
Setting Goals to Reduce Cardiovascular Risk: A Retrospective Chart Review of a Pharmacist-Led Initiative in the Workplace
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patient Population
2.2. Data Collection
2.3. Analytic Approach
3. Results
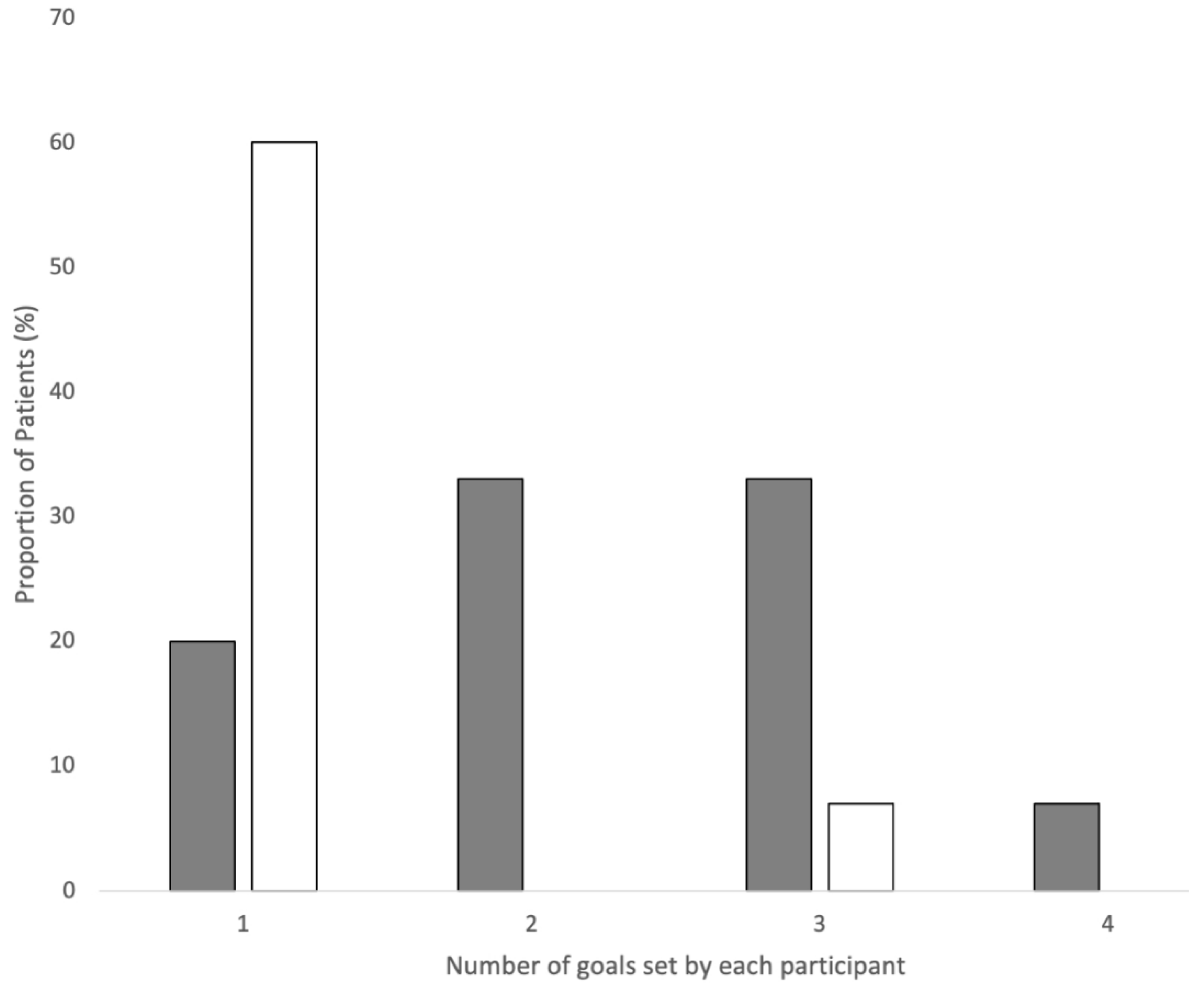
3.1. Patient CVD Prevention Goals: Initial Priorities
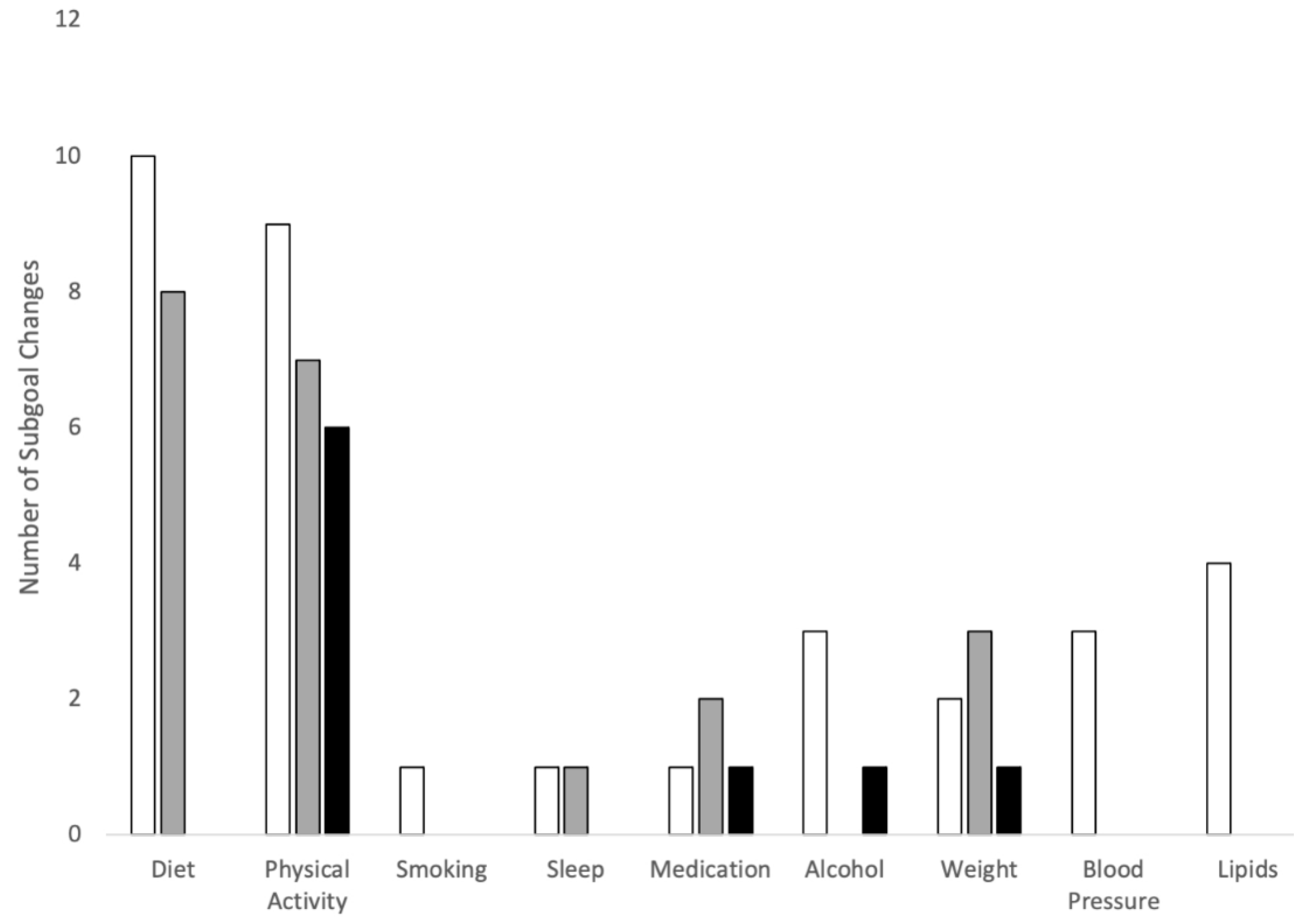
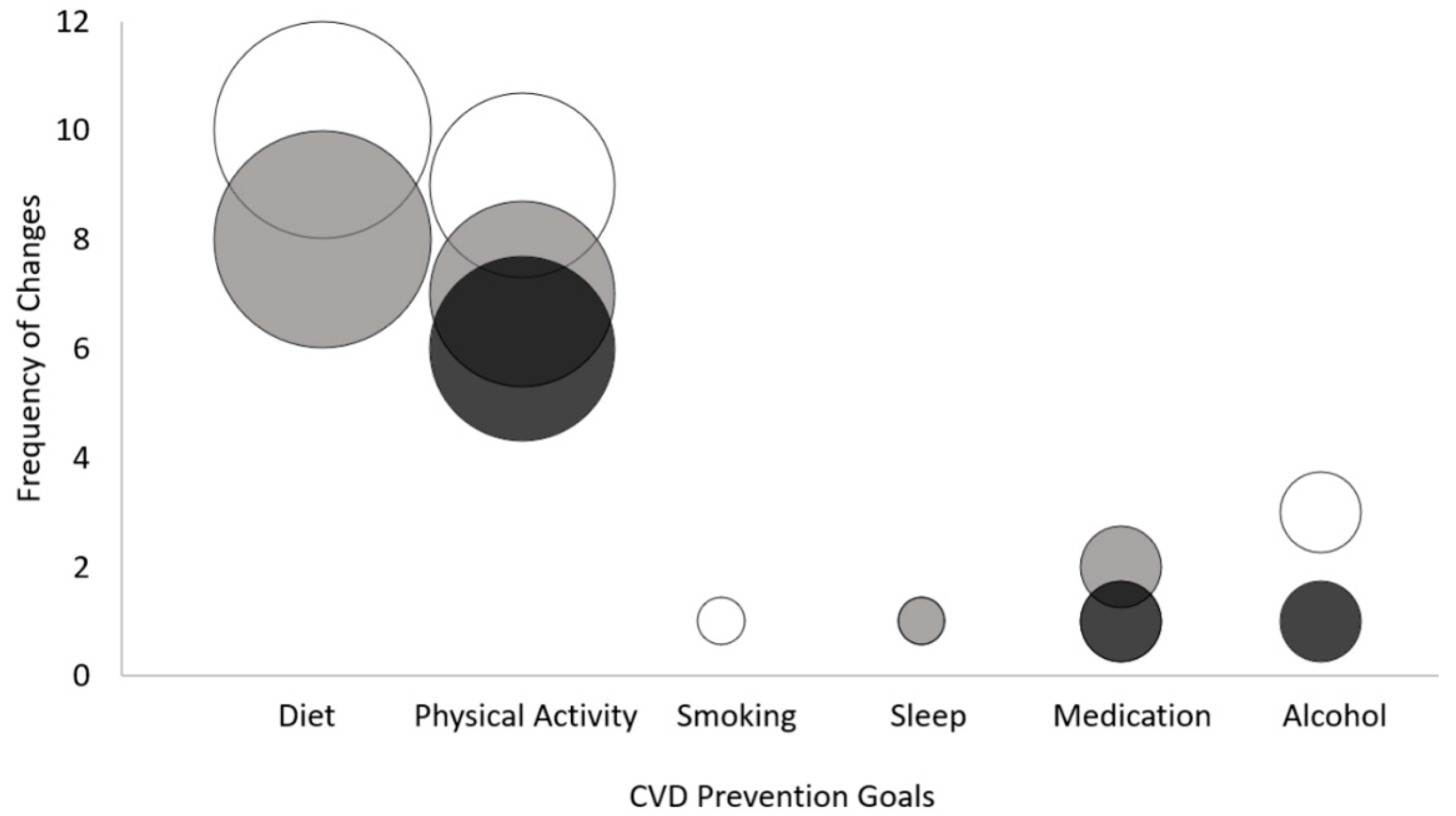
3.2. Patient CVD Prevention Goals over Time
3.3. Barriers to Patient Goals for CVD Prevention
4. Discussion
4.1. Relationship to Previous Work
4.2. Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistics Canada Leading Causes of Death, Total Population, by Age Group. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401 (accessed on 8 December 2022).
