
Shift Work Predicts Increases in Lipopolysaccharide-Binding Protein, Interleukin-10, and Leukocyte Counts in a Cross-Sectional Study of Healthy Volunteers Carrying Low-Grade Systemic Inflammation


Abstract
:1. Introduction
2. Materials and Methods
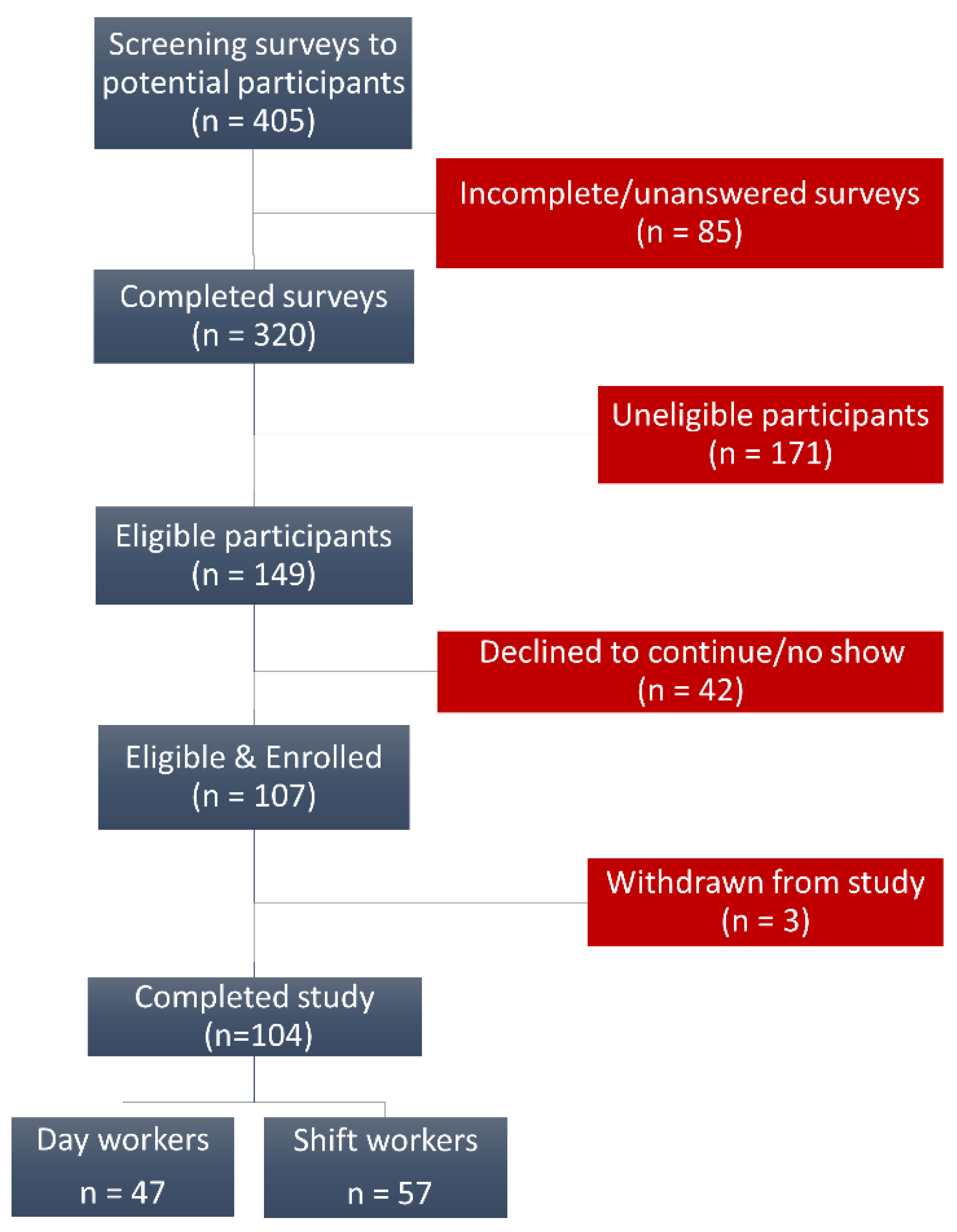
2.1. Study Cohort and Design
2.2. Exposure Criteria
2.3. Biological Samples, Risk Factors, and Biomarker Assessments
2.4. Data Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Assessment of Blood Pressure, Sleep Amount, and Plasma Cortisol
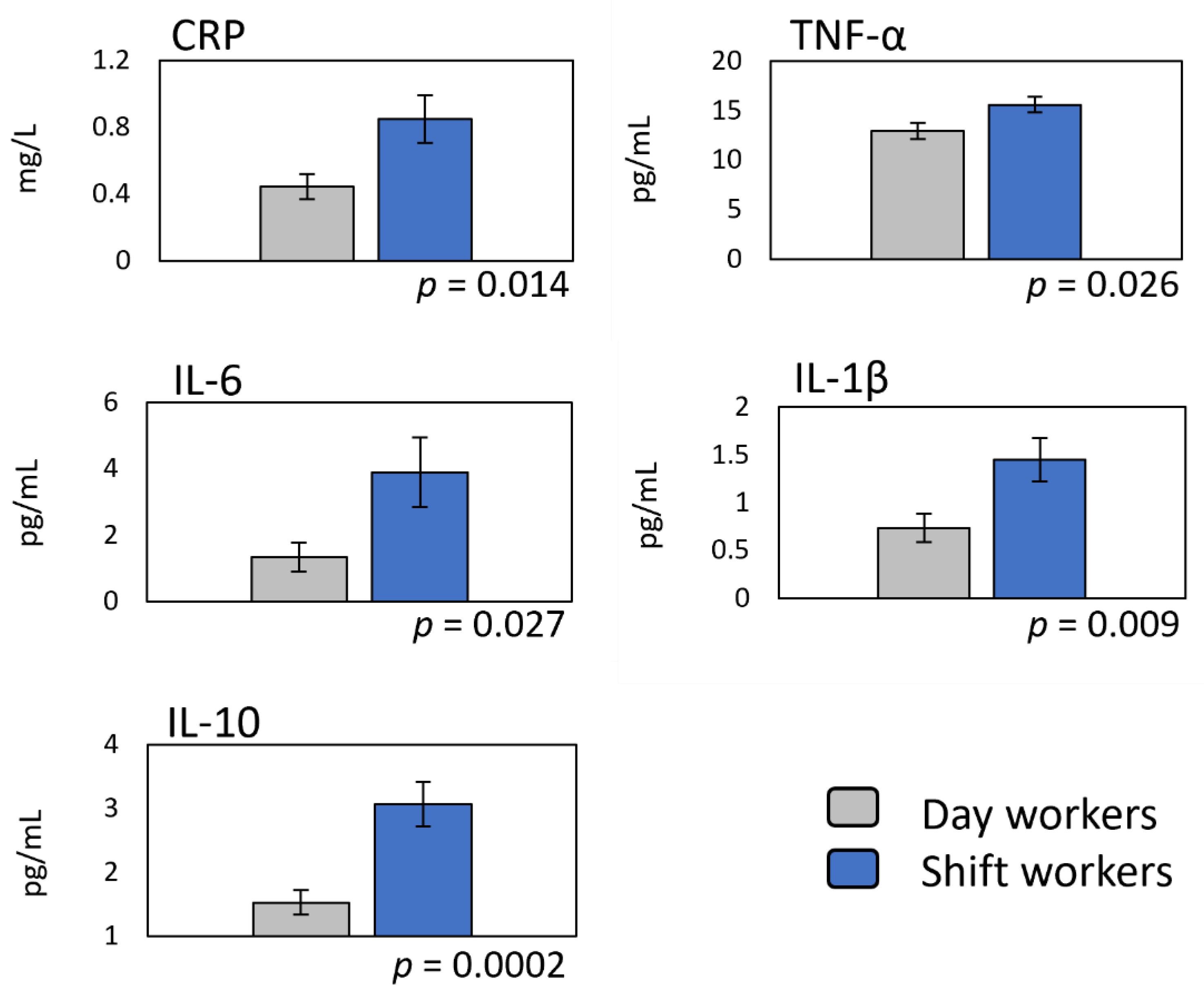
3.3. Markers of Systemic Inflammation in Shift Workers
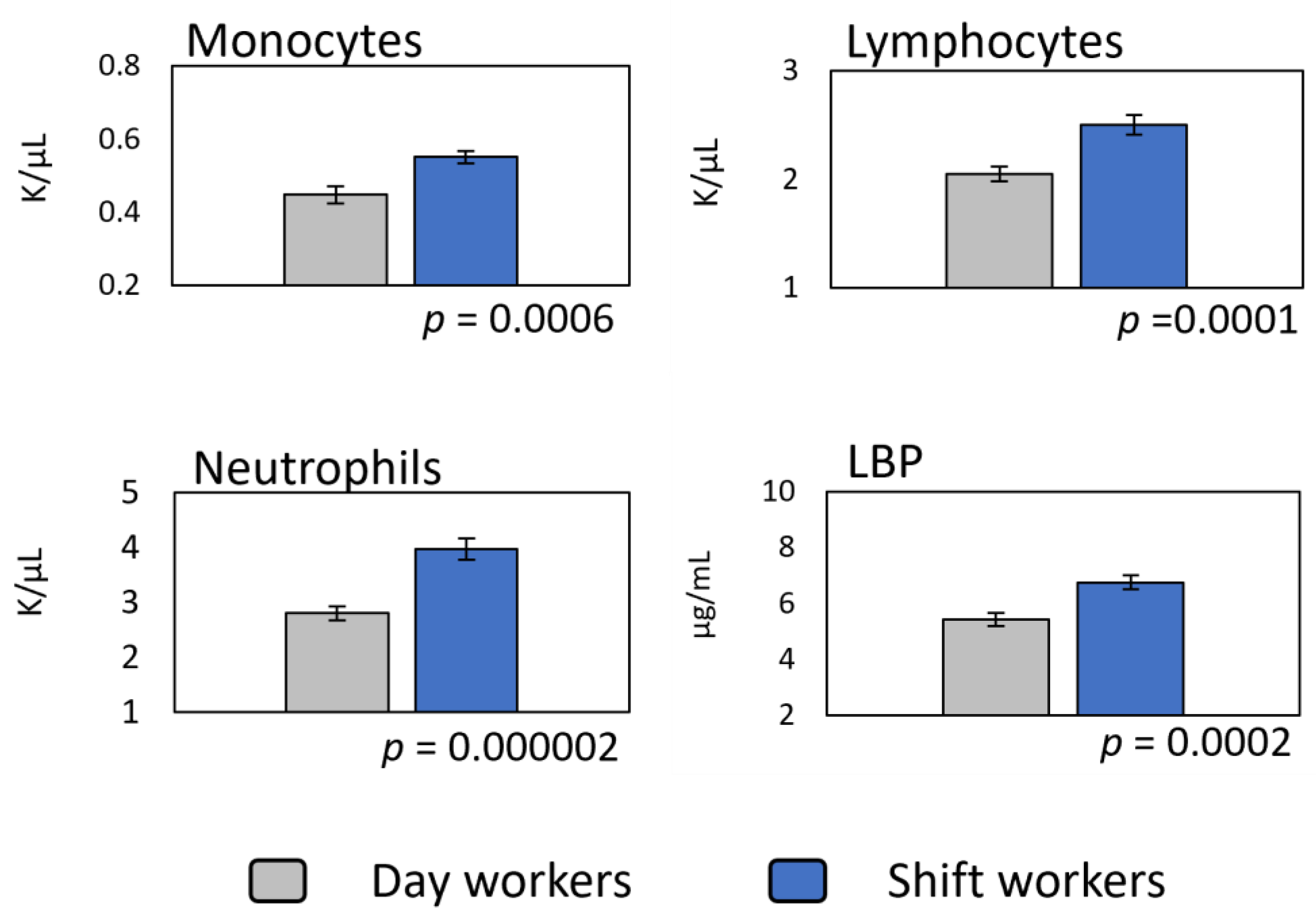
3.4. Relationship between Shift-Work Exposure, Leukocyte Counts, and Systemic Endotoxemia
4. Discussion
4.1. Low-Grade Systemic Inflammation in Shift Workers Is Promoted by Multiple Factors and Does Not Require a Lifetime of Exposure to Emerge
4.2. Systemic Endotoxemia as a Potential Mediator of Shift-Work-Related Effects
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hamermesh, D.; Stancanelli, E. Long Work Weeks and Strange Hours. ILR Rev. 2014, 68, 1007–1018. [Google Scholar] [CrossRef] [Green Version]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Fuchs, C.S.; Colditz, G.A. Night-shift work and risk of colorectal cancer in the nurses’ health study. J. Natl. Cancer Inst. 2003, 95, 825–828. [Google Scholar] [CrossRef] [Green Version]
- Schernhammer, E.S.; Kroenke, C.H.; Laden, F.; Hankinson, S.E. Night work and risk of breast cancer. Epidemiology 2006, 17, 108–111. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Tergas, A.I.; Mateen, F.J.; Bhayani, N.H.; Oh, J. Night-shift work and risk of breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2013, 138, 291–301. [Google Scholar] [CrossRef]
- Lahti, T.A.; Partonen, T.; Kyyrönen, P.; Kauppinen, T.; Pukkala, E. Night-time work predisposes to non-Hodgkin lymphoma. Int. J. Cancer 2008, 123, 2148–2151. [Google Scholar] [CrossRef]
- Conlon, M.; Lightfoot, N.; Kreiger, N. Rotating shift work and risk of prostate cancer. Epidemiology 2007, 18, 182–183. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Ozasa, K.; Mikami, K.; Wakai, K.; Fujino, Y.; Watanabe, Y.; Miki, T.; Nakao, M.; Hayashi, K.; Suzuki, K.; et al. Prospective cohort study of the risk of prostate cancer among rotating-shift workers: Findings from the Japan collaborative cohort study. Am. J. Epidemiol. 2006, 164, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Segawa, K.; Nakazawa, S.; Tsukamoto, Y.; Kurita, Y.; Goto, H.; Fukui, A.; Takano, K. Peptic ulcer is prevalent among shift workers. Dig. Dis. Sci. 1987, 32, 449–453. [Google Scholar] [CrossRef]
