
The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
- Population: CBCT scans of oral and maxillofacial area in humans.
- Index test: Diagnostic tool based on semi-automatic and fully automatic algorithm.
- Reference test: Experts judge or manual tracing.
- Diagnosis of Interest: IAC/IAN localization.
2.1. Searching Strategy
2.2. Eligibility Criteria
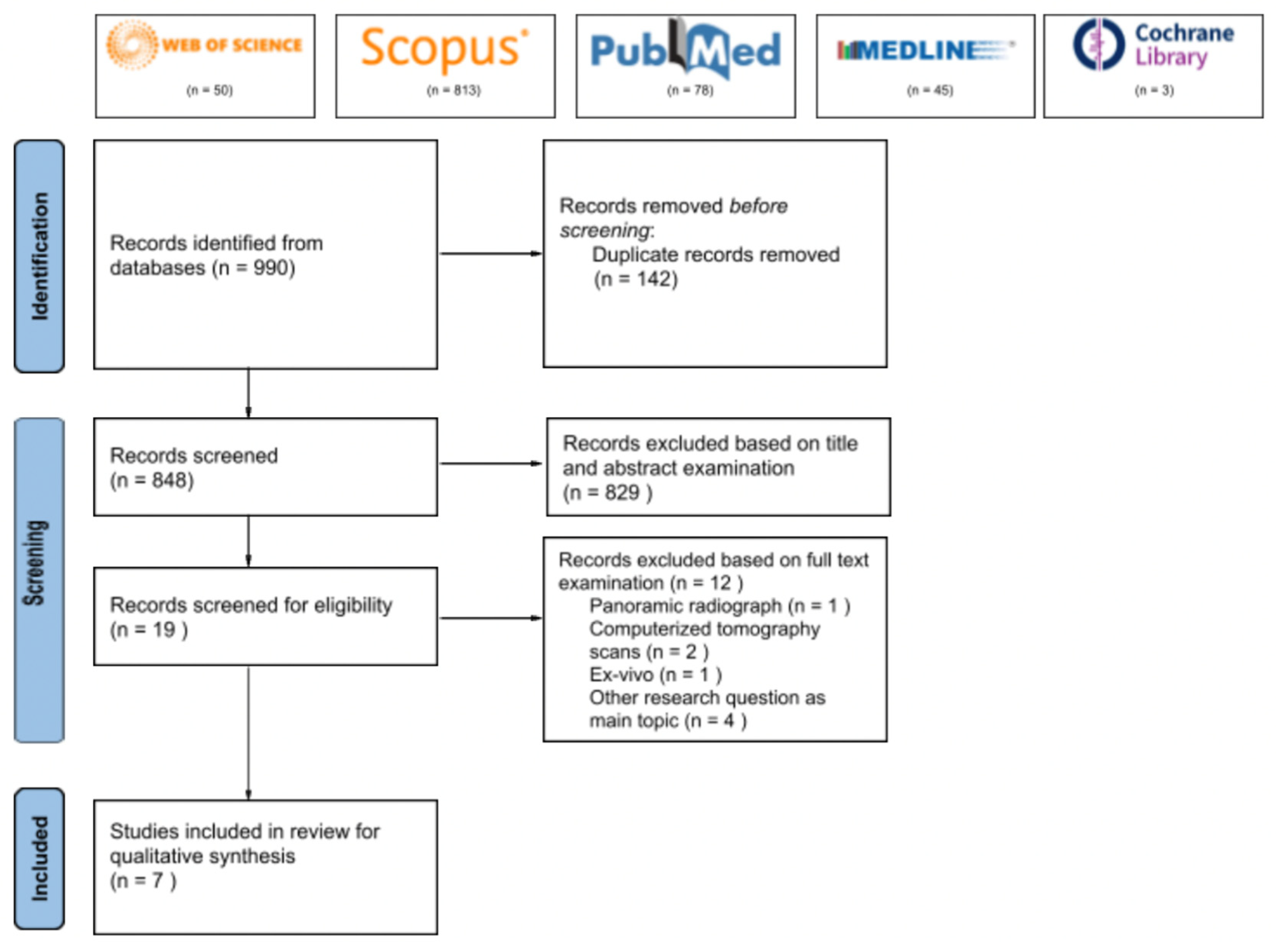
2.3. Study Selection
2.4. Critical Appraisal and Data Extraction
3. Results
3.1. Search Result
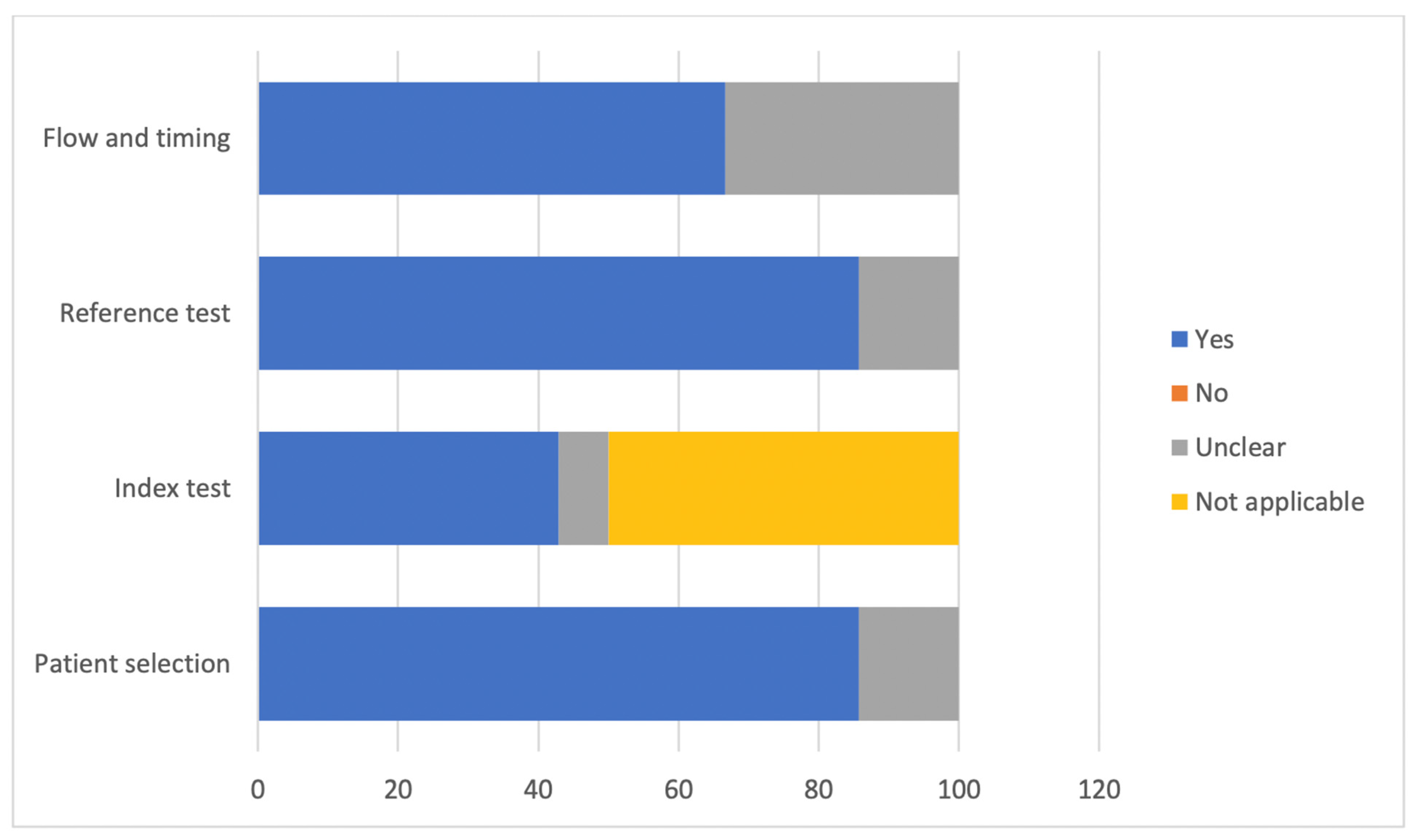
3.2. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Amisha Malik, P.; Pathania, M.; Rathaur, V.K. Overview of artificial intelligence in medicine. J. Fam. Med. Prim. Care 2019, 8, 2328–2331. [Google Scholar] [CrossRef]
- Panch, T.; Szolovits, P.; Atun, R. Artificial intelligence, machine learning and health systems. J. Glob. Health 2018, 8, 020303. [Google Scholar] [CrossRef]
- Helm, J.M.; Swiergosz, A.M.; Haeberle, H.S.; Karnutaet, J.M.; Schaffer, J.L.; Krebs, V.E.; Spitzer, A.I.; Ramkumar, P.N. Machine Learning and Artificial Intelligence: Definitions, Applications, and Future Directions. Curr. Rev. Musculoskelet. Med. 2020, 13, 69–76. [Google Scholar] [CrossRef]
- Lee, R.S.T. Artificial Intelligence in Daily Life; Springer: Singapore, 2020. [Google Scholar] [CrossRef]
- Lee, D.; Yoon, S.N. Application of Artificial Intelligence-Based Technologies in the Healthcare Industry: Opportunities and Challenges. Int. J. Environ. Res. Public Health 2021, 18, 271. [Google Scholar] [CrossRef]
- Bohr, A.; Memarzadeh, K. The rise of artificial intelligence in healthcare applications. In Artificial Intelligence in Healthcare; Academic Press: Cambridge, MA, USA, 2020; pp. 25–60. [Google Scholar] [CrossRef]
- Benke, K.; Benke, G. Artificial Intelligence and Big Data in Public Health. Int. J. Environ. Res. Public Health 2018, 15, 2796. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, D.A.; Rosman, G.; Rus, D.; Meireles, O.R. Artificial Intelligence in Surgery: Promises and Perils. Ann. Surg. 2018, 268, 70–76. [Google Scholar] [CrossRef]
