]
- Chaudhury, H.; Mahmood, A.; Valente, M. Advantages and Disadvantages of Single-Versus Multiple-Occupancy Rooms in Acute Care Environments: A Review and Analysis of the Literature. Environ. Behav. 2005, 37, 760–786. [Google Scholar] [CrossRef]
- Abbott, K.M.; Bettger, J.P.; Hampton, K.; Kohler, H.-P. Exploring the Use of Social Network Analysis to Measure Social Integration among Older Adults in Assisted Living. Fam. Community Health 2012, 35, 322–333. [Google Scholar] [CrossRef]
- Lee, D.T.F.; Woo, J.; Mackenzie, A.E. The Cultural Context of Adjusting to Nursing Home Life: Chinese Elders’ Perspectives. Gerontologist 2002, 42, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Low, L.P.L.; Lee, D.T.F.; Chan, A.W.Y. An Exploratory Study of Chinese Older People’s Perceptions of Privacy in Residential Care Homes. J. Adv. Nurs. 2007, 57, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.M.; Robinson, J.C. Social Network Analysis: Presenting an Underused Method for Nursing Research. J. Adv. Nurs. 2018, 74, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.-T. The Social Networks of Nursing-Home Residents in Hong Kong. Ageing Soc. 2009, 29, 163–178. [Google Scholar] [CrossRef]
- Abbott, K.M.; Pachucki, M.C. Associations between Social Network Characteristics, Cognitive Function, and Quality of Life among Residents in a Dementia Special Care Unit: A Pilot Study. Dementia 2017, 16, 1004–1019. [Google Scholar] [CrossRef]
- Casey, A.-N.S.; Low, L.-F.; Jeon, Y.-H.; Brodaty, H. Residents Perceptions of Friendship and Positive Social Networks within a Nursing Home. Gerontologist 2016, 56, 855–867. [Google Scholar] [CrossRef] [Green Version]
- Willcocks, D.; Peace, S.; Kellaher, L. Private Lives in Public Places; Routledge: Abingdon, UK, 1987. [Google Scholar] [CrossRef] [Green Version]
- Applegate, M.; Morse, J.M. Personal Privacy and Interactional Patterns in a Nursing Home. J. Aging Stud. 1994, 8, 413–434. [Google Scholar] [CrossRef]
- Bland, R. Independence, Privacy and Risk: Two Contrasting Approaches to Residential Care for Older People. Ageing Soc. 1999, 19, 539–560. [Google Scholar] [CrossRef] [Green Version]
- Choi, N.G.; Ransom, S.; Wyllie, R.J. Depression in Older Nursing Home Residents: The Influence of Nursing Home Environmental Stressors, Coping, and Acceptance of Group and Individual Therapy. Aging Ment. Health 2008, 12, 536–547. [Google Scholar] [CrossRef]
- Lu, Y.; Cai, H.; Bosch, S.J. Key Spatial Factors Influencing the Perceived Privacy in Nursing Units: An Exploration Study with Eight Nursing Units in Hong Kong. HERD Health Environ. Res. Des. J. 2017, 10, 37–48. [Google Scholar] [CrossRef]
- Barnes, S. The Design of Caring Environments and the Quality of Life of Older People. Ageing Soc. 2002, 22, 775–789. [Google Scholar] [CrossRef] [Green Version]
- Cohen, U.; Weisman, J. Holding on to Home: Designing Environments for People with Dementia; Johns Hopkins University Press: Baltimore, MD, USA, 1991. [Google Scholar]
- Zeisel, J. I’m Still Here: A New Philosophy of Alzheimer’s Care; Penguin: London, UK, 2009. [Google Scholar]
- Koncelik, J. Designing the Open Nursing Home; Dowden, Hutchinson & Ross: Stroudsburg, PA, USA, 1976; Volume 27. [Google Scholar]
