
Sociodemographic Factors Associated with Vaccine Hesitancy in Central Texas Immediately Prior to COVID-19 Vaccine Availability


Abstract
:1. Introduction
2. Materials and Methods
3. Results
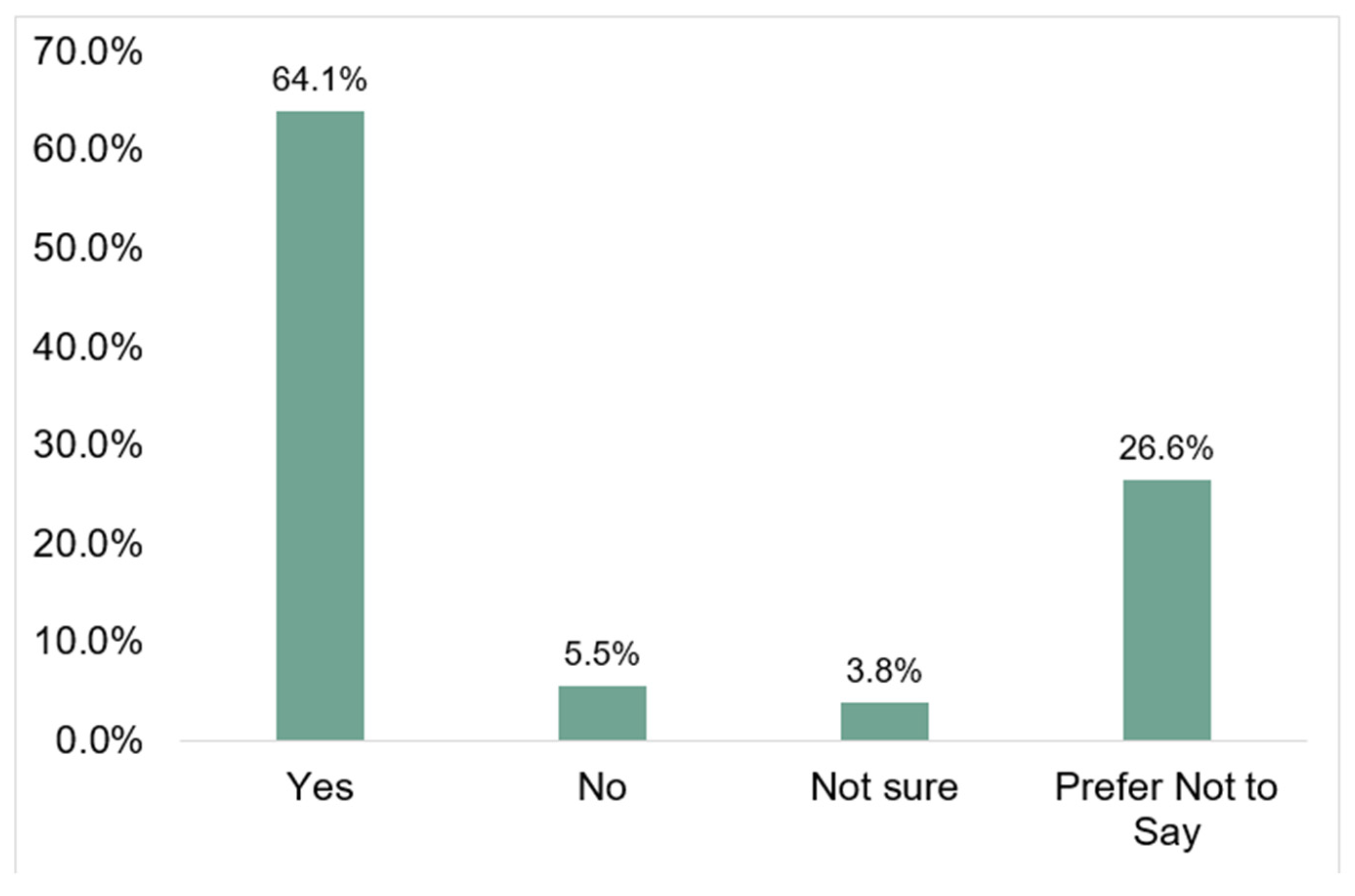
3.1. General Findings
3.2. Unadjusted Bivariate
3.3. Logistic Regression
4. Discussion
4.1. Recommendations
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. 2014. Available online: http://https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 4 November 2021).