- Drake, C.L.; Roehrs, T.; Richardson, G.; Walsh, J.K.; Roth, T. Shift work sleep disorder: Prevalence and consequences beyond that of symptomatic day workers. Sleep 2004, 27, 1453–1462. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, B.; Knutsson, A.; Lindahl, B. Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27, 485 people. Occup. Environ. Med. 2001, 58, 747–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, B.; Alfredsson, L.; Knutsson, A.; Andersson, E.; Torén, K. Total mortality and cause-specific mortality of Swedish shift- and dayworkers in the pulp and paper industry in 1952–2001. Scand. J. Work Environ. Health 2005, 31, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Nakagawa, H.; Miura, K.; Soyama, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nogawa, K. Shift work and the risk of diabetes mellitus among Japanese male factory workers. Scand. J. Work Environ. Health 2005, 31, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Tenkanen, L.; Sjöblom, T.; Härmä, M. Joint effect of shift work and adverse life-style factors on the risk of coronary heart disease. Scand. J. Work Environ. Health 1998, 24, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haupt, C.M.; Alte, D.; Dörr, M.; Robinson, D.M.; Felix, S.B.; John, U.; Völzke, H. The relation of exposure to shift work with atherosclerosis and myocardial infarction in a general population. Atherosclerosis 2008, 201, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Tüchsen, F.; Hannerz, H.; Burr, H. A 12 year prospective study of circulatory disease among Danish shift workers. Occup. Environ. Med. 2006, 63, 451–455. [Google Scholar] [CrossRef] [Green Version]
- Magrini, A.; Pietroiusti, A.; Coppeta, L.; Babbucci, A.; Barnaba, E.; Papadia, C.; Iannaccone, U.; Boscolo, P.; Bergamaschi, E.; Bergamaschi, A. Shift work and autoimmune thyroid disorder. Int. J. Immunopathol. Pharmacol. 2006, 19 (Suppl. S4), 31–36. [Google Scholar]
- Hedström, A.K.; Åkerstedt, T.; Hillert, J.; Olsson, T.; Alfredsson, L. Shift work at young age is associated with increased risk for multiple sclerosis. Ann. Neurol. 2011, 70, 733–741. [Google Scholar] [CrossRef]
- Loef, B.; van Baarle, D.; van der Beek, A.J.; Sanders, E.A.M.; Bruijning-Verhagen, P.; Proper, K.I. Shift Work and Respiratory Infections in Health-Care Workers. Am. J. Epidemiol. 2019, 188, 509–517. [Google Scholar] [CrossRef]
- Mohren, D.C.; Jansen, N.W.; Kant, I.J.; Galama, J.; van den Brandt, P.A.; Swaen, G.M. Prevalence of common infections among employees in different work schedules. J. Occup. Environ. Med. 2002, 44, 1003–1011. [Google Scholar] [CrossRef] [Green Version]
- Vijayalaxmi, M.; George, A.; Nambiar, N. A Study of General Health Pattern among Night Shift Work Employees in a Tertiary Care. JAIR 2014, 3, 176–183. [Google Scholar]
- World Health Organization IARC. Night shift work. In IARC Monographs on the Identification of Carcinogenic Hazards to Humans; IARC: Lyon, France, 2020; Volume 124, pp. 1–371. [Google Scholar]
- Ryan, S.; Taylor, C.T.; McNicholas, W.T. Systemic inflammation: A key factor in the pathogenesis of cardiovascular complications in obstructive sleep apnea syndrome? Postgrad. Med. J. 2009, 85, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Bojarski, C. Malignant transformation in inflammatory bowel disease: Prevention, surveillance and treatment—New techniques in endoscopy. Dig. Dis. 2009, 27, 571–575. [Google Scholar] [CrossRef]