- Schwarz, B.; Chaudhury, H.; Tofle, R.B. Effect of Design Interventions on a Dementia Care Setting. Am. J. Alzheimers Dis. Other Dement. 2004, 19, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Fleming, R.; Bennett, K. The Environmental Audit Tool Handbook; University of Wollongong: Wollongong, NSW, Australia, 2017; p. 76. [Google Scholar]
- Parker, C.; Barnes, S.; Mckee, K.; Morgan, K.; Torrington, J.; Tregenza, P. Quality of Life and Building Design in Residential and Nursing Homes for Older People. Ageing Soc. 2004, 24, 941–962. [Google Scholar] [CrossRef] [Green Version]
- Sloane, P.; Mitchell, C.; Weisman, G.D.; Zimmerman, S.; Foley, K.M.L.; Lynn, M.; Calkins, M.P.; Lawton, M.P.; Terei, J.; Grant, L.; et al. Therapeutic Environment Screening Survey for Nursing Homes (TESS-NH). J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, S69–S78. [Google Scholar] [CrossRef] [Green Version]
- Chaudhury, H.; Hung, L.; Rust, T.; Wu, S. Do Physical Environmental Changes Make a Difference? Supporting Person-Centered Care at Mealtimes in Nursing Homes. Dementia 2016, 16, 878–896. [Google Scholar] [CrossRef] [PubMed]
- Xuan, X.; Li, Z.; Chen, X. An Empirical Examination of Nursing Units in China Based on Nurse Experience. HERD Health Environ. Res. Des. J. 2019, 12, 108–123. [Google Scholar] [CrossRef]
- Cummings, S.M. Predictors of Psychological Well-Being among Assisted-Living Residents. Health Soc. Work 2002, 27, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.M.; Kemp, B.J. Quality of Life in Assisted Living Homes: A Multidimensional Analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2000, 55, P117–P127. [Google Scholar] [CrossRef] [Green Version]
- Yang, A.C.H.; Lau, N.; Ho, J.C.F. The Role of Bedroom Privacy in Social Interaction among Elderly Residents in Nursing Homes: An Exploratory Case Study of Hong Kong. Sensors 2020, 20, 4101. [Google Scholar] [CrossRef]
- Rahmatikargar, B.; Zadeh, P.M.; Kobti, Z. Social Isolation Detection in Palliative Care Using Social Network Analysis. In Proceedings of the 2022 22nd IEEE International Symposium on Cluster, Cloud and Internet Computing (CCGrid), Taormina, Italy, 16–19 May 2022; pp. 905–912. [Google Scholar] [CrossRef]
- Kermani, M.A.M.A.; Sani, S.A.; Zand, H. Resident’s Alzheimer Disease and Social Networks within a Nursing Home. In Complex Networks & Their Applications IX; Benito, R.M., Cherifi, C., Cherifi, H., Moro, E., Rocha, L.M., Sales-Pardo, M., Eds.; Studies in Computational Intelligence; Springer International Publishing: Cham, Switzerland, 2021; pp. 335–345. [Google Scholar] [CrossRef]
- Kang, B.; Scales, K.; McConnell, E.S.; Song, Y.; Lepore, M.; Corazzini, K. Nursing Home Residents’ Perspectives on Their Social Relationships. J. Clin. Nurs. 2020, 29, 1162–1174. [Google Scholar] [CrossRef]
- Park, N.S. The Relationship of Social Engagement to Psychological Well-Being of Older Adults in Assisted Living Facilities. J. Appl. Gerontol. 2009, 28, 461–481. [Google Scholar] [CrossRef]
