

Gender Differences in Socio-Demographic Factors Associated with Pre-Frailty in Japanese Rural Community-Dwelling Older Adults: A Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Items
2.2.1. Frailty
2.2.2. Social Aspects
2.2.3. Physical Aspects
2.2.4. Mental Aspects
2.2.5. Basic Attributes
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
3.1. Comparison of Pre-Frailty and Healthy Groups (Table 1)
3.1.1. Participant Characteristics

{kind=link}
| Men | Women | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Pre-Frailty | Healthy | p | Total | Pre-Frailty | Healthy | p | |||||||||
| (n = 203) | (n = 93) | (n = 110) | (n = 181) | (n = 103) | (n = 78) | |||||||||||
| n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | |||||||||||
| Demographic | Age (mean ± SD) | 74 | ±6 | 75 | ±6 | 74 | ±5 | 0.089 | 74 | ±6 | 75 | ±6 | 73 | ±5 | 0.019 | |
| Physical | DVS (mean ± SD) | 2.9 | ±2.4 | 2.6 | ±2.3 | 3.3 | ±2.4 | 0.075 | 3.9 | ±2.5 | 3.9 | ±2.7 | 3.8 | ±2.3 | 0.776 | |
| Exercise habit | yes | 153 | (77) | 65 | (71) | 88 | (81) | 0.094 | 146 | (84) | 81 | (82) | 65 | (87) | 0.389 | |
| no | 46 | (23) | 26 | (29) | 20 | (19) | 28 | (16) | 18 | (18) | 10 | (13) | ||||
| History of disease | yes | 40 | (22) | 19 | (23) | 21 | (22) | 0.933 | 37 | (22) | 16 | (17) | 21 | (30) | 0.042 | |
| no | 143 | (78) | 69 | (77) | 74 | (78) | 129 | (78) | 80 | (83) | 49 | (70) | ||||
| BMI | <18.5 | 10 | (5) | 8 | (9) | 2 | (2) | 0.047 | 17 | (10) | 10 | (10) | 7 | (10) | 0.941 | |
| ≥18.5 | 187 | (95) | 84 | (91) | 103 | (98) | 152 | (90) | 88 | (90) | 64 | (90) | ||||
| Subjective symptoms | no | 109 | (57) | 44 | (48) | 65 | (66) | 0.010 | 106 | (62) | 51 | (37) | 55 | (74) | 0.003 | |
| yes | 81 | (43) | 48 | (52) | 33 | (34) | 66 | (38) | 47 | (63) | 19 | (26) | ||||
| Mental | Depressive state | yes | 31 | (16) | 22 | (24) | 9 | (8.9) | 0.004 | 46 | (27) | 34 | (35) | 12 | (16) | 0.004 |
| no | 160 | (84) | 68 | (76) | 92 | (91) | 126 | (73) | 62 | (65) | 64 | (84) | ||||
| self-rated health | better | 177 | (93) | 78 | (87) | 99 | (98) | 0.003 | 156 | (89) | 84 | (85) | 72 | (95) | 0.037 | |
