
Alcohol and Cannabis Use Trajectories and Outcomes in a Sample of Hispanic, White, and Asian Sexual and Gender Minority Emerging Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Alcohol and Cannabis Use Trajectories
2.1.2. Sexual Orientation and/or Gender Minority Status
2.1.3. Racial/Ethnic Identity Groups
2.1.4. Covariates
2.1.5. Outcomes at Wave 12
2.2. Analyses
3. Results
3.1. Sample Characteristics
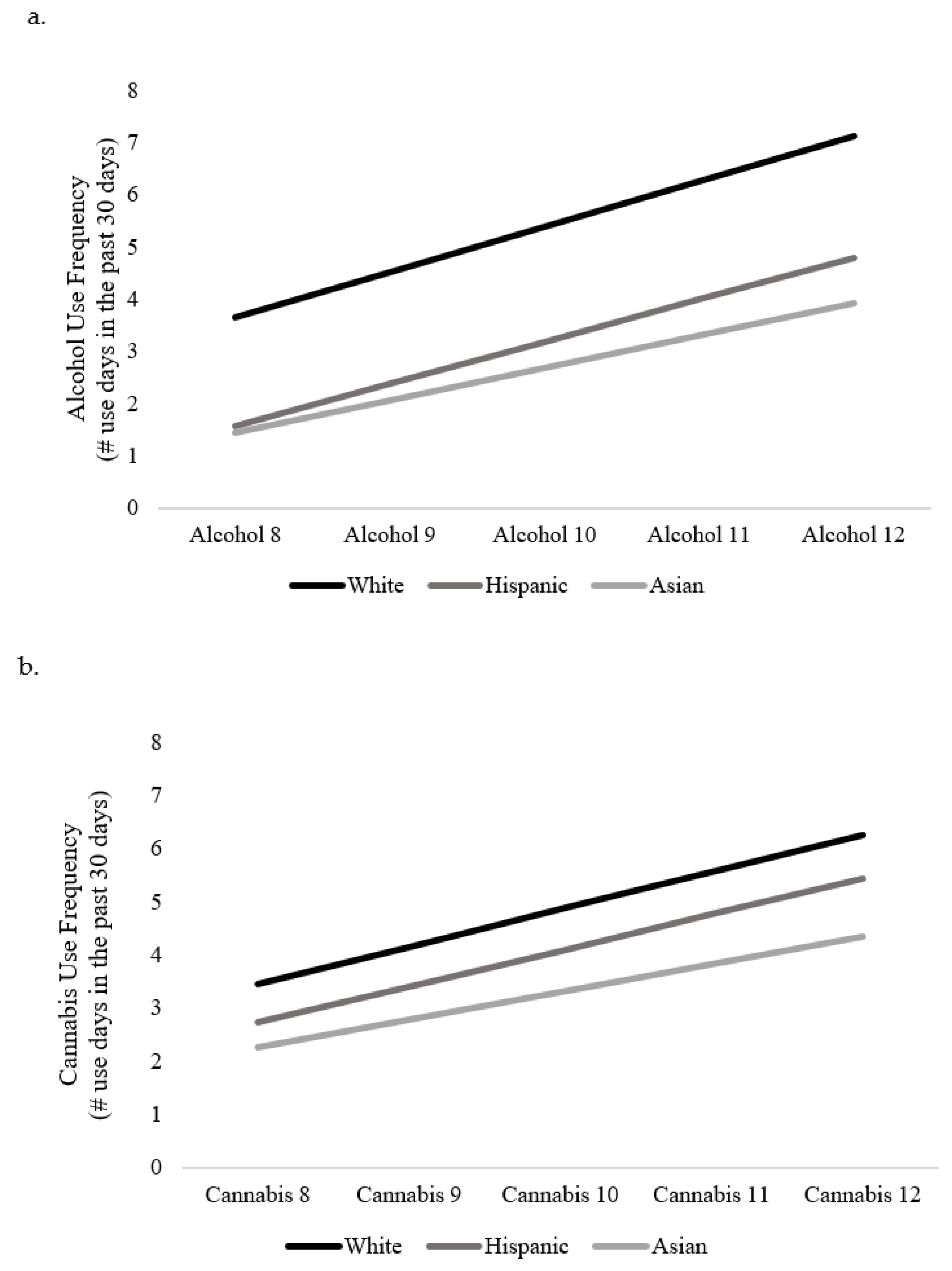
3.2. Predictors of Intercept and Slope of Alcohol Use
3.3. Racial/Ethnic Differences for Wave 12 Outcomes Controlling for Alcohol Use Trajectories
3.4. Predictors of Intercept and Slope of Cannabis Use
3.5. Racial/Ethnic Differences for Wave 12 Outcomes Controlling for Cannabis Use Trajectories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine. The Health of Lesbian, Gay, Bisexual and Transgender People: Building a Foundation for Better Understanding; The National Academies: Washington, DC, USA, 2011. [Google Scholar]
- National Academies of Sciences. Engineering and Medicine, Understanding the Well-Being of LGBTQI+ Populations; Patterson, C.J., Sepúlveda, M.-J., White, J., Eds.; The National Academies Press: Washington, DC, USA, 2020; p. 436. [Google Scholar]
- Meyer, I.H. Minority stress and mental health in gay men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.C.; Arriaga, A.S.; Gobble, T.; Wille, L. Stress and substance use among sexual and gender minority individuals across the lifespan. Neurobiol. Stress 2018, 10, 100146. [Google Scholar] [CrossRef]
- Goldbach, J.T.; Gibbs, J. A developmentally informed adaptation of minority stress for sexual minority adolescents. J. Adolesc. 2016, 55, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, A.; Davis, J.P.; Goldbach, J.T. Gender and Sexual Identities Predicting Patterns of Co-occurring Health Risks Among Sexual Minority Youth: A Latent Class Analysis Approach. Prev. Sci. 2020, 21, 908–916. [Google Scholar] [CrossRef]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanf. Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- Schuler, M.S.; Prince, D.M.; Breslau, J.; Collins, R.L. Substance Use Disparities at the Intersection of Sexual Identity and Race/Ethnicity: Results from the 2015–2018 National Survey on Drug Use and Health. LGBT Health 2020, 7, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Parent, M.C.; DeBlaere, C.; Moradi, B. Approaches to Research on Intersectionality: Perspectives on Gender, LGBT, and Racial/Ethnic Identities. Sex Roles 2013, 68, 639–645. [Google Scholar] [CrossRef]
- Bowleg, L. The Problem with the Phrase Women and Minorities: Intersectionality—an Important Theoretical Framework for Public Health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef]
