
Exploring Potential Benefits of Accumulated Multicomponent-Training in Non-Active Older Adults: From Physical Fitness to Mental Health

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Research Design
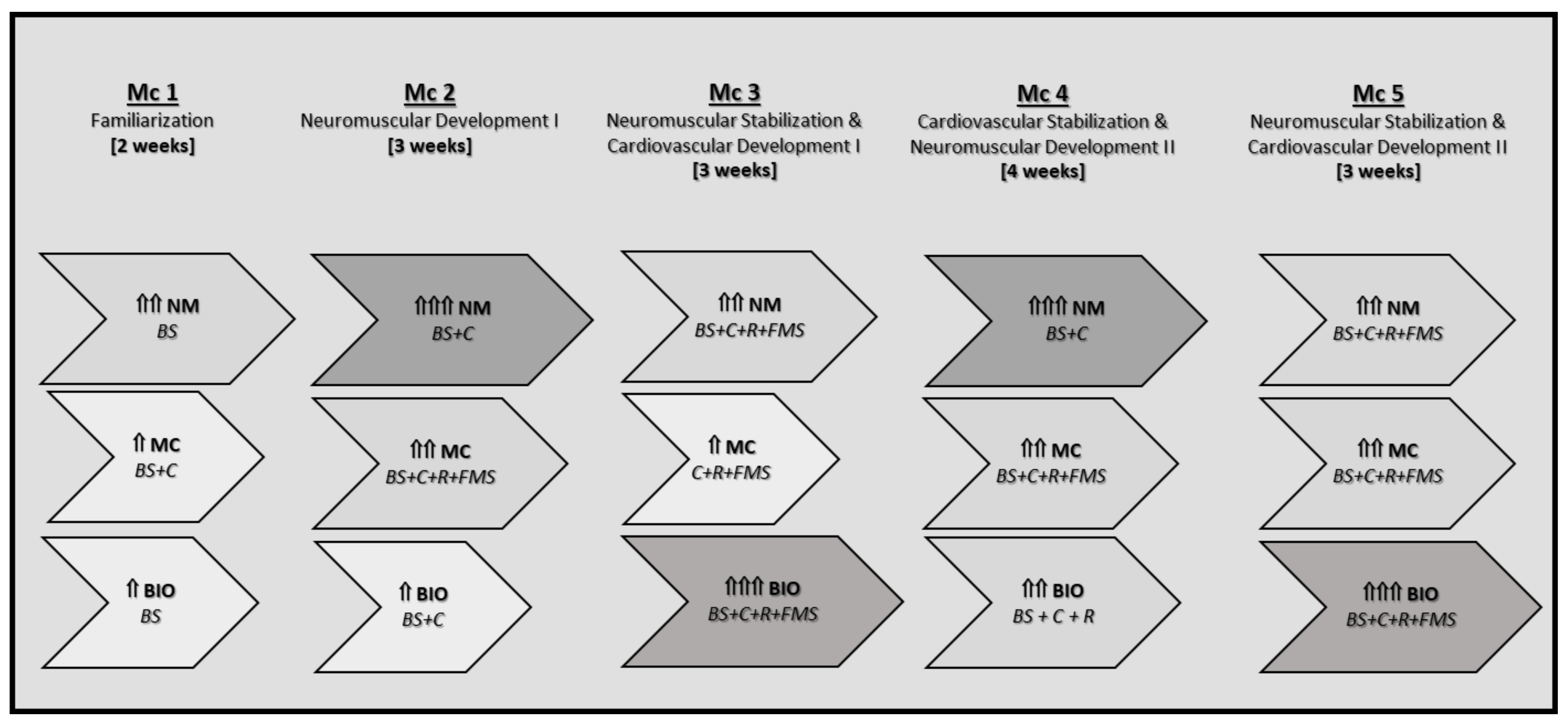
2.3. The EFAM-UV© Multicomponent Training Program
- (1)
- 10 to 15 min neuromuscular activation, based on gait training, plus postural control exercises, increasing the cognitive executive constraints according to the individual capacities.
- (2)
- 15 to 20 min of neuromuscular development strength plus balance exercises (exercises with elastic bands and dumbbells on alternating days, increasing their demands on motor control).
- (3)
- 15 to 20 min of bioenergetics (by means of gait training sequences, rhythm exercises, or functional motor skills) on different days, depending on the periodized objectives.
- (4)
- 5 to 10 min of cool down with playful and social tasks (tailoring the social interaction tasks in a way that included executive function challenges whenever possible, because both social interaction and executive function share common important mechanisms that are benefited by exercise [53]).