- Smith, E.R. The Canadian Heart Health Strategy and Action Plan. Can. J. Cardiol. 2009, 25, 451–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarride, J.-E.; Lim, M.; DesMeules, M.; Luo, W.; Burke, N.; O’Reilly, D.; Bowen, J.; Goeree, R. A review of the cost of cardiovascular disease. Can. J. Cardiol. 2009, 25, e195–e202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, X.; Quek, R.G.W.; Gandra, S.R.; Cappell, K.A.; Fowler, R.; Cong, Z. Productivity loss and indirect costs associated with cardiovascular events and related clinical procedures. BMC Health Serv. Res. 2015, 15, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zusman, E.Z.; Kapanen, A.I.; Klaassen, A.; Reardon, J. Workplace cardiovascular risk reduction by healthcare professionals—A systematic review. Occup. Med. 2021, 71, 270–276. [Google Scholar] [CrossRef]
- Pesis-Katz, I.; Smith, J.A.; Norsen, L.; Devoe, J.; Singh, R. Reducing Cardiovascular Disease Risk for Employees Through Participation in a Wellness Program. Popul. Health Manag. 2020, 23, 212–219. Available online: https://pubmed.ncbi.nlm.nih.gov/31513466/ (accessed on 1 September 2022). [CrossRef] [PubMed]
- Gobis, B.; Leung, L.; Min, J.; Thalakada, R.; Reardon, J.; Zed, P.J. The UBC Pharmacists Clinic. Can. Pharm. J./Rev. Des Pharm. Du Can. 2016, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapanen, A.I.; Conklin, A.I.; Gobis, B.; Leung, L.; Yuen, J.; Zed, P.J. Pharmacist-led cardiovascular risk prevention in Western Canada: A qualitative study. Int. J. Pharm. Pract. 2020, 29, 45–54. [Google Scholar] [CrossRef]
- Gobis, B.; Kapanen, A.I.; Reardon, J.; Min, J.; Li, K.H.; Lynd, L.; Zed, P.J. Cardiovascular Risk Reduction in the Workplace With CAMMPUS (Cardiovascular Assessment and Medication Management by Pharmacists at the UBC Site). Ann. Pharmacother. 2019, 53, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–14. Available online: https://pubmed.ncbi.nlm.nih.gov/28351367/ (accessed on 1 September 2022). [CrossRef] [PubMed] [Green Version]
- O’Connor, E.A.; Evans, C.V.; Rushkin, M.C.; Redmond, N.; Lin, J.S. Behavioral Counseling to Promote a Healthy Diet and Physical Activity for Cardiovascular Disease Prevention in Adults with Cardiovascular Risk Factors: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA—J. Am. Med. Assoc. 2020, 324. [Google Scholar] [CrossRef]
- Groeneveld, I.F.; Proper, K.I.; van der Beek, A.J.; Hildebrandt, V.H.; van Mechelen, W. Short and long term effects of a lifestyle intervention for construction workers at risk for cardiovascular disease: A randomized controlled trial. BMC Public Health 2011, 11, 836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardcastle, S.J.; Taylor, A.H.; Bailey, M.P.; Harley, R.A.; Hagger, M.S. Effectiveness of a motivational interviewing intervention on weight loss, physical activity and cardiovascular disease risk factors: A randomised controlled trial with a 12-month post-intervention follow-up. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shilts, M.K.; Horowitz, M.; Townsend, M.S. Goal Setting as a Strategy for Dietary and Physical Activity Behavior Change: A Review of the Literature. Am. J. Health Promot. 2004, 19, 81–93. [Google Scholar] [CrossRef] [PubMed]
- McEwan, D.; Harden, S.M.; Zumbo, B.D.; Sylvester, B.D.; Kaulius, M.; Ruissen, G.R.; Dowd, A.J.; Beauchamp, M.R. The effectiveness of multi-component goal setting interventions for changing physical activity behaviour: A systematic review and meta-analysis. Health Psychol. Rev. 2015, 10, 67–88. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.M.; Kataoka-Yahiro, M. Themes in the Literature Related to Cardiovascular Disease Risk Reduction. J. Cardiovasc. Nurs. 2009, 24, 268–276. [Google Scholar] [CrossRef]
