
A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Study Eligibility
2.3. Literature Search
2.4. Study Selection and Data Abstraction
2.5. Risk of Bias Assessment
2.6. Data Analysis
3. Results
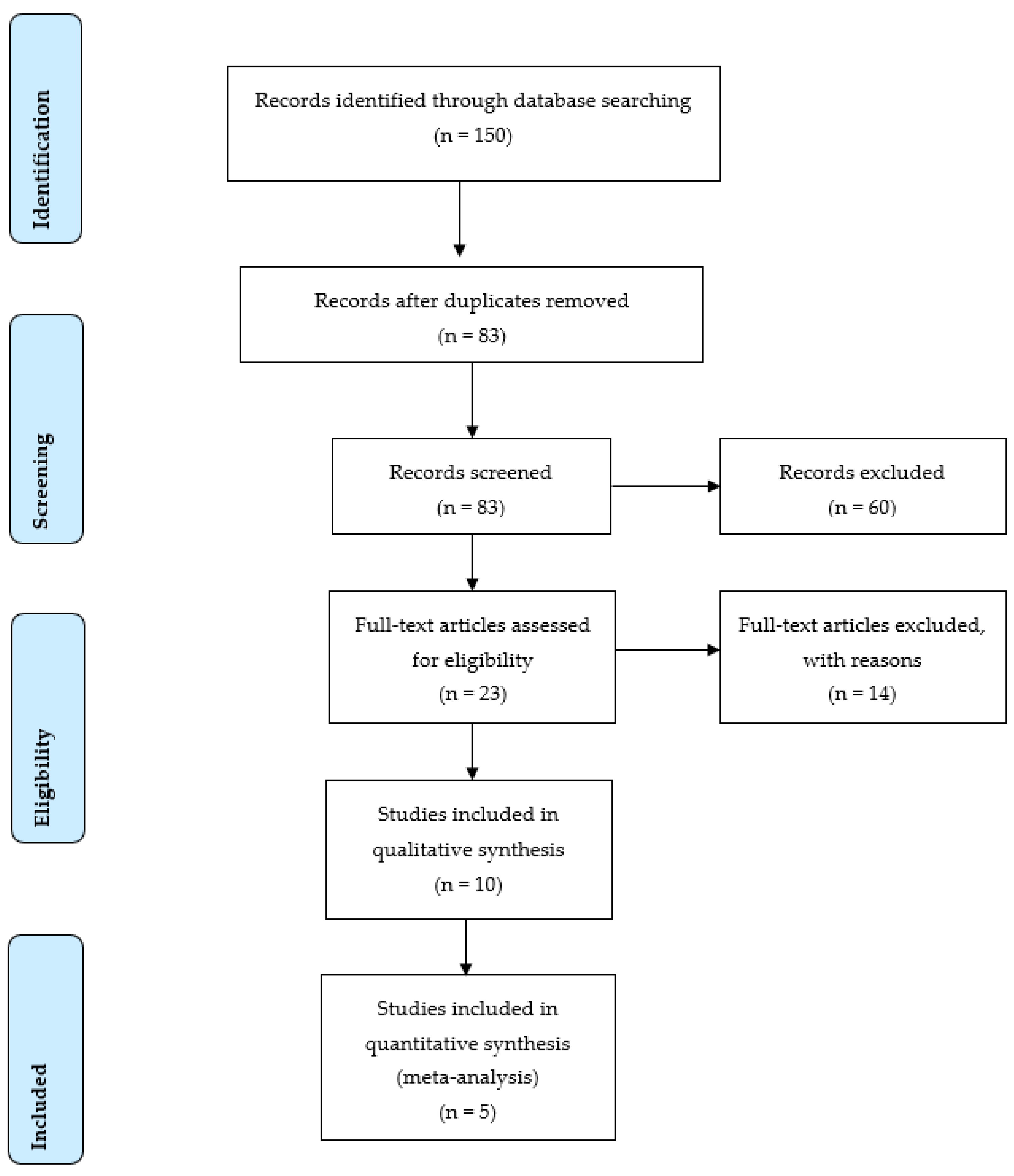
3.1. General Overview
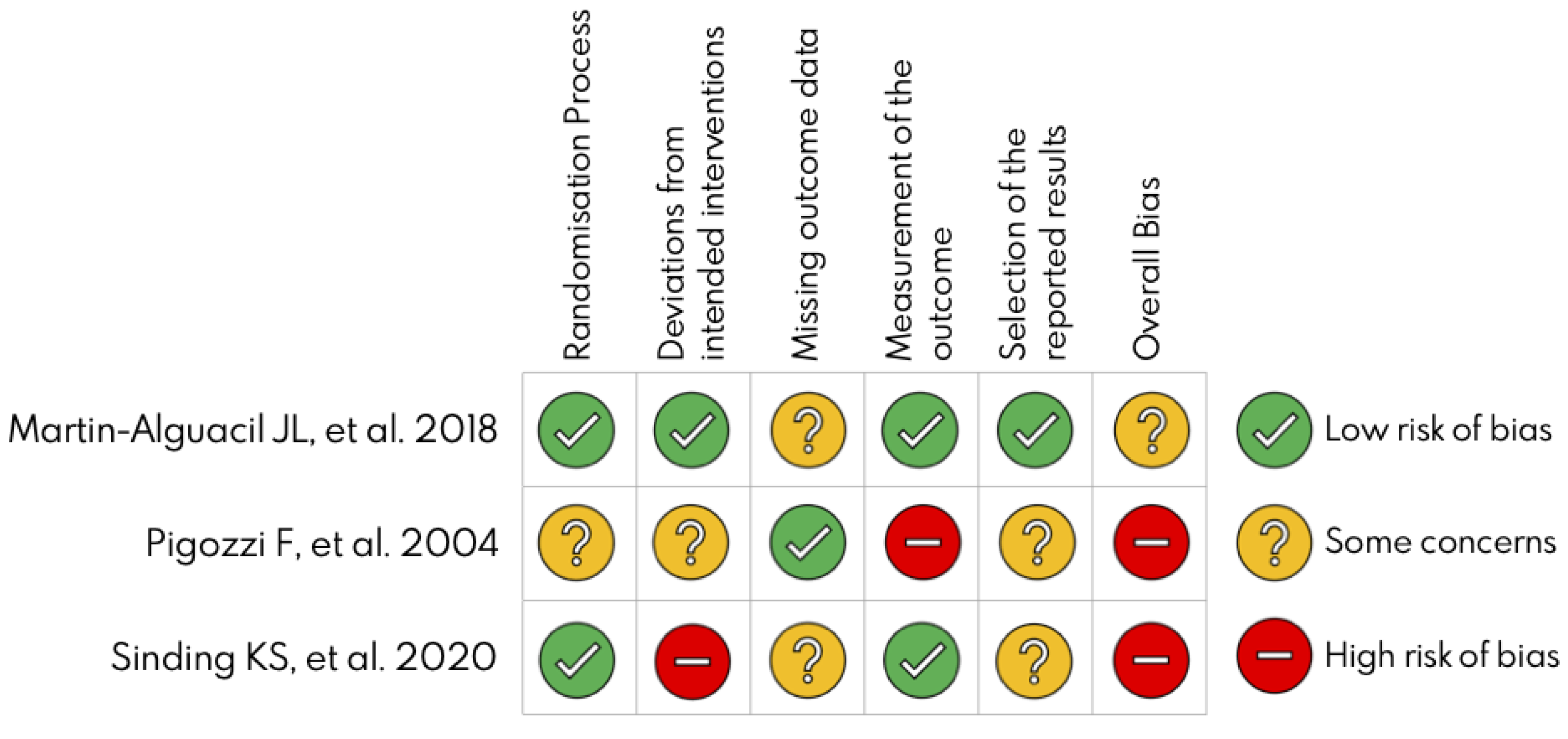
3.2. Risk of Bias
3.3. Combined Outcomes
3.3.1. Three Months
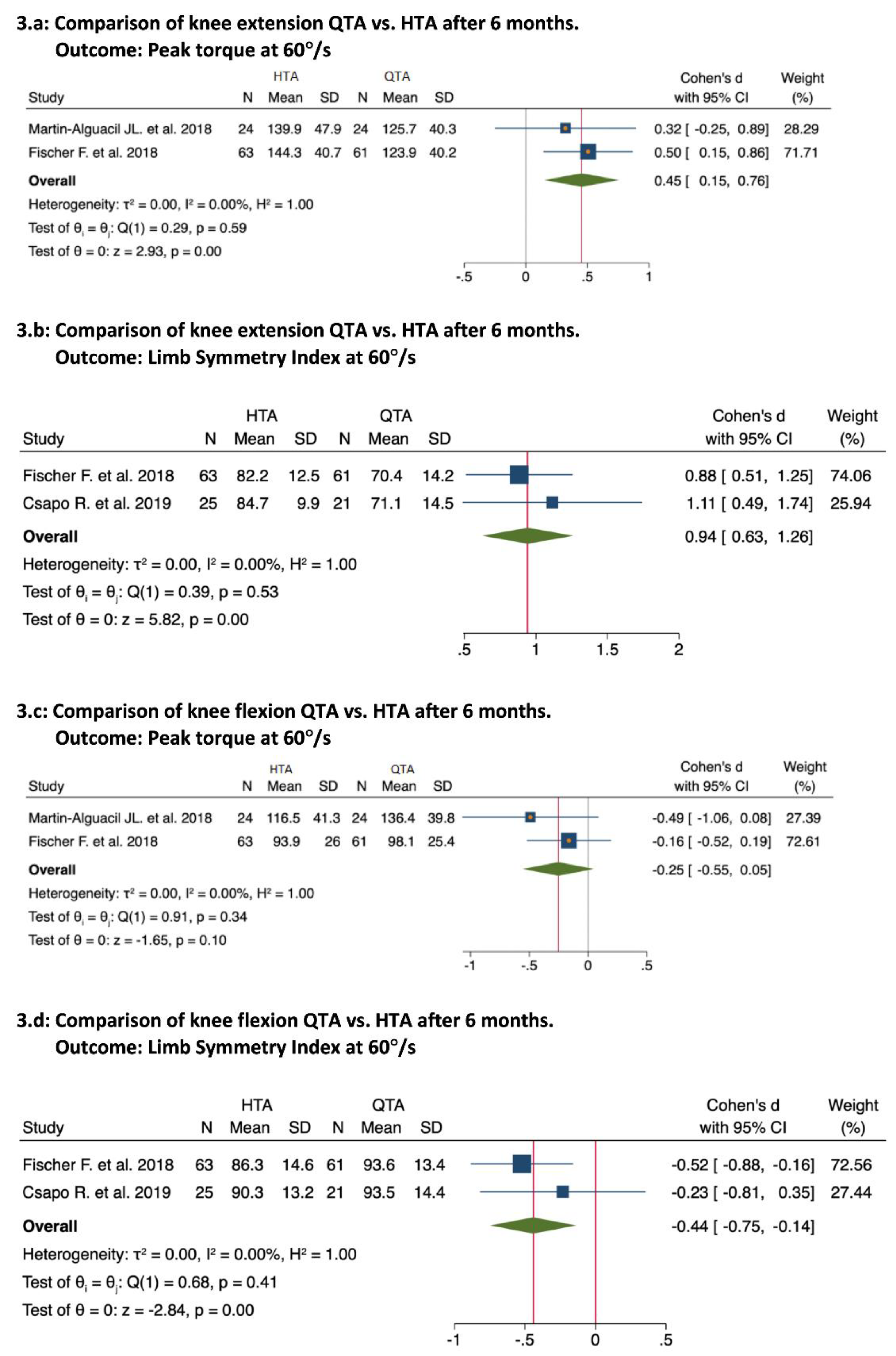
3.3.2. Six Months
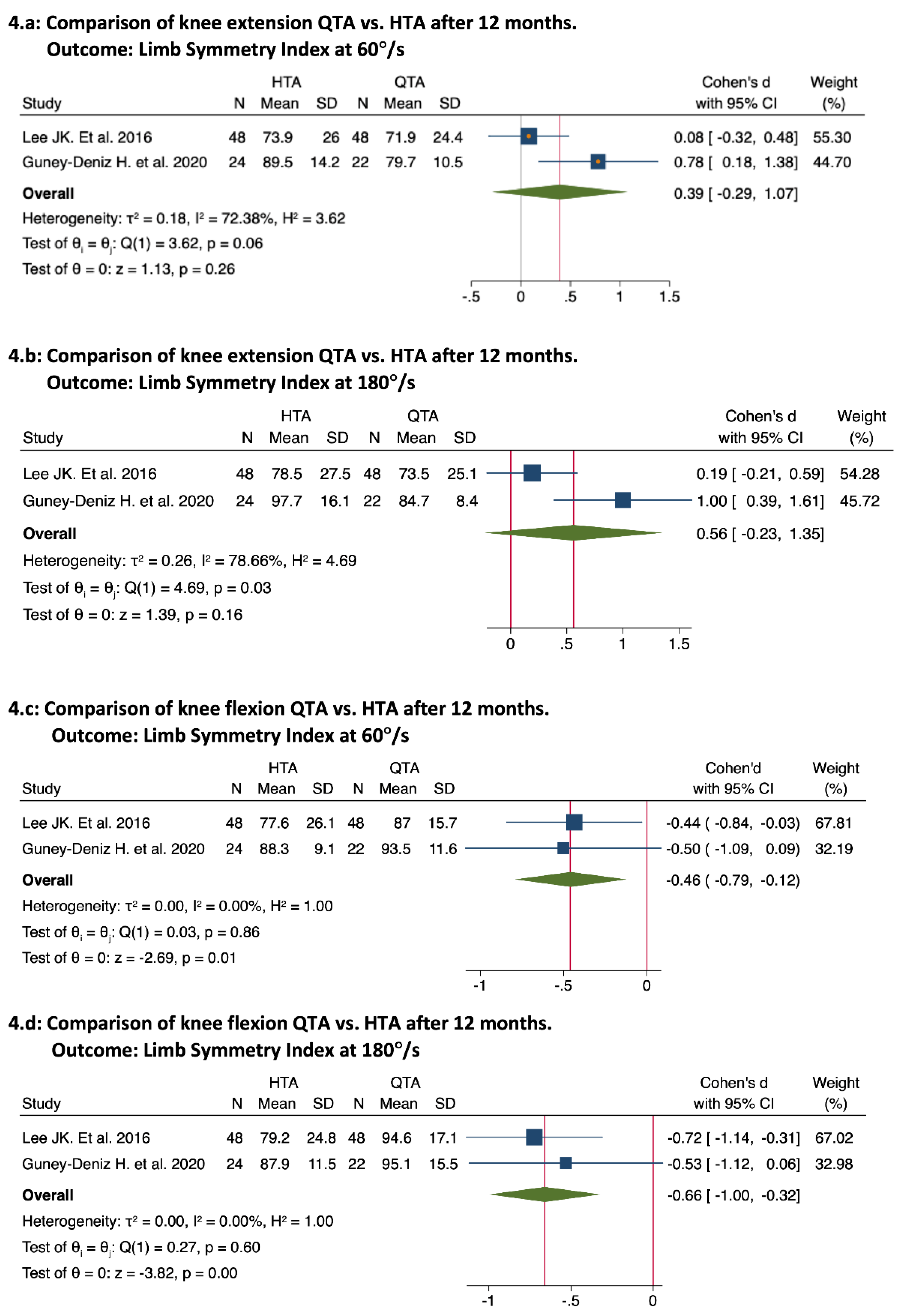
3.3.3. Twelve Months
3.3.4. Twenty-Four Months
3.4. Return to Sport and Rehabilitation Protocols
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef] [PubMed]
- Janssen, K.W.; Orchard, J.W.; Driscoll, T.R.; van Mechelen, W. High Incidence and Costs for Anterior Cruciate Ligament Reconstructions Performed in Australia from 2003–2004 to 2007–2008: Time for an Anterior Cruciate Ligament Register by Scandinavian Model? Scand. J. Med. Sci. Sports 2012, 22, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Gans, I.; Retzky, J.S.; Jones, L.C.; Tanaka, M.J. Epidemiology of Recurrent Anterior Cruciate Ligament Injuries in National Collegiate Athletic Association Sports: The Injury Surveillance Program, 2004–2014. Orthop. J. Sports Med. 2018, 6, 2325967118777823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, U.G.; Nagai, K.; Salvatore, G.; Cella, E.; Candela, V.; Cappelli, F.; Ciccozzi, M.; Denaro, V. Epidemiology of Anterior Cruciate Ligament Reconstruction Surgery in Italy: A 15-Year Nationwide Registry Study. J. Clin. Med. 2021, 10, 223. [Google Scholar] [CrossRef]
- Griffin, L.Y.; Albohm, M.J.; Arendt, E.A.; Bahr, R.; Beynnon, B.D.; Demaio, M.; Dick, R.W.; Engebretsen, L.; Garrett, W.E.J.; Hannafin, J.A.; et al. Understanding and Preventing Noncontact Anterior Cruciate Ligament Injuries: A Review of the Hunt Valley II Meeting, January 2005. Am. J. Sports Med. 2006, 34, 1512–1532. [Google Scholar] [CrossRef]
- Holm, I.; Oiestad, B.E.; Risberg, M.A.; Aune, A.K. No Difference in Knee Function or Prevalence of Osteoarthritis after Reconstruction of the Anterior Cruciate Ligament with 4-Strand Hamstring Autograft versus Patellar Tendon-Bone Autograft: A Randomized Study with 10-Year Follow-Up. Am. J. Sports Med. 2010, 38, 448–454. [Google Scholar] [CrossRef]
- Ellman, M.B.; Sherman, S.L.; Forsythe, B.; LaPrade, R.F.; Cole, B.J.; Bach, B.R.J. Return to Play Following Anterior Cruciate Ligament Reconstruction. J. Am. Acad. Orthop. Surg. 2015, 23, 283–296. [Google Scholar] [CrossRef]
- Harris, J.D.; Abrams, G.D.; Bach, B.R.; Williams, D.; Heidloff, D.; Bush-Joseph, C.A.; Verma, N.N.; Forsythe, B.; Cole, B.J. Return to Sport after ACL Reconstruction. Orthopedics 2014, 37, e103-8. [Google Scholar] [CrossRef] [Green Version]
- Sousa, P.L.; Krych, A.J.; Cates, R.A.; Levy, B.A.; Stuart, M.J.; Dahm, D.L. Return to Sport: Does Excellent 6-Month Strength and Function Following ACL Reconstruction Predict Midterm Outcomes? Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1356–1363. [Google Scholar] [CrossRef]