- Street, D.; Burge, S.; Quadagno, J.; Barrett, A. The Salience of Social Relationships for Resident Well-Being in Assisted Living. J. Gerontol. B Psychol. Sci. Soc. Sci. 2007, 62, S129–S134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.-T.; Lee, C.K.L.; Chan, A.C.M.; Leung, E.M.F.; Lee, J.-J. Social Network Types and Subjective Well-Being in Chinese Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64B, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Harasemiw, O.; Newall, N.; Shooshtari, S.; Mackenzie, C.; Menec, V. From Social Integration to Social Isolation: The Relationship between Social Network Types and Perceived Availability of Social Support in a National Sample of Older Canadians. Res. Aging 2017, 40, 715–739. [Google Scholar] [CrossRef] [PubMed]
- Wenger, G.C. Social Networks and Gerontology. Rev. Clin. Gerontol. 1996, 6, 285–293. [Google Scholar] [CrossRef]
- Fiori, K.L.; Antonucci, T.C.; Cortina, K.S. Social Network Typologies and Mental Health among Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, P25–P32. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhang, Y. Social Network Types and the Health of Older Adults: Exploring Reciprocal Associations. Soc. Sci. Med. 2015, 130, 59–68. [Google Scholar] [CrossRef]
- Ye, X.; Liu, X. Integrating Social Networks and Spatial Analyses of the Built Environment. Environ. Plan. B Urban Anal. City Sci. 2018, 45, 395–399. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Wang, Y. Measuring Segregation between Rural Migrants and Local Residents in Urban China: An Integrated Spatio-Social Network Analysis of Kecun in Guangzhou. Environ. Plan. B Urban Anal. City Sci. 2018, 45, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Wasserman, S.; Faust, K. Social Network Analysis: Methods and Application; Cambridge University Press: New York, NY, USA, 1994. [Google Scholar]
- Calkins, M.P. Evidence-Based Long Term Care Design. NeuroRehabilitation 2009, 25, 145–154. [Google Scholar] [CrossRef]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From Social Integration to Health: Durkheim in the New Millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef]
- Helleringer, S.; Kohler, H.; Kalilani-Phiri, L.; Mkandawire, J.; Armbruster, B. The Reliability of Sexual Partnership Histories: Implications for the Measurement of Partnership Concurrency during Survey. AIDS 2011, 25, 503–511. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.; Christakas, N. Social Networks and Health. Annu. Rev. Sociol. 2008, 34, 405–429. [Google Scholar] [CrossRef] [Green Version]
- Capriglione, D.; Casinelli, D.; Ferrigno, L. Use of Frequency Diversity to Improve the Performance of RSSI-Based Distance Measurements. In Proceedings of the 2015 IEEE International Workshop on Measurements Networking (M N), Coimbra, Portugal, 12–13 October 2015; pp. 1–6. [Google Scholar] [CrossRef]
- Montanari, A.; Nawaz, S.; Mascolo, C.; Sailer, K. A Study of Bluetooth Low Energy Performance for Human Proximity Detection in the Workplace. In Proceedings of the 2017 IEEE International Conference on Pervasive Computing and Communications (PerCom), Kona, HI, USA, 13–17 March 2017; pp. 90–99. [Google Scholar] [CrossRef] [Green Version]
- Borgatti, S.P.; Everett, M.G.; Freeman, L.C. Ucinet 6 for Windows: Software for Social Network Analysis; Analytic Technologies: Harvard, MA, USA, 2002. [Google Scholar]
- Foltz-Gray, D. Intimate Strangers. When Roommates Clash, Caregivers Can Ease the Tension--or Make It Worse. Contemp. Longterm. Care 1995, 18, 34–37. [Google Scholar]