- Mifsud, J.L.; Galea, J.; Garside, J.; Stephenson, J.; Astin, F. Motivational interviewing to support modifiable risk factor change in individuals at increased risk of cardiovascular disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0241193. [Google Scholar] [CrossRef]
- Brown, V.A.; Bartholomew, L.K.; Naik, A.D. Management of chronic hypertension in older men: An exploration of patient goal-setting. Patient Educ. Couns. 2007, 69, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Vaalburg, A.M.; Wattel, E.; Boersma, P.; Hertogh, C.; Gobbens, R. Goal-setting in geriatric rehabilitation: Can the nursing profession meet patients’ needs? A narrative review. Nurs. Forum 2021, 56, 648–659. [Google Scholar] [CrossRef]
- Rose, A.; Rosewilliam, S.; Soundy, A. Shared decision making within goal setting in rehabilitation settings: A systematic review. Patient Educ. Couns. 2016, 100, 65–75. [Google Scholar] [CrossRef]
- Sugavanam, T.; Mead, G.; Bulley, C.; Donaghy, M.; Van Wijck, F. The effects and experiences of goal setting in stroke rehabilitation—A systematic review. Disabil. Rehabil. 2012, 35, 177–190. [Google Scholar] [CrossRef]
- D’Cruz, K.; Unsworth, C.; Roberts, K.; Morarty, J.; Turner-Stokes, L.; Wellington-Boyd, A.; Matchado, J.; Lannin, N.A. Engaging patients with moderate to severe acquired brain injury in goal setting. Int. J. Ther. Rehabil. 2016, 23, 20–31. [Google Scholar] [CrossRef]
- van der Kluit, M.J.; Dijkstra, G.J.; de Rooij, S.E. Goals of older hospitalised patients: A qualitative descriptive study. BMJ Open 2019, 9, e029993. [Google Scholar] [CrossRef] [Green Version]
- Holliday, R.C.; Ballinger, C.; Playford, E.D. Goal setting in neurological rehabilitation: Patients’ perspectives. Disabil. Rehabil. 2007, 29, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, B.; Slomic, M. Negotiating Goals: Exploring the Dialogue Between Professionals and Patients in Team-Meetings. Prof. Prof. 2021, 11. [Google Scholar] [CrossRef]
- Draaistra, H.; Singh, M.D.; Ireland, S.; Harper, T. Patients’ perceptions of their roles in goal setting in a spinal cord injury regional rehabilitation program. Can. J. Neurosci. Nurs. 2012, 34, 22–30. [Google Scholar] [PubMed]
- Mowrer, J.L.; Tapp, H.; Ludden, T.; Kuhn, L.; Taylor, Y.; Courtlandt, C.; Alkhazraji, T.; Reeves, K.; Steuerwald, M.; Andrew, M.; et al. Patients’ and providers’ perceptions of asthma and asthma care: A qualitative study. J. Asthma 2015, 52, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Morris, H.L.; Carlyle, K.E.; Elston Lafata, J. Adding the patient’s voice to our understanding of collaborative goal setting: How do patients with diabetes define collaborative goal setting? Chronic Illn. 2016, 12, 261–271. [Google Scholar] [CrossRef]
- Nelis, S.M.; Thom, J.M.; Jones, I.; Hindle, J.V.; Clare, L. Goal-setting to Promote a Healthier Lifestyle in Later Life: Qualitative Evaluation of the AgeWell Trial. Clin. Gerontol. 2017, 41, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Siegert, R.J.; Taylor, W.J. Theoretical aspects of goal-setting and motivation in rehabilitation. Disabil. Rehabil. 2004, 26, 1–8. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care. Circulation 2008, 117, 743–753. Available online: https://www.ahajournals.org/doi/abs/10.1161/circulationaha.107.699579 (accessed on 24 April 2022). [CrossRef]
- Body Mass Index (BMI) Nomogram—Canada.ca. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/healthy-weights/canadian-guidelines-body-weight-classification-adults/body-mass-index-nomogram.html (accessed on 8 December 2022).
