
Total Hemoglobin Trajectories from Pregnancy to Postpartum in Rural Northeast Brazil: Differences between Adolescent and Adult Women

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Location
2.2. Population and Sample
2.3. Instruments
2.4. Measurements
2.4.1. Total Hemoglobin Concentration (THB)
2.4.2. Weight and Height
2.5. Procedures
2.6. Ethics
2.7. Data Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fisher, A.; Nemeth, E. Iron homeostasis during pregnancy. Am. J. Clin. Nutr. 2017, 106 (Suppl. S6), 1567S–1574S. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O. Iron status during pregnancy: Setting the stage for mother and infant. Am. J. Clin. Nutr. 2005, 81, 1218s–1222s. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.K.; Tan, E.L. Alterations in physiology and anatomy during pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.M.; Crespo-Bellido, M.; Dewey, K.G. Variation in hemoglobin across the life cycle and between males and females. Ann. N. Y. Acad. Sci. 2019, 1450, 105–125. [Google Scholar] [CrossRef]
- Bakrim, S.; Motiaa, Y.; Ouarour, A.; Masrar, A. Hematological parameters of the blood count in a healthy population of pregnant women in the Northwest of Morocco (Tetouan-M’diq-Fnideq provinces). Pan Afr. Med. J. 2018, 29, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, J.G.; Barateiro, A.; Peixoto, E.P.M.; Barros, A.B.C.S.; Souza, R.M.; Clark, T.G.; Campino, S.; Wrenger, C.; Wunderlich, G.; Palmisano, G.; et al. Adverse pregnancy outcomes are associated with Plasmodium vivax malaria in a prospective cohort of women from the Brazilian Amazon. PLOS Negl. Trop. Dis. 2021, 15, e0009390. [Google Scholar] [CrossRef]
- Zillmer, K.; Pokharel, A.; Spielman, K.; Kershaw, M.; Ayele, K.; Kidane, Y.; Belachew, T.; Houser, R.F.; Kennedy, E.; Griffiths, J.K.; et al. Predictors of anemia in pregnant women residing in rural areas of the Oromiya region of Ethiopia. BMC Nutr. 2017, 3, 65. [Google Scholar] [CrossRef] [Green Version]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Fujimori, E.; Sato, A.P.S.; Szarfarc, S.C.; Veiga, G.V.; Oliveira, V.A.; Colli, C.; Moreira-Araújo, R.; de Arruda, I.K.G.; Uchimura, T.T.; Brunken, G.S.; et al. Anemia in Brazilian pregnant women before and after flour fortification with iron. Rev. Saúde Pública 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Holness, N. A global perspective on adolescent pregnancy. Int. J. Nurs. Pract. 2015, 21, 677–681. [Google Scholar] [CrossRef]
- Gibbs, C.M.; Wendt, A.; Peters, S.; Hogue, C.J. The impact of early age at first childbirth on maternal and infant health. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. S1), 259–284. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health of Brazil. Information System on Live Births (SINASC), Single Health System Department of Informatics (DATASUS). 2019. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvuf.def (accessed on 3 February 2022).
- The World Bank Group. Adolescent Fertility Rate (Births per 1000 Women Ages 15–19). 2021. Available online: https://data.worldbank.org/indicator/sp.ado.tfrt (accessed on 13 May 2021).
- Berhe, B.; Mardu, F.; Legese, H.; Gebrewahd, A.; Gebremariam, G.; Tesfay, K.; Kahsu, G.; Negash, H.; Adhanom, G. Prevalence of anemia and associated factors among pregnant women in Adigrat General Hospital, Tigrai, northern Ethiopia, 2018. BMC Res. Notes 2019, 12, 310. [Google Scholar] [CrossRef] [PubMed]
- Ampiah, M.K.M.; Kovey, J.J.; Apprey, C.; Annan, R.A. Comparative analysis of trends and determinants of anaemia between adult and teenage pregnant women in two rural districts of Ghana. BMC Public Health 2019, 19, 1379. [Google Scholar] [CrossRef] [PubMed]
- Câmara, S.M.A.; Sentell, T.; Bassani, D.G.; Domingues, M.R.; Pirkle, C.M. Strenghtening health research capacity to address adolescent fertility in Northeast Brazil. J. Glob. Health 2019, 9, 010303. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- O’Broin, S.D.; Gunter, E.W. Screening of folate status with use of dried blood spots on filter paper. Am. J. Clin. Nutr. 1999, 70, 359–367. [Google Scholar] [CrossRef] [PubMed]
- McDade, T.W. Development and validation of assay protocols for use with dried blood spot samples. Am. J. Hum. Biol. 2014, 26, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics Software. Available online: https://www.qualtrics.com (accessed on 10 May 2017).
