
Greater Risk of Pregnancy Complications for Female Surgeons: A Cross-Sectional Electronic Survey
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
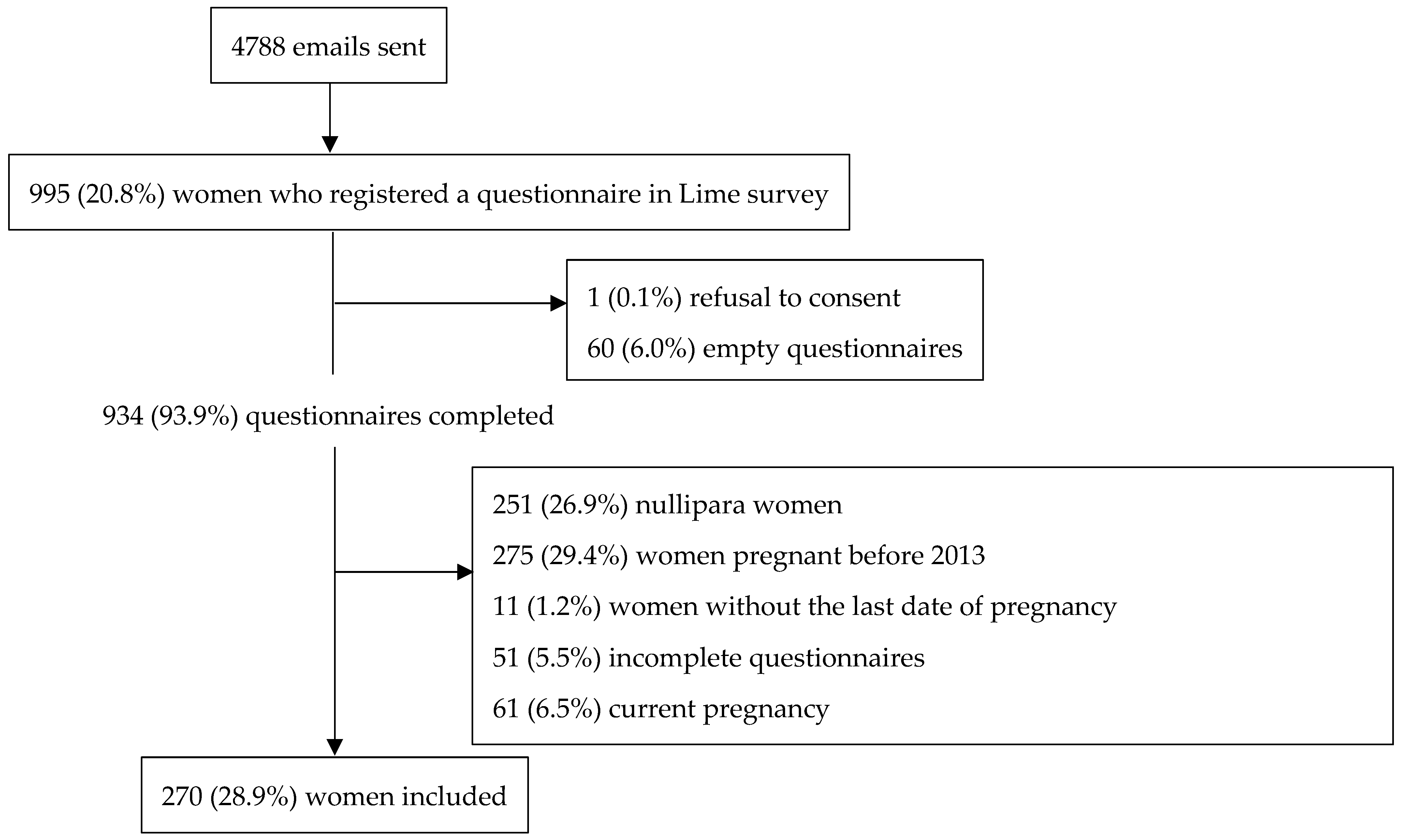
2.1. Study Cohort and Design
2.2. Outcome
2.3. Exposure
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Summary of the Study Findings
4.2. Comparison with Other Studies
4.3. Explanation of Findings
4.4. Strengths and Limitations
4.5. Implications for Healthcare Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, S. Occupational, environmental and lifestyle factors associated with spontaneous abortion. Reprod. Sci. 2011, 18, 915–930. [Google Scholar] [CrossRef] [PubMed]
- Chudnovets, A.; Liu, J.; Narasimhan, H.; Liu, Y.; Burd, I. Role of Inflammation in Virus Pathogenesis during Pregnancy. J. Virol. 2020, 95, e01381-19. [Google Scholar] [CrossRef] [PubMed]
- Bonzini, M.; Coggon, D.; Palmer, K.T. Risk of prematurity, low birthweight and pre-eclampsia in relation to working hours and physical activities: A systematic review. Occup. Environ. Med. 2007, 64, 228–243. [Google Scholar] [CrossRef] [Green Version]
- De Santis, M.; Cesari, E.; Nobili, E.; Straface, G.; Cavaliere, A.F.; Caruso, A. Radiation effects on development. Birth Defects Res. Part C Embryo Today 2007, 81, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Dranitsaris, G.; Johnston, M.; Poirier, S.; Schueller, T.; Milliken, D.; Green, E.; Zanke, B. Are health care providers who work with cancer drugs at an increased risk for toxic events? A systematic review and meta-analysis of the literature. J. Oncol. Pharm. Pract. 2005, 11, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.C.; Rocheleau, C.M.; Whelan, E.A.; Lividoti Hibert, E.N.; Grajewski, B.; Spiegelman, D.; Rich-Edwards, J.W. Occupational exposures among nurses and risk of spontaneous abortion. Am. J. Obstet. Gynecol. 2012, 206, 327.e1–327.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warembourg, C.; Cordier, S.; Garlantézec, R. An update systematic review of fetal death, congenital anomalies, and fertility disorders among health care workers. Am. J. Ind. Med. 2017, 60, 578–590. [Google Scholar] [CrossRef]
- Bonzini, M.; Palmer, K.T.; Coggon, D.; Carugno, M.; Cromi, A.; Ferrario, M.M. Shift work and pregnancy outcomes: A systematic review with meta-analysis of currently available epidemiological studies. BJOG 2011, 118, 1429–1437. [Google Scholar] [CrossRef] [Green Version]
- Lawson, C.C.; Whelan, E.A.; Hibert, E.N.; Grajewski, B.; Spiegelman, D.; Rich-Edwards, J.W. Occupational factors and risk of preterm birth in nurses. Am. J. Obstet. Gynecol. 2009, 200, 51.e1–51.e8. [Google Scholar] [CrossRef] [Green Version]
