
School Feeding as a Protective Factor against Insulin Resistance: The Study of Cardiovascular Risks in Adolescents (ERICA)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
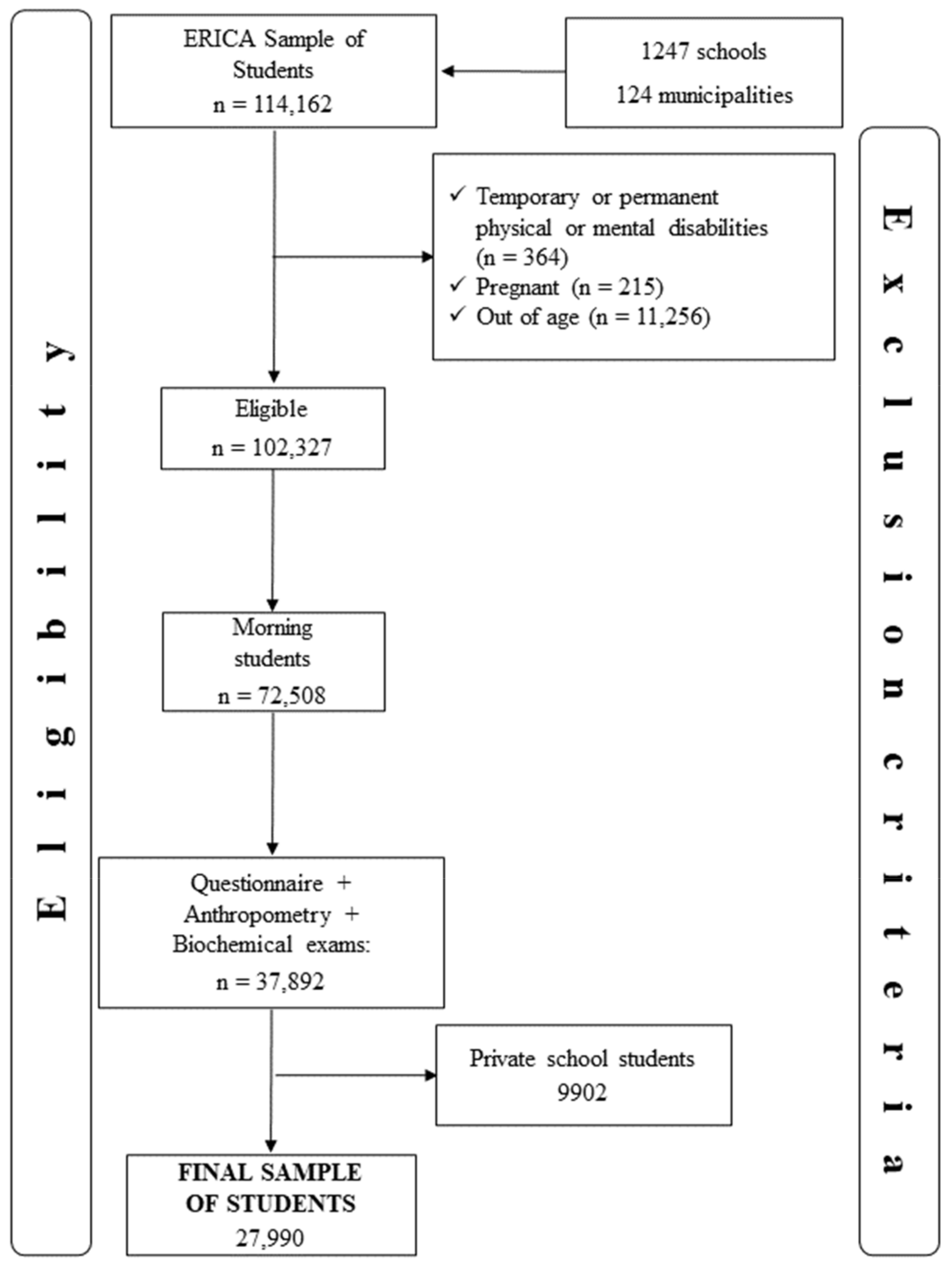
2.2. Setting and Participants
2.3. Variables and Categories
2.4. Insulin Resistance Markers (Outcome)
2.5. Contextual Characteristics (Exposure Variables Related to School)
2.6. Individual Characteristics (Exposure Variable Related to School)
2.7. Individual Characteristics (Confounders)
2.8. Statistical Analysis
2.9. Ethical Aspects
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- WHO. Nutrition in Adolescence—Issues and Challenges for the Health Sector; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Goncalves, V.S.; Duarte, E.C.; Dutra, E.S.; Barufaldi, L.A.; Carvalho, K.M. Characteristics of the school food environment associated with hypertension and obesity in Brazilian adolescents: A multilevel analysis of the Study of Cardiovascular Risks in Adolescents (ERICA). Public Health Nutr. 2019, 22, 2625–2634. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Pouliou, T.; Murphy, S.; Waters, E.; A Komro, K.; Gibbs, L.; Magnus, D.; Campbell, R. The World Health Organization’s Health Promoting Schools framework: A Cochrane systematic review and meta-analysis. BMC Public Health 2015, 15, 130. [Google Scholar] [CrossRef] [PubMed]
- Welker, E.; Lott, M.; Story, M. The School Food Environment and Obesity Prevention: Progress Over the Last Decade. Curr. Obes. Rep. 2016, 5, 145–155. [Google Scholar] [CrossRef]
- BRASIL. Lei N 11.947, de 16 de JUNHO de 2009. Atualizada pelas Leis n 12.982 de 28 de maio de 2014 e 12.695, de julho de 2012. Conversão da Medida Provisória no 455, de 2008 2009. Available online: https://www.planalto.gov.br/ccivil_03/_ato2007-2010/2009/lei/l11947.htm (accessed on 4 May 2020).
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Peñalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Da Silva, T.P.R.; Matozinhos, F.P.; Gratão, L.H.A.; Rocha, L.L.; Vilela, L.A.; de Oliveira, T.R.P.R.; Cunha, C.D.F.; Mendes, L.L. Coexistence of risk factors for cardiovascular diseases among Brazilian adolescents: Individual characteristics and school environment. PLoS ONE 2021, 16, e0254838. [Google Scholar]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Kuschnir, M.C.C.; Bloch, K.V.; Szklo, M.; Klein, C.H.; Barufaldi, L.A.; Abreu, G.D.A.; Schaan, B.; Veiga, G.V.D.; Silva, T.L.N.D.; De Vasconcellos, M.T.; et al. ERICA: Prevalence of metabolic syndrome in Brazilian adolescents. Rev. Saude Publ. 2016, 50, 1–13. [Google Scholar] [CrossRef]