- Balsam, K.F.; Molina, Y.; Blayney, J.A.; Dillworth, T.; Zimmerman, L.; Kaysen, D. Racial/ethnic differences in identity and mental health outcomes among young sexual minority women. Cult. Divers. Ethn. Minor. Psychol. 2015, 21, 380–390. [Google Scholar] [CrossRef]
- Halkitis, P.N.; Siconolfi, D.E.; Stults, C.B.; Barton, S.; Bub, K.; Kapadia, F. Modeling substance use in emerging adult gay, bisexual, and other YMSM across time: The P18 cohort study. Drug Alcohol. Depend. 2014, 145, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Substance Abuse and Mental Health Services Administration. 2019 NSDUH Detailed Tables; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2020. [Google Scholar]
- Adams, S.H.; Knopf, D.K.; Park, M.J. Prevalence and Treatment of Mental Health and Substance Use Problems in the Early Emerging Adult Years in the United States. Emerg. Adulthood 2013, 2, 163–172. [Google Scholar] [CrossRef]
- Schulenberg, J.E.; Patrick, M.E.; Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Miech, R.A. Monitoring the Future National Survey Results on Drug Use, 1975–2020: Volume II, College Students and Adults Ages 19–60; Institute for Social Research, The University of Michigan: Ann Arbor, MI, USA, 2021. [Google Scholar]
- Takeda, K.; Rosenthal, L.; Arora, P.G. Internalizing symptoms, intersectional discrimination, and social support among Asian-Pacific Islander sexual and gender minority adults. Cult. Divers. Ethn. Minority Psychol. 2021, 27, 418–430. [Google Scholar] [CrossRef]
- Becerra, M.B.; Rodriquez, E.J.; Avina, R.M.; Becerra, B.J. Experiences of violence and mental health outcomes among Asian American transgender adults in the United States. PLoS ONE 2021, 16, e0247812. [Google Scholar] [CrossRef] [PubMed]
- Tucker, J.S.; Rodriguez, A.; Davis, J.P.; Klein, D.J.; D’Amico, E.J. Simultaneous trajectories of alcohol and cannabis use from adolescence to emerging adulthood: Associations with role transitions and functional outcomes. Psychol. Addict. Behav. 2021, 35, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Schulte, M.T.; Hser, Y.-I. Substance Use and Associated Health Conditions throughout the Lifespan. Public Health Rev. 2013, 35, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, K.M.; Meehan, B.T.; Trim, R.S.; Chassin, L. Marker or mediator? The effects of adolescent substance use on young adult educational attainment. Addiction 2006, 101, 1730–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, I.; Henderson, J.; Goldstein, A.; Peterson-Badali, M. Youth Perspectives on the Transition to Adulthood. Emerg. Adulthood 2015, 4, 92–103. [Google Scholar] [CrossRef]