- Goldberg, R.B. Cytokine and cytokine-like inflammation markers, endothelial dysfunction, and imbalanced coagulation in development of diabetes and its complications. J. Clin. Endocrinol. Metab. 2009, 94, 3171–3182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loef, B.; Nanlohy, N.M.; Jacobi, R.H.J.; van de Ven, C.; Mariman, R.; van der Beek, A.J.; Proper, K.I.; van Baarle, D. Immunological effects of shift work in healthcare workers. Sci. Rep. 2019, 9, 18220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, L.F.; Wang, C.P.; Tsai, I.T.; Hung, W.C.; Yu, T.H.; Wu, C.C.; Hsu, C.C.; Lu, Y.C.; Chung, F.M.; Jean, M.C. Relationship between shift work and peripheral total and differential leukocyte counts in Chinese steel workers. J. Occup. Health 2016, 58, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Wirth, M.D.; Andrew, M.E.; Burchfiel, C.M.; Burch, J.B.; Fekedulegn, D.; Hartley, T.A.; Charles, L.E.; Violanti, J.M. Association of shift-work and immune cells among police officers from the Buffalo Cardio-Metabolic Occupational Police Stress study. Chronobiol. Int. 2017, 34, 721–731. [Google Scholar] [CrossRef]
- Morris, M.C.; Gilliam, E.A.; Li, L. Innate immune programing by endotoxin and its pathological consequences. Front. Immunol. 2015, 5, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cani, P.D.; Amar, J.; Iglesias, M.A.; Poggi, M.; Knauf, C.; Bastelica, D.; Neyrinck, A.M.; Fava, F.; Tuohy, K.M.; Chabo, C.; et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes 2007, 56, 1761–1772. [Google Scholar] [CrossRef] [Green Version]
- Triantafilou, M.; Triantafilou, K. Lipopolysaccharide recognition: CD14, TLRs and the LPS-activation cluster. Trends Immunol. 2002, 23, 301–304. [Google Scholar] [CrossRef]
- Cohen, J. The detection and interpretation of endotoxemia. Intensive Care Med. 2000, 26 (Suppl. S1), S51–S56. [Google Scholar] [CrossRef]
- Novitsky, T.J. Limitations of the Limulus amebocyte lysate test in demonstrating circulating lipopolysaccharides. Ann. N. Y. Acad. Sci. 1998, 851, 416–421. [Google Scholar] [CrossRef]
- Gonzalez-Quintela, A.; Alonso, M.; Campos, J.; Vizcaino, L.; Loidi, L.; Gude, F. Determinants of serum concentrations of lipopolysaccharide-binding protein (LBP) in the adult population: The role of obesity. PLoS ONE 2013, 8, e54600. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef]
- Kapellos, T.S.; Bonaguro, L.; Gemünd, I.; Reusch, N.; Saglam, A.; Hinkley, E.R.; Schultze, J.L. Human Monocyte Subsets and Phenotypes in Major Chronic Inflammatory Diseases. Front. Immunol. 2019, 10, 2035. [Google Scholar] [CrossRef] [Green Version]
