
The Impact of COVID-19 Lockdown on Adults with Major Depressive Disorder from Catalonia: A Decentralized Longitudinal Study
 , , , ,
, , , ,  , , , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
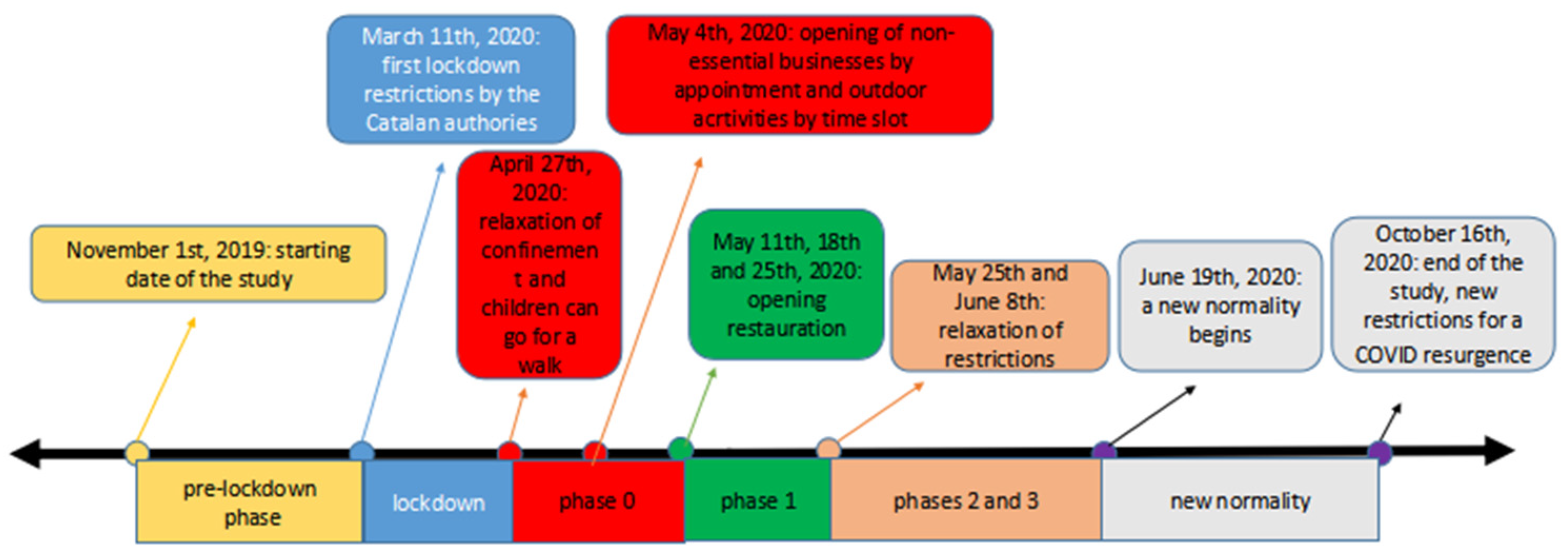
Pandemic Phases
- ▪
- Pre-lockdown (from 1 November 2019 to 10 March 2020);
- ▪
- Lockdown (from 11 March 2020 to 26 April 2020);
- ▪
- Later restrictions were lifted gradually through four phases of the post-lockdown:
- ▪
- Phase 0 (from 27 April 2020 to 10 or 17 or 24 May 2020 *);
- ▪
- Phase 1 (from 11 or 18 or 25 May 2020 to 24 May or 7 June 2020 *);
- ▪
- Phases 2 and 3 (from 25 May or 8 June 2020 to 18 June 2020 *);
- ▪
- “New-normality” (from 19 June 2020 to 16 October 2020).