- Silins, E.; Horwood, L.J.; Patton, G.C.; Fergusson, D.M.; Olsson, C.A.; Hutchinson, D.M.; Spry, E.; Toumbourou, J.W.; Degenhardt, L.; Swift, W.; et al. Young adult sequelae of adolescent cannabis use: An integrative analysis. Lancet Psychiatry 2014, 1, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Green, K.M.; Musci, R.J.; Johnson, R.M.; Matson, P.A.; Reboussin, B.A.; Ialongo, N.S. Outcomes associated with adolescent marijuana and alcohol use among urban young adults: A prospective study. Addict. Behav. 2015, 53, 155–160. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, E.J.; Tucker, J.S.; Miles, J.N.V.; Ewing, B.A.; Shih, R.A.; Pedersen, E.R. Alcohol and marijuana use trajectories in a diverse longitudinal sample of adolescents: Examining use patterns from age 11 to 17 years. Addiction 2016, 111, 1825–1835. [Google Scholar] [CrossRef]
- Dunbar, M.S.; Tucker, J.S.; Ewing, B.A.; Parast, L.; Pedersen, E.R.; Rodriguez, A.; D’Amico, E.J. Ethnic Differences in Cigarette Use Trajectories and Health, Psychosocial, and Academic Outcomes. J. Adolesc. Health 2017, 62, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Tucker, J.S.; Rodriguez, A.; Dunbar, M.S.; Pedersen, E.R.; Davis, J.P.; Shih, R.A.; D’Amico, E.J. Cannabis and tobacco use and co-use: Trajectories and correlates from early adolescence to emerging adulthood. Drug Alcohol Depend. 2019, 204, 107499. [Google Scholar] [CrossRef] [PubMed]
- Kakade, M.; Duarte, C.S.; Liu, X.; Fuller, C.J.; Drucker, E.; Hoven, C.; Fan, B.; Wu, P. Adolescent Substance Use and Other Illegal Behaviors and Racial Disparities in Criminal Justice System Involvement: Findings from a US National Survey. Am. J. Public Health 2012, 102, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, M.S.; Siconolfi, D.; Rodriguez, A.; Seelam, R.; Davis, J.P.; Tucker, J.S.; D’Amico, E.J. Alcohol use and cannabis use trajectories and sexual/gender minority disparities in young adulthood. Psychol. Addict. Behav. 2022. [Google Scholar] [CrossRef]
- Poteat, V.P.; Scheer, J.R.; Chong, E.S.K. Sexual orientation-based disparities in school and juvenile justice discipline: A multiple group comparison of contributing factors. J. Educ. Psychol. 2016, 108, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Himmelstein, K.E.W.; Brückner, H. Criminal-Justice and School Sanctions Against Nonheterosexual Youth: A National Longitudinal Study. Pediatrics 2011, 127, 49–57. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, E.J.; Tucker, J.S.; Miles, J.N.V.; Zhou, A.J.; Shih, R.A.; Green, H.D. Preventing Alcohol Use with a Voluntary After-School Program for Middle School Students: Results from a Cluster Randomized Controlled Trial of CHOICE. Prev. Sci. 2012, 13, 415–425. [Google Scholar] [CrossRef]
- Johnston, L.D.; O’Malley, P.M.; Miech, R.A.; Bachman, J.G.; Schulenberg, J.E. Monitoring the Future National Survey Results on Drug Use, 1975–2015: Overview, Key Findings on Adolescent Drug Use; Institute for Social Research: Ann Arbor, MI, USA, 2016. [Google Scholar]
- Economic Research Service. National Food Security Surveys—Measurement; U.S. Department of Agriculture: Washington, DC, USA, 2021. [Google Scholar]