- Castanon-Cervantes, O.; Wu, M.; Ehlen, J.C.; Paul, K.; Gamble, K.L.; Johnson, R.L.; Besing, R.C.; Menaker, M.; Gewirtz, A.T.; Davidson, A.J. Dysregulation of inflammatory responses by chronic circadian disruption. J. Immunol. 2010, 185, 5796–5805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, K.L.; Castanon-Cervantes, O.; Evans, J.A.; Davidson, A.J. Environmental circadian disruption elevates the IL-6 response to lipopolysaccharide in blood. J. Biol. Rhythms 2013, 28, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Brager, A.J.; Ehlen, J.C.; Castanon-Cervantes, O.; Natarajan, D.; Delisser, P.; Davidson, A.J.; Paul, K.N. Sleep loss and the inflammatory response in mice under chronic environmental circadian disruption. PLoS ONE 2013, 8, e63752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). State-specific prevalence of obesity among adults—United States, 2007. MMWR Morb. Mortal. Wkly. Rep. 2008, 57, 765–768. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Differences in prevalence of obesity among black, white, and Hispanic adults—United States, 2006–2008. MMWR Morb. Mortal. Wkly. Rep. 2009, 58, 740–744. [Google Scholar]
- Yamasaki, F.; Schwartz, J.E.; Gerber, L.M.; Warren, K.; Pickering, T.G. Impact of shift work and race/ethnicity on the diurnal rhythm of blood pressure and catecholamines. Hypertension 1998, 32, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Vimalananda, V.G.; Palmer, J.R.; Gerlovin, H.; Wise, L.A.; Rosenzweig, J.L.; Rosenberg, L.; Ruiz Narváez, E.A. Night-shift work and incident diabetes among African-American women. Diabetologia 2015, 58, 699–706. [Google Scholar] [CrossRef] [Green Version]
- Pan, A.; Schernhammer, E.S.; Sun, Q.; Hu, F.B. Rotating night shift work and risk of type 2 diabetes: Two prospective cohort studies in women. PLoS Med. 2011, 8, e1001141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieu, S.J.; Curhan, G.C.; Schernhammer, E.S.; Forman, J.P. Rotating night shift work and disparate hypertension risk in African Americans. J. Hypertens. 2012, 30, 61–66. [Google Scholar] [CrossRef]
- Sponholtz, T.R.; Bethea, T.N.; Ruiz-Narváez, E.A.; Boynton-Jarrett, R.; Palmer, J.R.; Rosenberg, L.; Wise, L.A. Night Shift Work and Fecundability in Late Reproductive-Aged African American Women. J. Womens Health 2021, 30, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Zahodne, L.B.; Kraal, A.Z.; Zaheed, A.; Farris, P.; Sol, K. Longitudinal effects of race, ethnicity, and psychosocial disadvantage on systemic inflammation. SSM Popul. Health 2019, 7, 100391. [Google Scholar] [CrossRef] [PubMed]
- Stepanikova, I.; Bateman, L.B.; Oates, G.R. Systemic Inflammation in Midlife: Race, Socioeconomic Status, and Perceived Discrimination. Am. J. Prev. Med. 2017, 52 (Suppl. S1), S63–S76. [Google Scholar] [CrossRef] [Green Version]
- Stepanikova, I.; Oates, G.R.; Bateman, L.B. Does one size fit all? The role of body mass index and waist circumference in systemic inflammation in midlife by race and gender. Ethn. Health 2017, 22, 169–183. [Google Scholar] [CrossRef] [Green Version]