3. Measures
3.1. Depression
3.2. Anxiety Symptoms
3.3. Socialdemographic Variables
4. Statistical Analysis
5. Results
6. Discussion
7. Implications and Future Directions
8. Limitations and Strengths
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aRMT | active remote measurement technology |
| GAD-7 | item Generalized anxiety disorder-7 item |
| IQR | Interquartile ranges |
| MDD | Major depressive disorder |
| ML | maximum likelihood |
| pRMT | passive remote measurement technology |
| PHQ-8 | Patient health questionnaire 8-item |
| RADAR-CNS | Remote assessment of disease and relapse—central nervous system |
| REDCap | Research electronic data capture |
| RADAR-MDD | Remote Assessment of Disease and Relapse-Major Depressive Disorder |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019|Enhanced Reader. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Huang, W.; Pan, H.; Huang, T.; Wang, X.; Ma, Y. Mental Health During the COVID-19 Outbreak in China: A Meta-Analysis. Psychiatr. Q. 2020, 91, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- RESOLUCIÓ SLT/704/2020, d’11 de Març. 2020. Available online: https://cido.diba.cat/legislacio/9956651/resolucio-slt7042020-d11-de-marc-per-la-qual-sadopten-mesures-de-distanciament-social-en-relacio-amb-els-esdeveniments-multitudinaris-per-a-la-prevencio-i-el-control-de-la-infeccio-pel-sars-cov-2-departament-de-salut (accessed on 22 April 2022).
- Jefatura de Estado. Disposición 4911, BOE n.°130. 2020. Available online: https://www.boe.es/boe/dias/2020/05/09/pdfs/BOE-A-2020-4911.pdf (accessed on 22 April 2022).
- Jefatura de Estado. Disposición 4791, BOE n.°123. 2020. Available online: https://www.boe.es/boe/dias/2020/05/03/pdfs/BOE-A-2020-4791.pdf (accessed on 22 April 2022).
- Jefatura de Estado. Disposición 7351, BOE n.°107. 2021. Available online: https://www.boe.es/boe/dias/2021/05/05/pdfs/BOE-A-2021-7351.pdf (accessed on 22 April 2022).
- Jefatura de Estado. Orden SND/399/2020, de 9 de Mayo, BOE n.°4911. 2020. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-4911 (accessed on 22 April 2022).
- LA CIUTAT Diari Digital de Proximitat El Garraf Passa a La Fase 1 Del Desconfinament. Available online: https://laciutat.cat/laciutatdelgarraf/el-garraf-passa-a-la-fase-1-del-desconfinament# (accessed on 22 April 2022).
- Ajuntament de Barcelona Www.Barcelona.Cat. Available online: https://ajuntament.barcelona.cat/premsa/2020/05/24/barcelona-a-punt-per-entrar-a-la-fase-1-de-desescalada/ (accessed on 22 April 2022).
- Ajuntament de Barcelona Www.Barcelona.Cat. Available online: https://www.barcelona.cat/infobarcelona/es/tema/informacion-sobre-la-gestion-del-covid-19/fase-2-nuevas-medidas-menos-restricciones-y-mas-actividades-2_957887.html (accessed on 22 April 2022).
- betevé Barcelona Passa a Fase 3 de La Descalada Dijous. Available online: https://beteve.cat/societat/fase-3-barcelona-desescalada/ (accessed on 22 April 2022).
- Jefatura de Estado Orden SND/414/2020, de 16 de Mayo, BOE n.°5088. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-5088 (accessed on 22 April 2022).
- SER Estos Son Los Territorios Que Pasan a La Fase 2 Del Plan de Desescalada. Available online: https://cadenaser.com/ser/2020/05/22/sociedad/1590151185_824572.html (accessed on 22 April 2022).
- SER Estos Son Los Territorios Que Pasan a La Fase 3 Del Plan de Desescalada y a La Nueva Normalidad El 15 de Junio. Available online: https://cadenaser.com/ser/2020/06/12/sociedad/1591953793_476365.html (accessed on 22 April 2022).
- RESOLUCIÓ INT/1433/2020, de 18 de Juny. 2020. Available online: https://cido.diba.cat/legislacio/10313804/resolucio-int14332020-de-18-de-juny-de-delegacio-de-determinades-facultats-derivades-de-lincompliment-de-la-normativa-reguladora-de-lestat-dalarma-departament-dinterior (accessed on 22 April 2022).