- Casilla-Lennon, M.; Hanchuk, S.; Zheng, S.; Kim, D.D.; Press, B.; Nguyen, J.V.; Grimshaw, A.; Leapman, M.S.; Cavallo, J.A. Pregnancy in physicians: A scoping review. Am. J. Surg. 2022, 223, 36–46. [Google Scholar] [CrossRef]
- Rangel, E.L.; Castillo-Angeles, M.; Easter, S.R.; Atkinson, R.B.; Gosain, A.; Hu, Y.Y.; Cooper, Z.; Dey, T.; Kim, E. Incidence of Infertility and Pregnancy Complications in US Female Surgeons. JAMA Surg. 2021, 156, 905. [Google Scholar] [CrossRef] [PubMed]
- Scully, R.E.; Stagg, A.R.; Melnitchouk, N.; Davids, J.S. Pregnancy outcomes in female physicians in procedural versus non-procedural specialties. Am. J. Surg. 2017, 214, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.C.; McNamara, D.A. Pregnancy and the Surgeon-Too Many Opinions, Too Little Evidence. JAMA Surg. 2017, 152, 997–998. [Google Scholar] [CrossRef]
- Briggs, G.G.; Freeman, R.K.; Yaffe, S.J. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Katz, V.L. Work and work-related stress in pregnancy. Clin. Obstet. Gynecol. 2012, 55, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Korkmaz, A.; Rosales-Corral, S.A. Melatonin and stable circadian rhythms optimize maternal, placental and fetal physiology. Hum. Reprod. Update 2013, 20, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Lerner, L.B.; Stolzmann, K.L.; Gulla, V.D. Birth trends and pregnancy complications among women urologists. J. Am. Coll. Surg. 2009, 208, 293–297. [Google Scholar] [CrossRef]
- Hamilton, A.R.; Tyson, M.D.; Braga, J.A.; Lerner, L.B. Childbearing and pregnancy characteristics of female orthopaedic surgeons. J. Bone Jt. Surg. 2012, 94, e77. [Google Scholar] [CrossRef]
- Croteau, A.; Marcoux, S.; Brisson, C. Work activity in pregnancy, preventive measures, and the risk of delivering a small-for-gestational-age infant. Am. J. Public Health 2006, 96, 846–855. [Google Scholar] [CrossRef]
- Niedhammer, I.; O’Mahony, D.; Daly, S.; Morrison, J.J.; Kelleher, C.C. Occupational predictors of pregnancy outcomes in Irish working women in the Lifeways cohort. BJOG 2009, 116, 943–952. [Google Scholar] [CrossRef] [Green Version]
- Blondel, B.; Gonzalez, L.; Raynaud, P. Enquête Nationale Périnatale Rapport 2016; INSERM (Institut National de la Santé et de la Recherche Médicale): Paris, France, 2017. [Google Scholar]
- Demiguel, V.; Blondel, B.; Bonnet, C.; Nguyen-Thanh, V.; Saurel-Cubizolles, M.-J.; Regnault, N. Trends in Tobacco Smoking in Pregnant Women: Data from French National Perinatal Surveys. Int. J. Public Health 2021, 66, 602873. [Google Scholar] [CrossRef]