2.4. Outcomes
2.5. Statistical Analysis
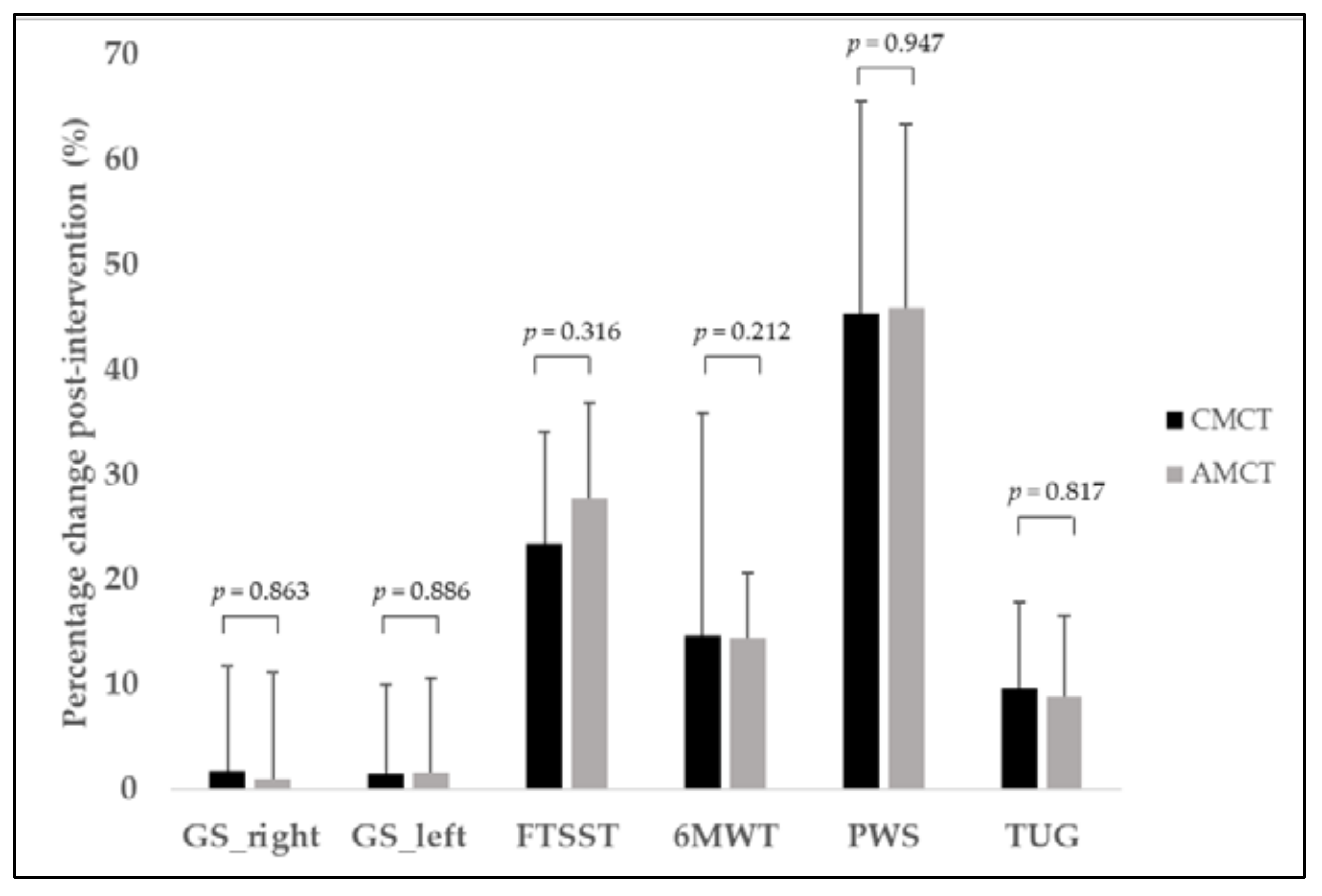
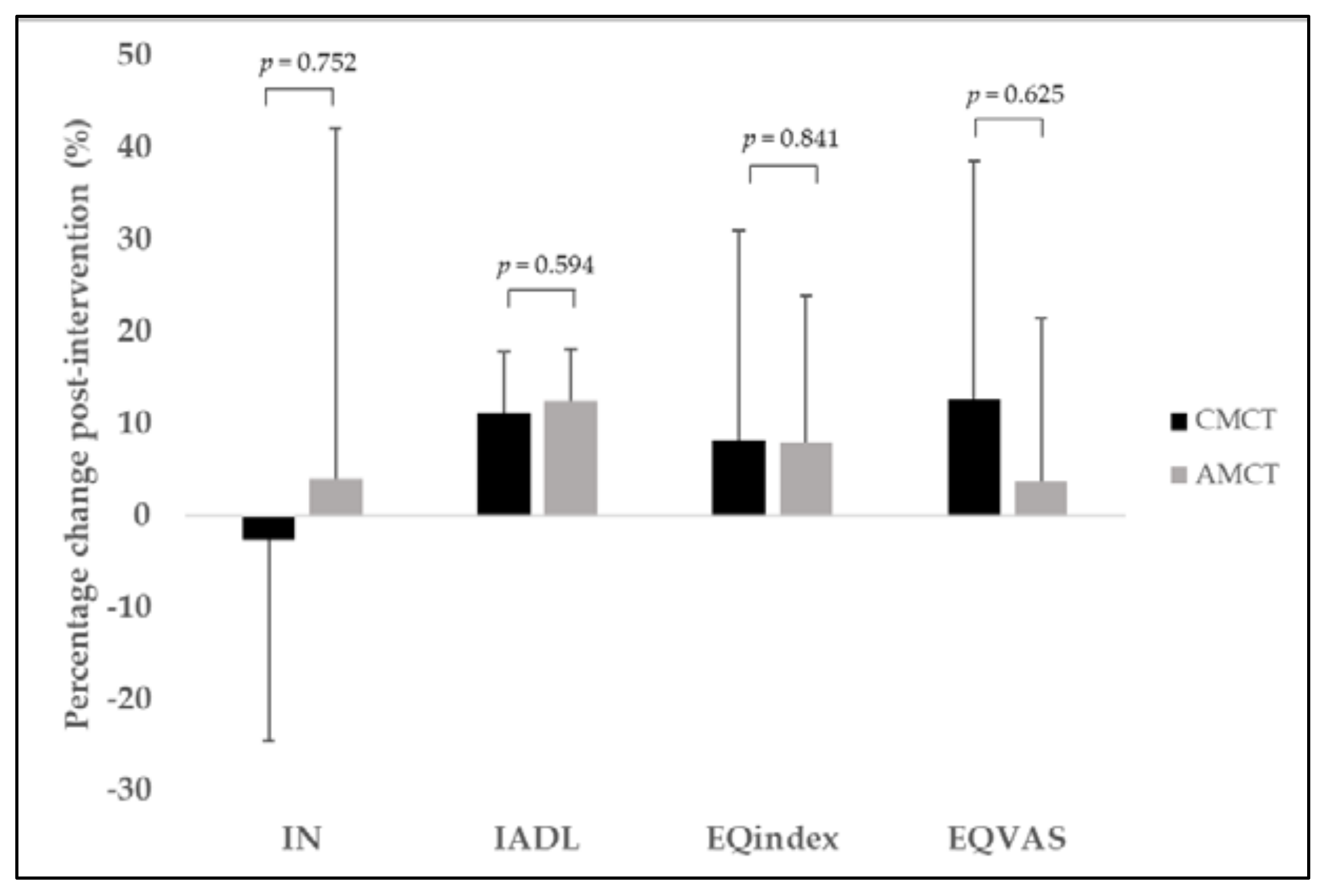
3. Results
4. Discussion
5. Conclusions and Practical Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoorens, S.; Ghez, J.; Guerin, B.; Schweppenstedde, D.; Hellgren, T.; Horvath, V.; Graf, M.; Janta, B.; Drabble, S.; Kobzar, S. Europe’s Societal Challenges: An Analysis of Global Societal Trends to 2030 and Their Impact on the EU; RAND Corporation: Santa Monica, CA, USA, 2013; Volume RR-479-EC. [Google Scholar]
- Nyman, S.R.; Barker, A.; Haines, T.; Horton, K.; Musselwhite, C.; Peeters, G.; Victor, C.R.; Wolff, J.K. The Palgrave Handbook of Ageing and Physical Activity Promotion; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Rose, D.J.; Fisher, K.L. The Role of Government Policy in Promoting Physical Activity. In the Palgrave Handbook of Ageing Physical Activity Promotion; Nyman, S.R., Barker, A., Haines, T., Horton, K., Musselwhite, C., Peeters, G., Victor, C.R., Wolff, J.K., Eds.; Palgrave Macmillan: Cham, Switzerland, 2018; pp. 607–626. [Google Scholar]
- Onambele-Pearson, G.; Ventre, J.; Brown, J.A. Reducing Sedentary Behaviour Among Older People. In the Palgrave Handbook of Ageing Physical Activity Promotion; Nyman, S.R., Barker, A., Haines, T., Horton, K., Musselwhite, C., Peeters, G., Victor, C.R., Wolff, J.K., Eds.; Palgrave Macmillan: Cham, Switzerland, 2018; pp. 653–673. [Google Scholar]
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- da Silva, V.D.; Tribess, S.; Meneguci, J.; Sasaki, J.E.; Garcia-Meneguci, C.A.; Carneiro, J.A.O.; Virtuoso, J.S. Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, P.C.; Larsen, R.N.; Dunstan, D.W.; Owen, N.; Kingwell, B.A. Sitting less and moving more: Implications for hypertension. Hypertension 2018, 72, 1037–1046. [Google Scholar] [CrossRef]