- Rothrauff, B.B.; Jorge, A.; de Sa, D.; Kay, J.; Fu, F.H.; Musahl, V. Anatomic ACL Reconstruction Reduces Risk of Post-Traumatic Osteoarthritis: A Systematic Review with Minimum 10-Year Follow-Up. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1072–1084. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Marshall, H.A.; Goodrich, J.A.; McCarty, E.C. Quadriceps Tendon Autograft for Primary Anterior Cruciate Ligament Reconstruction: A Systematic Review of Comparative Studies with Minimum 2-Year Follow-Up. Arthroscopy 2018, 34, 1699–1707. [Google Scholar] [CrossRef]
- Winkler, P.W.; Vivacqua, T.; Thomassen, S.; Lovse, L.; Lesniak, B.P.; Getgood, A.M.J.; Musahl, V. Quadriceps Tendon Autograft Is Becoming Increasingly Popular in Revision ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2021, 30, 149–160. [Google Scholar] [CrossRef] [PubMed]
- van Eck, C.F.; Illingworth, K.D.; Fu, F.H. Quadriceps Tendon: The Forgotten Graft. Arthroscopy 2010, 26, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Pigozzi, F.; Di Salvo, V.; Parisi, A. Isokinetic Evaluation of Anterior Cruciate Ligament Reconstruction: Quadriceps Tendon versus Patellar Tendon. J. Sports Med. Phys. Fit. 2004, 44, 288–293. [Google Scholar]
- Lee, J.K.; Lee, S.; Lee, M.C. Outcomes of Anatomic Anterior Cruciate Ligament Reconstruction: Bone-Quadriceps Tendon Graft versus Double-Bundle Hamstring Tendon Graft. Am. J. Sports Med. 2016, 44, 2323–2329. [Google Scholar] [CrossRef]
- Kurz, A.; Evaniew, N.; Yeung, M.; Samuelsson, K.; Peterson, D.; Ayeni, O.R. Credibility and Quality of Meta-Analyses Addressing Graft Choice in Anterior Cruciate Ligament Reconstruction: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 538–551. [Google Scholar] [CrossRef]
- Sajovic, M.; Strahovnik, A.; Dernovsek, M.Z.; Skaza, K. Quality of Life and Clinical Outcome Comparison of Semitendinosus and Gracilis Tendon versus Patellar Tendon Autografts for Anterior Cruciate Ligament Reconstruction: An 11-Year Follow-up of a Randomized Controlled Trial. Am. J. Sports Med. 2011, 39, 2161–2169. [Google Scholar] [CrossRef]
- Maletis, G.B.; Inacio, M.C.S.; Funahashi, T.T. Risk Factors Associated with Revision and Contralateral Anterior Cruciate Ligament Reconstructions in the Kaiser Permanente ACLR Registry. Am. J. Sports Med. 2015, 43, 641–647. [Google Scholar] [CrossRef]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Hamstring Strength Recovery after Hamstring Tendon Harvest for Anterior Cruciate Ligament Reconstruction: A Comparison between Graft Types. Arthroscopy 2010, 26, 462–469. [Google Scholar] [CrossRef]
- Perriman, A.; Leahy, E.; Semciw, A.I. The Effect of Open- Versus Closed-Kinetic-Chain Exercises on Anterior Tibial Laxity, Strength, and Function Following Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. J. Orthop. Sports Phys. Ther. 2018, 48, 552–566. [Google Scholar] [CrossRef]