- Ward, C.; Lewis, S.; Coleman, T. Prevalence of maternal smoking and environmental tobacco smoke exposure during pregnancy and impact on birth weight: Retrospective study using Millennium Cohort. BMC Public Health 2007, 7, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauer, L.; Miller, D.; Schueler, B.; Silberzweig, J.; Balter, S.; Bartal, G.; Chambers, C.; Collins, J.; Damilakis, J.; Dixon, R. Society of Interventional Radiology Safety and Health Committee. Cardiovascular and Interventional Radiological Society of Europe Standards of Practice Committee Occupational radiation protection of pregnant or potentially pregnant workers in IR: A joint guideline of the Society of Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2015, 26, 171–181. [Google Scholar] [PubMed]
- Anderson, M.; Goldman, R.H. Occupational Reproductive Hazards for Female Surgeons in the Operating Room: A Review. JAMA Surg. 2020, 155, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Ghatan, C.E.; Fassiotto, M.; Jacobsen, J.P.; Sze, D.Y.; Kothary, N. Occupational Radiation Exposure during Pregnancy: A Survey of Attitudes and Practices among Interventional Radiologists. J. Vasc. Interv. Radiol. 2016, 27, 1013–1020.e3. [Google Scholar] [CrossRef] [Green Version]
- Downes, J.; Rauk, P.N.; VanHeest, A.E. Occupational hazards for pregnant or lactating women in the orthopaedic operating room. J. Am. Acad. Orthop. Surg. 2014, 22, 326–332. [Google Scholar] [CrossRef]
- Norton, P.; Pinho, P.; Xará, D.; Pina, F.; Norton, M. Assessment of anesthetic gases in a central hospital. Porto Biomed. J. 2020, 5, e076. [Google Scholar] [CrossRef]
- Manangama, G.; Audignon-Durand, S.; Migault, L.; Gramond, C.; Zaros, C.; Teysseire, R.; Sentilhes, L.; Brochard, P.; Lacourt, A.; Delva, F. Maternal occupational exposure to carbonaceous nanoscale particles and small for gestational age and the evolution of head circumference in the French Longitudinal Study of Children-Elfe study. Environ. Res. 2020, 185, 109394. [Google Scholar] [CrossRef]
- Hougaard, K.S.; Campagnolo, L.; Chavatte-Palmer, P.; Tarrade, A.; Rousseau-Ralliard, D.; Valentino, S.; Park, M.V.; de Jong, W.H.; Wolterink, G.; Piersma, A.H. A perspective on the developmental toxicity of inhaled nanoparticles. Reprod. Toxicol. 2015, 56, 118–140. [Google Scholar] [CrossRef]
- Conseil National de l’Ordre des Médeccins. Atlas de la Démographie Médicale en France. Situation au 1er Janvier 2018. Available online: https://www.conseil-national.medecin.fr/sites/default/files/external-package/analyse_etude/hb1htw/cnom_atlas_2018_0.pdf (accessed on 12 August 2021).