- Mintz, Y.; Brodie, R. Introduction to artificial intelligence in medicine. Minim. Invasive Ther. Allied Technol. 2019, 28, 73–81. [Google Scholar] [CrossRef]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Hassani, H.; Andi, P.A.; Ghodsi, A.; Norouzi, K.; Komendantova, N.; Unger, S. Shaping the Future of Smart Dentistry: From Artificial Intelligence (AI) to Intelligence Augmentation (IA). IoT 2021, 2, 510–523. [Google Scholar] [CrossRef]
- Samiuddin Ahmed, M.; Chaturya, K.; Vinay Chandra Tiwari, R.; Virk, I.; Kumar Gulia, S.; Rajkumar Pandey, P.; Tiwari, H. Digital Dentistry-New Era in Dentistry. J. Adv. Med. Dent. Sci. Res. 2020, 8, 67–70. [Google Scholar] [CrossRef]
- Krishna, A.B.; Tanveer, A.; Bhagirath, P.V.; Gannepalli, A. Role of artificial intelligence in diagnostic oral pathology—A modern approach. J. Oral Maxillofac. Pathol. 2020, 24, 152–156. [Google Scholar] [CrossRef]
- Kar, A.; Wreesmann, V.B.; Shwetha, V.; Thakur, S.; Rao, V.U.; Arakeri, G.; Brennan, P.A. Improvement of oral cancer screening quality and reach: The promise of artificial intelligence. J. Oral Pathol. Med. 2020, 49, 727–730. [Google Scholar] [CrossRef]
- Alkilzy, M.; Midani, R.; Höfer, M.; Splieth, C. Improving Toothbrushing with a Smartphone App: Results of a Randomized Controlled Trial. Caries Res. 2019, 53, 628–635. [Google Scholar] [CrossRef]
- Klingberg, G.; Sillén, R.; Norén, J.G. Machine learning methods applied on dental fear and behavior management problems in children. Acta Odontol. Scand. 1999, 57, 207–215. [Google Scholar] [CrossRef]
- Aminoshariae, A.; Kulild, J.; Nagendrababu, V. Artificial Intelligence in Endodontics: Current Applications and Future Directions. J. Endod. 2021, 47, 1352–1357. [Google Scholar] [CrossRef]
- Putra, R.H.; Doi, C.; Yoda, N.; Astuti, E.R.; Sasaki, K. Current applications and development of artificial intelligence for digital dental radiography. Dentomaxillofac. Radiol. 2021, 50, 20210197. [Google Scholar] [CrossRef]
- Brown, J.; Jacobs, R.; Levring Jäghagen, E.; Lindh, C.; Baksi, G.; Schulze, D.; Schulze, R.; European Academy of DentoMaxilloFacial Radiology. Basic training requirements for the use of dental CBCT by dentists: A position paper prepared by the European Academy of DentoMaxilloFacial Radiology. Dentomaxillofac. Radiol. 2014, 43, 20130291. [Google Scholar] [CrossRef] [Green Version]