- Sellami, M.; Gasmi, M.; Denham, J.; Hayes, L.D.; Stratton, D.; Padulo, J.; Bragazzi, N. Effects of acute and chronic exercise on immunological parameters in the elderly aged: Can physical activity counteract the effects of aging? Front. Immunol. 2018, 9, 2187. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune–metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Pratt, M.; Varela, A.R.; Salvo, D.; Kohl, H.W., III; Ding, D. Attacking the pandemic of physical inactivity: What is holding us back? BMJ Publ. Group Ltd Br. Assoc. Sport Exerc. Med. 2020, 54, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Varela, A.R.; Bauman, A.E.; Ekelund, U.; Lee, I.-M.; Heath, G.; Katzmarzyk, P.T.; Reis, R.; Pratt, M. Towards better evidence-informed global action: Lessons learnt from the Lancet series and recent developments in physical activity and public health. Br. J. Sports Med. 2020, 54, 462–468. [Google Scholar] [CrossRef] [Green Version]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of physical exercise on cognitive functioning and wellbeing: Biological and psychological benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef]
- Papalia, G.F.; Papalia, R.; Diaz Balzani, L.A.; Torre, G.; Zampogna, B.; Vasta, S.; Fossati, C.; Alifano, A.M.; Denaro, V. The effects of physical exercise on balance and prevention of falls in older people: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 2595. [Google Scholar] [CrossRef]
- Raynor, A.J.; Iredale, F.; Crowther, R.; White, J.; Dare, J. It’s not just physical: Exercise physiologist-led exercise program promotes functional and psychosocial health outcomes in aged care. J. Aging Phys. Act. 2020, 28, 104–113. [Google Scholar] [CrossRef]
- Departentment of Health and Human Services (Ed.) 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report Services; US Department of Health and Human Services: Washington, DC, USA, 2018; p. 779.
