
Tonsillectomy in Adults over 40 Years of Age Does Not Increase the Risk of Pneumonia: A Three-Year Longitudinal Follow-Up Study


Abstract
:1. Introduction
2. Materials and Methods
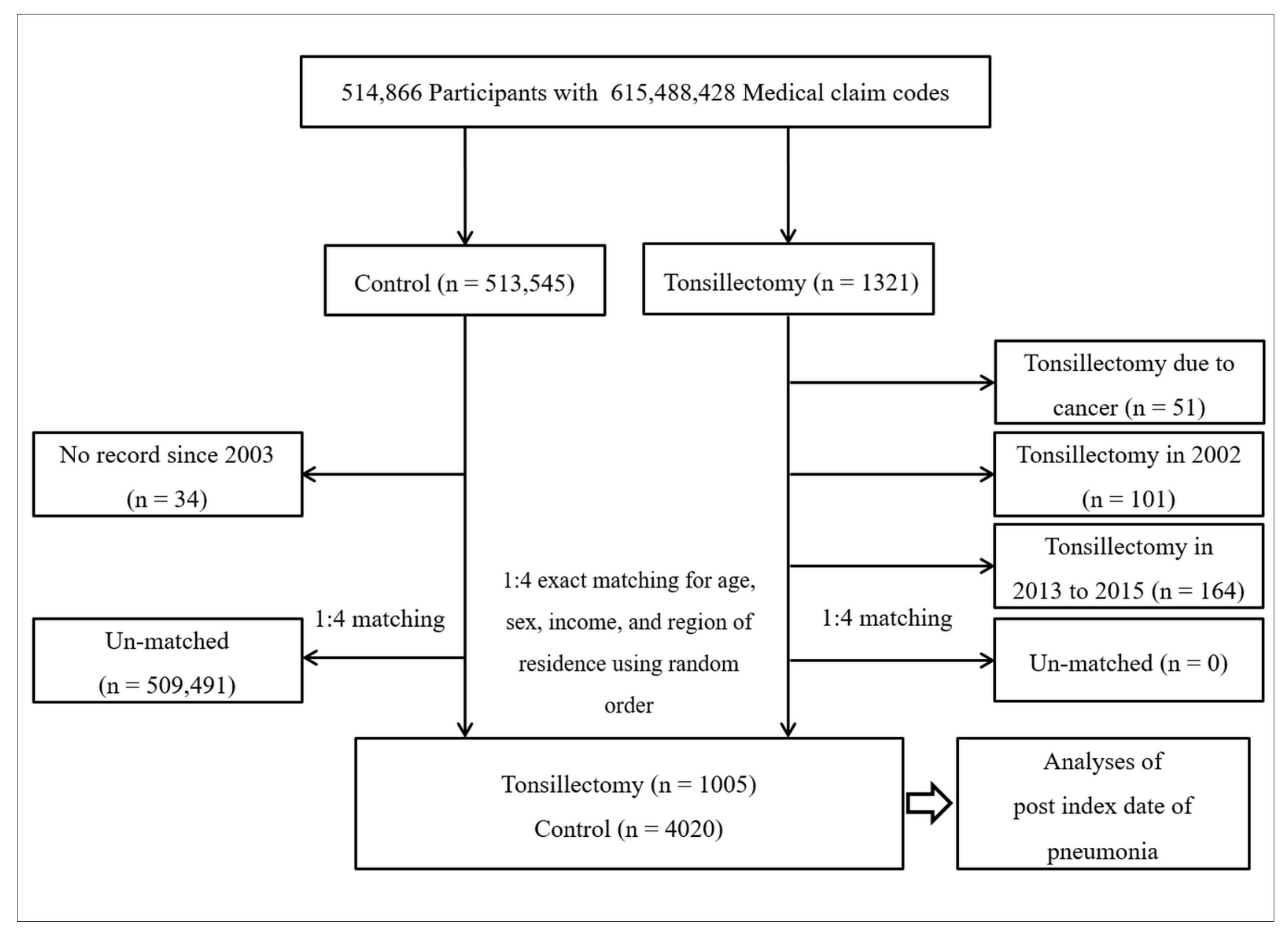
2.1. Study Population
2.2. Participant Selection
2.3. Tonsillectomy (Independent Variable)
2.4. Pneumonia (Dependent Variable)
2.5. Covariates
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paradise, J.L.; Bluestone, C.D.; Colborn, D.K.; Bernard, B.S.; Rockette, H.E.; Kurs-Lasky, M. Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children. Pediatrics 2002, 110, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.M.; Roman, S.A.; Sosa, J.A.; Judson, B.L. Safety of adult tonsillectomy: A population-level analysis of 5968 patients. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 197–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, J.L.; Jekel, J.F.; Freeman, D.H., Jr. Changes in age and sex specific tonsillectomy rates: United States, 1970–1977. Am. J. Public Health 1982, 72, 488–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boss, E.F.; Marsteller, J.A.; Simon, A.E. Outpatient tonsillectomy in children: Demographic and geographic variation in the United States, 2006. J. Pediatr. 2012, 160, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Min, C.; Lee, W.H.; Choi, H.G. Tonsillectomy increases the risk of retropharyngeal and parapharyngeal abscesses in adults, but not in children: A national cohort study. PLoS ONE. 2018, 13, e0193913. [Google Scholar] [CrossRef]
- Choi, H.G.; Hah, J.H.; Jung, Y.H.; Kim, D.W.; Sung, M.W. Influences of demographic changes and medical insurance status on tonsillectomy and adenoidectomy rates in Korea. Eur. Arch. Otorhinolaryngol. 2014, 271, 2293–2298. [Google Scholar] [CrossRef] [PubMed]
- Elinder, K.; Söderman, A.C.; Stalfors, J.; Knutsson, J. Factors influencing morbidity after paediatric tonsillectomy: A study of 18,712 patients in the National Tonsil Surgery Register in Sweden. Eur. Arch. Otorhinolaryngol. 2016, 273, 2249–2256. [Google Scholar] [CrossRef] [PubMed]
- Lundström, F.; Stalfors, J.; Østvoll, E.; Sunnergren, O. Practice, complications and outcome in Swedish tonsil surgery 2009–2018. An observational longitudinal national cohort study. Acta Otolaryngol. 2020, 140, 589–596. [Google Scholar] [CrossRef]