- Freed, G.L.; Clark, S.J.; Butchart, A.T.; Singer, D.C.; Davis, M.M. Parental Vaccine Safety Concerns in 2009. Pediatrics 2010, 125, 654–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gust, D.A.; Strine, T.W.; Maurice, E.; Smith, P.; Yusuf, H.; Wilkinson, M.; Battaglia, M.; Wright, R.; Schwartz, B. Underimmunization among children: Effects of vaccine safety concerns on immunization status. Pediatrics 2004, 114, e16–e22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudino, J.A.; Robison, S. Risk factors associated with parents claiming personal-belief exemptions to school immunization requirements: Community and other influences on more skeptical parents in Oregon, 2006. Vaccine 2012, 30, 1132–1142. [Google Scholar] [CrossRef]
- Salmon, D.A.; Sotir, M.J.; Pan, W.K.; Berg, J.L.; Omer, S.B.; Stokley, S.; Hopfensperger, D.J.; Davis, J.P.; Halsey, N.A. Parental vaccine refusal in Wisconsin: A case-control study. WMJ 2009, 108, 17–23. [Google Scholar] [PubMed]
- Prislin, R.; Dyer, J.A.; Blakely, C.H.; Johnson, C.D. Immunization status and sociodemographic characteristics: The mediating role of beliefs, attitudes, and perceived control. Am. J. Public Health 1998, 88, 1821–1826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb Hooper, M.; Nápoles, A.M.; Pérez-Stable, E.J. No Populations Left Behind: Vaccine Hesitancy and Equitable Diffusion of Effective COVID-19 Vaccines. J. Gen. Intern. Med. 2021, 36, 2130–2133. [Google Scholar] [CrossRef]
- Barsade, J.; Exactor, F.C.; Mellon, G.C.C.; Dhanini, L.; Franz, B.; Gilovich, T.; Grant, A.; Lewis, N.; Young, D.S.; Rubicon, F.C.; et al. COVID-19 Vaccination Uptake Behavioral Science Task Force: Final Report. 2021. Available online: https://faculty.wharton.upenn.edu/wp-content/uploads/2018/01/Covid-19-Behavioral-Science-Task-Force-Report-Final-2021-02-23.pdf (accessed on 6 November 2021).
- Bauchner, H.; Malani, P.N.; Sharfstein, J. Reassuring the Public and Clinical Community about the Scientific Review and Approval of a COVID-19 Vaccine. JAMA 2020, 324, 1296–1297. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.L.; Borio, L. Finding effective treatments for COVID-19: Scientific integrity and public confidence in a time of cri-sis. JAMA 2020, 323, 1899–1900. [Google Scholar] [CrossRef] [PubMed]
- Dal-Ré, R.; Caplan, A.L.; Gluud, C.; Porcher, R. Ethical and scientific considerations regarding the early approval and deploy-ment of a COVID-19 vaccine. Ann. Intern. Med. 2021, 174, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Avorn, J.; Kesselheim, A. Regulatory Decision-making on COVID-19 Vaccines during a Public Health Emergency. JAMA 2020, 324, 1284–1285. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID Data Tracker. 2021. Available online: https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status (accessed on 25 November 2021).