- Harris, P.B.; McBride, G.; Ross, C.; Curtis, L. A Place to Heal: Environmental Sources of Satisfaction among Hospital Patients1. J. Appl. Soc. Psychol. 2002, 32, 1276–1299. [Google Scholar] [CrossRef]
- Kane, R.A.; Baker, M.O.; Salmon, J.; Veazie, W. Consumer Perspectives on Private versus Shared Accommodations in Assisted Living Settings; American Association of Retired Persons: Washington, DC, USA, 1998; p. 65. [Google Scholar]
- Ulrich, R.; Quan, X.; Zimring, C.; Joseph, A.; Choudbary, R. The Role of the Physical Environment in the Hospital of the 21st Century: A Once-in-a-Lifetime Opportunity; The Center for Health Design: Concord, CA, USA, 2004; p. 69. [Google Scholar]
- Johnson, C.A. Privacy as Personal Control. Man-Environ. Interact. Eval. Appl. Part 1974, 2, 83–100. [Google Scholar]
- Calkins, M.P. From Research to Application: Supportive and Therapeutic Environments for People Living with Dementia. Gerontologist 2018, 58 (Suppl. 1), S114–S128. [Google Scholar] [CrossRef]
- Haywood, A.; Barnes, S.; Marsh, H.; Parker, S.G. Does the Design of Settings Where Acute Care Is Delivered Meet the Needs of Older People? Perspectives of Patients, Family Carers, and Staff. HERD Health Environ. Res. Des. J. 2018, 11, 177–188. [Google Scholar] [CrossRef] [Green Version]
- Lawton, M.P.; Fulcomer, M.; Kleban, M.H. Architecture for the Mentally Impaired Elderly. Environ. Behav. 1984, 16, 730–757. [Google Scholar] [CrossRef]
- Lee, J.H.; Ostwald, M.J.; Lee, H. Measuring the Spatial and Social Characteristics of the Architectural Plans of Aged Care Facilities. Front. Archit. Res. 2017, 6, 431–441. [Google Scholar] [CrossRef]
- Kane, R.A.; Lum, T.Y.; Cutler, L.J.; Degenholtz, H.B.; Yu, T.-C. Resident Outcomes in Small-House Nursing Homes: A Longitudinal Evaluation of the Initial Green House Program. J. Am. Geriatr. Soc. 2007, 55, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, K.; Nakashima, T.; Nakanishi, M. Provision of Individualized Care and Built Environment of Nursing Homes in Japan. Arch. Gerontol. Geriatr. 2013, 56, 416–424. [Google Scholar] [CrossRef] [PubMed]
- te Boekhorst, S.; Depla, M.F.I.A.; de Lange, J.; Pot, A.M.; Eefsting, J.A. The Effects of Group Living Homes on Older People with Dementia: A Comparison with Traditional Nursing Home Care. Int. J. Geriatr. Psychiatry 2009, 24, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, H.; Zwakhalen, S.M.G.; van Rossum, E.; Ambergen, T.; Kempen, G.I.J.M.; Hamers, J.P.H. Dementia Care Redesigned: Effects of Small-Scale Living Facilities on Residents, Their Family Caregivers, and Staff. J. Am. Med. Dir. Assoc. 2010, 11, 662–670. [Google Scholar] [CrossRef]
- Anderson, D.C.; Grey, T.; Kennelly, S.; O’Neill, D. Nursing Home Design and COVID-19: Balancing Infection Control, Quality of Life, and Resilience. J. Am. Med. Dir. Assoc. 2020, 21, 1519–1524. [Google Scholar] [CrossRef]
- Granger, W. Viewing, Watching, Observing: Aging and the Architecture of Intermediate Space. PLATFORM. 2020. Available online: https://www.platformspace.net/home/viewing-watching-observing-aging-and-the-architecture-of-intermediate-space (accessed on 28 November 2022).
- Legislative Council. Residential Care Homes Legislation (Miscellaneous Amendments) Bill 2022. 2022. Available online: https://www.legco.gov.hk/yr2022/english/brief/lwbcr150931722_20220511-e.pdf (accessed on 7 February 2023).