- Lautenschlager, N.T.; Almeida, O.P.; Flicker, L.; Janca, A. Can physical activity improve the mental health of older adults? Ann. Gen. Hosp. Psychiatry 2004, 3, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Breda, J.; Jakovljevic, J.; Rathmes, G.; Mendes, R.; Fontaine, O.; Hollmann, S.; Rütten, A.; Gelius, P.; Kahlmeier, S.; Galea, G. Promoting health-enhancing physical activity in Europe: Current state of surveillance, policy development and implementation. Health Policy 2018, 122, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Gomes, M.; Figueiredo, D.; Teixeira, L.; Poveda, V.; Paúl, C.; Santos-Silva, A.; Costa, E. Physical inactivity among older adults across Europe based on the SHARE database. Age Ageing 2017, 46, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Rebelo-Marques, A.; De Sousa Lages, A.; Andrade, R.; Ribeiro, C.F.; Mota-Pinto, A.; Carrilho, F.; Espregueira-Mendes, J. Aging hallmarks: The benefits of physical exercise. Front. Endocrinol. 2018, 9, 258. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Off. J. Am. Coll. Sports Med. 2011, 26. [Google Scholar] [CrossRef]
- Taylor, J.; Walsh, S.; Kwok, W.; Pinheiro, M.B.; de Oliveira, J.S.; Hassett, L.; Bauman, A.; Bull, F.; Tiedemann, A.; Sherrington, C. A scoping review of physical activity interventions for older adults. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herold, F.; Hamacher, D.; Schega, L.; Müller, N.G. Thinking while moving or moving while thinking–concepts of motor-cognitive training for cognitive performance enhancement. Front. Aging Neurosci. 2018, 10, 228. [Google Scholar] [CrossRef] [Green Version]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of physical exercise interventions on gait-related dual-task interference in older adults: A systematic review and meta-analysis. Gerontology 2016, 62, 94–117. [Google Scholar] [CrossRef] [PubMed]
- Yerrakalva, D.; Cooper, A.; Westgate, K.; Khaw, K.-T.; Wareham, N.; Brage, S.; Griffin, S.; Wijndaele, K. The descriptive epidemiology of the diurnal profile of bouts and breaks in sedentary time in older English adults. Int. J. Epidemiol. 2017, 46, 1871–1881. [Google Scholar] [CrossRef] [PubMed]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Baptista, F.; Owen, N. Breaking-up sedentary time is associated with physical function in older adults. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2015, 70, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Benatti, F.B.; Ried-Larsen, M.J. The effects of breaking up prolonged sitting time: A review of experimental studies. Med. Sci. Sports Exerc. 2015, 47, 2053–2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartini, C.; Wannamethee, S.G.; Iliffe, S.; Morris, R.W.; Ash, S.; Lennon, L.; Whincup, P.H.; Jefferis, B.J. Diurnal patterns of objectively measured physical activity and sedentary behaviour in older men. BMC Public Health 2015, 15, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Naranjo-Orellana, J.; Álvarez Medina, J.; Blasco-Lafarga, C.; Gaztañaga Aurrekoetxea, T. Obesity and physical exercise in adults/Obesidad y ejercicio físico en adultos. Arch. Med. Deporte 2020, 37, 326–337. [Google Scholar] [CrossRef]
- Dondzila, C.J.; Gennuso, K.P.; Swartz, A.M.; Tarima, S.; Lenz, E.K.; Stein, S.S.; Kohl, R.J.; Strath, S.J. Dose-response walking activity and physical function in older adults. J. Aging Phys. Act. 2015, 23, 194–199. [Google Scholar] [CrossRef]
- Monteagudo, P.; Roldán, A.; Cordellat, A.; Gómez-Cabrera, M.C.; Blasco-Lafarga, C. Continuous compared to accumulated walking-training on physical function and health-related quality of life in sedentary older persons. Int. J. Environ. Res. Public Health 2020, 17, 6060. [Google Scholar] [CrossRef]
- Blasco-Lafarga, C.; Monteagudo, P.; Roldán, A.; Cordellat, A.; Pesce, C. Strategies to change body composition in older adults: Do type of exercise and dose distribution matter? J. Sports Med. Phys. Fit. 2020, 60, 10. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.-M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081. [Google Scholar] [CrossRef] [Green Version]