| poor | 14 | (7) | 12 | (13) | 2 | (1.9) | 19 | (11) | 15 | (15) | 4 | (5) | ||||
| Social | Solitary living | yes | 23 | (11) | 12 | (13) | 11 | (10) | 0.629 | 25 | (14) | 17 | (17) | 8 | (10) | 0.208 |
| no | 178 | (89) | 79 | (87) | 99 | (90) | 154 | (86) | 84 | (83) | 70 | (90) | ||||
| Solitary eating | no | 162 | (81) | 71 | (76) | 91 | (85) | 0.118 | 139 | (77) | 73 | (72) | 66 | (85) | 0.039 | |
| yes | 38 | (19) | 22 | (24) | 16 | (15) | 41 | (23) | 29 | (28) | 12 | (15) | ||||
| Job | yes | 91 | (45) | 38 | (41) | 53 | (48) | 0.328 | 43 | (24) | 22 | (22) | 21 | (28) | 0.370 | |
| no | 111 | (55) | 54 | (59) | 57 | (52) | 134 | (76) | 79 | (78) | 55 | (72) | ||||
| Economic status | difficult | 55 | (27) | 31 | (34) | 24 | (22) | 0.113 | 39 | (22) | 23 | (23) | 16 | (21) | 0.728 | |
| usually | 125 | (62) | 53 | (58) | 72 | (65) | 130 | (73) | 74 | (73) | 56 | (73) | ||||
| afford | 21 | (11) | 7 | (8) | 14 | (13) | 9 | (5) | 4 | (3.9) | 5 | (6) | ||||
| Outings at least once a week | yes | 189 | (95) | 88 | (97) | 101 | (94) | 0.511 | 173 | (97) | 97 | (96) | 76 | (99) | 0.391 | |
| no | 9 | (5) | 3 | (3) | 6 | (6) | 5 | (3) | 4 | (3.9) | 1 | (1) | ||||
| Intimate friend | yes | 165 | (85) | 74 | (82) | 91 | (87) | 0.391 | 158 | (91) | 88 | (89) | 70 | (93) | 0.315 | |
| no | 30 | (15) | 16 | (18) | 14 | (13) | 16 | (9) | 11 | (11) | 5 | (7) | ||||
| Being invited by someone | yes | 91 | (47) | 42 | (48) | 49 | (46) | 0.835 | 106 | (60) | 55 | (54) | 51 | (66) | 0.113 | |
| no | 103 | (53) | 46 | (52) | 57 | (54) | 72 | (40) | 46 | (46) | 26 | (34) | ||||
| Sources of health information | family and friend | 106 | (54) | 46 | (51) | 60 | (57) | 0.442 | 118 | (66) | 62 | (61) | 56 | (73) | 0.113 | |
| otherwise | 90 | (46) | 44 | (49) | 46 | (43) | 60 | (34) | 39 | (39) | 21 | (27) | ||||
| Community participation in middle age | yes | 117 | (60) | 49 | (55) | 68 | (64) | 0.197 | 102 | (59) | 49 | (50) | 53 | (71) | 0.006 | |
| no | 78 | (40) | 40 | (45) | 38 | (36) | 71 | (41) | 49 | (50) | 22 | (29) | ||||
| Participation in social activities at least once a week | yes | 96 | (49) | 41 | (45) | 55 | (53) | 0.245 | 79 | (47) | 40 | (43) | 39 | (52) | 0.221 | |