- Macleod, I.; Heath, N. Cone-beam computed tomography (CBCT) in dental practice. Dent Update 2008, 35, 590–598. [Google Scholar] [CrossRef]
- Hung, K.; Yeung, A.W.K.; Tanaka, R.; Bornstein, M.M. Current Applications, Opportunities, and Limitations of AI for 3D Imaging in Dental Research and Practice. Int. J. Environ. Res. Public Health 2020, 17, 4424. [Google Scholar] [CrossRef]
- Nagi, R.; Aravinda, K.; Rakesh, N.; Gupta, R.; Pal, A.; Mann, A.K. Clinical applications and performance of intelligent systems in dental and maxillofacial radiology: A review. Imaging Sci. Dent 2020, 50, 81–92. [Google Scholar] [CrossRef]
- Nguyen, J.D.; Duong, H. Anatomy, Head and Neck, Alveolar Nerve. StatPearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK546712/ (accessed on 1 November 2021).
- Wolf, K.T.; Brokaw, E.J.; Bell, A.; Joy, A. Variant Inferior Alveolar Nerves and Implications for Local Anesthesia. Anesth. Prog. 2016, 63, 84–90. [Google Scholar] [CrossRef]
- Ozturk, A.; Potluri, A.; Vieira, A.R. Position and course of the mandibular canal in skulls. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 453–458. [Google Scholar] [CrossRef]
- Shavit, I.; Juodzbalys, G. Inferior alveolar nerve injuries following implant placement—Importance of early diagnosis and treatment: A systematic review. J. Oral Maxillofac. Res. 2014, 5, e2. [Google Scholar] [CrossRef] [Green Version]
- Rood, J.P.; Shehab, B.A. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br. J. Oral Maxillofac. Surg. 1990, 28, 20–25. [Google Scholar] [CrossRef]
- Kaasalainen, T.; Ekholm, M.; Siiskonen, T.; Kortesniemi, M. Dental cone beam CT: An updated review. Phys. Med. 2021, 88, 193–217. [Google Scholar] [CrossRef]
- Weckx, A.; Agbaje, J.O.; Sun, Y.; Jacobs, R.; Politis, C. Visualization techniques of the inferior alveolar nerve (IAN): A narrative review. Surg. Radiol. Anat. 2016, 38, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Hung, K.; Montalvao, C.; Tanaka, R.; Kawai, T.; Bornstein, M.M. The use and performance of artificial intelligence applications in dental and maxillofacial radiology: A systematic review. Dentomaxillofac. Radiol. 2020, 49, 20190107. [Google Scholar] [CrossRef]