- Smith, A.H.; Capin, J.J.; Zarzycki, R.; Snyder-Mackler, L. Athletes with Bone-Patellar Tendon-Bone Autograft for Anterior Cruciate Ligament Reconstruction Were Slower to Meet Rehabilitation Milestones and Return-to-Sport Criteria Than Athletes With Hamstring Tendon Autograft or Soft Tissue Allograft: Secondary. J. Orthop. Sports Phys. Ther. 2020, 50, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Logerstedt, D.S.; Hunter-Giordano, A.; Axe, M.J.; Snyder-Mackler, L. Current Concepts for Anterior Cruciate Ligament Reconstruction: A Criterion-Based Rehabilitation Progression. J. Orthop. Sports Phys. Ther. 2012, 42, 601–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Grinsven, S.; van Cingel, R.E.H.; Holla, C.J.M.; van Loon, C.J.M. Evidence-Based Rehabilitation Following Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1128–1144. [Google Scholar] [CrossRef] [PubMed]
- Karasel, S.; Akpinar, B.; Gülbahar, S.; Baydar, M.; El, O.; Pinar, H.; Tatari, H.; Karaoğlan, O.; Akalin, E. Clinical and Functional Outcomes and Proprioception after a Modified Accelerated Rehabilitation Program Following Anterior Cruciate Ligament Reconstruction with Patellar Tendon Autograft. Acta Orthop. Traumatol. Turc. 2010, 44, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Wiese-bjornstal, D.M.; Smith, A.M.; Shaffer, S.M.; Morrey, M.A. An Integrated Model of Response to Sport Injury: Psychological and Sociological Dynamics. J. Appl. Sport Psychol. 1998, 10, 46–69. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to Sport Following Anterior Cruciate Ligament Reconstruction Surgery: A Systematic Review and Meta-Analysis of the State of Play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef]
- Meierbachtol, A.; Yungtum, W.; Paur, E.; Bottoms, J.; Chmielewski, T.L. Psychological and Functional Readiness for Sport Following Advanced Group Training in Patients with Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2018, 48, 864–872. [Google Scholar] [CrossRef]
- Schmitt, L.C.; Paterno, M.V.; Hewett, T.E. The Impact of Quadriceps Femoris Strength Asymmetry on Functional Performance at Return to Sport Following Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2012, 42, 750–759. [Google Scholar] [CrossRef] [Green Version]
- Welling, W.; Benjaminse, A.; Lemmink, K.; Dingenen, B.; Gokeler, A. Progressive Strength Training Restores Quadriceps and Hamstring Muscle Strength within 7 Months after ACL Reconstruction in Amateur Male Soccer Players. Phys. Ther. Sport 2019, 40, 10–18. [Google Scholar] [CrossRef]
- Marcolin, A.L.V.; Cardin, S.P.; Magalhães, C.S. Muscle Strength Assessment among Children and Adolescents with Growing Pains and Joint Hypermobility. Braz. J. Phys. Ther. 2009, 13, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Pua, Y.H.; Bryant, A.L.; Steele, J.R.; Newton, R.U.; Wrigley, T. V Isokinetic Dynamometry in Anterior Cruciate Ligament Injury and Reconstruction. Ann. Acad. Med. Singap. 2008, 37, 330–340. [Google Scholar]