- Özdemir, B.C.; Dotto, G.P. Racial Differences in Cancer Susceptibility and Survival: More Than the Color of the Skin? Trends Cancer 2017, 3, 181–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, C.J.; Purvis, T.E.; Mistretta, J.; Hu, K.; Scheer, F.A.J.L. Circadian Misalignment Increases C-Reactive Protein and Blood Pressure in Chronic Shift Workers. J. Biol. Rhythms 2017, 32, 154–164. [Google Scholar] [CrossRef] [Green Version]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Meier-Ewert, H.K.; Ridker, P.M.; Rifai, N.; Regan, M.M.; Price, N.J.; Dinges, D.F.; Mullington, J.M. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J. Am. Coll. Cardiol. 2004, 43, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Hannibal, K.E.; Bishop, M.D. Chronic stress, cortisol dysfunction, and pain: A psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Janicki-Deverts, D.; Doyle, W.J.; Miller, G.E.; Frank, E.; Rabin, B.S.; Turner, R.B. Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proc. Natl. Acad. Sci. USA 2012, 109, 5995–5999. [Google Scholar] [CrossRef] [Green Version]
- Sesso, H.D.; Buring, J.E.; Rifai, N.; Blake, G.J.; Gaziano, J.M.; Ridker, P.M. C-Reactive Protein and the Risk of Developing Hypertension. JAMA 2003, 290, 2945–2951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faraut, B.; Boudjeltia, K.Z.; Vanhamme, L.; Kerkhofs, M. Immune, inflammatory and cardiovascular consequences of sleep restriction and recovery. Sleep Med. Rev. 2012, 16, 137–149. [Google Scholar] [CrossRef]
- Puttonen, S.; Viitasalo, K.; Härmä, M. Effect of shift-work on systemic markers of inflammation. Chronobiol. Int. 2011, 28, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Khosro, S.; Alireza, S.; Omid, A.; Forough, S. Night work and inflammatory markers. Indian J. Occup. Environ. Med. 2011, 15, 38–41. [Google Scholar] [CrossRef]
- Kim, S.W.; Jang, E.C.; Kwon, S.C.; Han, W.; Kang, M.S.; Nam, Y.H.; Lee, Y.J. Night shift work and inflammatory markers in male workers aged 20–39 in a display manufacturing company. Ann. Occup. Environ. Med. 2016, 28, 48. [Google Scholar] [CrossRef] [Green Version]
- Saraiva, M.; O’Garra, A. The regulation of IL-10 production by immune cells. Nat. Rev. Immunol. 2010, 10, 170–181. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, W.; Rutz, S.; Crellin, N.K.; Valdez, P.A.; Hymowitz, S.G. Regulation and functions of the IL-10 family of cytokines in inflammation and disease. Annu. Rev. Immunol. 2011, 29, 71–109. [Google Scholar] [CrossRef]
- Krueger, J.M.; Obál, F.J.; Fang, J.; Kubota, T.; Taishi, P. The role of cytokines in physiological sleep regulation. Ann. N. Y. Acad. Sci. 2001, 933, 211–221. [Google Scholar] [CrossRef]
- van der Poll, T.; Marchant, A.; van Deventer, S.J. The role of interleukin-10 in the pathogenesis of bacterial infection. Clin. Microbiol. Infect. 1997, 3, 605–607. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Fischer, C.P. Physiological roles of muscle-derived interleukin-6 in response to exercise. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 265–271. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Zoumakis, M.; Bixler, E.O.; Lin, H.M.; Prolo, P.; Vela-Bueno, A.; Kales, A.; Chrousos, G.P. Impaired nighttime sleep in healthy old versus young adults is associated with elevated plasma interleukin-6 and cortisol levels: Physiologic and therapeutic implications. J. Clin. Endocrinol. Metab. 