- Petruccelli, J.L.; Saboia, A.L. Ethnic-Racial Characteristics of the Population: Classifications and Identities; Series Studies and Analyses. Demographic and Socioeconomic Information (Suppl. 2); Brazilian Institute of Geography and Statistics: Rio of Janeiro, Brazil, 2014. [Google Scholar]
- Ministry of Health of Brazil. Bolsa Família Program. 2020. Available online: https://bfa.saude.gov.br/public/file/faq_bfa.pdf (accessed on 26 June 2020).
- Andrade, R.B.; Pirkle, C.M.; Sentell, T.; Bassani, D.; Domingues, M.R.; Câmara, S.M.A. Adequacy of Prenatal Care in Northeast Brazil: Pilot Data Comparing Attainment of Standard Care Criteria for First-Time Adolescent and Adult Pregnant Women. Int. J. Women’s Health 2020, 12, 1023–1031. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations. Latin American and Caribbean Scale of Food Safety (ELCSA): User Manual and Applications. ELCSA Scientific Committee. 2012. Available online: http://www.fao.org/3/a-i3065s.pdf (accessed on 17 September 2020).
- Churchill, D.; Nair, M.; Stanworth, S.J.; Knight, M. The change in haemoglobin concentration between the first and third trimesters of pregnancy: A population study. BMC Pregnancy Childbirth 2019, 19, 359. [Google Scholar] [CrossRef] [Green Version]
- Cao, C.; O’Brien, K.O. Pregnancy and iron homeostasis: An update. Nutr. Rev. 2013, 71, 35–51. [Google Scholar] [CrossRef]
- Cecchi, F.; Pancani, S.; Vannetti, F.; Boni, R.; Castagnoli, C.; Paperini, A.; Pasquini, G.; Sofi, F.; Molino-Lova, R.; Macchi, C.; et al. Hemoglobin concentration is associated with self-reported disability and reduced physical performance in a community dwelling population of nonagenarians: The Mugello Study. Intern. Emerg. Med. 2017, 12, 1167–1173. [Google Scholar] [CrossRef]