- Drouin, J.M.; Valovich-mcLeod, T.C.; Shultz, S.J.; Gansneder, B.M.; Perrin, D.H. Reliability and Validity of the Biodex System 3 pro Isokinetic Dynamometer Velocity, Torque and Position Measurements. Eur. J. Appl. Physiol. 2004, 91, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Zemach, L.; Almoznino, S.; Barak, Y.; Dvir, Z. Quadriceps Insufficiency in Patients with Knee Compromise: How Many Velocities Should an Isokinetic Test Protocol Consist Of? Isokinet Exerc. Sci. 2009, 17, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Yapici, A.; Findikoglu, G.; Dundar, U. Do Isokinetic Angular Velocity and Contraction Types Affect the Predictors of Different Anaerobic Power Tests? J. Sports Med. Phys. Fit. 2016, 56, 383–391. [Google Scholar]
- Undheim, M.B.; Cosgrave, C.; King, E.; Strike, S.; Marshall, B.; Falvey, A.; Franklyn-Miller, A. Isokinetic Muscle Strength and Readiness to Return to Sport Following Anterior Cruciate Ligament Reconstruction: Is There an Association? A Systematic Review and a Protocol Recommendation. Br. J. Sports Med. 2015, 49, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.T.; McClelland, J.A.; Feller, J.A.; Webster, K.E. Knee Muscle Strength after Quadriceps Tendon Autograft Anterior Cruciate Ligament Reconstruction: Systematic Review and Meta-Analysis. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 2918–2933. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [Green Version]
- Locke, S.R.; McKay, R.C.; Jung, M.E. “I’m Just Too Busy to Exercise”: Reframing the Negative Thoughts Associated with Exercise-Related Cognitive Errors. Psychol. Sport Exerc. 2019, 43, 279–287. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Csapo, R.; Hoser, C.; Gföller, P.; Raschner, C.; Fink, C. Fitness, Knee Function and Competition Performance in Professional Alpine Skiers after ACL Injury. J. Sci. Med. Sport 2019, 22, S39–S43. [Google Scholar] [CrossRef] [PubMed]
- Fischer, F.; Fink, C.; Herbst, E.; Hoser, C.; Hepperger, C.; Blank, C.; Gföller, P. Higher Hamstring-to-Quadriceps Isokinetic Strength Ratio during the First Post-Operative Months in Patients with Quadriceps Tendon Compared to Hamstring Tendon Graft Following ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Seong, S.C.; Lee, S.; Lee, M.C. Anterior Cruciate Ligament Reconstruction: Quadriceps versus Patellar Autograft. Clin. Orthop. Relat. Res. 2008, 466, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Martin-Alguacil, J.L.; Arroyo-Morales, M.; Martín-Gomez, J.L.; Monje-Cabrera, I.M.; Abellán-Guillén, J.F.; Esparza-Ros, F.; Lozano, M.L.; Cantarero-Villanueva, I. Strength Recovery after Anterior Cruciate Ligament Reconstruction with Quadriceps Tendon versus Hamstring Tendon Autografts in Soccer Players: A Randomized Controlled Trial. Knee 2018, 25, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Guney-Deniz, H.; Harput, G.; Kaya, D.; Nyland, J.; Doral, M.N. Quadriceps Tendon Autograft ACL Reconstructed Subjects Overshoot Target Knee Extension Angle during Active Proprioception Testing. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 645–652. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Sinding, K.S.; Nielsen, T.G.; Hvid, L.G.; Lind, M.; Dalgas, U. Effects of Autograft Types on Muscle Strength and Functional Capacity in Patients Having Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. Sports Med. 2020, 50, 1393–1403. [Google Scholar] [CrossRef]