2003, 88, 2087–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelsch, S.; Boehlig, A.; Hohenadel, M.; Nitsche, I.; Bauer, K.; Sack, U. The impact of acute stress on hormones and cytokines, and how their recovery is affected by music-evoked positive mood. Sci. Rep. 2016, 6, 23008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrovsky, N.; McNair, P.; Harrison, L.C. Diurnal rhythms of pro-inflammatory cytokines: Regulation by plasma cortisol and therapeutic implications. Cytokine 1998, 10, 307–312. [Google Scholar] [CrossRef]
- Gamble, K.L.; Berry, R.; Frank, S.J.; Young, M.E. Circadian clock control of endocrine factors. Nat. Rev. Endocrinol. 2014, 10, 466–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.R.; Matthews, J.P.; Kanabrocki, E.L.; Sothern, R.B.; Roitman-Johnson, B.; Scheving, L.E. Circadian rhythmometry of serum interleukin-2, interleukin-10, tumor necrosis factor-alpha, and granulocyte-macrophage colony-stimulating factor in men. Chronobiol. Int. 1995, 12, 19–27. [Google Scholar] [CrossRef]
- Lundkvist, G.B.; Robertson, B.; Mhlanga, J.D.; Rottenberg, M.E.; Kristensson, K. Expression of an oscillating interferon-gamma receptor in the suprachiasmatic nuclei. Neuroreport 1998, 9, 1059–1063. [Google Scholar] [CrossRef]
- Takane, H.; Ohdo, S.; Baba, R.; Koyanagi, S.; Yukawa, E.; Higuchi, S. Relationship between 24-hour rhythm in antiviral effect of interferon-beta and interferon-alpha/beta receptor expression in mice. Jpn. J. Pharmacol. 2002, 90, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Rahman, S.A.; Castanon-Cervantes, O.; Scheer, F.A.; Shea, S.A.; Czeisler, C.A.; Davidson, A.J.; Lockley, S.W. Endogenous circadian regulation of pro-inflammatory cytokines and chemokines in the presence of bacterial lipopolysaccharide in humans. Brain Behav. Immun. 2015, 47, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Reinhardt, É.L.; Fernandes, P.A.; Markus, R.P.; Fischer, F.M. Daily rhythm of salivary IL-1ß, cortisol and melatonin in day and night workers. Work 2012, 41 (Suppl. S1), 5788–5790. [Google Scholar] [CrossRef] [Green Version]
- Kervezee, L.; Cuesta, M.; Cermakian, N.; Boivin, D.B. Simulated night shift work induces circadian misalignment of the human peripheral blood mononuclear cell transcriptome. Proc. Natl. Acad. Sci. USA 2018, 115, 5540–5545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loef, B.; Baarle, D.V.; van der Beek, A.J.; Beekhof, P.K.; van Kerkhof, L.W.; Proper, K.I. The association between exposure to different aspects of shift work and metabolic risk factors in health care workers, and the role of chronotype. PLoS ONE 2019, 14, e0211557. [Google Scholar] [CrossRef] [Green Version]
- Cuesta, M.; Boudreau, P.; Dubeau-Laramée, G.; Cermakian, N.; Boivin, D.B. Simulated Night Shift Disrupts Circadian Rhythms of Immune Functions in Humans. J. Immunol. 2016, 196, 2466–2475. [Google Scholar] [CrossRef] [Green Version]
- Almeida, C.M.; Malheiro, A. Sleep, immunity and shift workers: A review. Sleep Sci. 2016, 9, 164–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labrecque, N.; Cermakian, N. Circadian Clocks in the Immune System. J. Biol. Rhythms 2015, 30, 277–290. [Google Scholar] [CrossRef]