- Leung. Hong Kong Welfare Minister Warns Low-Quality Care Homes Could Be Replaced. South China Morning Post. Hong Kong, 15 May 2022. Available online: https://www.scmp.com/news/hong-kong/society/article/3177852/hong-kong-welfare-minister-warns-low-quality-care-homes (accessed on 7 February 2023).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Geometrical Indicators | References |
|---|---|---|
| Bedroom occupancy | How many people share the bedroom? (Five or more = 0; Four = 1; Three = 2; Two or less = 3) | [24,50] |
| Bedroom adjacency | What type of space is the bedroom next to? (Public space = 0; Semi-public space = 1; Semi-private space = 2; Private space = 3) | [26,27] |
| Transitional spaces | How many transitional spaces between the bedroom and common area? (None = 0; One = 1; Two = 2; Three or more = 3) | [1,28,29] |
| Visibility | Can residents see the common areas? (Yes = 0; No = 1) | [30,31] |
| Visual privacy | Can residents’ beds be seen from the common areas? (Yes = 0; No = 1) | [4,32] |
| Three-Bedroom | Four-Bedroom (Corridor) | Four-Bedroom (Common) | Five-Bedroom | Total | |
|---|---|---|---|---|---|
| % of sample | 14.58% | 37.50% | 31.25% | 16.66% | 100% |
| Gender | |||||
| Male | 1 | 11 | 9 | 3 | 24 |
| Female | 6 | 7 | 6 | 5 | 24 |
| Total | 7 | 18 | 15 | 8 | 48 |
| Architectural Factor | Three-Bedroom | Four-Bedroom (Corridor) | Four-Bedroom (Common) | Five-Bedroom |
|---|---|---|---|---|
| Bedroom occupancy | 2 | 1 | 1 | 0 |
| Bedroom adjacency | 2 | 1 | 0 | 1 |
| Transitional spaces | 2 | 1 | 0 | 2 |
| Visual privacy | 1 | 1 | 0 | 1 |
| Visibility | 0 | 1 | 1 | 0 |
| Total | 7 | 5 | 2 | 4 |
| Residents of | Number of Network Partners | Frequency of Interaction | Degree Centrality |
|---|---|---|---|
| Three-bedroom | 1.10 | 2.86 | 0.07 |
| Four-bedroom (common) | 2.43 | 4.60 | 0.04 |
| Four-bedroom (corridor) | 1.85 | 4.44 | 0.23 |
| Five-bedroom | 2.79 | 2.75 | 0.06 |
| Mean | 2.08 | 3.98 | 0.12 |
| Cluster | Cluster 1. Diverse (Common Area) | Cluster 2. Diverse (Bedroom) | Cluster 3. Non-Roommate-Focused (Common Area) | Cluster 4. Roommate-Focused (Bedroom) | Cluster 5. Restricted (Bedroom) | Mean |
|---|---|---|---|---|---|---|
| Of sample | 10.42% | 20.83% | 22.92% | 29.17% | 16.67% | |
| Gender | ||||||
| Male | 90.00% | 60.00% | 18.18% | 57.14% | 25.00% | |
| Female | 10.00% | 40.00% | 81.82% | 42.86% | 75.00% | |
| Mean number of network partners by location | ||||||
| Roommates in own bedrooms | 2.33 (0.21) | 2.93 (0.48) | 1.36 (0.77) | 2.59 (0.65) | 0.95 (0.44) | 2.03 |
| Non-roommates in other bedrooms | 4.80 (1.48) | 4.50 (1.72) | 4.27 (1.56) | 3.71 (0.10) | 2.88 (1.96) | 4.03 |
| Roommates in common areas | 0.68 (0.29) | 0.08 (0.07) | 0.07 (0.09) | 0.05 (0.10) | 0.01 (0.01) | 0.18 |
| Non-roommates in common areas | 1.09 (0.47) | 1.21 (0.33) | 2.08 (0.61) | 0.56 (0.41) | 0.32 (0.34) | 1.05 |
| Mean frequency of interacting with … | ||||||
| Roommates in own bedrooms | 18.60 (1.67) | 22.60 (2.46) | 11.18 (6.06) | 20.00 (2.86) | 8.75 (2.76) | 16.23 |
| Non-roommates in other bedrooms | 22.80 (9.78) | 27.80 (6.73) | 24.36 (9.56) | 17.36 (6.22) | 8.13 (5.91) | 20.09 |
| None, being away from others | 2.00 (3.94) | 2.50 (3.37) | 1.55 (1.57) | 0.50 (0.94) | 0.13 (0.35) | 1.33 |