- Staffileno, B.A.; Braun, L.T.; Rosenson, R.S. The accumulative effects of physical activity in hypertensive post-menopausal women. Eur. J. Cardiovasc. Prev. Rehabil. 2001, 8, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Leitão, L.; Pereira, A.; Mazini, M.; Venturini, G.; Campos, Y.; Vieira, J.; Novaes, J.; Vianna, J.; da Silva, S.; Louro, H. Effects of three months of detraining on the health profile of older women after a multicomponent exercise program. Int. J. Environ. Res. Public Health 2019, 16, 3881. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, C.V.L.; de Rezende, T.J.R.; Weiler, M.; Magalhães, T.N.C.; Carletti-Cassani, A.F.M.K.; Silva, T.Q.A.C.; Joaquim, H.P.G.; Talib, L.L.; Forlenza, O.V.; Franco, M.P. Cognitive and structural cerebral changes in amnestic mild cognitive impairment due to Alzheimer’s disease after multicomponent training. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C.; Sanchis-Sanchis, R.; Sanchis-Soler, G.; San Inocencio-Cuenca, D.; Llorens-Soriano, P. Entrenamiento Neuromotor en pacientes ancianos pluripatológicos en las Unidades de Hospitalización a Domicilio: Estudio piloto. Cuad. Psicol. Deporte 2019, 19, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, A.K.; Griebler, E.M.; da Silva, W.A.; Sant, D.P.; da Silva, P.C.; Possamai, V.D.; Martins, V.F. Does a Multicomponent Exercise Program Improve Physical Fitness in Older Adults? Findings From a 5-Year Longitudinal Study. J. Aging Phys. Act. 2021, 1, 1–8. [Google Scholar]
- Moradell, A.; Navarrete-Villanueva, D.; Fernández-García, Á.I.; Sagarra-Romero, L.; Marín-Puyalto, J.; Pérez-Gómez, J.; Gesteiro, E.; Ara, I.; Casajus, J.A.; Gómez-Cabello, A. Effects of a multicomponent exercise program, a detraining period and dietary intake prediction of body composition of frail and pre-frail older adults from the exernet elder 3.0 study. Sustainability 2020, 12, 9894. [Google Scholar] [CrossRef]
- Sunde, S.; Hesseberg, K.; Skelton, D.A.; Ranhoff, A.H.; Pripp, A.H.; Aarønæs, M.; Brovold, T. Effects of a multicomponent high intensity exercise program on physical function and health-related quality of life in older adults with or at risk of mobility disability after discharge from hospital: A randomised controlled trial. BMC Geriatr. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Bouaziz, W.; Lang, P.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pract. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- Blasco-Lafarga, C.; Cordellat, A.; Forte, A.; Roldán, A.; Monteagudo, P. Short and long-term trainability in older adults: Training and detraining following two years of multicomponent cognitive—physical exercise training. Int. J. Environ. Res. Public Health 2020, 17, 5984. [Google Scholar] [CrossRef]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E.D. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Aging 2015, 10, 1711. [Google Scholar] [CrossRef] [Green Version]
- Monteagudo, P.; Cordellat, A.; Roldán, A.; Gómez-Cabrera, M.; Blasco-Lafarga, C. Effects of multicomponent exercise on metabolic health parameters in elderly. MOJ Sports Med. 2019, 3, 70–74. [Google Scholar]
- Roldán, A.; Cordellat, A.; Monteagudo, P.; García-Lucerga, C.; Blasco-Lafarga, N.M.; Gomez-Cabrera, M.C.; Blasco-Lafarga, C. Beneficial effects of inspiratory muscle training combined with multicomponent training in elderly active women. Res. Q. Exerc. Sport 2019, 90, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Sanchis, R.; Blasco-Lafarga, C.; Encarnación-Martínez, A.; Pérez-Soriano, P. Changes in plantar pressure and spatiotemporal parameters during gait in older adults after two different training programs. Gait Posture 2020, 77, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Soler, G.; Saninocencio, D.; Llorens, P.; Blasco-Lafarga, C. Reducción de la sobrecarga del cuidador tras entrenamiento supervisado en ancianos pluripatológicos y paliativos. Cuad. Psicol. Deporte 2021, 21, 271–281. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.; De La Cámara, C.; Ventura, T.; Pascual, F.; Montanes, J.; Aznar, S. Revalidation and standardization of the cognition mini-exam (first Spanish version of the Mini-Mental Status Examination) in the general geriatric population. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Blasco-Lafarga, C.; Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Monteagudo, P.; Sanchis-Soler, G.; Sanchis-Sanchis, R. Método de Entrenamiento Funcional Cognitivo Neuromotor; University of Valencia: Valencia, Spain, 2016. [Google Scholar]