- Semasaka, J.P.S.; Krantz, G.; Nzayirambaho, M.; Munyanshongore, C.; Edvardsson, K.; Mogren, I. Self-reported pregnancy-related health problems and self-rated health status in Rwandan women postpartum: A population-based cross-sectional study. BMC Pregnancy Childbirth 2016, 16, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kekäläinen, P.; Juuti, M.; Walle, T.; Laatikainen, T. Pregnancy planning in type 1 diabetic women improves glycemic control and pregnancy outcomes. J. Matern.-Fetal Neonatal Med. 2016, 29, 2252–2258. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Pearce, E.N. Preconception care to Optimize Pregnancy Outcomes. JAMA 2021, 326, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Chiossi, G.; Palomba, S.; Costantine, M.M.; Falbo, A.I.; Harirah, H.M.; Saade, G.R.; La Sala, G.B. Reference intervals for hemoglobin and hematocrit in a low-risk pregnancy cohort: Implications of racial differences. J. Matern.-Fetal Neonatal Med. 2019, 32, 2897–2904. [Google Scholar] [CrossRef]
- Mohamed, M.A.; Ahmad, T.; Macri, C.; Aly, H. Racial disparities in maternal hemoglobin concentrations and pregnancy outcomes. J. Perinat. Med. 2012, 40, 141–149. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Adolescent (n = 50) | Adults (n = 50) | p Value | |
|---|---|---|---|
| Median (IQR) or n (%) | |||
| Years of schooling | 9.00 (3) | 12.00 (4) | <0.001 |
| Race | 0.198 | ||
| White | 13 (26.0%) | 19 (38.0%) | |
| Mixed race/black | 37 (74.0%) | 31 (62.0%) | |
| Income sufficiency a | 0.715 | ||
| Very sufficient | 9 (18.0%) | 12 (24.5%) | |
| Suitable | 29 (58.0%) | 27 (55.1%) | |
| Not at all | 12 (24.0%) | 10 (20.4%) | |
| Bolsa famíliaa | 0.052 | ||
| Yes | 39 (78.0%) | 28 (56.0%) | |
| No | 11 (22.0%) | 21 (42.0%) | |
| Marital status | 0.096 | ||
| Married/Common law | 35 (70.0%) | 42 (42.0%) | |
| Single/Separated/Divorced | 15 (30.0%) | 8 (16.0%) | |
| Childhood SES a | 0.363 | ||
| Good | 23 (47.9%) | 17 (34.0%) | |
| Moderate | 19 (39.6%) | 26 (52.0%) | |