- Chissini, R.D.B.C.; Kuschnir, M.C.; de Oliveira, C.L.; Giannini, D.T.; Santos, B. Cutoff values for HOMA-IR associated with metabolic syndrome in the Study of Cardiovascular Risk in Adolescents (ERICA Study). Nutrition 2020, 71, 110608. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [Green Version]
- Bloch, K.V.; Szklo, M.; Kuschnir, M.C.C.; De Azevedo, A.G.; Barufaldi, L.A.; Klein, C.H.; De Vasconcelos, M.T.L.; Veiga, J.P.C.B.; Figueiredo, V.C.; Dias, A.; et al. The study of cardiovascular risk in adolescents—ERICA: Rationale, design and sample characteristics of a national survey examining cardiovascular risk factor profile in Brazilian adolescents. BMC Public Health 2015, 15, 94. [Google Scholar]
- Vasconcellos, M.T.L.; do Silva, P.L.N.; Szklo, M.; Kuschnir, M.C.C.; Klein, C.H.; De Abreu, G.A.; Barufaldi, L.A.; Bloch, K.V. Desenho da amostra do Estudo de Riscos Cardiovasculares em Adolescentes (ERICA). Cad. Saude Publ. 2015, 31, 921–930. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- De Carvalho, M.H.C. I Diretriz Brasileira de Diagnóstio Tratamento da Síndrome Metabólica. Arq. Bras. Cardiol. 2005, 84, 1–28. [Google Scholar]
- Tanner, J.M. Growth at Adolescence; Blackwell Scientific Publications: Hoboken, NJ, USA, 1962. [Google Scholar]
- Farias Júnior, J.C.D.; Lopes, A.D.S.; Mota, J.; Santos, M.P.; Ribeiro, J.C.; Hallal, P.C. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: Uma adaptação do Self—Administered Physical Activity Checklist. Rev. Bras. Epidemiol. 2012, 15, 198–210. [Google Scholar] [CrossRef]
- Laird, N.M.; Ware, J.H. Random-Effects Models for Longitudinal Data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Rabe-Hesketh, S.; Skrondal, A. Multilevel modelling of complex survey data. J. R. Stat. Soc. Ser. 2006, 169, 805–827. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behavior change: A systematic review of behavior theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and environmental influences on adolescent eating behaviors. Am. Diet. Assoc. 2002, 102, S40–S51. [Google Scholar] [CrossRef]
- De Assunção Bezerra, M.K.; Freese De Carvalho, E.; Souza Oliveira, J.; Pessoa Cesse, E.Â.; De Lira, P.I.C.; Cavalcante, J.G.T.; Leal, V.S. Health promotion initiatives at school related to overweight, insulin resistance, hypertension and dyslipidemia in adolescents: A cross-sectional study in Recife, Brazil. BMC Public Health 2018, 18, 223. [Google Scholar] [CrossRef]
- Deboer, M.D. Assessing and managing the metabolic syndrome in children and adolescents. Nutrients 2019, 11, 1788. [Google Scholar] [CrossRef] [Green Version]