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Quinn, S.; Jamison, A.; Musa, D.; Hilyard, K.; Freimuth, V. Exploring the Continuum of Vaccine Hesitancy between African American and White Adults: Results of a Qualitative Study. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Jamison, A.; Quinn, S.; Freimuth, V. “You don’t trust a government vaccine”: Narratives of institutional trust and influenza vaccination among African American and white adults. Soc. Sci. Med. 2019, 221, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of COVID-19 Vaccine Hesitancy Among Blacks. Clin. Infect. Dis. 2021, 73, 1784–1789. [Google Scholar] [CrossRef]
- Nowak, G.J.; Cacciatore, M.A.; Len-Ríos, M.E. Understanding and Increasing Influenza Vaccination Acceptance: Insights from a 2016 National Survey of U.S. Adults. Int. J. Environ. Res. Public Health 2018, 15, 711. [Google Scholar] [CrossRef] [Green Version]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Doherty, I.A.; Pilkington, W.; Brown, L.; Billings, V.; Hoffler, U.; Paulin, L.; Kimbro, K.S.; Baker, B.; Zhang, T.; Locklear, T.; et al. COVID-19 vaccine hesitancy in underserved communities of North Carolina. PLoS ONE 2021, 16, e0248542. [Google Scholar] [CrossRef]
- Ojha, R.P.; Stallings-Smith, S.; Flynn, P.M.; Adderson, E.E.; Offutt-Powell, T.N.; Gaur, A.H. The Impact of Vaccine Concerns on Racial/Ethnic Disparities in Influenza Vaccine Uptake among Health Care Workers. Am. J. Public Health 2015, 105, e35–e41. [Google Scholar] [CrossRef] [PubMed]
- Momplaisir, F.M.; Kuter, B.J.; Ghadimi, F.; Browne, S.; Nkwihoreze, H.; Feemster, K.A.; Frank, I.; Faig, W.; Shen, A.K.; Offit, P.A.; et al. Racial/Ethnic Differences in COVID-19 Vaccine Hesitancy Among Health Care Workers in 2 Large Academic Hospitals. JAMA Netw. Open 2021, 4, e2121931. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Bean-Mayberry, B.; Yano, E.M.; Mor, M.K.; Bayliss, N.K.; Xu, X.; Fine, M.J. Does sex influence immunization status for influenza and pneumonia in older veterans? Gender and immunizations in older veterans. J. Am. Geriatr. Soc. 2009, 57, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.-J.; Hung, M.-C.; Srivastav, A.; Grohskopf, L.A.; Kobayashi, M.; Harris, A.M.; Dooling, K.L.; Markowitz, L.E.; Rodriguez-Lainz, A.; Williams, W.W. Surveillance of Vaccination Coverage Among Adult Populations —United States, 2018. MMWR. Surveill. Summ. 2021, 70, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Workbook: COVID-19 Vaccine in Texas (Dashboard). Texas Department of State Health Service COVID-19 Vaccine Tracker. Data for 21 December 2021. Available online: http://Tabexternal.dshs.texas.gov (accessed on 22 December 2021).
- U.S. Census Bureau QuickFacts: Travis County, Texas. Census Bureau QuickFacts. Available online: https://www.census.gov/quickfacts/traviscountytexas (accessed on 20 December 2021).