- Cavaignac, E.; Coulin, B.; Tscholl, P.; Nik Mohd Fatmy, N.; Duthon, V.; Menetrey, J. Is Quadriceps Tendon Autograft a Better Choice Than Hamstring Autograft for Anterior Cruciate Ligament Reconstruction? A Comparative Study with a Mean Follow-up of 3.6 Years. Am. J. Sports Med. 2017, 45, 1326–1332. [Google Scholar] [CrossRef]
- Hunnicutt, J.L.; Gregory, C.M.; McLeod, M.M.; Woolf, S.K.; Chapin, R.W.; Slone, H.S. Quadriceps Recovery After Anterior Cruciate Ligament Reconstruction with Quadriceps Tendon Versus Patellar Tendon Autografts. Orthop. J. Sports Med. 2019, 7, 2325967119839786. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Hurley, E.T.; Calvo-Gurry, M.; Withers, D.; Farrington, S.K.; Moran, R.; Moran, C.J. Quadriceps Tendon Autograft in Anterior Cruciate Ligament Reconstruction: A Systematic Review. Arthroscopy 2018, 34, 1690–1698. [Google Scholar] [CrossRef] [PubMed]
- Salas, V.E.R.; de Oliveira, D.E.; de Lima, M.V.; Duarte Junior, A.; Guglielmetti, L.G.B.; de Cury, R.P.L.; Jorge, P.B. Quadriceps Autograft in Anterior Cruciate Ligament Reconstruction: A Literature Review. Rev. Bras. De Med. Do Esporte 2020, 26, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Ajrawat, P.; Dwyer, T.; Whelan, D.; Theodoropoulos, J.; Murnaghan, L.; Bhargava, M.; Ogilvie-Harris, D.; Chahal, J. A Comparison of Quadriceps Tendon Autograft with Bone-Patellar Tendon-Bone Autograft and Hamstring Tendon Autograft for Primary Anterior Cruciate Ligament Reconstruction: A Systematic Review and Quantitative Synthesis. Clin. J. Sport Med. 2019, 31, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Prodromos, C.C.; Han, Y.S.; Keller, B.L.; Bolyard, R.J. Stability Results of Hamstring Anterior Cruciate Ligament Reconstruction at 2- to 8-Year Follow-Up. Arthroscopy 2005, 21, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Mouarbes, D.; Menetrey, J.; Marot, V.; Courtot, L.; Berard, E.; Cavaignac, E. Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts. Am. J. Sports Med. 2019, 47, 3531–3540. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) Study Design | Objective | Participants | Rehabilitation Procedures (Duration) | Outcomes Measures | Evaluation Follow-Up | Participants Gender n (%) | Principal Findings |
|---|---|---|---|---|---|---|---|
| Cavaignac, E., et al., 2017 [48] Cohort study | To compare isokinetic strength test of HTA and QTA, stability, functional outcomes scores, anterior knee pain and reoperation rate. | 95 patients QTA; n = 45; 32.1 ± 8 years HTA; n = 41; 30.9 ± 9 years. | – | Functional outcome (KOOS, Tegner and IKDC), Joint stability KT-1000, Lachman, pivot shift), anterior knee pain (Shelbourne-Trumper score), and isokinetic strength. | 6 and 43 months post-surgery | QTA: 55% male HTA: 58% male | The use of a QTA graft in ACL reconstruction leads to equal or better functional outcomes than does the use of an HTA graft, without affecting morbidity. |