- von Hippel, W. Aging, executive functioning, and social control. Curr. Dir. Psychol. Sci. 2007, 16, 240–244. [Google Scholar] [CrossRef]
- Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Sanchis, G.; Blasco-Lafarga, C. 120 min/week of neuromotor multicomponent training are enough to improve executive function and functional fitness in older women. Exp. Gerontol. 2021, 145, 111199. [Google Scholar] [CrossRef]
- Mian, O.S.; Baltzopoulos, V.; Minetti, A.E.; Narici, M.V. The impact of physical training on locomotor function in older people. Sports Med. 2007, 37, 683–701. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Martin-Lesende, I.; Vrotsou, K.; Vergara, I.; Bueno, A.; Diez, A.; Nuñez, J. Design and validation of the vida questionnaire, for assessing instrumental activities of daily living in elderly people. J. Gerontol. Geriatr. Res. 2015, 4, 2. [Google Scholar]
- Golden, C. Stroop: Test. de Colores y Palabras; TEA Ediciones: Madrid, Spain, 1994. [Google Scholar]
- Rivera, D.; Perrin, P.; Stevens, L.; Garza, M.; Weil, C.; Saracho, C.; Rodriguez, W.; Rodriguez-Agudelo, Y.; Rábago, B.; Weiler, G. Stroop color-word interference test: Normative data for the Latin American Spanish speaking adult population. NeuroRehabilitation 2015, 37, 591–624. [Google Scholar] [CrossRef] [PubMed]
- Monteagudo, P.; Cordellat, A.; Roldán, A.; Pesce, C.; Blasco-Lafarga, C. Assessing health-related quality of life in older adults: EuroQol five-dimensional questionnaire vs the short form health survey. Sport Mont 2020, 18, 117–120. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.; Morley, J.; Anker, S.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.; Cesari, M.J. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 1–30. [Google Scholar] [CrossRef]
- Concannon, L.G.; Grierson, M.J.; Harrast, M.A. Exercise in the older adult: From the sedentary elderly to the masters athlete. PM&R 2012, 4, 833–839. [Google Scholar]
- Valdés-Badilla, P.A.; Gutiérrez-García, C.; Pérez-Gutiérrez, M.; Vargas-Vitoria, R.; López-Fuenzalida, A. Effects of physical activity governmental programs on health status in independent older adults: A systematic review. J. Aging Phys. Act. 2019, 27, 265–275. [Google Scholar] [CrossRef]
- Rejeski, W.J.; Mihalko, S.L. Physical activity and quality of life in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Victor, C.R. Current Issues and Debates in Promoting Physical Activity Among Older People. In the Palgrave Handbook of Ageing Physical Activity Promotion; Nyman, S.R., Barker, A., Haines, T., Horton, K., Musselwhite, C., Peeters, G., Victor, C.R., Wolff, J.K., Eds.; Palgrave Macmillan: Cham, Switzerland, 2018; pp. 627–629. [Google Scholar]
- Blasco-Lafarga, C.; Monteagudo, P.; Blasco-Lafarga, N.M.; Cordellat, A.; Roldán, A. Función ejecutiva, capacidad cardiovascular y calidad de vida en mayores del entorno rural: Impacto de un programa multidisciplinar. Comunidad 2016, 2, 1–6. [Google Scholar]
- Magutah, K.; Thairu, K.; Patel, N. Effect of short moderate intensity exercise bouts on cardiovascular function and maximal oxygen consumption in sedentary older adults. BMJ Open Sport Exerc. Med. 2020, 6, e000672. [Google Scholar] [CrossRef] [Green Version]
- Candela, F.; Zucchetti, G.; Ortega, E.; Rabaglietti, E.; Magistro, D. Preventing loss of basic activities of daily living and instrumental activities of daily living in elderly. Holist. Nurs. Pract. 2015, 29, 313–322. [Google Scholar] [CrossRef]
- Hairi, N.N.; Cumming, R.G.; Naganathan, V.; Handelsman, D.J.; Le Couteur, D.G.; Creasey, H.; Waite, L.M.; Seibel, M.J.; Sambrook, P.N. Loss of muscle strength, mass (sarcopenia), and quality (specific force) and its relationship with functional limitation and physical disability: The Concord Health and Ageing in Men Project. J. Am. Geriatr. Soc. 2010, 58, 2055–2062. [Google Scholar] [CrossRef]