- Rubin, G.J.; Wessely, S. The Psychological Effects of Quarantining a City. BMJ 2020, 368, m313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hampshire, A.; Trender, W.; Grant, J.E.; Mirza, M.B.; Moran, R.; Hellyer, P.J.; Chamberlain, S.R. Item-Level Analysis of Mental Health Symptom Trajectories during the COVID-19 Pandemic in the UK: Associations with Age, Sex and Pre-Existing Psychiatric Conditions. Compr. Psychiatry 2022, 114, 152298. [Google Scholar] [CrossRef] [PubMed]
- Kunzler, A.M.; Röthke, N.; Günthner, L.; Stoffers-Winterling, J.; Tüscher, O.; Coenen, M.; Rehfuess, E.; Schwarzer, G.; Binder, H.; Schmucker, C.; et al. Mental Burden and Its Risk and Protective Factors during the Early Phase of the SARS-CoV-2 Pandemic: Systematic Review and Meta-Analyses. Global. Health 2021, 17, 34. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Sánchez-González, E.; González-Bernal, J.J. Psychological Effects of Home Confinement and Social Distancing Derived from Covid-19 in the General Population—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6528. [Google Scholar] [CrossRef]
- Solé, B.; Verdolini, N.; Amoretti, S.; Montejo, L.; Rosa, A.R.; Hogg, B.; Garcia-Rizo, C.; Mezquida, G.; Bernardo, M.; Martinez-Aran, A.; et al. Effects of the COVID-19 Pandemic and Lockdown in Spain: Comparison between Community Controls and Patients with a Psychiatric Disorder. Preliminary Results from the BRIS-MHC STUDY. J. Affect. Disord. 2021, 281, 13–23. [Google Scholar] [CrossRef]
- Hamm, M.E.; Brown, P.J.; Karp, J.F.; Lenard, E.; Cameron, F.; Dawdani, A.; Lavretsky, H.; Miller, J.P.; Mulsant, B.H.; Pham, V.T.; et al. Experiences of American Older Adults with Pre-Existing Depression During the Beginnings of the COVID-19 Pandemic: A Multicity, Mixed-Methods Study. Am. J. Geriatr. Psychiatry 2020, 28, 924–932. [Google Scholar] [CrossRef]
- Quittkat, H.L.; Düsing, R.; Holtmann, F.J.; Buhlmann, U.; Svaldi, J.; Vocks, S. Perceived Impact of COVID-19 Across Different Mental Disorders: A Study on Disorder-Specific Symptoms, Psychosocial Stress and Behavior. Front. Psychol. 2020, 11, 586246. [Google Scholar] [CrossRef]
- García-Álvarez, L.; de la Fuente-Tomás, L.; García-Portilla, M.P.; Sáiz, P.A.; Lacasa, C.M.; Santo, F.D.; González-Blanco, L.; Bobes-Bascarán, M.T.; García, M.V.; Vázquez, C.Á.; et al. Early Psychological Impact of the 2019 Coronavirus Disease (COVID-19) Pandemic and Lockdown in a Large Spanish Sample. J. Glob. Health 2020, 10, 1–15. [Google Scholar] [CrossRef]
- González-Blanco, L.; Dal Santo, F.; García-Álvarez, L.; de la Fuente-Tomás, L.; Moya Lacasa, C.; Paniagua, G.; Sáiz, P.A.; García-Portilla, M.P.; Bobes, J. COVID-19 Lockdown in People with Severe Mental Disorders in Spain: Do They Have a Specific Psychological Reaction Compared with Other Mental Disorders and Healthy Controls? Schizophr. Res. 2020, 223, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, N.; Gil, S.; Chevalère, J.; Belletier, C.; Dezecache, G.; Huguet, P.; Droit-Volet, S. The Impact of the COVID-19 Pandemic on Vulnerable People Suffering from Depression: Two Studies on Adults in France. Int. J. Environ. Res. Public Health 2021, 18, 3250. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.G.; Paluszek, M.M.; Landry, C.A.; Rachor, G.S.; McKay, D.; Taylor, S. Do Pre-Existing Anxiety-Related and Mood Disorders Differentially Impact COVID-19 Stress Responses and Coping? J. Anxiety Disord. 2020, 74, 102271. [Google Scholar] [CrossRef] [PubMed]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do Psychiatric Patients Experience More Psychiatric Symptoms during COVID-19 Pandemic and Lockdown? A Case-Control Study with Service and Research Implications for Immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Korsnes, M.S.; Grødal, E.; Kjellén, E.; Kaspersen, T.M.C.; Gjellesvik, K.B.; Benth, J.Š.; McPherson, B.A. COVID-19 Concerns Among Old Age Psychiatric In- and Out-Patients and the Employees Caring for Them, a Preliminary Study. Front. Psychiatry 2020, 11, 576935. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Stevens, C.; Conrad, R.C.; Hahm, H.C. Evidence for Elevated Psychiatric Distress, Poor Sleep, and Quality of Life Concerns during the COVID-19 Pandemic among U.S. Young Adults with Suspected and Reported Psychiatric Diagnoses. Psychiatry Res. 2020, 292, 113345. [Google Scholar] [CrossRef]
- Zhu, J.H.; Li, W.; Huo, X.N.; Jin, H.M.; Zhang, C.H.; Yun, J.D.; Gao, L.G.; Cheung, T.; Hall, B.J.; Yang, B.; et al. The Attitude towards Preventive Measures and Knowledge of COVID-19 Inpatients with Severe Mental Illness in Economically Underdeveloped Areas of China. Psychiatr. Q. 2021, 92, 683–691. [Google Scholar] [CrossRef]
- Castaldelli-Maia, J.M.; Marziali, M.E.; Lu, Z.; Martins, S.S. Investigating the Effect of National Government Physical Distancing Measures on Depression and Anxiety during the COVID-19 Pandemic through Meta-Analysis and Meta-Regression. Psychol. Med. 2021, 51, 881–893. [Google Scholar] [CrossRef]
- Jin, Y.; Sun, T.; Zheng, P.; An, J. Mass Quarantine and Mental Health during COVID-19: A Meta-Analysis. J. Affect. Disord. 2021, 295, 1335–1346. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Wang, H. The Psychological and Mental Impact of Coronavirus Disease 2019 (COVID-19) on Medical Staff and General Public—A Systematic Review and Meta-Analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Phiri, P.; Ramakrishnan, R.; Rathod, S.; Elliot, K.; Thayanandan, T.; Sandle, N.; Haque, N.; Chau, S.W.; Wong, O.W.; Chan, S.S.; et al. An Evaluation of the Mental Health Impact of SARS-CoV-2 on Patients, General Public and Healthcare Professionals: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 34, 100806. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Global. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Franchini, L.; Ragone, N.; Seghi, F.; Barbini, B.; Colombo, C. Mental Health Services for Mood Disorder Outpatients in Milan during COVID-19 Outbreak: The Experience of the Health Care Providers at San Raffaele Hospital. Psychiatry Res. 2020, 292, 113317. [Google Scholar] [CrossRef] [PubMed]
- Frank, A.; Fatke, B.; Frank, W.; Förstl, H.; Hölzle, P. Depression, Dependence and Prices of the COVID-19-Crisis. Brain Behav. Immun. 2020, 87, 99. [Google Scholar] [CrossRef] [PubMed]