| Csapo, R., et al., 2019 [41] Retrospective cohort study | To assess the fitness of elite alpine skiers during recovery from ACL reconstruction and changes in performance level after return to competition. | 46 athletes; QTA; n = 21; HTA; n = 25. | – | Isokinetic dynamometry, back in action test battery (knee function after ACL recovery), VAS Functional outcome (Lysholm score, Tegner activity scale) | 15 days, 6, 12, and 24 months post-surgery | 20 male vs. 26 female | The rate of recovery of knee extensor muscle function may be slower following ACL reconstruction using QTA. On overage, athletes returned to competition within one year after surgery and succeeded in surpassing their baseline performance level within the first year after return to competition. |
| Fischer, F., et al., 2018 [42] Randomized Controlled Study | To compare isokinetic strength test for Quadriceps in who received either QTA or HTA autografts at two-time intervals within the first year after surgery. | 124 patients QTA; n = 61; 21.7 ± 7.4 years, HTA; n =63; 21.5 ± 6.9 years. | Isometric and closed chain exercises, bicycling running and sport-specific exercises post-operatively. | Isokinetic strength test. | 5.5- and 7.6-months post-surgery | QTA: male 34 (55.7). HTA: male 47 (74.6) | ACL reconstruction with a QTA autograft have a significantly higher H/Q ratio within one year after surgery compared to the HTA group. |
| Guney-Deniz, H., et al., 2020 [45] Cross-sectional, case–control study | To compare isokinetic strength test, the active joint position sense and knee functions in individuals who had anterior cruciate ligament (ACL) reconstruction with QTA, HTA, TAA and healthy individuals. | 67 subjects QTA; n = 22; 27.8 ± 2.8 years, HTA; n = 24; 26.7 ± 4.6 years, ATT; n = 21 26.4 ± 5.5 years, Control; n = 20 28.7 ± 3.1 years. | Post-operative protocol includes progressive quadriceps femoris strengthening with neuromuscular electrical stimulation, and neuromuscular control exercise training. | Isokinetic strength test and active joint position sense assessments | 13.5 months post-surgery | – | Knee proprioception deficits and impaired muscle strength were evident among patients at a mean 13.5 months post-ACL reconstruction compared with healthy controls. QTA group may be more likely to actively over-estimate knee position near terminal extension. |
| Han, H.S., et al., 2008 [43] Retrospective comparative study | To compare the clinical outcomes of anterior cruciate ligament reconstructions using QTA and PTA autografts. | 144 patients QTA; n = 72; 27.8 (15–51) * years, PTA; n = 72; 27.8 (15–51) * years | – | knee stability (KT-1000), Functional outcome (Lysholm and IKDC) and Isokinetic strength test. | Pre-surgery, 6, 12 and 24 months | QTA: 68 male vs PTA: 68 male. | QTA group showed clinical outcomes comparable to PTA group with anterior knee pain beingless severe in the former. The data indicate the quadriceps tendon can be a good alternative graft choice. |