| Poor | 6 (12.5%) | 7 (14.0%) | |
| Weight | 54.99 (10.32) | 61.49 (10.37) | 0.002 |
| Height | 156.91 (5.29) | 159.17 (6.20) | 0.052 |
| Self-perceived health | 0.790 | ||
| Good | 42 (84.0%) | 41 (82.0%) | |
| Poor | 8 (16.0%) | 9 (18.0%) | |
| Number of prenatal appointments b | 9.00 (3) | 9.00 (2) | 0.602 |
| Planned pregnancy | 0.420 | ||
| Yes, entirely | 20 (40.0%) | 24 (48.0%) | |
| Somewhat/Not at all | 30 (60.0%) | 26 (52.0%) | |
| Food security | 0.068 | ||
| Yes | 9 (18.0%) | 17 (34.0%) | |
| No | 41 (82.0%) | 33 (66.0%) | |
| Age at menarche c | 12.00 (1) | 12.00 (3) | 0.871 |
| Baseline (n = 100) | T1 (n = 88) | T2 (n = 86) | |
|---|---|---|---|
| Age group | Mean (SD) | ||
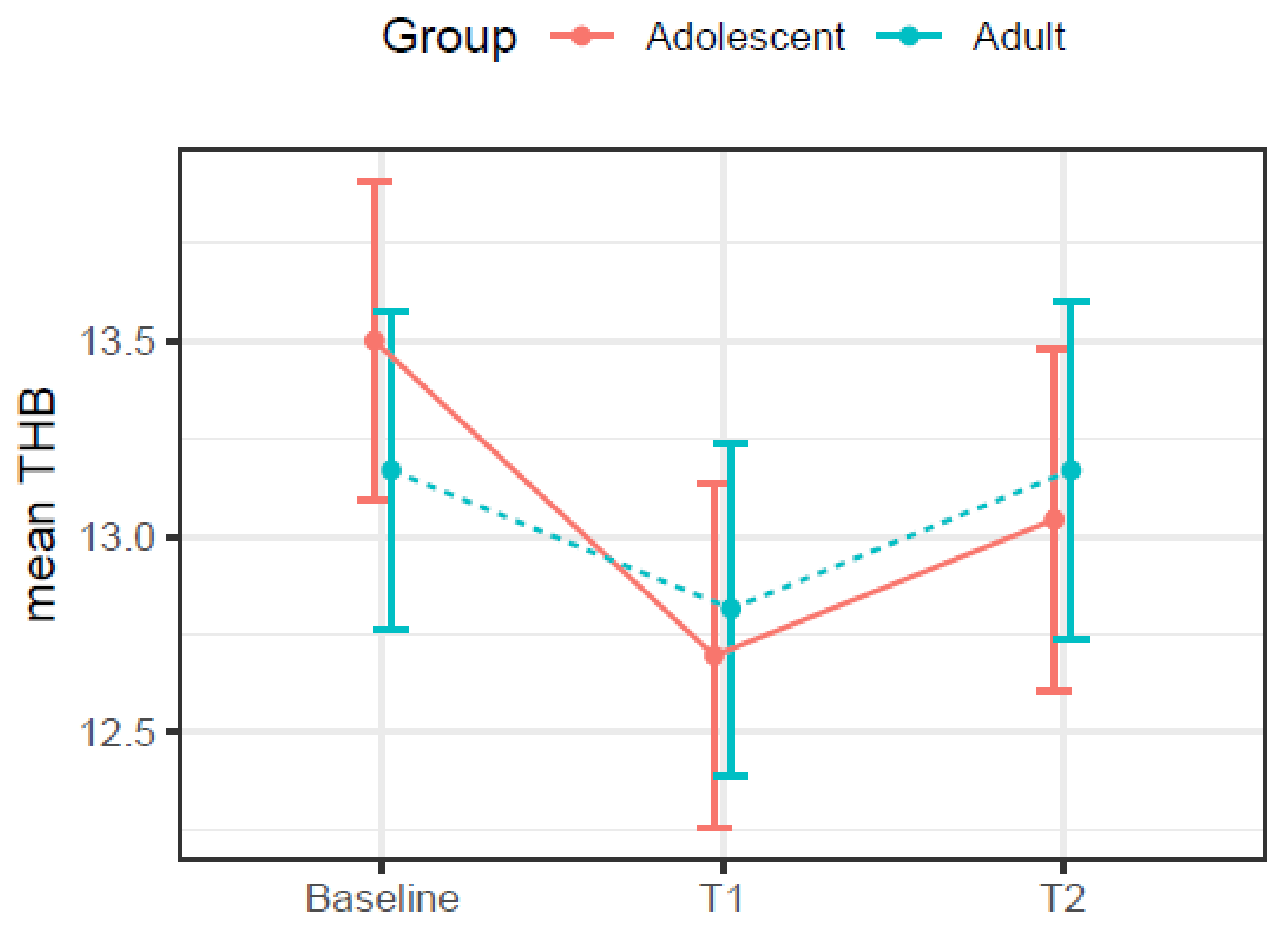
| Adolescents | 13.50 (1.32) | 12.70 (1.65) | 13.04 (1.51) |
| Adults | 13.17 (1.25) | 12.82 (1.27) | 13.17 (1.69) |
| p value a | 0.209 | 0.720 | 0.723 |
| Race | |||
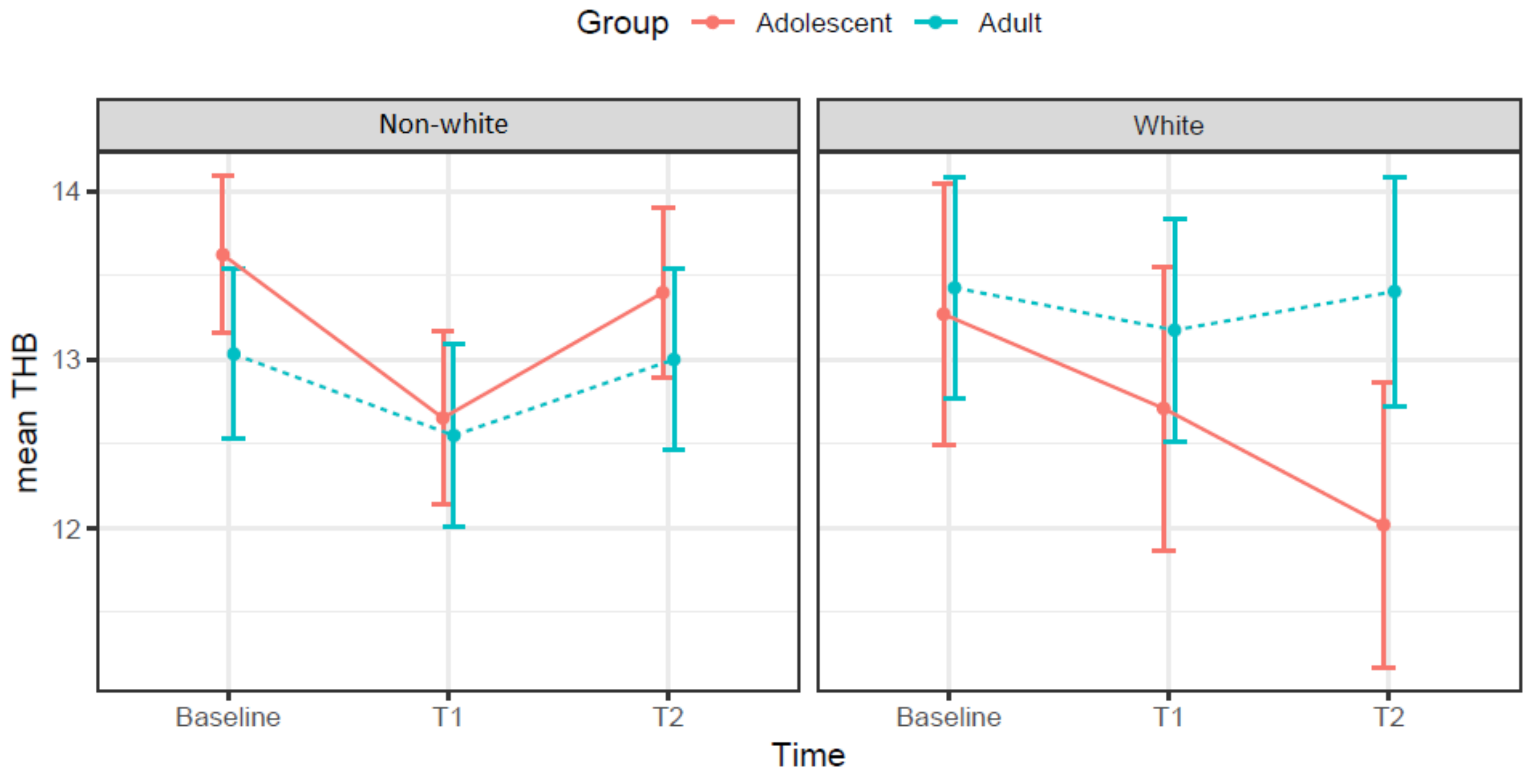
| White | 13.35 (1.44) | 12.96 (1.19) | 12.86 (1.21) |
| Mixed race/black | 13.33 (1.23) | 12.66 (1.57) | 13.23 (1.75) |
| p value a | 0.934 | 0.327 | 0.317 |
| Income sufficiency b | |||
| Very sufficient | 12.34 (1.01) | 12.75 (1.14) | 13.11 (1.39) |
| Suitable | 13.61 (1.28) | 12.90 (1.68) | 13.23 (1.78) |
| Not at all | 13.59 (1.13) | 12.45 (1.10) | 12.81 (1.35) |
| p value c | <0.001 ** | 0.502 | 0.616 |
| Bolsa famíliab | |||
| Yes | 13.38 (1.35) | 12.84 (1.50) | 12.85 (1.49) |
| No | 13.23 (1.18) | 12.62 (1.40) | 13.65 (1.72) |
| p value a | 0.591 | 0.517 | 0.031 |
| Marital status | |||
| Married/Common law | 13.38 (1.33) | 12.91 (1.36) | 13.06 (1.60) |
| Single/Separated/Divorced | 13.16 (1.16) | 12.03 (1.75) | 13.38 (1.57) |
| p value c | 0.489 | 0.033 | 0.531 |
| Childhood SES b | |||
| Good | 13.01 (1.14) | 12.75 (1.40) | 12.75 (1.66) |
| Moderate | 13.49 (1.28) | 12.68 (1.54) | 13.52 (1.68) |