- Man, K.; Loudon, A.; Chawla, A. Immunity around the clock. Science 2016, 354, 999–1003. [Google Scholar] [CrossRef] [Green Version]
- Sookoian, S.; Gemma, C.; Fernández Gianotti, T.; Burgueño, A.; Alvarez, A.; González, C.D.; Pirola, C.J. Effects of rotating shift work on biomarkers of metabolic syndrome and inflammation. J. Intern. Med. 2007, 261, 285–292. [Google Scholar] [CrossRef]
- Vaure, C.; Liu, Y.A. Comparative review of toll-like receptor 4 expression and functionality in different animal species. Front. Immunol. 2014, 5, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komai-Koma, M.; Gilchrist, D.S.; Xu, D. Direct recognition of LPS by human but not murine CD8+ T cells via TLR4 complex. Eur. J. Immunol. 2009, 39, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Troelstra, A.; Giepmans, B.N.; van Kessel, K.P.; Lichenstein, H.S.; Verhoef, J.; van Strijp, J.A. Dual effects of soluble CD14 on LPS priming of neutrophils. J. Leukoc. Biol. 1997, 61, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, R.; Geng, S.; Chen, K.; Diao, N.; Chu, H.W.; Li, L. Low-grade inflammatory polarization of monocytes impairs wound healing. J. Pathol. 2016, 238, 571–583. [Google Scholar] [CrossRef] [Green Version]
- Creely, S.J.; McTernan, P.G.; Kusminski, C.M.; Fisher, F.M.; Da Silva, N.F.; Khanolkar, M.; Evans, M.; Harte, A.L.; Kumar, S. Lipopolysaccharide activates an innate immune system response in human adipose tissue in obesity and type 2 diabetes. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E740–E747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, S.; Chen, K.; Yuan, R.; Peng, L.; Maitra, U.; Diao, N.; Chen, C.; Zhang, Y.; Hu, Y.; Qi, C.F.; et al. The persistence of low-grade inflammatory monocytes contributes to aggravated atherosclerosis. Nat. Commun. 2016, 7, 13436. [Google Scholar] [CrossRef]
- de Punder, K.; Pruimboom, L. Stress induces endotoxemia and low-grade inflammation by increasing barrier permeability. Front. Immunol. 2015, 6, 223. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.; Li, L. Molecular mechanisms and pathological consequences of endotoxin tolerance and priming. Arch. Immunol. Ther. Exp. 2012, 60, 13–18. [Google Scholar] [CrossRef]
- Wutzler, S.; Maier, M.; Lehnert, M.; Henrich, D.; Walcher, F.; Maegele, M.; Laurer, H.; Marzi, I. Suppression and recovery of LPS-stimulated monocyte activity after trauma is correlated with increasing injury severity: A prospective clinical study. J. Trauma 2009, 66, 1273–1280. [Google Scholar] [CrossRef]
- Fei, F.; Lee, K.M.; McCarry, B.E.; Bowdish, D.M. Age-associated metabolic dysregulation in bone marrow-derived macrophages stimulated with lipopolysaccharide. Sci. Rep. 2016, 6, 22637. [Google Scholar] [CrossRef] [PubMed]
- Huggard, D.; McGrane, F.; Lagan, N.; Roche, E.; Balfe, J.; Leahy, T.R.; Franklin, O.; Moreno, A.; Melo, A.M.; Doherty, D.G.; et al. Altered endotoxin responsiveness in healthy children with Down syndrome. BMC Immunol. 2018, 19, 31. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Day Workers n = 47 | Shift Workers n = 57 | |