- Jeong, J.; Choi, J.K.; Choi, H.S.; Hong, C.E.; Shin, H.A.; Chang, J.H. The Associations of Tonsillectomy with Adenoidectomy with Pneumonia and Appendicitis Based on National Sample Cohort Data from the Korean National Health Insurance Service. Int. Arch. Otorhinolaryngol. 2021, 25, e545–e550. [Google Scholar] [CrossRef] [PubMed]
- Brandtzaeg, P. Potential of nasopharynx-associated lymphoid tissue for vaccine responses in the airways. Am. J. Respir. Crit. Care Med. 2011, 183, 1595–1604. [Google Scholar] [CrossRef]
- Bernstein, J.M. Mucosal immunology of the upper respiratory tract. Respiration 1992, 59, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Tian, C.; Hromatka, B.S.; Kiefer, A.K.; Eriksson, N.; Noble, S.M.; Tung, J.Y.; Hinds, D.A. Genome-wide association and HLA region fine-mapping studies identify susceptibility loci for multiple common infections. Nat. Commun. 2017, 8, 599. [Google Scholar] [CrossRef] [Green Version]
- Byars, S.G.; Stearns, S.C.; Boomsma, J.J. Association of Long-Term Risk of Respiratory, Allergic, and Infectious Diseases with Removal of Adenoids and Tonsils in Childhood. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 594–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altwairqi, R.G.; Aljuaid, S.M.; Alqahtani, A.S. Effect of tonsillectomy on humeral and cellular immunity: A systematic review of published studies from 2009 to 2019. Eur. Arch. Otorhinolaryngol. 2020, 277, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Park, B.; Sim, S.; Ahn, S.H. Tonsillectomy Does Not Reduce Upper Respiratory Infections: A National Cohort Study. PLoS ONE 2016, 11, e0169264. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Oh, D.J.; Choi, H.G. Tonsillectomy does not reduce asthma in children: A longitudinal follow-up study using a national sample cohort. Sci. Rep. 2019, 9, 13382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional Association between GERD and Asthma: Two Longitudinal Follow-Up Studies Using a National Sample Cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e9. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Wee, J.H.; Choi, H.G.; Park, J.Y.; Hwang, Y.I.; Jang, S.H.; Jung, K.S. Association between statin medication and asthma/asthma exacerbation in a national health screening cohort. J. Allergy Clin. Immunol. Pract. 2021, 9, 2783–2791. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, C.H.; Yoo, D.M.; Min, C.Y.; Choi, H.G. Association between Chronic Obstructive Pulmonary Disease and Meniere’s Disease: A Nested Case-Control Study Using a National Health Screening Cohort. Int. J. Environ. Res. Public Health 2021, 18, 4536. [Google Scholar] [CrossRef]