| Hunnicut, J.K., et al., 2019 [49] Cohort Study | To compare quadriceps recovery and functional outcomes in patients with QTA versus PTA autografts. | 30 patients QTA; n = 15; 25.0 (14.0–41.0) years PTA; n = 15; 18.0 (15.0–32.0) years | – | Isometric and isokinetic strength testcentral Activation, MRI, Spatiotemporal Gait Hop Test and Functional outcome (IKDC, Lysholm, and KOOS) | 8 months post-surgery | QTA: male 12 vs. PTA: male 7 | Patients with QTA autografts demonstrated similar short-term quadriceps recovery and postsurgical outcomes compared with patients with PTA autografts. |
| Lee, J.K., et al., 2016 [15] Cohort study | To compare functional outcomes and knee joint stability of anatomic ACL reconstruction with double-bundle hamstring tendon and bone–quadriceps tendon autografts | 96 patients QTA; n = 48; 31.1 (17–57) * years, HTA; n = 48; 29.9 (17–58) * years | Post-operative protocol includes quadriceps-strengthening, continuous passive motion, open kinetic chain exercise and kinetic exercises. (6 months) | Knee stability (Manual laxity test, KT-2000) Functional outcome (IKDC, Tegner activity score, modified Lysholm score), anterior knee pain questionnaire, Isokinetic strength test and tunnel position evaluation by quadrant method. | Pre-surgery and 6 weeks, 3, 12 and 24 months post-surgery | QTA: male 44. PTA: male 44 | QTA group showed similar knee stability and functional outcomes when compared with the HTA autograft. Better flexor muscle strength recovery was found in the QTA, indicating a potential advantage of the QTA autograft in ACL reconstruction. |
| Martín-Alguacil, J.L., et al., 2018 [44] Randomized Controlled Study | To compare the strength recovery and functional outcomes of an anatomic single bundle reconstruction with QTA and HTA autografts in competitive soccer players. | 51 participants QTA; n = 26; 18.7 ± 3.6 years, HTA; n = 25; 19.2 ± 3.6 years. | Both groups followed the same pre-and-post rehabilitation protocol based on muscular strength, endurance and neuromuscular control. (24 weeks) | Isokinetic strength test Function outcome (Lysholm knee score and Cincinnati Knee Rating System) and knee stability with KT-2000. | Pre-surgery and 3, 6, 12 and 24 months post-surgery | QTA: male 23 (88.5). HTA: male 16 (54.0) | QTA group showed similar functional outcome results with a better isokinetic H/Q ratio compared to HTA group at 12 months of follow-up in soccer players. |
| Pigozzi E., et al., 2004 [14] Prospective randomized study | To compare the isokinetic recovery of thigh strength after ACL reconstruction by using patellar or quadriceps tendon as a graft. | 48 patients QTA; n = 24; 33 (21–47) years PTA; n = 24 35 (23–41) * years | Post rehabilitation program: continuous passive motion, walking, swimming, cycling and running at the end of 6 months. (6 months) | Counter movement jump, leg press, knee stability (KT-1000) and isokinetic strength tests. | Pre-surgery and 6 months post-surgery. | QTA: 17 male vs. PTA: 19 male | Significant improvement of the lower limb strength deficit using QTA compared to PTA that could encourage the use of QTA in order to achieve an easier rehabilitation and a faster Return to sport. |