- Litaker, J.R.; Tamez, N.; Durkalski, W.; Taylor, R. Using Health Insurance Network Provider Data and Public Data Sets to Identify SARS-CoV-2 Vaccinators in the USA. Front. Public Health 2021, 8, 616140. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics of the Respondent Population | n (%) |
|---|---|
| Sex (N = 1648) | |
| Female | 891 (54.1) |
| Male | 757 (45.9) |
| Age in Years (N = 1648) (Range: 20–86 years) | 1648 (100) |
| 18–24 years old | 24 (1.5) |
| 25–34 years old | 327 (19.8) |
| 35–44 years old | 381 (23.1) |
| 45–54 years old | 356 (21.6) |
| 55–64 years old | 501 (30.4) |
| ≥65 years old | 59 (3.6) |
| Race (N = 1648) (More than one race response could be selected) | |
| American Indian or Alaskan Native | 24 (1.5) * |
| Asian | 130 (7.9) * |
| Black or African American | 83 (5.0) * |
| Native Hawaiian or Other Pacific Islander | 6 (0.4) * |
| White | 1349 (81.9) * |
| Other | 112 (6.8) * |
| Ethnicity (N = 1648) | |
| No, not of Hispanic, Latino, or Spanish origin | 1324 (80.3) |
| Yes, Hispanic, Latino, or Spanish origin (More than one ethnicity could be selected) | 324 (19.7) |
| Mexican, Mexican American, Chicano | 245 (14.9) * |
| Puerto Rican | 11 (0.7) * |
| Cuban | 14 (0.8) * |
| Another Hispanic, Latino, or Spanish origin | 87 (5.3) * |
| Education (N = 1648) | |
| Less than some high school | 16 (1.0) |
| Some high school | 55 (3.3) |
| High School Diploma, GED, or equivalent | 162 (9.8) |
| Trade School | 47 (2.9) |
| Some College | 300 (18.2) |
| Associate Degree | 132 (8.0) |
| Bachelor’s Degree | 600 (36.4) |
| Graduate Degree | 329 (20.0) |
| Other | 7 (0.4) |
| Annual Household Income (N = 1648) | |
| Less than $10,000 per year | 159 (10.4) |
| $10,000–$29,999 | 461 (28.0) |
| $30,000–$39,999 | 216 (13.1) |
| $40,000–$49,999 | 154 (9.3) |
| $50,000–$75,999 | 242 (14.7) |
| $76,000–$99,999 | 104 (6.3) |
| $100,000 or above | 128 (7.8) |
| Prefer Not To Answer | 172 (10.4) |
| Variable | N | % | I Plan to Get the COVID-19 Vaccine When It Is Available? | Chi-Square (df) p-Value | |||
|---|---|---|---|---|---|---|---|
| Yes | No | Not Sure | Prefer Not to Say | ||||
| n (%) | n (%) | n (%) | n (%) | ||||
| Age Level (N = 1648) | 21.52 (6), p = 0.001 | ||||||
| 18–34 years of age | 351 | 21.3 | 226 (21.4) | 13 (14.3) | 13 (20.6) | 99 (22.6) | |
| 35–49 years of age | 559 | 33.9 | 332 (31.4) | 39 (42.9) | 34 (54.0) | 154 (35.2) | |
| 50+ year of age | 738 | 44.8 | 498 (47.2) | 39 (42.9) | 16 (25.4) | 185 (42.2) | |
| Education Level (N = 1641) | 30.35 (6), p < 0.001 | ||||||
| ≤High School Diploma † | 233 | 14.2 | 127 (12.0) | 21 (23.1) | 12 (19.4) | 73 (16.8) | |
| ≥HS Diploma ≤ Bachelor’s Degree ‡ | 347 | 21.1 | 198 (18.8) | 19 (20.9) | 18 (29.0) | 112 (25.8) | |
| ≥Bachelor’s Degree § | 1061 | 64.7 | 729 (69.2) | 51 (56.0) | 32 (51.6) | 249 (57.4) | |