- Sociedade Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes 2019–2020; Editora científica Clannad: São Paulo, Brazil, 2020. [Google Scholar]
- Sociedade Brasileira de Diabetes. Pesquisa Nacional de Saúde do Escolar: 2015; Instituto Brasileiro de Geografia e Estatística—IBGE: Rio de Janeiro, Brazil, 2015; Available online: https://ayanrafael.files.wordpress.com/2011/08/gil-a-c-mc3a9todos-e-tc3a9cnicas-de-pesquisa-social.pdf (accessed on 14 April 2020).
- De Andrade, M.I.S.; Oliveira, J.S.; Leal, V.S.; Cabral, P.C.; De Lira, P.I.C. Independent predictors of insulin resistance in Brazilian adolescents: Results of the study of cardiovascular risk in adolescents-Brazil. PLoS ONE 2021, 16, e0246445. [Google Scholar] [CrossRef]
- American Diabetes Association. 13. Children and Adolescents: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S163–S182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Improving care and promoting health in populations: Standards of medical care in diabetes−2021. Diabetes Care 2021, 44, S7–S14. [Google Scholar]


{kind=link}
| Individual Characteristics | Environmental Characteristics |
|---|---|
| Age (<15 years/≥15 years) | Location school area (Rural/Urban) |
| Sexual maturation (advanced-stage Tanner’s) | Sale of food at school (Yes/No) |
| Waist circumference (<percentile >90/> percentile >90) | Presence of vending machines (Yes/No) |
| Physical activity (sufficiently active/insufficiently active) | Presence of advertising of industrialized foods (Yes/No) |
| Mother’s education (illiterate or elementary school incomplete, elementary or high school complete, complete or incomplete higher education, or does not know/does not remember) | Sale of food in the vicinity of the school (Yes/No) |
| Ethnicity/skin color (white, black, or brown, Asian, indigenous, and does not know/prefers not to answer) | |
| Self-reported consumption of meals prepared in school (Yes/No) | |
| Purchased food at school (Yes/No) | |
| Blood glucose levels (Normal/Undesirable) | |
| Insulin levels (Borderline/High insulin) | |
| HOMA-IR (Normal/High) |
| Individual Characteristic | Total (n = 27,990) | Male (n = 13,951) | Female (n = 14,039) | |||
|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | |
| Age ≥ 15 years | 53.4 | - | 53.0 | - | 53.8 | - |
| Advanced stage of sexual maturation a | 75.8 | 74.7–76.9 | 78.1 | 77.1–79.3 | 73.6 | 72.1–75.2 |
| Ethnicity/skin color | ||||||
| White | 35.4 | 33.0–37.9 | 35.4 | 33.1–38.3 | 35.4 | 33.1–38.0 |
| Black or brown | 59.7 | 57.6–61.8 | 58.5 | 56.0–63.2 | 61.0 | 59.0–63.2 |
| Asian | 1.9 | 1.5–2.3 | 1.9 | 1.4–2.5 | 1.9 | 1.5–2.3 |