- Fritze-Büttner, F.; Toth, B.; Bühren, A.; Schlosser, K.; Schierholz, S.; Rumpel, B.; Helm, P.C.; Bauer, U.M.M.; Niethard, M.; Prediger, S.; et al. Surgery during pregnancy—Results of a German questionnaire. Innov. Surg. Sci. 2020, 5, 21–26. [Google Scholar] [CrossRef]
- Sorouri, K.; Khan, S.; Bowden, S.; Searle, S.; Carr, L.; Simpson, J.S. The Glaring Gender Bias in the Operating Room: A Qualitative Study of Factors Influencing Career Selection for First-Year Medical Students. J. Surg. Educ. 2021, 78, 1516–1523. [Google Scholar] [CrossRef]


{kind=link}
| Other Specialties N = 242 N (%) | Surgeon N = 28 N (%) | p-Value | |
|---|---|---|---|
| Age at last pregnancy Mean (Standard Deviation) | 34.5 (4.0) | 33.8 (3.5) | 0.27 |
| Age ≥ 35 years | 99 (40.9) | 13 (46.4) | 0.57 |
| Primiparous | 63 (26.0) | 7 (25.0) | 0.90 |
| Obstetrical history * | 61 (25.2) | 10 (35.7) | 0.23 |
| Surgical or medical history ** | 70 (28.9) | 6 (21.4) | 0.40 |
| Active smoking | 13 (5.4) | 2 (7.1) | 0.70 |
| Alcohol | 18 (7.4) | 3 (10.7) | 0.54 |
| Four or more physical or organizational constraints | 10 (4.1) | 4 (14.3) | 0.04 |
| On call duty in the 2nd and 3rd trimesters of pregnancy | 69 (28.5) | 17 (60.7) | 0.0005 |
| Home visits in the 2nd and 3rd trimesters of pregnancy | 91 (37.6) | 0 (0.0) | <0.0001 |
| Prolonged standing in the 2 and 3rd trimesters of pregnancy | 84 (34.7) | 17 (60.7) | 0.007 |
| Work > 42 h/week in the 2nd and 3rd trimesters of pregnancy | 113 (46.7) | 19 (67.9) | 0.04 |
| Heavy loads in the 2nd and 3rd trimesters of pregnancy | 14 (5.8) | 5 (17.9) | 0.03 |
| Teratogen infection during pregnancy *** | 4 (1.6) | 1 (3.6) | 0.47 |
| Exposure to at least one chemical agent | 50 (20.7) | 23 (82.1) | <0.0001 |
| Exposure to a cytostatic | 8 (3.3) | 2 (7.1) | 0.31 |
| Exposure to anesthetic gases | 10 (4.1) | 19 (67.9) | <0.0001 |
| Exposure to nitrous oxide | 43 (17.8) | 17 (60.7) | <0.0001 |
| Exposure to ionizing radiation | 21 (5.4) | 12 (42.9) | <0.0001 |
| Total Population | Female Surgeons | Other Specialities | ||
|---|---|---|---|---|
| Pregnancy Complication | N (%) | N (%) | N (%) | p-Value |
| Miscarriage | 16 (5.9) | 1 (3.6) | 15 (6.2) | 0.5 |
| Extra-uterine pregnancy | 4 (1.5) | 0 (0.0) | 4 (1.6) | 1.0 |
| Fetal growth restriction | 27 (10.0) | 8 (28.6) | 19 (7.8) | 0.003 |
| Prematurity | 6 (2.2) | 4 (14.3) | 2 (0.8) | 0.001 |
| Fetal congenital malformation | 2 (0.7) | 0 (0.0) | 2 (0.8) | 1.0 |
| Stillbirth | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Medical termination of pregnancy | 1 (0.4) | 0 (0.0) | 1 (0.4) | 1.0 |
| OR | 95% CI | p | |
|---|---|---|---|
| Surgery specialty (ref other specialties) | 3.17 | [1.38–7.27] | 6 |
| Age ≥ 35 years | 1.27 | [0.69–2.33] | 0.44 |
| Primiparous | 0.83 | [0.41–1.69] | 0.60 |
| Four or more physical or organizational constraints | 2.47 | [0.79–7.71] | 0.12 |
| Teratogen infection during pregnancy | 2.87 | [0.47–17.6] | 0.25 |
| Exposure to at least one chemical agent | 1.25 | [0.64–2.43] | 0.50 |
| Exposure to ionizing radiation | 0.77 | [0.41–1.46] | 0.42 |
| Active smoking | 1.57 | [0.48–5.14] | 0.45 |
| Alcohol | 0.98 | [0.32–3.06] | 0.98 |
| Surgical or medical history | 1.04 | [0.53–2.04] | 0.90 |
| Obstetrical history | 1.84 | [0.97–3.50] | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delva, F.; Carcasset, P.; Mouton, P.; Auguste-Virginie, R.; Lairez, F.; Sentilhes, L.; Brochard, P.; Joseph, J.-P. Greater Risk of Pregnancy Complications for Female Surgeons: A Cross-Sectional Electronic Survey. Int. J. Environ. Res. Public Health 2023, 20, 125. https://doi.org/10.3390/ijerph20010125
Delva F, Carcasset P, Mouton P, Auguste-Virginie R, Lairez F, Sentilhes L, Brochard P, Joseph J-P. Greater Risk of Pregnancy Complications for Female Surgeons: A Cross-Sectional Electronic Survey. International Journal of Environmental Research and Public Health. 2023; 20(1):125. https://doi.org/10.3390/ijerph20010125
Chicago/Turabian StyleDelva, Fleur, Pierre Carcasset, Pauline Mouton, Rivana Auguste-Virginie, Fanny Lairez, Loïc Sentilhes, Patrick Brochard, and Jean-Philippe Joseph. 2023. "Greater Risk of Pregnancy Complications for Female Surgeons: A Cross-Sectional Electronic Survey" International Journal of Environmental Research and Public Health 20, no. 1: 125. https://doi.org/10.3390/ijerph20010125