- Jindo, T.; Tsunoda, K.; Kitano, N.; Tsuji, T.; Abe, T.; Muraki, T.; Hotta, K.; Okura, T. Pedometers affect changes in lower-extremity physical function during a square-stepping exercise program in older Japanese adults. J. Geriatr. Phys. Ther. 2016, 39, 83–88. [Google Scholar] [CrossRef]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting time, physical activity, and risk of mortality in adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Ciprandi, D.; Zago, M.; Bertozzi, F.; Sforza, C.; Galvani, C. Influence of energy cost and physical fitness on the preferred walking speed and gait variability in elderly women. J. Electromyogr. Kinesiol. 2018, 43, 1–6. [Google Scholar] [CrossRef]
- Cordellat, A.; Roldán, A.; Monteagudor, P.; Forte Deltell, A.; Blasco-Lafarga, C. T test vs categorical analysis: Evolution of agility in older adults following two years of training. Retos 2021, 39, 988–992. [Google Scholar]
- Alexandre, T.S.; Meira, D.M.; Rico, N.C.; Mizuta, S.K. Accuracy of Timed Up and Go Test for screening risk of falls among community-dwelling elderly. Braz. J. Phys. Ther. 2012, 16, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buatois, S.; Miljkovic, D.; Manckoundia, P.; Gueguen, R.; Miget, P.; Vançon, G.; Perrin, P.; Benetos, A. Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older. J. Am. Geriatr. Soc. 2008, 56, 1575–1577. [Google Scholar] [CrossRef]
- Melby-Lervåg, M.; Redick, T.S.; Hulme, C. Working memory training does not improve performance on measures of intelligence or other measures of “far transfer” evidence from a meta-analytic review. Perspect. Psychol. Sci. 2016, 11, 512–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, L.; Murphy, K.; Andrews, G. Immediate and long-term efficacy of executive functions cognitive training in older adults: A systematic review and meta-analysis. Psychol. Bull. 2019, 145, 698–733. [Google Scholar] [CrossRef] [PubMed]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of physical-cognitive dual task training on executive function and gait performance in older adults: A randomized controlled trial. BioMed Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef]
- Jefferis, B.J.; Parsons, T.J.; Sartini, C.; Ash, S.; Lennon, L.T.; Papacosta, O.; Morris, R.W.; Wannamethee, S.G.; Lee, I.-M.; Whincup, P.H. Objectively measured physical activity, sedentary behaviour and all-cause mortality in older men: Does volume of activity matter more than pattern of accumulation? Br. J. Sports Med. 2019, 53, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Peven, J.C.; Grove, G.A.; Jakicic, J.M.; Alessi, M.G.; Erickson, K.I. Associations between short and long bouts of physical activity with executive function in older adults. J. Cogn. Enhanc. 2018, 2, 137–145. [Google Scholar] [CrossRef]
- Rodrigues, L.; Bherer, L.; Bosquet, L.; Vrinceanu, T.; Nadeau, S.; Lehr, L.; Bobeuf, F.; Kergoat, M.J.; Vu, T.T.M.; Berryman, N. Effects of an 8-week training cessation period on cognition and functional capacity in older adults. Exp. Gerontol. 2020, 134, 110890. [Google Scholar] [CrossRef] [PubMed]
- Takata, Y.; Ansai, T.; Soh, I.; Awano, S.; Yoshitake, Y.; Kimura, Y.; Sonoki, K.; Kagiyama, S.; Yoshida, A.; Nakamichi, I. Quality of life and physical fitness in an 85-year-old population. Arch. Gerontol. Geriatr. 2010, 50, 272–276. [Google Scholar] [CrossRef]
- Seino, S.; Kitamura, A.; Tomine, Y.; Tanaka, I.; Nishi, M.; Taniguchi, Y.; Yokoyama, Y.; Amano, H.; Fujiwara, Y.; Shinkai, S. Exercise arrangement is associated with physical and mental health in older adults. Med. Sci. Sports Exerc. 2019, 51, 1146. [Google Scholar] [CrossRef] [Green Version]
- Cress, M.E.; Buchner, D.; Prohaska, T.; Rimmer, J.; Brown, M.; Macera, C.; DePietro, L.; Chodzko-Zajko, W. Physical activity programs and behavior counseling in older adult populations. Med. Sci. Sports Exerc. Psychol. 2004, 36, 1997–2003. [Google Scholar] [CrossRef] [PubMed]