| Indigenous | 0.7 | 0.5–0.9 | 0.9 | 0.7–1.4 | 0.4 | 0.3–0.5 |
| Does not know/prefers not to answer | 2.4 | 2.0–2.8 | 3.3 | 2.7–4.0 | 1.4 | 1.1–1.8 |
| Mother’s education | ||||||
| Illiterate or ES incomplete | 23.0 | 20.5–25.8 | 23.1 | 19.5–27.0 | 23.0 | 21.2–25.0 |
| ES or HS complete | 33.5 | 31.4–35.6 | 32.1 | 29.3–35.0 | 35.1 | 33.1–37.0 |
| Complete or incomplete HE | 14.2 | 12.8–15.7 | 15.2 | 13.3–17.3 | 13.2 | 11.7–15.1 |
| Does not know/does not remember | 29.3 | 27.8–30.8 | 30.1 | 27.6–32.0 | 29.1 | 27.3–30.6 |
| Consumption of school feeding | 62.4 | 59.9–64.8 | 64.4 | 61.2–68.0 | 60.3 | 57.4–63.2 |
| Purchase of foods at the school cafeteria | 62.8 | 57.9–67.4 | 64.7 | 59.4–69.5 | 60.9 | 56.1–65.5 |
| Physically active b | 52.4 | 51.2–53.5 | 63.8 | 62.2–65.4 | 41.1 | 39.3–43.1 |
| Central obesity (waist circumference c) | 11.2 | 10.2–12.3 | 11.2 | 9.9–12.6 | 11.2 | 9.9–12.6 |
| Borderline or high insulin e | 12.2 | 11.1–13.5 | 9.7 | 8.4–11.1 | 14.8 | 13.3–16.4 |
| High HOMA-IR d | 24.7 | 22.8–26.7 | 14.5 | 12.9–16.4 | 35.1 | 32.1–37.5 |
| Undesirable blood glucose f | 4.6 | 3.8–5.4 | 6.2 | 4.9–7.7 | 3.1 | 2.4–3.7 |
| Characteristic | Public Schools (% Students) | |
|---|---|---|
| % | 95% CI | |
| School location area | ||
| Rural area | 6.1 | 1.8–19.1 |
| Urban area | 93.9 | 80.9–98.2 |
| School foods environment | ||
| Sale of food at school | 42.9 | 35.9–50.3 |
| Sweets, candies, lollipops, chocolates, etc. | 35.0 | 28.5–42.1 |
| Sweet or salty cookies | 30.7 | 25.3–36.6 |
| Soft drinks | 32.4 | 27.1–38.3 |
| Natural guarana | 8.9 | 6.7–11.8 |
| Snacks (fried or baked) | 38.3 | 31.5–45.6 |
| Sandwiches and/or pizza | 27.9 | 22.0–34.7 |
| Sale of food in school vending machines | 5.2 | 3.3–7.9 |
| Food | 1.1 | 0.6–1.7 |
| Drinks | 3.6 | 1.9–6.5 |
| Food and drinks | 0.5 | 0.2–1.3 |
| Advertisement of industrialized foods at school | 3.0 | 1.8–4.8 |
| Sweets, candies, lollipops, chocolates, etc. | 1.3 | 0.8–2.2 |
| Sweet or salty cookies | 1.0 | 0.2–3.3 |
| Soft drinks | 1.7 | 1.1–2.8 |
| Sandwiches and/or pizza | 0.08 | 0.02–0.3 |
| Noncarbonated sugary drinks (mate, tea, isotonic, natural guarana) | 0.7 | 0.3–1.6 |
| Others | 1.1 | 0.4–3.3 |
| Sale of food in the school’s immediate vicinity | 52.3 | 46.6–58.9 |
| Food | 28.6 | 23.6–34.3 |
| Drinks | 3.9 | 2.2–7.0 |
| Food and drinks | 19.8 | 15.6–24.7 |
| Characteristics | Crude Analysis | Adjusted Analysis 1 | ||||
|---|---|---|---|---|---|---|
| Coef. | 95% CI | p-Value | Coef. | 95% CI | p-Value | |
| HOMA-IR | ||||||
| Contextual level | ||||||
| Sale of foods at school | 0.001 | −0.08; 0.08 | 0.970 | |||