- D’Amelio, R.; Palmisano, L.; Le Moli, S.; Seminara, R.; Aiuti, F. Serum and salivary IgA levels in normal subjects: Comparison between tonsillectomized and non-tonsillectomized subjects. Int. Arch. Allergy Appl. Immunol. 1982, 68, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Van den Akker, E.H.; Sanders, E.A.; van Staaij, B.K.; Rijkers, G.T.; Rovers, M.M.; Hoes, A.W.; Schilder, A.G.M. Long-term effects of pediatric adenotonsillectomy on serum immunoglobulin levels: Results of a randomized controlled trial. Ann. Allergy Asthma Immunol. 2006, 97, 251–256. [Google Scholar] [CrossRef]
- Andreu-Ballester, J.C.; Perez-Griera, J.; Ballester, F.; Colomer-Rubio, E.; Ortiz-Tarin, I.; Penarroja Otero, C. Secretory immunoglobulin A (sIgA) deficiency in serum of patients with GALTectomy (appendectomy and tonsillectomy). Clin. Immunol. 2007, 123, 289–297. [Google Scholar] [CrossRef]
- Kaygusuz, I.; Alpay, H.C.; Gödekmerdan, A.; Karlidag, T.; Keles, E.; Yalcin, S.; Demir, N. Evaluation of long-term impacts of tonsillectomy on immune functions of children: A follow-up study. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.D.; Hung, S.H.; Lin, H.C.; Chen, K.C. Decreased clinic visits for acute respiratory infections following an adult tonsillectomy: A population-based study. Am. J. Otolaryngol. 2017, 38, 488–491. [Google Scholar] [CrossRef] [PubMed]
- Bitar, M.A.; Dowli, A.; Mourad, M. The effect of tonsillectomy on the immune system: A systematic review and meta-analysis. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Stelter, K. Tonsillitis and sore throat in children. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2014, 13, Doc07. [Google Scholar]
- Bergler, W.; Adam, S.; Gross, H.J.; Hormann, K.; Schwartz-Albiez, R. Age-dependent altered proportions in subpopulations of tonsillar lymphocytes. Clin. Exp. Immunol. 1999, 116, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chang, D.Y.; Kim, S.W.; Choi, Y.S.; Jeon, S.Y.; Racanelli, V.; Kim, D.W.; Shin, E.C. Age-related differences in human palatine tonsillar B cell subsets and immunoglobulin isotypes. Clin. Exp. Med. 2016, 16, 81–87. [Google Scholar] [CrossRef]
- Krone, C.L.; Trzciński, K.; Zborowski, T.; Sanders, E.A.M.; Bogaert, D. Impaired innate mucosal immunity in aged mice permits prolonged Streptococcus pneumoniae colonization. Infect. Immun. 2013, 81, 4615–4625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiskopf, D.; Weinberger, B.; Grubeck-Loebenstein, B. The aging of the immune system. Transpl. Int. 2009, 22, 1041–1050. [Google Scholar] [CrossRef]