| Race (N = 1648) | |||||||
| American Indian or Alaskan Native | 24 | 1.5 * | 13 (1.2) | 3 (3.3) | 1 (1.6) | 7 (1.6) | 2.59 (3), p = 0.459 |
| Asian | 130 | 7.9 * | 91 (8.6) | 4 (4.4) | 7 (11.1) | 28 (6.4)) | 4.55 (3), p = 0.208 |
| Black or African American | 83 | 5.0 * | 29 (2.7) | 13 (14.3) | 5 (7.9) | 36 (8.2) | 38.24 (3), p < 0.001 |
| Native Hawaiian or Other Pacific Islander | 6 | 0.4 * | 6 (.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3.38 (3), p = 0.337 |
| White | 1349 | 81.9 * | 896 (84.4) | 67 (73.6) | 44 (69.8) | 342 (78.1) | 20.84 (3), p < 0.001 |
| Other | 112 | 6.8 * | 62 (5.9) | 7 (7.7) | 9 (14.3) | 34 (7.8) | 7.77 (3), p = 0.051 |
| Annual Household Income (N = 1464) | 29.19 (18), p = 0.046 | ||||||
| <$10,000 | 159 | 10.9 | 90 (9.5) | 7 (9.0) | 9 (20.0) | 53 (13.6) | |
| $10,000–$29,999 | 461 | 31.5 | 287 (30.1) | 24 (30.8) | 17 (37.8) | 133 (34.2) | |
| $30,000–$39,999 | 216 | 14.8 | 135 (14.2) | 14 (17.9) | 7 (15.6) | 60 (15.4) | |
| $40,000–$49,999 | 154 | 10.5 | 100 (10.5) | 8 (10.3) | 4 (8.9) | 42 (10.8) | |
| $50,000–$75,999 | 242 | 16.5 | 163 (17.1) | 12 (15.4) | 7 (15.6) | 60 (15.4) | |
| $76,000–$99,999 | 104 | 7.1 | 78 (8.2) | 5 (6.4) | 1 (2.2) | 20 (5.1) | |
| $100,000 or more | 128 | 8.7 | 99 (10.4) | 8 (10.3) | 0 (0.0) | 21 (5.4) | |
| Sex (N = 1648) | 31.83 (3), p < 0.001 | ||||||
| Female | 891 | 54.1 | 517 (49.0) | 59 (64.8) | 43 (68.3) | 272 (62.1) | |
| Male | 757 | 45.9 | 539 (51.0) | 32 (35.2) | 20 (31.7) | 166 (37.9) | |
| Ethnicity (N = 1648) | 11.99 (3), p = 0.007 | ||||||
| Not of Hispanic, Latino, or Spanish origin | 1324 | 80.3 | 873 (82.7) | 71 (78.0) | 44 (69.8) | 336 (76.7) | |
| Hispanic, Latino, or Spanish origin | 324 | 19.7 * | 183 (17.3) | 20 (22.0) | 19 (30.2) | 102 (23.2) | |
| Mexican, Mexican American, Chicano | 245 | 14.9 * | 137 (13.0) | 14 (15.4) | 16 (25.4) | 78 (17.8) | 11.53 (3), p = 0.009 |
| Puerto Rican | 11 | 0.7 * | 5 (0.5) | 3 (3.3) | 0 (0.0) | 3 (0.7) | 10.51 (3), p = 0.015 |
| Cuban | 14 | 0.8 * | 9 (0.9) | 1 (1.1) | 0 (0.0) | 4 (0.9) | 0.628 (3), p = 0.890 |
| Other Hispanic, Latino, or Spanish origin | 87 | 5.3 * | 50 (4.7) | 3 (3.3) | 5 (7.9) | 29 (6.6) | 3.81 (3), p = 0.283 |
| Plans to Get the COVID-19 Vaccine When Available | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No, Not Sure, Prefer Not to Say | Unadjusted Prevalence Odds Ratio Yes vs. No, Not Sure, Prefer Not to Say | Adjusted Prevalence Odds Ratio Yes vs. No, Not Sure, Prefer Not to Say | |||||||
| Factor | n | % | n | % | POR | 95% CI | p-Value | POR | 95% CI | p-Value |
| Sex | 1056 | 100.0 | 592 | 100.0 | ||||||
| Male | 539 | 51.0 | 218 | 36.8 | 1.0 | 1.0 | ||||
| Female | 517 | 49.0 | 374 | 63.2 | 0.559 | 0.455, 0.687 | <0.001 | 0.650 | 0.518, 0.816 | <0.001 |