- Fletcher, R.H.; Fletcher, S.W.; Fletcher, G.S. Clinical Epidemiology: The Essentials. Diagnosis; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 108–144. [Google Scholar]
- Campbell, J.M.; Klugar, M.; Ding, S.; Carmody, D.P.; Hakonsen, S.J.; Jadotte, Y.T.; White, S.; Munn, Z. Diagnostic test accuracy: Methods for systematic review and meta-analysis. Int. J. Evid. Based Healthc. 2015, 13, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Orhan, K.; Bilgir, E.; Bayrakdar, I.S.; Ezhov, M.; Gusarev, M.; Shumilov, E. Evaluation of artificial intelligence for detecting impacted third molars on cone-beam computed tomography scans. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 333–337. [Google Scholar] [CrossRef]
- Liu, M.Q.; Xu, Z.N.; Mao, W.Y.; Li, Y.; Zhang, X.H.; Bai, H.L.; Ding, P.; Fu, K.Y. Deep learning-based evaluation of the relationship between mandibular third molar and mandibular canal on CBCT. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef]
- Bayrakdar, S.K.; Orhan, K.; Bayrakdar, I.S.; Bilgir, E.; Ezhov, M.; Gusarev, M.; Shumilov, E. A deep learning approach for dental implant planning in cone-beam computed tomography images. BMC Med. Imaging 2021, 21, 86. [Google Scholar] [CrossRef]
- Kwak, G.H.; Kwak, E.J.; Song, J.M.; Park, H.R.; Jung, Y.H.; Cho, B.H.; Hui, P.; Hwang, J.J. Automatic mandibular canal detection using a deep convolutional neural network. Sci. Rep. 2020, 10, 5711. [Google Scholar] [CrossRef]
- Jaskari, J.; Sahlsten, J.; Järnstedt, J.; Mehtonen, H.; Karhu, K.; Sundqvist, O.; Hietanen, A.; Varjonen, V.; Mattila, V.; Kaski, K. Deep Learning Method for Mandibular Canal Segmentation in Dental Cone Beam Computed Tomography Volumes. Sci. Rep. 2020, 10, 5842. [Google Scholar] [CrossRef] [Green Version]
- Abdolali, F.; Zoroofi, R.A.; Abdolali, M.; Yokota, F.; Otake, Y.; Sato, Y. Automatic segmentation of mandibular canal in cone beam CT images using conditional statistical shape model and fast marching. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 581–593. [Google Scholar] [CrossRef]