| Roommates in common areas | 11.60 (3.65) | 1.50 (1.78) | 4.09 (3.33) | 1.00 (1.52) | 0.63 (0.74) | 3.76 |
| Non-roommates in common areas | 13.40 (4.04) | 11.20 (2.78) | 14.82 (4.29) | 5.36 (3.34) | 2.13 (2.70) | 9.38 |
| Bedroom | Three-Bedroom | Four-Bedroom (Corridor) | Four-Bedroom (Common) | Five-Bedroom | |
|---|---|---|---|---|---|
| Cluster Type | |||||
| Diverse (in common area) | 0 (0.0%) | 5 (27.8%) | 0 (0.0%) | 0 (0.0%) | |
| Diverse (in bedroom) | 0 (0.0%) | 2 (11.1%) | 7 (46.7%) | 1 (12.5%) | |
| Non-roommate-focused (in common area) | 1 (14.3%) | 6 (33.3%) | 3 (20.0%) | 1 (12.5%) | |
| Roommate-focused (in bedroom) | 2 (28.6%) | 3 (16.7%) | 5 (33.3%) | 4 (50.0%) | |
| Restricted (in bedroom) | 4 (57.1%) | 2 (11.1%) | 0 (0.0%) | 2 (25.0%) | |
| Total | 7 | 18 | 15 | 8 | |
| Dependent Variables | Overall Privacy | Bedroom Occupancy | Visual Privacy | Visibility | Bedroom Adjacency | Transitional Spaces |
|---|---|---|---|---|---|---|
| Degree centrality | −0.305 * (0.035) | 0.055 (0.709) | −0.343 * (0.017) | 0.381 ** (0.008) | −0.349 * (0.015) | −0.414 ** (0.003) |
| Number of network partners according to location | ||||||
| Roommates in bedrooms | −0.087 (0.558) | −0.498 ** (<0.001) | 0.191 (0.193) | 0.056 (0.704) | −0.087 (0.555) | 0.08 (0.587) |
| Non-roommates in bedrooms | −0.225 (0.125) | 0.045 (0.759) | −0.222 (0.13) | 0.489 ** (<0.001) | −0.304 * (0.036) | −0.404 ** (0.004) |
| Roommates in common areas | −0.321 * (0.026) | 0.027 (0.856) | −0.380 ** (0.008) | 0.169 (0.251) | −0.315 * (0.029) | −0.317 * (0.028) |
| Non-roommates in common areas | −0.173 (0.241) | 0.035 (0.812) | −0.188 (0.201) | 0.266 (0.067) | −0.209 (0.155) | −0.259 (0.075) |
| Frequency of contact with … | ||||||
| Roommates in bedrooms | 0.091 (0.54) | −0.132 (0.372) | 0.203 (0.167) | 0.102 (0.489) | 0.055 (0.711) | 0.061 (0.679) |
| Non-roommates in bedrooms | −0.252 (0.084) | −0.118 (0.423) | −0.182 (0.217) | 0.358 * (0.012) | −0.298 * (0.04) | −0.307 * (0.034) |
| Roommates in common areas | −0.241 (0.098) | 0.151 (0.304) | −0.337 * (0.019) | 0.274 (0.059) | −0.27 (0.064) | −0.351 * (0.014) |
| Non-roommates in common areas | −0.321 * (0.026) | 0.033 (0.826) | −0.345 * (0.016) | 0.402 ** (0.005) | −0.367 * (0.01) | −0.428 ** (0.002) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, A.C.H.; Chaudhury, H.; Ho, J.C.F.; Lau, N. Measuring the Impact of Bedroom Privacy on Social Networks in a Long-Term Care Facility for Hong Kong Older Adults: A Spatio-Social Network Analysis Approach. Int. J. Environ. Res. Public Health 2023, 20, 5494. https://doi.org/10.3390/ijerph20085494
Yang ACH, Chaudhury H, Ho JCF, Lau N. Measuring the Impact of Bedroom Privacy on Social Networks in a Long-Term Care Facility for Hong Kong Older Adults: A Spatio-Social Network Analysis Approach. International Journal of Environmental Research and Public Health. 2023; 20(8):5494. https://doi.org/10.3390/ijerph20085494
Chicago/Turabian StyleYang, Aria C. H., Habib Chaudhury, Jeffrey C. F. Ho, and Newman Lau. 2023. "Measuring the Impact of Bedroom Privacy on Social Networks in a Long-Term Care Facility for Hong Kong Older Adults: A Spatio-Social Network Analysis Approach" International Journal of Environmental Research and Public Health 20, no. 8: 5494. https://doi.org/10.3390/ijerph20085494