- Iasevoli, F.; Fornaro, M.; D’Urso, G.; Galletta, D.; Casella, C.; Paternoster, M.; Buccelli, C.; De Bartolomeis, A. Psychological Distress in Patients with Serious Mental Illness during the COVID-19 Outbreak and One-Month Mass Quarantine in Italy. Psychol. Med. 2021, 51, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Muruganandam, P.; Neelamegam, S.; Menon, V.; Alexander, J.; Chaturvedi, S.K. COVID-19 and Severe Mental Illness: Impact on Patients and Its Relation with Their Awareness about COVID-19. Psychiatry Res. 2020, 291, 113265. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.Y.; Kok, A.A.L.; Eikelenboom, M.; Horsfall, M.; Jörg, F.; Luteijn, R.A.; Rhebergen, D.; van Oppen, P.; Giltay, E.J.; Penninx, B.W.J.H. The Mental Health Impact of the COVID-19 Pandemic on People with and without Depressive, Anxiety, or Obsessive-Compulsive Disorders: A Longitudinal Study of Three Dutch Case-Control Cohorts. Lancet Psychiatry 2021, 8, 121–129. [Google Scholar] [CrossRef]
- Leightley, D.; Lavelle, G.; White, K.M.; Sun, S.; Matcham, F.; Ivan, A.; Oetzmann, C.; Penninx, B.W.J.H.; Lamers, F.; Siddi, S.; et al. Investigating the Impact of COVID-19 Lockdown on Adults with a Recent History of Recurrent Major Depressive Disorder: A Multi-Centre Study Using Remote Measurement Technology. BMC Psychiatry 2021, 21, 435. [Google Scholar] [CrossRef]
- Siddi, S.; Giné-Vázquez, I.; Bailon, R.; Matcham, F.; Lamers, F.; Kontaxis, S.; Laporta, E.; Garcia, E.; Arranz, B.; Costa, G.D.; et al. Biopsychosocial Response to the COVID-19 Lockdown in People with Major Depressive Disorder and Multiple Sclerosis. J. Clin. Med. 2022, 11, 7163. [Google Scholar] [CrossRef]
- Matcham, F.; Barattieri Di San Pietro, C.; Bulgari, V.; De Girolamo, G.; Dobson, R.; Eriksson, H.; Folarin, A.A.; Haro, J.M.; Kerz, M.; Lamers, F.; et al. Remote Assessment of Disease and Relapse in Major Depressive Disorder (RADAR-MDD): A Multi-Centre Prospective Cohort Study Protocol. BMC Psychiatry 2019, 19, 72. [Google Scholar] [CrossRef] [Green Version]
- The Territorial Impact of COVID-19: Managing the Crisis across Levels of Government. Available online: https://www.oecd.org/coronavirus/policy-responses/the-territorial-impact-of-COVID-19-managing-the-crisis-across-levels-of-government-d3e314e1/ (accessed on 7 August 2022).
- COVID-19: Stringency Index—Our World in Data. Available online: https://ourworldindata.org/covid-stringency-index#learn-more-about-the-data-source-the-oxford-coronavirus-government-response-tracker (accessed on 26 January 2023).
- Aknin, L.B.; Andretti, B.; Goldszmidt, R.; Helliwell, J.F.; Petherick, A.; De Neve, J.E.; Dunn, E.W.; Fancourt, D.; Goldberg, E.; Jones, S.P.; et al. Policy Stringency and Mental Health during the COVID-19 Pandemic: A Longitudinal Analysis of Data from 15 Countries. Lancet Public Health 2022, 7, e417–e426. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, Y.; Rashid, Z.; Stewart, C.; Conde, P.; Begale, M.; Verbeeck, D.; Boettcher, S.; Dobson, R.; Folarin, A. Radar-Base: Open Source Mobile Health Platform for Collecting, Monitoring, and Analyzing Data Using Sensors, Wearables, and Mobile Devices. JMIR mHealth uHealth 2019, 7, e11734. [Google Scholar] [CrossRef] [Green Version]