- Bahrampour, E.; Zamani, A.; Kashkouli, S.; Soltanimehr, E.; Jahromi, M.G.; Pourshirazi, Z.S. Accuracy of software designed for automated localization of the inferior alveolar nerve canal on cone beam CT images. Dento Maxillo Facial Radiol. 2016, 45, 20150298. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; Bossuyt, P.M.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Ying, X. An Overview of Overfitting and its Solutions. J. Phys. Conf. Ser. 2019, 1168, 022022. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276. [Google Scholar] [CrossRef]
- Innes, E.; Straker, L. Reliability of work-related assessments. Work 1999, 13, 107–124. [Google Scholar]
- Eusebi, P. E-Mail Methodological Notes Diagnostic Accuracy Measures. Cerebrovasc. Dis. 2013, 36, 267–272. [Google Scholar] [CrossRef]
- Schulze, R.; Heil, U.; Groβ, D.; Bruellmann, D.D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A review. Dentomaxillofacial Radiol. 2011, 40, 265. [Google Scholar] [CrossRef] [Green Version]
- Sounderajah, V.; Ashrafian, H.; Rose, S.; Shah, N.H.; Ghassemi, M.; Golub, R.; Kahn, C.E.; Esteva, A.; Karthikesalingam, A.; Mateen, B.; et al. A quality assessment tool for artificial intelligence-centered diagnostic test accuracy studies: QUADAS-AI. Nat. Med. 2021, 27, 1663–1665. [Google Scholar] [CrossRef]
- Sounderajah, V.; Ashrafian, H.; Aggarwal, R.; de Fauw, J.; Denniston, A.K.; Greaves, F.; Karthikesalingam, A.; King, D.; Liu, X.; Markar, S.R.; et al. Developing specific reporting guidelines for diagnostic accuracy studies assessing AI interventions: The STARD-AI Steering Group. Nat. Med. 2020, 26, 807–808. [Google Scholar] [CrossRef]
- Rivera, S.C.; Liu, X.; Chan, A.W.; Denniston, A.K.; Calvert, M.J. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The SPIRIT-AI extension. Nat. Med. 2020, 26, 1351–1363. [Google Scholar] [CrossRef]
- Liu, X.; Rivera, S.C.; Moher, D.; Calvert, M.J.; Denniston, A.K. Reporting guidelines for clinical trial reports for interventions involving artificial intelligence: The CONSORT-AI extension. Nat. Med. 2020, 26, 1364–1374. [Google Scholar] [CrossRef]
- Clinical-Trials.ai|Home n.d. Available online: https://www.clinical-trials.ai/ (accessed on 1 November 2021).