- Pawelec, G.; Adibzadeh, M.; Solana, R.; Beckman, I. The T cell in the ageing individual. Mech. Ageing Dev. 1997, 93, 35–45. [Google Scholar] [CrossRef]
- Paganelli, R.; Scala, E.; Quinti, I.; Ansotegui, I.J. Humoral immunity in aging. Aging 1994, 6, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.Y.; Lee, B.S.; Kim, J.H.; Kim, J.J.; Jang, Y.; Choi, J.W.; Lee, D.J. Assessment of Volatile Sulfur Compounds in Adult and Pediatric Chronic Tonsillitis Patients Receiving Tonsillectomy. Clin. Exp. Otorhinolaryngol. 2018, 11, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.Y.; Riley, R.W.; Yu, M.S. Surgical Algorithm for Obstructive Sleep Apnea: An Update. Clin. Exp. Otorhinolaryngol. 2020, 13, 215–224. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| Tonsillectomy (n = 1005) | Control (n = 4020) | Standardized Difference | |
| Age (years old, n, %) | 0.00 | ||
| 40–44 | 123 (12.2) | 492 (12.2) | |
| 45–49 | 286 (28.5) | 1144 (28.5) | |
| 50–54 | 284 (28.3) | 1136 (28.3) | |
| 55–59 | 175 (17.4) | 700 (17.4) | |
| 60–64 | 89 (8.9) | 356 (8.9) | |
| 65–69 | 37 (3.7) | 148 (3.7) | |
| 70–74 | 4 (0.4) | 16 (0.4) | |
| 75–79 | 6 (0.6) | 24 (0.6) | |
| 80–84 | 1 (0.1) | 4 (0.1) | |
| Sex (n, %) | 0.00 | ||
| Male | 686 (68.3) | 2744 (68.3) | |
| Female | 319 (31.7) | 1276 (31.7) | |
| Income (n, %) | 0.00 | ||
| 1 (lowest) | 93 (9.3) | 372 (9.3) | |
| 2 | 100 (10.0) | 400 (10.0) | |
| 3 | 132 (13.1) | 528 (13.1) | |
| 4 | 216 (21.5) | 864 (21.5) | |
| 5 (highest) | 464 (46.2) | 1856 (46.2) | |
| Region of residence (n, %) | 0.00 | ||
| Urban | 495 (49.3) | 1980 (49.3) | |
| Rural | 510 (50.8) | 2040 (50.8) | |
| Total cholesterol level (mg/dL, mean, SD) | 200.0 (36.9) | 198.4 (36.4) | 0.04 |
| SBP (mm/Hg, mean, SD) | 125.5 (15.0) | 124.8 (15.6) | 0.05 |
| DBP (mm/Hg, mean, SD) | 79.4 (11.1) | 78.6 (10.6) | 0.07 |
| Fasting blood glucose level (mg/dL, mean, SD) | 98.8 (33.0) | 98.5 (30.6) | 0.01 |
| Obesity † (n, %) | 0.36 | ||
| Underweight | 5 (0.5) | 73 (1.8) | |
| Normal | 230 (22.9) | 1383 (34.4) | |
| Overweight | 266 (26.5) | 1139 (28.3) | |
| Obese I | 437 (43.5) | 1305 (32.5) | |
| Obese II | 67 (6.7) | 120 (3.0) | |
| Smoking status (n, %) | 0.12 | ||
| Nonsmoker | 602 (59.9) | 2422 (60.3) | |
| Past smoker | 167 (16.6) | 515 (12.8) | |
| Current smoker | 236 (23.5) | 1083 (26.9) | |