- Matcham, F.; Carr, E.; White, K.M.; Leightley, D.; Lamers, F.; Siddi, S.; Annas, P.; Haro, J.M.; Horsfall, M.; Ivan, A.; et al. Predictors of Engagement with Remote Sensing Technologies for Symptom Measurement in Major Depressive Disorder. J. Affect Disord. 2022, 310, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a Measure of Current Depression in the General Population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, J.; Douglas, B.; Saikat, D.; Deepayan, S.; R Core Team. Nlme: Linear and Nonlinear Mixed Effects Models; R Package Version 3.1-152; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Sun, S.; Folarin, A.A.; Ranjan, Y.; Rashid, Z.; Conde, P.; Stewart, C.; Cummins, N.; Matcham, F.; Costa, G.D.; Simblett, S.; et al. Using Smartphones and Wearable Devices to Monitor Behavioral Changes during COVID-19. J. Med. Internet Res. 2020, 22, e19992. [Google Scholar] [CrossRef]
- Fleischmann, E.; Dalkner, N.; Fellendorf, F.T.; Reininghaus, E.Z. Psychological Impact of the COVID-19 Pandemic on Individuals with Serious Mental Disorders: A Systematic Review of the Literature. World J. Psychiatry 2021, 11, 1387–1406. [Google Scholar] [CrossRef]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies Comparing Mental Health before versus during the COVID-19 Pandemic in 2020. J. Affect. Disord. 2022, 296, 567–576. [Google Scholar] [CrossRef]
- Kontaxis, S.; Gil, E.; Marozas, V.; Lazaro, J.; Garcia, E.; Posadas-De Miguel, M.; Siddi, S.; Bernal, M.L.; Aguilo, J.; Haro, J.M.; et al. Photoplethysmographic Waveform Analysis for Autonomic Reactivity Assessment in Depression. IEEE Trans. Biomed. Eng. 2021, 68, 1273–1281. [Google Scholar] [CrossRef]
- Osório, C.; Probert, T.; Jones, E.; Young, A.H.; Robbins, I. Adapting to Stress: Understanding the Neurobiology of Resilience. Behav. Med. 2017, 43, 307–322. [Google Scholar] [CrossRef] [Green Version]
- Jefatura de Estado Real Decreto 463/2020, de 14 de Marzo, BOE n.°3692; 2020. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-2020-3692 (accessed on 22 April 2022).
- García-Esquinas, E.; Ortolá, R.; Gine-Vázquez, I.; Carnicero, J.A.; Mañas, A.; Lara, E.; Alvarez-Bustos, A.; Vicente-Rodriguez, G.; Sotos-Prieto, M.; Olaya, B.; et al. Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the Covid-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2021, 18, 7067. [Google Scholar] [CrossRef]
- RESOLUCIÓ SLT/719/2020, de 12 de Març; 2020. Available online: https://cido.diba.cat/legislacio/9970276/resolucio-slt7192020-de-12-de-marc-per-la-qual-sadopten-mesures-addicionals-per-a-la-prevencio-i-el-control-de-la-infeccio-pel-sars-cov-2-departament-de-salut (accessed on 22 April 2022).
- RESOLUCIÓ SLT/720/2020, de 13 de Març; 2020. Available online: https://cido.diba.cat/legislacio/9956411/resolucio-slt7202020-de-13-de-marc-per-la-qual-sadopten-noves-mesures-addicionals-per-a-la-prevencio-i-el-control-de-la-infeccio-pel-sars-cov-2-departament-de-salut (accessed on 22 April 2022).
- RESOLUCIÓ SLT/746/2020, de 18 de Març; 2020. Available online: https://cido.diba.cat/legislacio/9954147/resolucio-slt7462020-de-18-de-marc-per-la-qual-sadopten-noves-mesures-complementaries-per-a-la-prevencio-i-el-control-de-la-infeccio-pel-sars-cov-2-departament-de-salut (accessed on 22 April 2022).
- RESOLUCIÓ SLT/761/2020, de 23 de Març; 2020. Available online: https://cido.diba.cat/legislacio/9960076/resolucio-slt7612020-de-23-de-marc-per-la-qual-sadopten-noves-mesures-complementaries-per-a-la-prevencio-i-el-control-de-la-infeccio-pel-sars-cov-2-departament-de-salut (accessed on 22 April 2022).