| no | 100 | (51) | 51 | (55) | 49 | (47) | 90 | (53) | 54 | (57) | 36 | (48) | ||||
| Friends who listen to one’s concerns | yes | 60 | (30) | 30 | (33) | 30 | (28) | 0.403 | 102 | (58) | 53 | (52) | 49 | (64) | 0.110 | |
| no | 140 | (70) | 61 | (67) | 79 | (72) | 75 | (42) | 48 | (48) | 27 | (36) | ||||
| Listening to a friend’s concerns | yes | 64 | (32) | 31 | (34) | 33 | (31) | 0.560 | 102 | (59) | 54 | (55) | 48 | (64) | 0.210 | |
| no | 134 | (68) | 59 | (66) | 75 | (69) | 72 | (41) | 45 | (45) | 27 | (36) | ||||
3.1.2. Social Aspects
3.1.3. Physical Aspects
3.1.4. Mental Aspects
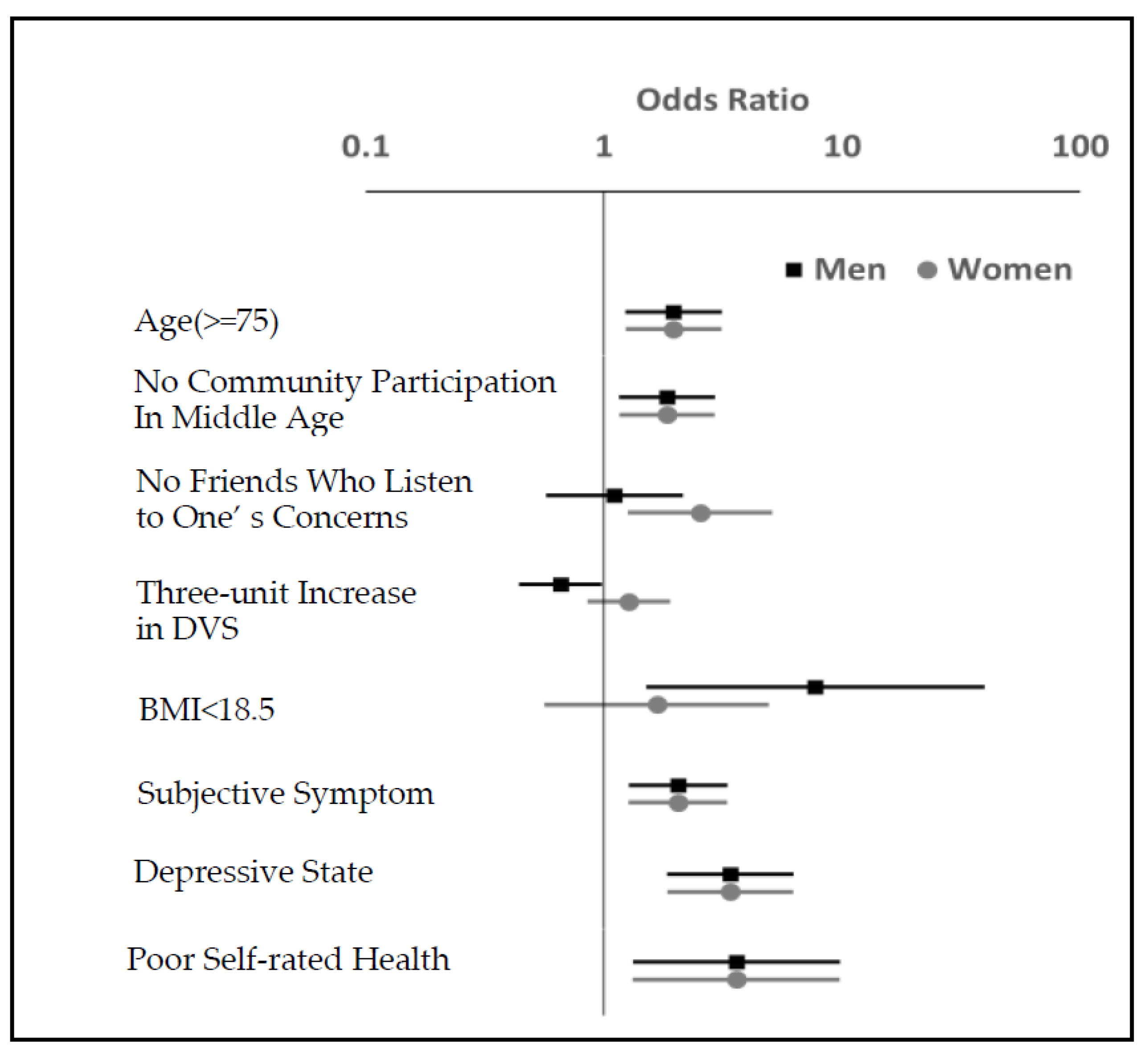
3.2. Factors Associated with Pre-Frailty
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Junius-Walker, U.; Onder, G.; Soleymani, D.; Wiese, B.; Albaina, O.; Bernabei, R.; Marzetti, E.; ADVANTAGE JA WP4 Group. The essence of frailty: A systematic review and qualitative synthesis on frailty concepts and definitions. Eur. J. Intern. Med. 2018, 56, 3–10. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D.; et al. Global incidence of frailty and prefrailty among community-dwelling older adults: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e198398. [Google Scholar] [CrossRef] [Green Version]
- Jang, A.R.; Won, C.W.; Sagong, H.; Bae, E.; Park, H.; Yoon, J.Y. Social factors predicting improvement of frailty in community-dwelling older adults: Korean Frailty and Aging Cohort Study. Geriatr. Gerontol. Int. 2021, 21, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M.G.A. In search of an integral conceptual definition of frailty: Opinions of experts. J. Am. Med. Dir. Assoc. 2010, 11, 338–343. [Google Scholar] [CrossRef]
- Dedeyne, L.; Deschodt, M.; Verschueren, S.; Tournoy, J.; Gielen, E. Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: A systematic review. Clin. Interv. Aging 2017, 12, 873–896. [Google Scholar] [CrossRef] [Green Version]