- Bodenheimer, T.; Handley, M.A. Goal-setting for behavior change in primary care: An exploration and status report. Patient Educ. Couns. 2009, 76, 174–180. [Google Scholar] [CrossRef] [PubMed]
- LaBrie, J.W.; Quinlan, T.; Schiffman, J.E.; Earleywine, M.E. Performance of Alcohol and Safer Sex Change Rulers Compared with Readiness to Change Questionnaires. Psychol. Addict. Behav. 2005, 19, 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabi, D.M.; McBrien, K.A.; Sapir-Pichhadze, R.; Nakhla, M.; Ahmed, S.B.; Dumanski, S.M.; Butalia, S.; Leung, A.A.; Harris, K.C.; Cloutier, L.; et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2020, 36, 596–624. [Google Scholar] [CrossRef] [PubMed]
- Bryman, A. Social Research Methods, 5th ed.; Oxford Press: London, UK, 2015. [Google Scholar]
- Laddu, D.; Ma, J.; Kaar, J.; Ozemek, C.; Durant, R.W.; Campbell, T.; Welsh, J.; Turrise, S. Health Behavior Change Programs in Primary Care and Community Practices for Cardiovascular Disease Prevention and Risk Factor Management Among Midlife and Older Adults: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e533–e549. Available online: https://pubmed.ncbi.nlm.nih.gov/34732063/ (accessed on 5 May 2022). [CrossRef]
- Hunter, C.; Chew-Graham, C.A.; Langer, S.; Drinkwater, J.; Stenhoff, A.; Guthrie, E.A.; Salmon, P. “I wouldn’t push that further because I don’t want to lose her”: A multiperspective qualitative study of behaviour change for long-term conditions in primary care. Health Expect. 2015, 18, 1995–2010. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, K.; Handley, M.; Wong, S.; Sharifi, C.; Gjeltema, K.; Schillinger, D.; Bodenheimer, T. Behavior-change action plans in primary care: A feasibility study of clinicians. J. Am. Board Fam. Med. 2006, 19, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Paxton, R.J.; Taylor, W.C.; Hudnall, G.E.; Christie, J. Goal Setting to Promote a Health Lifestyle. Int. Proc. Chem. Biol. Environ Eng. 2012, 39, 101. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3904755/ (accessed on 1 September 2022).