| Poor | 13.62 (1.54) | 13.05 (1.45) | 12.75 (0.92) |
| p value c | 0.152 | 0.738 | 0.090 |
| Self-perceived health | |||
| Good | 13.48 (1.28) | 12.74 (1.51) | 13.11 (1.64) |
| Poor | 12.64 (1.14) | 12.83 (1.07) | 13.11 (1.18) |
| p value | 0.014 a | 0.864 | 0.992 |
| Planned pregnancy | |||
| Yes, entirely | 13.61 (1.45) | 12.80 (1.40) | 13.48 (1.64) |
| Somewhat/Not at all | 13.11 (1.11) | 12.74 (1.51) | 12.83 (1.51) |
| p value a | 0.058 | 0.845 | 0.061 |
| Food security | |||
| Yes | 12.96 (1.23) | 13.21 (1.37) | 12.79 (1.78) |
| No | 13.47 (1.29) | 12.62 (1.46) | 13.20 (1.53) |
| p value a | 0.085 | 0.107 | 0.314 |
| Type of delivery d | |||
| Vaginal | 13.34 (1.32) | 12.91 (1.49) | 12.87 (1.41) |
| Cesarean | 13.32 (1.37) | 12.58 (1.43) | 13.33 (1.74) |
| p value a | 0.951 | 0.301 | 0.184 |
| Breastfeeding e | |||
| Yes | 13.40 (1.35) | 12.76 (1.44) | 13.05 (1.55) |
| No | 12.65 (0.77) | 13.03 (0.96) | 13.68 (1.87) |
| p value a | 0.277 | 0.301 | 0.434 |
| Baseline (n = 100) | T1 (n = 88) | T2 (n = 86) | ||||
|---|---|---|---|---|---|---|
| Coefficient | p a | Coefficient | p a | Coefficient | p a | |
| Years of schooling | −0.087 | 0.395 | −0.035 | 0.748 | −0.046 | 0.673 |
| Weight | 0.094 | 0.357 b | 0.218 | 0.043 b | −0.860 | 0.429 b |
| Height | 0.093 | 0.363 b | 0.226 | 0.036 b | 0.049 | 0.651 |
| Number of prenatal appointments | −0.118 | 0.301 | −0.084 | 0.460 | −0.006 | 0.960 |
| Age at menarche | 0.044 | 0.670 | 0.087 | 0.423 | 0.015 | 0.892 |
| Variables | β | 95% CI | p Value |
|---|---|---|---|
| Intercept | 13.56 | 13.10, 14.02 | <0.001 |
| Group (adult) | −0.67 | −1.28, −0.06 | 0.033 |
| Time 1-Baseline | −0.86 | −1.43, −0.28 | 0.003 |
| Time 2-baseline | −0.49 | −1.06, 0.08 | 0.092 |
| Race (white) | −0.55 | −1.13, 0.04 | 0.067 |
| SRH (poor) | −0.44 | −0.94, 0.07 | 0.090 |
| Planned pregnancy (Yes, entirely) | 0.39 | 0.02, 0.75 | 0.039 |