- Kidd, T.; Mold, F.; Jones, C.; Ream, E.; Grosvenor, W.; Sund-Levander, M.; Tingström, P.; Carey, N. What are the most effective interventions to improve physical performance in pre-frail and frail adults? A systematic review of randomised control trials. BMC Geriatr. 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Fan, W.; Zhu, B.; Ma, C.; Tan, X.; Gu, Y. Frailty Risk Prediction Model among Older Adults: A Chinese Nation-Wide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8410. [Google Scholar] [CrossRef]
- Duppen, D.; van der Elst, M.C.J.; Dury, S.; Lambotte, D.; De Donder, L. The social environment’s relationship with frailty: Evidence from existing studies. J. Appl. Gerontol. 2019, 38, 3–26. [Google Scholar] [CrossRef]
- Kanamori, S.; Kai, Y.; Aida, J.; Kondo, K.; Kawachi, I.; Hirai, H.; Shirai, K.; Ishikawa, Y.; Suzuki, K. Social participation and the prevention of functional disability in older Japanese: The JAGES cohort study. PLoS ONE 2014, 9, e99638. [Google Scholar] [CrossRef]
- Chon, D.; Lee, Y.; Jinhee, K.; Kyung-eun, L. The association between frequency of social contact and frailty in older people: Korean Frailty and Aging Cohort Study (KFACS). J. Korean Med. Sci. 2018, 33, e332. [Google Scholar] [CrossRef]
- Arizaga-Iribarren, N.; Irazusta, A.; Mugica-Errazquin, I.; Virgala-García, J.; Amonarraiz, A.; Kortajarena, M. Sex Differences in Frailty Factors and Their Capacity to Identify Frailty in Older Adults Living in Long-Term Nursing Homes. Int. J. Environ. Res. Public Health 2023, 20, 54. [Google Scholar] [CrossRef]
- Ayeni, A.; Sharples, A.; Hewson, D. The Association between Social Vulnerability and Frailty in Community Dwelling Older People: A Systematic Review. Geriatrics 2022, 7, 104. [Google Scholar] [CrossRef]
- Woo, J.; Goggins, W.; Sham, A.; Ho, S.C. Social determinants of frailty. Gerontology 2005, 51, 402–408. [Google Scholar] [CrossRef]
- Japanese Ministry of Internal Affairs and Communications. Portal Site of Official Statistics of Japan. 2021. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&layout=data (accessed on 10 October 2022).
- Japanese Ministry of Health, Labour and Welfare. The Manuals of the Evaluation for Ability to Perform Daily Activities on Preventive Care. 2012. Available online: https://www.mhlw.go.jp/topics/2009/05/dl/tp0501-1_1.pdf (accessed on 10 October 2022).