| Age (years) | 1056 | 100 | 592 | 100 | ||||||
| 50+ | 498 | 47.2 | 240 | 40.5 | 1.0 | 1.0 | ||||
| 35–49 | 332 | 31.4 | 227 | 38.3 | 0.705 | 0.561, 0.886 | 0.003 | 0.689 | 0.534, 0.890 | 0.004 |
| 18–34 | 226 | 21.4 | 125 | 21.1 | 0.871 | 0.667, 1.14 | 0.313 | 0.867 | 0.641, 1.171 | 0.352 |
| Hispanic, Latino, or Spanish Ethnicity | 1056 | 100.0 | 1324 | 100.0 | ||||||
| No | 873 | 82.7 | 451 | 76.2 | 1.0 | 1.0 | ||||
| Yes | 183 | 17.3 | 141 | 23.8 | 0.670 | 0.524, 0.859 | 0.001 | 0.826 | 0.622, 1.096 | 0.186 |
| Black or African American | 1056 | 100.0 | 592 | 100.0 | ||||||
| No | 1027 | 97.3 | 538 | 90.9 | 1.0 | 1.0 | ||||
| Yes | 29 | 2.7 | 54 | 9.1 | 0.281 | 0.177, 0.447 | <0.001 | 0.351 | 0.211, 0.584 | <0.001 |
| Education Level | 1054 | 100.0 | 587 | 100.0 | ||||||
| ≥4-year college | 658 | 62.4 | 271 | 46.2 | 1.0 | 1.0 | ||||
| >HS < 4-year college | 269 | 25.5 | 210 | 35.8 | 0.528 | 0.420, 0.664 | <0.001 | 0.572 | 0.442, 0.739 | <0.001 |
| ≤HS | 127 | 12.0 | 106 | 18.1 | 0.493 | 0.368, 0.662 | <0.001 | 0.565 | 0.401, 0.795 | 0.001 |
| Household Income | 952 | 100.0 | 512 | 100 | ||||||
| $100,000 or more | 99 | 10.4 | 29 | 5.7 | 1.0 | 1.0 | ||||
| $76,000–$99,999 | 78 | 8.2 | 26 | 5.1 | 0.879 | 0.479, 1.61 | 0.68 | 0.939 | 0.506, 1.741 | 0.841 |
| $50,000–$75,999 | 163 | 17.1 | 79 | 15.4 | 0.604 | 0.369, 0.99 | 0.044 | 0.687 | 0.415, 1.136 | 0.144 |
| $40,000–$49,999 | 100 | 10.5 | 54 | 10.5 | 0.543 | 0.319, 0.922 | 0.023 | 0.682 | 0.395, 1.178 | 0.170 |
| $30,000–$39,999 | 135 | 14.2 | 81 | 15.8 | 0.488 | 0.297, 0.803 | 0.004 | 0.623 | 0.373, 1.041 | 0.071 |
| $10,000–$29,999 | 287 | 30.1 | 174 | 34.0 | 0.483 | 0.301, 0.761 | 0.001 | 0.632 | 0.395, 1.011 | 0.056 |
| <$10,000 | 90 | 9.5 | 69 | 13.5 | 0.382 | 0.227, 0.642 | <0.001 | 0.565 | 0.327, 0.976 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Litaker, J.R.; Tamez, N.; Lopez Bray, C.; Durkalski, W.; Taylor, R. Sociodemographic Factors Associated with Vaccine Hesitancy in Central Texas Immediately Prior to COVID-19 Vaccine Availability. Int. J. Environ. Res. Public Health 2022, 19, 368. https://doi.org/10.3390/ijerph19010368
Litaker JR, Tamez N, Lopez Bray C, Durkalski W, Taylor R. Sociodemographic Factors Associated with Vaccine Hesitancy in Central Texas Immediately Prior to COVID-19 Vaccine Availability. International Journal of Environmental Research and Public Health. 2022; 19(1):368. https://doi.org/10.3390/ijerph19010368
Chicago/Turabian StyleLitaker, John R., Naomi Tamez, Carlos Lopez Bray, Wesley Durkalski, and Richard Taylor. 2022. "Sociodemographic Factors Associated with Vaccine Hesitancy in Central Texas Immediately Prior to COVID-19 Vaccine Availability" International Journal of Environmental Research and Public Health 19, no. 1: 368. https://doi.org/10.3390/ijerph19010368