- Schwendicke, F.; Singh, T.; Lee, J.H.; Gaudin, R.; Chaurasia, A.; Wiegand, T.; Uribe, S.; Krois, J. Artificial intelligence in dental research: Checklist for authors, reviewers, readers. J. Dent. 2021, 107, 103610. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| CBCT scans of oral and maxillofacial area for humans | Panoramic and CT scans of oral and maxillofacial area Inhumans |
| Diagnostic tool based on semi-automatic and fully automatic algorithm | CBCT scans of oral and maxillofacial area in animals |
| Experts judge or manual technique | Tracing any oral and maxillofacial structure rather than the IAN/IAC |
| Tracing the IAN/IAC | Pilot, ex-vivo studies, conference paper/review |
| Retrospective clinical trials, cross-sectional, case-control study | Full text not accessible |
| Studies published in any language and with the full text is accessible | |
| No date restriction |
| Author, Study Location, and Year of Publication | Algorithm | Total Sample | Persons Executing and Interpreting Reference Tests | Software Used for Reference Test Method | Data Sets Used for Training, Validation and Test | Validation Technique | Sensitivity | Specificity | Accuracy | Agreement between Methods | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | Expertise | ||||||||||
| Orhan et al., Turkey, 2021. [37] | U-net-like (Diagnocat ©) | 85 | 1 | OMF radiologist | N/A | N/A | N/A | N/A | N/A | N/A | Kappa statistics = 0.762 |
| Liu et al., China, 2021. [38] | Two U-Net, One ResNet-34 | 229 | 2 | OMF radiologists with 10 years of experience | Manually modification using Multi-Planar Reformation (MPR) | 154, 30, 45 (train, valid, test) | Train, validation, and test split | 90.2% | 95.0% | 93.3% | Kendall’s coefficient = 0.901 |
| Bayrakdar et al., Turkey, 2021. [39] | U-net-like, (Diagnocat ©) | 75 | 1 | OMF radiologist with 8 years of experience | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Kwak et al., Korea, 2020. [40] | 2D SegNet, 2D U-Net, 3D U-Net | 102 | 3 | Two trained researchers, One OMF radiologist with 6 years of experience | INVIVO™(Anatomage, San Jose, CA, USA) | 6:2:2 (train:valid:test) | Train, validation, and test split | N/A | N/A | 96 % (2D SegNet), 84% (2D U-Net), 99% (3D U-Net) | N/A |
| Jaskari et al., Finland, 2020. [41] | Fully convolutional deep neural network | 637 | 2 | OMF radiologist with 34 years experience and resident in dental and maxillofacial radiologist with 10 years of experience | Planmeca Romexis® 4.6.2.R software | 457, 52, 128 (train, valid, test) | Train, validation, and test split | N/A | N/A | 90% | N/A |
| Abdolali et al., Iran, 2016. [42] | Statistical shape models | 120 | 2 | Radiologists with at least 10 years of experience | N/A | 84 (training set) | Leave-one-out cross-validation | N/A | N/A | N/A | N/A |
| Bahrampour et al., Iran, 2016 [43] | Automated algorithm | 40 | 2 | Maxillofacial radiologists | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, J.; Olszewski, R.; Dyszkiewicz-Konwińska, M. The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 560. https://doi.org/10.3390/ijerph19010560
Issa J, Olszewski R, Dyszkiewicz-Konwińska M. The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(1):560. https://doi.org/10.3390/ijerph19010560
Chicago/Turabian StyleIssa, Julien, Raphael Olszewski, and Marta Dyszkiewicz-Konwińska. 2022. "The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 1: 560. https://doi.org/10.3390/ijerph19010560