- Baggio, S.; Iglesias, K.; Studer, J.; Gmel, G. An 8-Item Short Form of the Inventory of Dimensions of Emerging Adulthood (IDEA) Among Young Swiss Men. Eval. Health Prof. 2014, 38, 246–254. [Google Scholar] [CrossRef] [Green Version]
- DeWalt, D.A.; Thissen, D.; Stucky, B.D.; Langer, M.M.; DeWitt, E.M.; Irwin, D.E.; Lai, J.-S.; Yeatts, K.B.; Gross, H.E.; Taylor, O.; et al. PROMIS Pediatric Peer Relationships Scale: Development of a peer relationships item bank as part of social health measurement. Health Psychol. 2013, 32, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys: Results from Two Population-Based Studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Schat, A.C.H.; Kelloway, E.K.; Desmarais, S. The Physical Health Questionnaire (PHQ): Construct Validation of a Self-Report Scale of Somatic Symptoms. J. Occup. Health Psychol. 2005, 10, 363–381. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Buysse, D.J.; Yu, L.; Moul, D.E.; Germain, A.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Shablesky-Cade, M.A.; Pilkonis, P.A. Development and Validation of Patient-Reported Outcome Measures for Sleep Disturbance and Sleep-Related Impairments. Sleep 2010, 33, 781–792. [Google Scholar] [CrossRef] [Green Version]
- Center for Behavioral Health Statistics and Quality. 2019 National Survey on Drug Use and Health (NSDUH): CAI Specifications for Programming (English Version); Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018. [Google Scholar]
- Duncan, T.E.; Duncan, S.C.; Strycker, L.A. An Introduction to Latent Variable Growth Curve Modeling: Concepts, Issues, and Applications; Lawrence Erlbaum Associates: Malwah, NJ, USA, 1999. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Coulter, R.W.; Ware, D.; Fish, J.N.; Plankey, M.W. Latent Classes of Polysubstance Use Among Adolescents in the United States: Intersections of Sexual Identity with Sex, Age, and Race/Ethnicity. LGBT Health 2019, 6, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.M.; Motter, L.A.; Tanis, J. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey; National Center for Transgender Equality and National Gay and Lesbian Task Force: Washington, DC, USA, 2011. [Google Scholar]
- Schuler, M.S.; Prince, D.M.; Collins, R.L. Disparities in Social and Economic Determinants of Health by Sexual Identity, Gender, and Age: Results from the 2015–2018 National Survey on Drug Use and Health. LGBT Health 2021, 8, 330–339. [Google Scholar] [CrossRef]
- Bowleg, L. When Black + Lesbian + Woman ≠ Black Lesbian Woman: The Methodological Challenges of Qualitative and Quantitative Intersectionality Research. Sex Roles 2008, 59, 312–325. [Google Scholar] [CrossRef]
- Shih, R.A.; Tucker, J.S.; Miles, J.N.V.; Ewing, B.A.; Pedersen, E.R.; D’Amico, E.J. Differences in substance use and substance use risk factors by Asian subgroups. Asian Am. J. Psychol. 2015, 6, 38–46. [Google Scholar] [CrossRef]