| Alcohol consumption (n, %) | 0.01 | ||
| <1 time a week | 644 (64.1) | 2558 (63.6) | |
| ≥1 time a week | 361 (35.9) | 1462 (36.4) | |
| CCI score (score, n, %) | 0.22 | ||
| 0 | 733 (72.9) | 3178 (79.1) | |
| 1 | 161 (16.0) | 390 (9.7) | |
| 2 | 67 (6.7) | 207 (5.2) | |
| ≥3 | 44 (4.4) | 245 (6.1) | |
| Asthma (n, %) | 215 (21.4) | 639 (15.9) | 0.14 |
| COPD (n, %) | 50 (5.0) | 169 (4.2) | 0.04 |
| Pre-ID pneumonia for 1y (n, %) | 0.00 | ||
| 0 times | 990 (98.5) | 3960 (98.5) | |
| ≥1 times | 15 (1.5) | 60 (1.5) | |
| Post-ID pneumonia (mean, SD) | |||
| First year-period | 0.03 (0.27) | 0.03 (0.34) | 0.01 |
| Second year-period | 0.04 (0.37) | 0.04 (0.36) | 0.02 |
| Third year-period | 0.04 (0.50) | 0.03 (0.36) | 0.03 |
| Characteristics | Mean ± SD in Tonsillectomy Group | Mean ± SD in Control Group | Linear Regression of Tonsillectomy for Pneumonia | |||
|---|---|---|---|---|---|---|
| Simple † | p-Value | Multiple †,‡ | p-Value | |||
| Post-ID 1y pneumonia | 0.03 ± 0.27 | 0.03 ± 0.34 | 0.003 (−0.020 to 0.025) | 0.812 | 0.001 (−0.021 to 0.024) | 0.918 |
| Post-ID 2y pneumonia | 0.04 ± 0.37 | 0.04 ± 0.36 | 0.007 (−0.016 to 0.031) | 0.537 | 0.006 (−0.018 to 0.030) | 0.616 |
| Post-ID 3y pneumonia | 0.04 ± 0.50 | 0.03 ± 0.36 | 0.013 (−0.014 to 0.040) | 0.329 | 0.011 (−0.016 to 0.039) | 0.408 |
| Characteristics | Mean ± SD in Tonsillectomy Group | Mean ± SD in Control Group | Linear Regression of Tonsillectomy for Pneumonia | |||
|---|---|---|---|---|---|---|
| Simple † | p-Value | Multiple †,‡ | p-Value | |||
| Age 40–59 years old (n = 4340) | ||||||
| Post-ID 1y pneumonia | 0.03 ± 0.25 | 0.02 ± 0.25 | 0.005 (−0.014 to 0.023) | 0.625 | 0.004 (−0.015 to 0.023) | 0.675 |
| Post-ID 2y pneumonia | 0.04 ± 0.33 | 0.02 ± 0.24 | 0.016 (−0.004 to 0.035) | 0.110 | 0.016 (−0.004 to 0.035) | 0.119 |
| Post-ID 3y pneumonia | 0.03 ± 0.49 | 0.03 ± 0.35 | 0.005 (−0.023 to 0.033) | 0.734 | 0.003 (−0.025 to 0.032) | 0.811 |
| Age ≥60 years old (n = 685) | ||||||
| Post-ID 1y pneumonia | 0.07 ± 0.38 | 0.08 ± 0.69 | −0.009 (−0.129 to 0.110) | 0.881 | −0.031 (−0.151 to 0.008) | 0.607 |
| Post-ID 2y pneumonia | 0.08 ± 0.54 | 0.13 ± 0.75 | −0.046 (−0.171 to 0.080) | 0.475 | −0.038 (−0.164 to 0.089) | 0.558 |
| Post-ID 3y pneumonia | 0.12 ± 0.58 | 0.05 ± 0.43 | 0.068 (−0.018 to 0.153) | 0.122 | 0.065 (−0.020 to 0.151) | 0.135 |
| Males (n = 3430) | ||||||
| Post-ID 1y pneumonia | 0.03 ± 0.28 | 0.02 ± 0.28 | 0.007 (−0.017 to 0.030) | 0.579 | 0.007 (−0.017 to 0.030) | 0.568 |