|---|---|---|
| Asian (%) | 6.4 | 7 |
| Black (%) | 57.4 | 35 |
| Hispanic (%) | 2.1 | 3.5 |
| Mixed (%) | 2.1 | 3.5 |
| White (%) | 32 | 51 |
| Gender (% females) | 82 | 89 |
| Occupation (% healthcare) | 77 | 84 |
| BMI (kg/m2) | 25 ± 0.38 | 24.03 ± 0.37 |
| * Age (years) | 35.32 ± 1.24 | 28.26 ± 0.62 |
| * Shift duration (h) | 9.36 ± 0.27 | 11.78 ± 0.12 |
| * Shift-work exposure (years) | 0 | 3.97 ± 0.51 |
| Day Workers n = 47 | Shift Workers n = 57 | |
|---|---|---|
| Systolic blood pressure (mm Hg) | 120.73 ± 1.79 | 121.64 ± 1.36 |
| Diastolic blood pressure (mm Hg) | 76.21 ± 1.10 | 78.21 ± 1.09 |
| * Total sleep time (min per day) | 395.9 ± 13.90 | 326.85 ± 8.94 |
| * Plasma cortisol (ng/mL) | 131.55 ± 10.93 | 183.07 ± 14.56 |
| Outcome Variables | Regression Coefficient | 95% (CI) | p | Overall Model Fit |
|---|---|---|---|---|
| CRP (mg/L) | 0.415 | −0.145–0.844 | 0.058 | F (5, 98) = 1.46, R2 = 0.06, p = 0.22 |
| TNF-α (pg/mL) | 3.081 | 0.165–6.001 | 2.096 | F (5, 98) = 1.78, R2 = 0.07, p = 0.14 |
| IL-1β (pg/mL) | 0.816 | 0.104–1.528 | 0.025 | F (5, 98) = 1.80, R2 = 0.07, p = 0.13 |
| IL-6 (pg/mL) | 2.542 | −0.379–5.463 | 0.087 | F (5, 98) = 3.66, R2 = 0.13, p = 0.008 |
| * IL-10 (pg/mL) | 1.674 | 0.617–2.732 | 0.002 | F (5, 98) = 3.56, R2 = 0.12, p = 0.009 |
| * Monocytes (K/μL) | 0.117 | 0.047–0.186 | 0.001 | F (5, 98) = 4.19, R2 = 0.15, p = 0.003 |
| * Lymphocytes (K/μL) | 0.328 | 0.038–0.618 | 0.027 | F (5, 98) = 4.93, R2 = 0.17, p = 0.001 |
| * Neutrophils (K/μL) | 1.121 | 0.511–1.731 | 0.000 | F (5, 98) = 5.65, R2 = 0.18, p = 0.0004 |
| * LBP (μg/mL) | 1.312 | 0.422–2.202 | 0.000 | F (5, 98) = 5.43, R2 = 0.18, p = 0.0005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atwater, A.Q.; Immergluck, L.C.; Davidson, A.J.; Castanon-Cervantes, O. Shift Work Predicts Increases in Lipopolysaccharide-Binding Protein, Interleukin-10, and Leukocyte Counts in a Cross-Sectional Study of Healthy Volunteers Carrying Low-Grade Systemic Inflammation. Int. J. Environ. Res. Public Health 2021, 18, 13158. https://doi.org/10.3390/ijerph182413158
Atwater AQ, Immergluck LC, Davidson AJ, Castanon-Cervantes O. Shift Work Predicts Increases in Lipopolysaccharide-Binding Protein, Interleukin-10, and Leukocyte Counts in a Cross-Sectional Study of Healthy Volunteers Carrying Low-Grade Systemic Inflammation. International Journal of Environmental Research and Public Health. 2021; 18(24):13158. https://doi.org/10.3390/ijerph182413158
Chicago/Turabian StyleAtwater, Aisha Q., Lilly Cheng Immergluck, Alec J. Davidson, and Oscar Castanon-Cervantes. 2021. "Shift Work Predicts Increases in Lipopolysaccharide-Binding Protein, Interleukin-10, and Leukocyte Counts in a Cross-Sectional Study of Healthy Volunteers Carrying Low-Grade Systemic Inflammation" International Journal of Environmental Research and Public Health 18, no. 24: 13158. https://doi.org/10.3390/ijerph182413158