- Sampaio, P.Y.S.; Sampaio, R.A.C.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Sampaio, P.Y.S.; Sampaio, R.A.C.; Yamada, M.; Ogita, M.; Arai, H. Validation and translation of the Kihon Checklist (frailty index) into Brazilian Portuguese. Geriatr. Gerontol. Int. 2014, 14, 561–569. [Google Scholar] [CrossRef]
- Maseda, A.; Lorenzo-López, L.; López-López, R.; Arai, H.; Millán-Calenti, J.C. Spanish translation of the Kihon Checklist (frailty index). Geriatr. Gerontol. Int. 2017, 17, 515–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sentandreu-Mañó, T.; Cezón-Serrano, N.; Cebrià I Iranzo, M.A.; Tortosa-Chuliá, M.A.; Tomás, J.M.; Salom Terrádez, J.R.; Balasch-Bernat, M. Kihon Checklist to assess frailty in older adults: Some evidence on the internal consistency and validity of the Spanish version. Geriatr. Gerontol. Int. 2021, 21, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Tao, A.; Zhang, Y.; Qiu, X.; Arai, H.; Wang, Q. Simplified Chinese translation of the Kihon checklist. Geriatr. Gerontol. Int. 2020, 20, 643–644. [Google Scholar] [CrossRef]
- Assantachai, P.; Muangpaisan, W.; Intalapaporn, S.; Jongsawadipatana, A.; Arai, H. Kihon Checklist: Thai version. Geriatr. Gerontol. Int. 2021, 21, 749–752. [Google Scholar] [CrossRef]
- Esenkaya, M.E.; Dokuzlar, O.; Soysal, P.; Smith, L.; Jackson, S.E.; Isik, A.T. Validity of the Kihon Checklist for evaluating frailty status in Turkish older adults. Geriatr. Gerontol. Int. 2019, 19, 616–621. [Google Scholar] [CrossRef]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Jpn. J. Public Health 2003, 50, 1117–1124. [Google Scholar]
- Whooley, M.A.; Avins, A.L.; Miranda, J.; Browner, W.S. Case-finding instruments for depression. Two questions are as good as many. J. Gen. Intern. Med. 1997, 12, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, N.C.; Kim, J.; DiNitto, D.M.; Marti, C.N. Perceived social cohesion, frequency of going out, and depressive symptoms in older adults: Examination of longitudinal relationships. Gerontol. Geriatr. Med. 2015, 1, 2333721415615478. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, H.; Okada, S.; Shirasawa, M. Factors associated with social activities among the elderly in a metropolitan area: Physical, psychological, and socio-environmental parameters. Jpn. J. Public Health 2006, 53, 504–515. [Google Scholar]
- Carlisle, K.; Farmer, J.; Taylor, J.; Larkins, S.; Evans, R. Evaluating community participation: A comparison of participatory approaches in the planning and implementation of new primary health-care services in northern Australia. Int. J. Health Plann Manag. 2018, 33, 704–722. [Google Scholar] [CrossRef]
- Kishi, R.; Horikawa, N. Role of the social support network which influences age of death and physical function of elderly people: Study of trends in and outside of Japan and future problems. Jpn. J. Public Health 2004, 51, 79–93. [Google Scholar]
- Bowling, A. Social support and social networks: Their relationship to the successful and unsuccessful survival of elderly people in the community. An analysis of concepts and a review of the evidence. Fam. Pract. 1991, 8, 68–83. [Google Scholar] [CrossRef] [PubMed]
- Murata, C.; Saito, Y.; Kondo, K.; Hirai, H. Social support and depression among community living older people. Jpn. J. Gerontol. 2011, 33, 15–22. [Google Scholar]
- Schaefer, C.; Coyne, J.C.; Lazarus, R.S. The health-related functions of social support. J. Behav. Med. 1981, 4, 381–406. [Google Scholar] [CrossRef]
- Feng, Z.; Lugtenberg, M.; Franse, C.; Fang, X.; Hu, S.; Jin, C.; Raat, H. Risk factors and protective factors associated with incident or increase of frailty among community-dwelling older adults: A systematic review of longitudinal studies. PLoS ONE 2017, 12, e0178383. [Google Scholar] [CrossRef]
- Kimura, H.; Nishino, M.; Koga, K.; Kukihara, H. Preventive care for frail seniors living alone in the community-Special characteristics compared with seniors living with others. Asian Pac. J. Dis. Manag. 2020, 9, 11–18. [Google Scholar] [CrossRef]