- Elmer, P.J.; Obarzanek, E.; Vollmer, W.M.; Simons-Morton, D.; Stevens, V.J.; Young, D.R.; Lin, P.-H.; Champagne, C.; Harsha, D.W.; Svetkey, L.P.; et al. Effects of Comprehensive Lifestyle Modification on Diet, Weight, Physical Fitness, and Blood Pressure Control: 18-Month Results of a Randomized Trial. Ann. Intern. Med. 2006, 144, 485–495. [Google Scholar] [CrossRef]
- Fleig, L.; Küper, C.; Lippke, S.; Schwarzer, R.; Wiedemann, A.U. Cross-behavior associations and multiple health behavior change: A longitudinal study on physical activity and fruit and vegetable intake. J. Health Psychol. 2015, 20, 525–534. Available online: https://journals.sagepub.com/doi/10.1177/1359105315574951 (accessed on 1 September 2022). [CrossRef] [Green Version]
- Whitehead, L.; Glass, C.C.; Abel, S.L.; Sharp, K.; Coppell, K.J. Exploring the role of goal setting in weight loss for adults recently diagnosed with pre-diabetes. BMC Nurs. 2020, 19, 1–7. [Google Scholar] [CrossRef]
- Mosca, L.; Hammond, G.; Mochari-Greenberger, H.; Towfighi, A.; Albert, M.A. Fifteen-year trends in awareness of heart disease in women: Results of a 2012 American Heart Association national survey. Circulation 2013, 127, 1254–1263. Available online: https://www.ahajournals.org/doi/abs/10.1161/CIR.0b013e318287cf2f (accessed on 5 September 2022). [CrossRef] [PubMed]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2018, 9, 147–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mailey, E.L.; Huberty, J.; Dinkel, D.; McAuley, E. Physical activity barriers and facilitators among working mothers and fathers. BMC Public Health 2014, 14, 657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lara, J.; McCrum, L.-A.; Mathers, J.C. Association of Mediterranean diet and other health behaviours with barriers to healthy eating and perceived health among British adults of retirement age. Maturitas 2014, 79, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.; Kafchinski, M.; Vrazel, J.; Sullivan, P. Motivators, Barriers, and Beliefs Regarding Physical Activity in an Older Adult Population. J. Geriatr. Phys. Ther. 2011, 34, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.B.; Leppin, A.; Jarbøl, D.E.; Søndergaard, J.; Larsen, P.V. Barriers to lifestyle changes for prevention of cardiovascular disease—A survey among 40–60-year old Danes. BMC Cardiovasc. Disord. 2017, 17, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQuaiz, A.M.; Tayel, S.A. Barriers to a healthy lifestyle among patients attending primary care clinics at a university hospital in Riyadh. Ann. Saudi Med. 2009, 29, 30–35. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | Frequency (%)/Mean (SD)/Median (IQR) |
|---|---|
| Age | 57 years (5.7) |
| Male | 13 (87%) |
| Family History of CVD | 6 (40%) |
| Job title | |
| Library and Information technology (IT) | 7 (46%) |
| Research | 2 (16%) |
| Administration and other staff | 7 (38%) |
| Weight (kg) | 86.4 (13.3) |
| Height (cm) | 172.9 (10.4) |
| Body mass index, BMI (kg/m2) | 28.1 (3.82) |
| Waist circumference (cm) | 99 (18) |
| Males | 99 (14.5) |
| Females | 98.5 (NA) |
| Weight status | |
| Underweight (<18.5 kg/m2) | 0 (0%) |
| Normal (18.5–24.9 kg/m2) | 4 (29%) |
| Overweight (25.0–29.9 kg/m2) | 3 (21%) |
| Obese (≥30.0 kg/m2) | 7 (50%) |
| Blood pressure (mm Hg) | |
| Systolic (SBP) | 129 (17) |
| Diastolic (DBP) | 84.5 (6) |
| Triglycerides | 2.0 (0.24) |
| High-density lipoprotein (HDL) | 1.11 (0.29) |
| Low-density lipoprotein (LDL) | 3.35 (0.72) |
| Total cholesterol | 5.36 (1.02) |
| Framingham Risk Score (FRS) | 18.3 (5.8) |
| Level of cardiac risk | |
| Moderate (10–19%) | 11 (73%) |
| High (20% and above) | 4 (27%) |
| Hypertensive (AOBP > 135/85 mm Hg) | |