{kind=link}
| Full Analytic Sample (n = 359) | White (n = 107) | Hispanic (n = 188) | Asian (n = 64) | Group Difference | |
|---|---|---|---|---|---|
| % (n)/ Mean (SD) | % (n)/ Mean (SD) | % (n)/ Mean (SD) | % (n)/ Mean (SD) | p | |
| Race/ethnicity | |||||
| White | 29.8% (107) | -- | -- | -- | -- |
| Asian | 17.8% (64) | -- | -- | -- | |
| Hispanic | 52.4% (188) | -- | -- | -- | |
| Age (wave 8) | 18.3 (0.8) | 18.3 (0.7) | 18.2 (0.8) | 18.2 (0.8) | 0.4717 |
| Age (wave 12) | 22.5 (0.8) | 22.6 (0.7) | 22.5 (0.8) | 22.4 (0.7) | 0.4222 |
| Assigned Sex at Birth | |||||
| Male | 32.0% (115) | 29.9% (32) | 33.0% (62) | 32.8% (21) | 0.8533 |
| Female | 68.0% (244) | 70.1% (75) | 67.0% (126) | 67.2% (43) | |
| Intersex/other | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Gender Identity | |||||
| Man | 29.8% (107) | 27.1% (29) | 31.9% (60) | 28.1% (18) | 0.3105 |
| Woman | 64.4% (231) | 62.6% (67) | 63.8% (120) | 68.8% (44) | |
| Gender neutral | 4.2% (15) | 6.5% (7) | 3.2% (6) | 3.1% (2) | |
| Another identity | 1.7% (6) | 3.7% (4) | 1.1% (2) | 0 (0) | |
| Mother’s Education | |||||
| <High school | 16.2% (58) | 1.9% (2) | 28.7% (54) | 3.1% (2) | <0.0001 |
| High school | 15.6% (56) | 12.2% (13) | 18.1% (34) | 14.1% (9) | |
| Some college | 20.6% (74) | 22.4% (24) | 21.8% (41) | 14.1% (9) | |
| Associate’s degree | 7.0% (25) | 7.5% (8) | 6.9% (13) | 6.3% (4) | |
| College degree or higher | 37.1% (133) | 52.3% (56) | 20.7% (39) | 59.4% (38) | |
| Don’t know | 3.6% (13) | 3.7% (4) | 3.7% (7) | 3.1% (2) | |
| SGM characteristics a | |||||
| Sexual orientation | |||||
| Straight/heterosexual | 8.4% (30) | 6.5% (7) | 7.5% (14) | 14.1% (9) | 0.2314 |
| Gay | 14.2% (51) | 11.2% (12) | 16.5% (31) | 12.5% (8) | |
| Lesbian | 9.8% (35) | 14.0% (15) | 8.5% (16) | 6.3% (4) | |
| Bisexual | 57.1% (205) | 57.0% (61) | 59.0% (111) | 51.6% (33) | |
| Questioning | 10.6% (38) | 11.2% (12) | 8.5% (16) | 15.6% (10) | |
| Asexual | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Same-sex vaginal/anal sex | 47.1% (168) | 41.5% (44) | 52.9% (99) | 39.1% (25) | 0.0623 |
| Different gender identity vs. sex assigned at birth | 8.4% (30) | 15.9% (17) | 4.3% (8) | 7.8% (5) | 0.0024 |
| Gender neutral or other gender identity | 5.9% (21) | 10.3% (11) | 4.3% (8) | 3.1% (2) | 0.1937 |
| Transgender identity | 2.8% (10) | 6.5% (7) | 0.5% (1) | 3.1% (2) | 0.0104 |
| Intersex/other | 0 (0) | 0 (0) | 0 (0) | 0 (0) | -- |
| Hispanic (Reference Group Is White) | Asian (Reference Group Is White) | ||
|---|---|---|---|
| Domain | Outcome Variable | Standardized Beta (95% CI) p-Value | Standardized Beta (95% CI) p-Value |
| Education | Educational attainment post-high school (yes) | −0.374 (−0.682, −0.066) p = 0.017 | 0.070 (−0.359, 0.499) p = 0.749 |