| Post-ID 2y pneumonia | 0.05 ± 0.39 | 0.03 ± 0.36 | 0.018 (−0.011 to 0.047) | 0.233 | 0.021 (−0.009 to 0.050) | 0.173 |
| Post-ID 3y pneumonia | 0.05 ± 0.59 | 0.02 ± 0.27 | 0.026 (−0.003 to 0.056) | 0.082 | 0.026 (−0.004 to 0.056) | 0.091 |
| Females (n = 1595) | ||||||
| Post-ID 1y pneumonia | 0.03 ± 0.25 | 0.04 ± 0.45 | −0.005 (−0.056 to 0.045) | 0.833 | −0.009 (−0.060 to 0.041) | 0.713 |
| Post-ID 2y pneumonia | 0.03 ± 0.31 | 0.04 ± 0.34 | −0.015 (−0.055 to 0.025) | 0.466 | −0.021 (−0.061 to 0.019) | 0.307 |
| Post-ID 3y pneumonia | 0.03 ± 0.24 | 0.05 ± 0.50 | −0.014 (−0.071 to 0.042) | 0.625 | −0.017 (−0.074 to 0.040) | 0.554 |
| No history of Pre-ID pneumonia for 1y (n = 4950) | ||||||
| Post-ID 1y pneumonia | 0.03 ± 0.26 | 0.02 ± 0.27 | 0.006 (−0.013 to 0.024) | 0.559 | 0.003 (−0.015 to 0.022) | 0.728 |
| Post-ID 2y pneumonia | 0.04 ± 0.37 | 0.03 ± 0.33 | 0.013 (−0.009 to 0.036) | 0.253 | 0.010 (−0.013 to 0.033) | 0.381 |
| Post-ID 3y pneumonia | 0.04 ± 0.49 | 0.03 ± 0.35 | 0.008 (−0.018 to 0.035) | 0.542 | 0.006 (−0.021 to 0.033) | 0.647 |
| ≥1 times history of Pre-ID pneumonia for 1y (n = 75) | ||||||
| Post-ID 1y pneumonia | 0.27 ± 0.80 | 0.45 ± 1.67 | −0.183 (−1.085 to 0.719) | 0.686 | 0.059 (−1.092 to 1.210) | 0.918 |
| Post-ID 2y pneumonia | 0.00 ± 0.00 | 0.37 ± 1.13 | −0.367 (−0.905 to 0.171) | 0.178 | −0.377 (−1.043 to 0.290) | 0.261 |
| Post-ID 3y pneumonia | 0.47 ± 0.92 | 0.12 ± 0.56 | 0.350 (−0.029 to 0.729) | 0.070 | 0.419 (−0.060 to 0.898) | 0.085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.J.; Min, C.; Yoo, D.M.; Lee, S.Y.; Choi, H.G. Tonsillectomy in Adults over 40 Years of Age Does Not Increase the Risk of Pneumonia: A Three-Year Longitudinal Follow-Up Study. Int. J. Environ. Res. Public Health 2021, 18, 13059. https://doi.org/10.3390/ijerph182413059
Park SJ, Min C, Yoo DM, Lee SY, Choi HG. Tonsillectomy in Adults over 40 Years of Age Does Not Increase the Risk of Pneumonia: A Three-Year Longitudinal Follow-Up Study. International Journal of Environmental Research and Public Health. 2021; 18(24):13059. https://doi.org/10.3390/ijerph182413059
Chicago/Turabian StylePark, Sung Joon, Chanyang Min, Dae Myoung Yoo, Sei Young Lee, and Hyo Geun Choi. 2021. "Tonsillectomy in Adults over 40 Years of Age Does Not Increase the Risk of Pneumonia: A Three-Year Longitudinal Follow-Up Study" International Journal of Environmental Research and Public Health 18, no. 24: 13059. https://doi.org/10.3390/ijerph182413059