- Fulop, T.; Larbi, A.; Witkowski, J.M.; McElhaney, J.; Loeb, M.; Mitnitski, A.; Pawelec, G. Aging, frailty and age-related diseases. Biogerontology 2010, 11, 547–563. [Google Scholar] [CrossRef] [PubMed]
- Saadeh, M.; Welmer, A.K.; Dekhtyar, S.; Fratiglioni, L.; Calderón-Larrañaga, A. The role of psychological and social well-being on physical function trajectories in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1579–1585. [Google Scholar] [CrossRef]
- Fujii, K.; Fujii, Y.; Kubo, Y.; Tateoka, K.; Liu, J.; Nagata, K.; Nakashima, D.; Okura, T. Frail Older Adults without Occupational Dysfunction Maintain Good Subjective Well-Being: A Cross-Sectional Study. Healthcare 2022, 10, 1922. [Google Scholar] [CrossRef]
- Rockwood, K.; Andrew, M.; Mitnitski, A. A comparison of two approaches to measuring frailty in elderly people. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 738–743. [Google Scholar] [CrossRef]
- Xue, Q.-L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial manifestations of frailty criteria and the development of frailty phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Yoshizaki, T.; Yokoyama, Y.; Oue, A.; Kawaguchi, H. Association of dietary variety with nutrient and food group intake and frailty among community-dwelling Japanese older adults. Jpn. J. Nutr. Diet. 2019, 77, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Seino, S.; Kitamura, A.; Tomine, Y.; Tanaka, I.; Nishi, M.; Nofuji, Y.; Yokoyama, Y.; Nonaka, K.; Kuraoka, M.; Amano, H.; et al. Awareness of the term “frailty” and its correlates among older adults living in a metropolitan area. Jpn. J. Public Health 2020, 67, 399–412. [Google Scholar] [CrossRef]
- Harada, K.; Takaizumi, K.; Shibata, A.; Oka, K.; Nakamura, Y. Relationships between perception of exercise guidelines 2006, perception of other health promotion policies, and demographic variables. Jpn. J. Public Health 2009, 56, 737–743. [Google Scholar]
- Yoshizawa, Y.; Tanaka, T.; Takahashi, K.; Fujisaki, M.; Iijima, K. The associations of frailty with regular participation in physical, cultural, and community social activities among independent elders in Japan. Jpn. J. Public Health 2019, 66, 306–316. [Google Scholar] [CrossRef]
- Kondo, K. Progress in aging epidemiology in Japan: The JAGES project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef] [PubMed]

| Men (n = 203) | Women (n = 181) | ||||
|---|---|---|---|---|---|
| OR | (95% CI) | OR | (95% CI) | ||
| Demographic | Age | ||||
| ≥75 | 1.96 | (1.23–3.12) | Same as OR in men | ||
| 65–74 | 1 | ||||
| Social | Community participation in middle age | ||||
| no | 1.84 | (1.16–2.92) | Same as OR in men | ||
| yes | 1 | ||||
| Friends who listen to one’s concerns | |||||
| no | 1.05 | (0.54–2.05) | 2.54 | (1.26–5.10) | |
| yes | 1 | 1 | |||
| Physical | DVS | ||||
| Three more groups of food | 0.66 | (0.44–0.98) | 1.27 | (0.85–1.90) | |
| BMI | |||||
| <18.5 | 7.69 | (1.50–39.56) | 1.67 | (0.56–4.93) | |
| ≥18.5 | 1 | 1 | |||
| Subjective symptoms | |||||
| yes | 2.05 | (1.27–3.29) | Same as OR in men | ||
| no | 1 | ||||
| Mental | Depressive state | ||||
| yes | 3.39 | (1.84–6.25) | Same as OR in men | ||
| no | 1 | ||||
| Self-rated health | |||||
| poor | 3.60 | (1.32–9.78) | Same as OR in men | ||
| better | 1 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibata, A.; Suzuki, A.; Takahashi, K. Gender Differences in Socio-Demographic Factors Associated with Pre-Frailty in Japanese Rural Community-Dwelling Older Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 1091. https://doi.org/10.3390/ijerph20021091
Shibata A, Suzuki A, Takahashi K. Gender Differences in Socio-Demographic Factors Associated with Pre-Frailty in Japanese Rural Community-Dwelling Older Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(2):1091. https://doi.org/10.3390/ijerph20021091
Chicago/Turabian StyleShibata, Aki, Asuka Suzuki, and Kenzo Takahashi. 2023. "Gender Differences in Socio-Demographic Factors Associated with Pre-Frailty in Japanese Rural Community-Dwelling Older Adults: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 2: 1091. https://doi.org/10.3390/ijerph20021091