| Group (adult) × Time(T1) | 0.47 | −0.33, 1.26 | 0.252 |
| Group (adult) × Time(T2) | 0.46 | −0.33, 1.26 | 0.255 |
| Group (adult) × Race (white) | 1.01 | 0.23, 1.80 | 0.012 |
| Adolescents | Adults | |||
|---|---|---|---|---|
| Variables | β (95% CI) | p | β (95% CI) | p |
| Intercept | 13.62 (13.09, 14.15) | <0.001 | 12.83 (12.36, 13.31) | <0.001 |
| Time 1-baseline | −0.86 (−1.42, −0.30) | 0.003 | −0.40 (−0.95, 0.15) | 0.158 |
| Time 2-baseline | −0.48 (−1.04, 0.08) | 0.092 | −0.03 (−0.59, 0.52) | 0.903 |
| Planned pregnancy (yes) | 0.18 (−0.43, 0.79) | 0.560 | 0.57 (0.11, 1.02) | 0.015 |
| Race (white) | −0.56 (−1.23, 0.11) | 0.100 | 0.46 (−0.01, 0.93) | 0.057 |
| SRH (poor) | −0.28 (−1.06, 0.51) | 0.486 | −0.58 (−1.22, 0.06) | 0.075 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, R.N.d.; Pirkle, C.M.; Sentell, T.; Peltzer, N.K.; Wu, Y.Y.; Domingues, M.R.; Câmara, S.M.A. Total Hemoglobin Trajectories from Pregnancy to Postpartum in Rural Northeast Brazil: Differences between Adolescent and Adult Women. Int. J. Environ. Res. Public Health 2022, 19, 3897. https://doi.org/10.3390/ijerph19073897
Silva RNd, Pirkle CM, Sentell T, Peltzer NK, Wu YY, Domingues MR, Câmara SMA. Total Hemoglobin Trajectories from Pregnancy to Postpartum in Rural Northeast Brazil: Differences between Adolescent and Adult Women. International Journal of Environmental Research and Public Health. 2022; 19(7):3897. https://doi.org/10.3390/ijerph19073897
Chicago/Turabian StyleSilva, Raí Nabichedí da, Catherine M. Pirkle, Tetine Sentell, Nicole Kahielani Peltzer, Yan Yan Wu, Marlos R. Domingues, and Saionara M. A. Câmara. 2022. "Total Hemoglobin Trajectories from Pregnancy to Postpartum in Rural Northeast Brazil: Differences between Adolescent and Adult Women" International Journal of Environmental Research and Public Health 19, no. 7: 3897. https://doi.org/10.3390/ijerph19073897