| Employment and economic stability | Unemployed full- or part-time (yes) | 0.069 (−0.282, 0.421) p = 0.699 | 0.039 (−0.384, 0.461) p = 0.857 |
| Number of times fired from job in past year | 0.141 (−0.305, 0.587) p = 0.535 | 0.009 (−0.560, 0.578) p = 0.975 | |
| Experienced homelessness (yes) | −0.348 (−0.736, 0.041) p = 0.079 | −0.332 (−0.875, 0.211) p = 0.231 | |
| Experienced food insecurity (yes) | 0.126 (−0.190, 0.443) p = 0.434 | −0.133 (−0.546, 0.279) p = 0.526 | |
| Transition to adult roles | IDEA scale | −0.272 (−0.568, 0.024) p = 0.072 | −0.040 (−0.405, 0.324) p = 0.828 |
| Criminal justice involvement | Instances of being in trouble with police in past year | 0.096 (−0.338, 0.530) p = 0.665 | 0.164 (−0.333, 0.662) p = 0.517 |
| Social functioning | PROMIS Social Functioning score | 0.094 (−0.161, 0.349) p = 0.472 | 0.147 (−0.181, 0.475) p = 0.379 |
| Loneliness score | −0.164 (−0.442, 0.114) p = 0.247 | −0.122 (−0.457, 0.212) p = 0.474 | |
| Physical health | Physical health score | −0.172 (−0.436, 0.091) p = 0.200 | −0.193 (−0.536, 0.150) p = 0.271 |
| Behavioral health | Anxiety—GAD-7 score | 0.043 (−0.231, 0.318 ) p = 0.758 | −0.145 (−0.485, 0.196) p = 0.405 |
| Depression—PHQ 8 score | 0.037 (−0.241, 0.315) p = 0.793 | −0.076 (−0.430, 0.279) p = 0.675 | |
| PTSD—PCL-5 score | 0.025 (−0.355, 0.406) p = 0.897 | 0.137 (−0.433, 0.706) p = 0.638 | |
| Sex with casual partner after using alcohol, marijuana, or other drugs (yes) | −0.067 (−0.423, 0.289) p = 0.712 | −0.579 (−1.102, −0.056) p = 0.030 | |
| Sex with casual partner without condom (yes) | 0.087 (−0.302, 0.475) p = 0.662 | −0.508 (−1.079, 0.064) p = 0.082 | |
| Sleep quality | 0.042 (−0.223, 0.306) p = 0.758 | −0.105 (−0.457, 0.247) p = 0.560 | |
| Number of casual sex partners | 0.101 (−0.371, 0.572) p = 0.676 | −0.012 (−0.516, 0.493) p = 0.963 | |
| Unmet treatment need | Unmet treatment need for alcohol or other drug use (yes) | −0.019 (−0.543, 0.505) p = 0.943 | −0.195 (−0.950, 0.560) p = 0.613 |
| Unmet treatment need for mental health (yes) | −0.074 (−0.396, 0.249) p = 0.655 | −0.130 (−0.554, 0.294) p = 0.549 |
| Hispanic (Reference Group Is White) | Asian (Reference Group Is White) | ||
|---|---|---|---|
| Domain | Outcome Variable | Standardized Beta (95% CI) p-Value | Standardized Beta (95% CI) p-Value |
| Education | Educational attainment post-high school (yes) | −0.405 (−0.699, −0.112) p = 0.007 | −0.007 (−0.388, 0.374) p = 0.971 |
| Employment and economic stability | Unemployed full- or part-time (yes) | 0.039 (−0.298, 0.376) p = 0.820 | −0.003 (−0.407, 0.401) p = 0.990 |
| Number of times fired from job in past year | 0.169 (−0.080, 0.418) p = 0.183 | 0.043 (−0.267, 0.353) p = 0.788 | |
| Experienced homelessness (yes) | −0.303 (−0.678, 0.072) p = 0.113 | −0.261 (−0.755, 0.232) p = 0.299 | |