| Sinding, K.S., et al., 2020 [47] Prospective randomized controlled clinical trial | To investigate the effects of QTA vs. HTA on thigh muscle strength and functional capacity, and a patient-reported outcome 1 year after ACL-R, and to compare the results to healthy controls. | 150 patients QTA; n = 50; 128.7 ± 6.4 years, HTA; n = 50; 28.3 ± 6.2 years, CON; n = 50; 28.3 ± 6.2 years | Post rehabilitation program: days 1–14: full support to pain threshold, free movement, no bandages; weeks 3–12: frequent movement exercises supervised by a physiotherapist, bicycle ergometer, full weight bearing; months 4–9: running allowed; months 10–12: contact sports. allowed. (12 months) | Isokinetic strength test, one leg hop test and Functional outcome with IKDC | 12.5 months post-surgery | QTA: male 25 (60%) HTA: male 23 (53%) vs. CON: male 27 (54%) | HTA leading to impairments of knee extensor and knee flexor muscle strength, while QTA results in more pronounced impairments of knee extensor only. Functional capacity and functional outcome was unaffected by autograft type, with the former showing impairment compared to healthy controls. |
| D1 | D2 | D3 | D4 | D5 | D6 | D7 | Overall Judgement | |
|---|---|---|---|---|---|---|---|---|
| Cavaignac E., et al., 2017 [48] | Serious | Low | Low | Low | Serious | Low | Low | Serious |
| Csapo R., et al., 2019 [41] | Moderate | Moderate | Low | Low | Low | Low | Serious | Serious |
| Fischer F., et al., 2018 [42] | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
| Han H.S., et al., 2008 [43] | Serious | Low | Low | Low | Critical | Low | Moderate | Critical |
| Guney-Deniz H., et al., 2020 [45] | Serious | Low | Low | Low | Low | Low | Low | Serious |
| Hunnicutt J.L., et al., 2019 [49] | Serious | Low | Low | Low | Low | Low | Moderate | Serious |
| Lee J.K., et al., 2016 [15] | Serious | Moderate | Low | Low | Low | Low | Moderate | Serious |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herbawi, F.; Lozano-Lozano, M.; Lopez-Garzon, M.; Postigo-Martin, P.; Ortiz-Comino, L.; Martin-Alguacil, J.L.; Arroyo-Morales, M.; Fernandez-Lao, C. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. Int. J. Environ. Res. Public Health 2022, 19, 6764. https://doi.org/10.3390/ijerph19116764
Herbawi F, Lozano-Lozano M, Lopez-Garzon M, Postigo-Martin P, Ortiz-Comino L, Martin-Alguacil JL, Arroyo-Morales M, Fernandez-Lao C. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. International Journal of Environmental Research and Public Health. 2022; 19(11):6764. https://doi.org/10.3390/ijerph19116764
Chicago/Turabian StyleHerbawi, Fahed, Mario Lozano-Lozano, Maria Lopez-Garzon, Paula Postigo-Martin, Lucia Ortiz-Comino, Jose Luis Martin-Alguacil, Manuel Arroyo-Morales, and Carolina Fernandez-Lao. 2022. "A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts" International Journal of Environmental Research and Public Health 19, no. 11: 6764. https://doi.org/10.3390/ijerph19116764