| Yes | 4 (29%) |
| No | 10 (71%) |
| Category | Goal | Frequency of Reported Goal | Subgoal | Frequency of Reported Goal * |
|---|---|---|---|---|
| Health Behaviour | ||||
| Diet | Change Quantity | 25 | Reduce red meat intake | 4 |
| Reduce processed/convenience food intake | 2 | |||
| Reduce salt intake | 2 | |||
| Reduce sugary food intake | 3 | |||
| Reduce carbohydrate intake | 4 | |||
| Increase water intake | 1 | |||
| Increase vegetable intake | 9 | |||
| Change Timing/Frequency | 1 | Eat earlier in the evening | 1 | |
| Improve Quality | 9 | Incorporate heart healthy foods and fats | 4 | |
| Follow diet models (ex. Mediterranean diet, Healthy plate model) | 5 | |||
| Physical Activity | Increase Quantity | 12 | Increase frequency | 9 |
| Increase duration | 3 | |||
| Change Timing (leisure-based vs. transport-based) | 6 | Increase intensity | 4 | |
| Increase outdoor exercise | 2 | |||
| Smoking | Smoking Cessation | 2 | Stop Cold Turkey | 2 |
| Medication use | Optimize Medication Therapy | 2 | Start Medication | 1 |
| Adhere to Medication | 1 | |||
| Sleep | Improve Sleep Quality | 1 | Avoid fluids late in the evening before bed | 1 |
| Get to bed earlier | 1 | |||
| Alcohol | Reduce Alcohol Intake | 3 | Reduce Alcohol Intake | 3 |
| Health measure | ||||
| Weight | Reduce Weight Measures | 6 | Reduce Weight Measures | 6 |
| Blood pressure | Reduce Blood Pressure Readings | 3 | Reduce Blood Pressure Readings | 3 |
| Lipids | Improve Cholesterol Levels Reduce | 5 | Triglyceride and LDL Cholesterol Levels | 4 |
| Increase HDL Cholesterol Levels | 1 |
| Goal Barriers | Description | Example |
|---|---|---|
| Physical (bodily) limitation | Patients report that physical limits of their body do not permit them to move forward in their pursuit of their goal (e.g., Injury, recovery from surgery, illness) | “Recovering from hip surgery” |
| Physical (external) limitation | Patients report that physical factors from the outside world limit their opportunities to carry out their behavioural goal activities (e.g. COVID-19 pandemic, change in weather, health provider assessment required) | “physical activity has reduced due to weather—no gardening or yard work” “limited w/COVID as cannot go to gym” |
| Time limitation | Patients report that time constraints limit their ability to carry out behavioural goal activities | “Getting busy with work, no time to prepare healthy snacks” |
| Psychological limitation (lack of motivation, cravings, biases) | Patients report that there are psychological barriers which render them unable to make progress. | “trouble getting out of bed in the morning for exercise” “Finding it somewhat difficult to stick with this, feels he is craving salt more” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaassen, A.E.; Kapanen, A.I.; Zed, P.J.; Conklin, A.I. Setting Goals to Reduce Cardiovascular Risk: A Retrospective Chart Review of a Pharmacist-Led Initiative in the Workplace. Int. J. Environ. Res. Public Health 2023, 20, 846. https://doi.org/10.3390/ijerph20010846
Klaassen AE, Kapanen AI, Zed PJ, Conklin AI. Setting Goals to Reduce Cardiovascular Risk: A Retrospective Chart Review of a Pharmacist-Led Initiative in the Workplace. International Journal of Environmental Research and Public Health. 2023; 20(1):846. https://doi.org/10.3390/ijerph20010846
Chicago/Turabian StyleKlaassen, Alicia E., Anita I. Kapanen, Peter J. Zed, and Annalijn I. Conklin. 2023. "Setting Goals to Reduce Cardiovascular Risk: A Retrospective Chart Review of a Pharmacist-Led Initiative in the Workplace" International Journal of Environmental Research and Public Health 20, no. 1: 846. https://doi.org/10.3390/ijerph20010846