| Experienced food insecurity (yes) | 0.239 (−0.061, 0.539) p = 0.119 | −0.001 (−0.400, 0.397) p = 0.994 | |
| Transition to adult roles | IDEA scale | −0.336 (−0.577, −0.095) p = 0.006 | −0.132 (−0.436, 0.172) p = 0.395 |
| Criminal justice involvement | Instances of being in trouble with police in past year | 0.096 (−0.155, 0.346) p = 0.455 | 0.167 (−0.144, 0.477) p = 0.293 |
| Social functioning | PROMIS Social Functioning score | −0.003 (−0.252, 0.247) p = 0.983 | 0.017 (−0.293, 0.328) p = 0.913 |
| Loneliness score | −0.139 (−0.390, 0.112) p = 0.277 | −0.104 (−0.415, 0.208) p = 0.514 | |
| Physical health | Physical health score | −0.171 (−0.420, 0.079) p = 0.180 | −0.190 (−0.500, 0.120) p = 0.230 |
| Behavioral health | Anxiety—GAD-7 score | −0.009 (−0.260, 0.242) p = 0.945 | −0.217 (−0.528, 0.094) p = 0.171 |
| Depression—PHQ 8 score | 0.017 (−0.233, 0.268) p = 0.893 | −0.107 (−0.418, 0.204) p = 0.502 | |
| PTSD—PCL-5 score | −0.181 (−0.511, 0.149) p = 0.282 | 0.038 (−0.445, 0.520) p = 0.878 | |
| Sex with casual partner after using alcohol, marijuana, or other drugs (yes) | −0.190 (−0.538, 0.158) p = 0.285 | −0.737 (−1.268, −0.206) p = 0.007 | |
| Sex with casual partner without condom (yes) | 0.047 (−0.332, 0.427) p = 0.806 | −0.589 (−1.141, −0.037) p = 0.037 | |
| Sleep quality | 0.035 (−0.213, 0.284) p = 0.780 | −0.110 (−0.419, 0.199) p = 0.486 | |
| Number of casual sex partners | 0.118 (−0.135, 0.372) p = 0.359 | −0.003 (−0.317, 0.310) p = 0.983 | |
| Unmet treatment need | Unmet treatment need for alcohol or other drug use (yes) | −0.104 (−0.620, 0.413) p = 0.694 | −0.371 (−1.101, 0.360) p = 0.320 |
| Unmet treatment need for mental health (yes) | −0.199 (−0.507, 0.108) p = 0.203 | −0.293 (−0.701, 0.116) p = 0.160 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dunbar, M.S.; Siconolfi, D.; Rodriguez, A.; Seelam, R.; Davis, J.P.; Tucker, J.S.; D’Amico, E.J. Alcohol and Cannabis Use Trajectories and Outcomes in a Sample of Hispanic, White, and Asian Sexual and Gender Minority Emerging Adults. Int. J. Environ. Res. Public Health 2022, 19, 2059. https://doi.org/10.3390/ijerph19042059
Dunbar MS, Siconolfi D, Rodriguez A, Seelam R, Davis JP, Tucker JS, D’Amico EJ. Alcohol and Cannabis Use Trajectories and Outcomes in a Sample of Hispanic, White, and Asian Sexual and Gender Minority Emerging Adults. International Journal of Environmental Research and Public Health. 2022; 19(4):2059. https://doi.org/10.3390/ijerph19042059
Chicago/Turabian StyleDunbar, Michael S., Daniel Siconolfi, Anthony Rodriguez, Rachana Seelam, Jordan P. Davis, Joan S. Tucker, and Elizabeth J. D’Amico. 2022. "Alcohol and Cannabis Use Trajectories and Outcomes in a Sample of Hispanic, White, and Asian Sexual and Gender Minority Emerging Adults" International Journal of Environmental Research and Public Health 19, no. 4: 2059. https://doi.org/10.3390/ijerph19042059