- ELNACIONAL.CAT. El Garraf y El Alt Penedès Vuelven a Integrarse En El Territorio de Barcelona. Available online: https://www.elnacional.cat/es/politica/coronavirus-garraf-alt-penedes-territorio-barcelona_511356_102.html (accessed on 22 April 2022).
- Jefatura de Estado Disposición 11590, BOE n.°260. 2020. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-11590 (accessed on 22 April 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N = 121 | |
|---|---|---|
| Gender, N (%) | Male | 40 (33.1) |
| Female | 81 (66.9) | |
| Comorbidity 1, N (%) | Yes | 74 (61.2) |
| No | 47 (38.8) | |
| Age, Median (IQR) | 58 (52–64) | |
| Marital status, N (%) | with a partner | 68 (56.2) |
| without a partner | 53 (42.8) | |
| People living with, N (%) | alone | 22 (18.2) |
| two | 40 (33.1) | |
| three | 37 (30.6) | |
| four or more | 22 (18.2) | |
| Employment, N (%) | Employed | 43 (35.5) |
| Unemployed 2 | 78 (64.5) | |
| Income 3, N (%) | <15,000 € | 33 (27.3) |
| 15,000 €–24,000 € | 48 (39.7) | |
| >24,000 € | 40 (33.1) | |
| Age of finishing education, mean (SD) | 17.6 (4.95) | |
| Pre-lockdown PHQ-8 | Mean | 12.90 |
| Median (IQR) | 13 (10.2) | |
| Pre-lockdown GAD-7 | Mean | 10.76 |
| Median (IQR) | 10 (5.2) | |
| Pre-lockdown PHQ-8, N (%) | PHQ-8 < 10 | 39 (32.2) |
| PHQ-8 ≥ 10 | 82 (67.8) | |
| Pre-lockdown GAD-7, N (%) | GAD-7 < 10 | 43 (35.5) |
| GAD-7 ≥ 10 | 78 (64.5) |
| Coef. 1 | CI (95%) | p-Value | |
|---|---|---|---|
| Pre-lockdown | Ref | - | - |
| Lockdown | 0.866 | [0.430 to 1.303] | ≤0.001 |
| Phase 0 | 1.135 | [0.560 to 1.711] | ≤0.001 |
| Phase 1 | −0.004 | [−0.709 to 0.700] | 0.990 |
| Phase 2–3 | 0.098 | [−0.770 to 0.967] | 0.824 |
| New-normality | −0.099 | [−0.437 to 0.238] | 0.562 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavalle, R.; Condominas, E.; Haro, J.M.; Giné-Vázquez, I.; Bailon, R.; Laporta, E.; Garcia, E.; Kontaxis, S.; Alacid, G.R.; Lombardini, F.; et al. The Impact of COVID-19 Lockdown on Adults with Major Depressive Disorder from Catalonia: A Decentralized Longitudinal Study. Int. J. Environ. Res. Public Health 2023, 20, 5161. https://doi.org/10.3390/ijerph20065161
Lavalle R, Condominas E, Haro JM, Giné-Vázquez I, Bailon R, Laporta E, Garcia E, Kontaxis S, Alacid GR, Lombardini F, et al. The Impact of COVID-19 Lockdown on Adults with Major Depressive Disorder from Catalonia: A Decentralized Longitudinal Study. International Journal of Environmental Research and Public Health. 2023; 20(6):5161. https://doi.org/10.3390/ijerph20065161
Chicago/Turabian StyleLavalle, Raffaele, Elena Condominas, Josep Maria Haro, Iago Giné-Vázquez, Raquel Bailon, Estela Laporta, Ester Garcia, Spyridon Kontaxis, Gemma Riquelme Alacid, Federica Lombardini, and et al. 2023. "The Impact of COVID-19 Lockdown on Adults with Major Depressive Disorder from Catalonia: A Decentralized Longitudinal Study" International Journal of Environmental Research and Public Health 20, no. 6: 5161. https://doi.org/10.3390/ijerph20065161