| Sale of food in school vending machines | −0.037 | −0.21; 0.12 | 0.649 | |||
| Advertisement of industrialized foods at school | −0.097 | −0.28; 0.09 | 0.300 | |||
| Sale of food in the school’s immediate vicinity | −0.051 | −0.13; 0.03 | 0.210 | |||
| Individual level | ||||||
| Consumption of school feeding | −0.141 | −0.19; −0.09 | <0.0001 | −0.135 | −0.19; −0.08 | <0.0001 |
| Purchase of foods at the school cafeteria | 0.022 | −0.03; 0.08 | 0.447 | |||
| INSULIN | ||||||
| Contextual level | ||||||
| Sale of foods at school | 0.007 | −0.32; 0.33 | 0.967 | |||
| Sale of food in school vending machines | −0.200 | −0.87; 0.47 | 0.556 | |||
| Advertisement of industrialized foods at school | −0.301 | −1.06; 0.46 | 0.441 | |||
| Sale of food in the school’s immediate vicinity | −0.106 | −0.43; 0.22 | 0.521 | |||
| Individual level | ||||||
| Consumption of school feeding | −0.503 | −0.68; −0.32 | <0.0001 | −0.469 | −0.66; −0.28 | <0.0001 |
| Purchase of foods at the school cafeteria | 0.025 | −0.18; 0.24 | 0.813 | |||
| GLUCOSE | ||||||
| Contextual level | ||||||
| Sale of foods at school | −0.097 | −0.58; 0.39 | 0.695 | |||
| Sale of food in school vending machines | 0.171 | −0.83; 1.17 | 0.737 | |||
| Advertisement of industrialized foods at school | −0.637 | −1.78; 0.51 | 0.274 | |||
| Sale of food in the school’s immediate vicinity | −0.429 | −0.92; 0.06 | 0.084 | |||
| Individual level | ||||||
| Consumption of school feeding | −0.630 | −0.87; −0.39 | <0.0001 | −0.634 | −0.88; −0.39 | <0.0001 |
| Purchase of foods at the school cafeteria | 0.613 | 0.33; 0.89 | <0.0001 | 0.455 | 0.16; 0.75 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamura, A.B.; Gonçalves, V.S.S.; de Carvalho, K.M.B. School Feeding as a Protective Factor against Insulin Resistance: The Study of Cardiovascular Risks in Adolescents (ERICA). Int. J. Environ. Res. Public Health 2022, 19, 10551. https://doi.org/10.3390/ijerph191710551
Okamura AB, Gonçalves VSS, de Carvalho KMB. School Feeding as a Protective Factor against Insulin Resistance: The Study of Cardiovascular Risks in Adolescents (ERICA). International Journal of Environmental Research and Public Health. 2022; 19(17):10551. https://doi.org/10.3390/ijerph191710551
Chicago/Turabian StyleOkamura, Aline Bassetto, Vivian Siqueira Santos Gonçalves, and Kênia Mara Baiocchi de Carvalho. 2022. "School Feeding as a Protective Factor against Insulin Resistance: The Study of Cardiovascular Risks in Adolescents (ERICA)" International Journal of Environmental Research and Public Health 19, no. 17: 10551. https://doi.org/10.3390/ijerph191710551