- McCorry, M.J.; Murphy, M.H.; Bleakley, C.; Mair, J. Effectiveness of physical activity and sedentary behaviour interventions in altering sedentary behaviour among older adults: A systematic review. Lancet 2018, 392, S61. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total, N = 24 | CMCT, N = 14 | AMCT, N = 10 | p a | |
|---|---|---|---|---|
| Age | 71.75 ± 4.51 | 71.07 ± 5.09 | 72.70 ± 3.59 | 0.395 |
| Weight, kg | 72.42 ± 13.86 | 72.95 ± 12.39 | 71.67 ± 16.37 | 0.829 |
| Height, m | 1.59 ± 0.09 | 1.59 ± 0.09 | 1.59 ± 0.10 | 0.912 |
| BMI, kg/m2 | 28.12 ± 3.50 | 28.35 ± 3.46 | 27.79 ± 3.70 | 0.708 |
| SBP, mmHg | 149.12 ± 19.38 | 145.29 ± 20.40 | 154.50 ± 17.43 | 0.260 |
| DBP, mmHg | 82.42 ± 9.89 | 81.43 ± 10.17 | 83.80 ± 9.86 | 0.574 |
| SpO2, % | 96.96 ± 1.33 | 96.93 ± 1.33 | 97.00 ± 1.41 | 0.886 |
| HR, bpm | 72.58 ± 9.50 | 71.14 ± 6.83 | 74.60 ± 12.46 | 0.391 |
| Sex | ||||
| Females, % (n) | 58.30 (14) | 64.30 (9) | 50.00 (5) | 0.678 |
| Males, % (n) | 41.70 (10) | 35.70 (5) | 50.00 (5) |
| ANOVA Factors | Variable | Type III Sum of Squares | df | Mean Square | F | p | Partial Eta Squared |
|---|---|---|---|---|---|---|---|
| Intervention | BMI | 1.01 | 1 | 1.01 | 2.393 | 0.136 | 0.098 |
| GSright | 0.08 | 1 | 0.08 | 0.02 | 0.892 | 0.001 | |
| GSleft | 0.33 | 1 | 0.33 | 0.12 | 0.735 | 0.005 | |
| FTSST | 105.86 | 1 | 105.86 | 79.00 | 0.001 * | 0.782 | |
| 6MWT | 49291.67 | 1 | 49291.67 | 52.63 | 0.001 * | 0.705 | |
| PWS | 2.55 | 1 | 2.55 | 149.00 | 0.001 * | 0.871 | |
| TUG | 5.56 | 1 | 5.56 | 30.34 | 0.001 * | 0.580 | |
| IN | 2.91 | 1 | 2.91 | 0.09 | 0.770 | 0.004 | |
| IADL | 164.06 | 1 | 164.06 | 98.21 | 0.001 * | 0.817 | |
| EQindex | 0.03 | 1 | 0.03 | 3.87 | 0.062 ꝉ | 0.150 | |
| EQVAS | 174.21 | 1 | 174.21 | 1.92 | 0.180 | 0.080 | |
| Intervention × Dose-distribution | BMI | 0.41 | 1 | 0.41 | 0.96 | 0.337 | 0.042 |
| GSright | 1.07 | 1 | 1.07 | 0.25 | 0.619 | 0.011 | |
| GSleft | 0.51 | 1 | 0.51 | 0.18 | 0.676 | 0.008 | |
| FTSST | 0.11 | 1 | 0.11 | 0.09 | 0.772 | 0.004 | |
| 6MWT | 1052.92 | 1 | 1052.92 | 1.12 | 0.300 | 0.049 | |
| PWS | 0.01 | 1 | 0.01 | 0.52 | 0.478 | 0.023 | |
| TUG | 0.01 | 1 | 0.01 | 0.07 | 0.800 | 0.003 | |
| IN | 24.15 | 1 | 24.15 | 0.73 | 0.402 | 0.032 | |
| IADL | 0.729 | 1 | 0.729 | 0.44 | 0.516 | 0.019 | |
| EQindex | <0.001 | 1 | <0.001 | 0.01 | 0.957 | <0.001 | |
| EQVAS | 49.71 | 1 | 49.71 | 0.55 | 0.467 | 0.024 |
| Pre-CMCT | Post-CMCT | ES | Pre-AMCT | Post-AMCT | ES | |
|---|---|---|---|---|---|---|
| BMI, kg/m2 | 28.35 ± 3.46 | 28.24 ± 3.27 | 0.03 | 27.79 ± 3.70 | 27.31 ± 2.99 | 0.14 |
| GSright, kg | 30.73 ± 10.39 | 31.11 ± 10.66 | 0.04 | 34.46 ± 11.01 | 34.24 ± 9.57 | 0.02 |
| GSleft, kg | 28.16 ± 9.36 | 28.54 ± 9.72 | 0.04 | 31.64 ± 10.74 | 31.60 ± 9.30 | 0.01 |
| FTSST, s | 12.55 ± 2.83 | 9.44 ± 1.72 ** | 1.33 | 10.37 ± 2.35 | 7.46 ± 1.75 ** | 1.40 |
| 6MWT, m | 474.14 ± 93.60 | 529.64 ± 82.76 ** | 0.63 | 515.10 ± 20.24 | 589.60 ± 40.38 ** | 2.33 |
| PWS, m/s | 1.00 ± 0.18 | 1.44 ± 0.26 ** | 1.97 | 1.09 ± 0.80 | 1.58 ± 0.18 ** | 0.84 |
| TUG, s | 7.49 ± 1.11 | 6.77 ± 1.16 ** | 0.63 | 6.84 ± 1.01 | 6.18 ± 0.62 * | 0.79 |
| IN | −3.57 ± 8.47 | −4.51 ± 7.31 | 0.12 | −8.87 ± 10.28 | −6.93 ± 12.89 | 0.17 |
| IADL | 33.07 ± 2.87 | 36.57 ± 1.65 ** | 1.50 | 32.80 ± 1.93 | 36.80 ± 0.92 ** | 2.65 |
| EQindex | 0.85 ± 0.11 | 0.90 ± 0.10 | 0.48 | 0.86 ± 0.17 | 0.91 ± 0.12 | 0.34 |
| EQVAS | 74.07 ± 17.97 | 80.00 ± 10.38 | 0.40 | 83.20 ± 10.17 | 85.00 ± 10.27 | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monteagudo, P.; Cordellat, A.; Roldán, A.; Gómez-Cabrera, M.C.; Pesce, C.; Blasco-Lafarga, C. Exploring Potential Benefits of Accumulated Multicomponent-Training in Non-Active Older Adults: From Physical Fitness to Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 9645. https://doi.org/10.3390/ijerph18189645
Monteagudo P, Cordellat A, Roldán A, Gómez-Cabrera MC, Pesce C, Blasco-Lafarga C. Exploring Potential Benefits of Accumulated Multicomponent-Training in Non-Active Older Adults: From Physical Fitness to Mental Health. International Journal of Environmental Research and Public Health. 2021; 18(18):9645. https://doi.org/10.3390/ijerph18189645
Chicago/Turabian StyleMonteagudo, Pablo, Ana Cordellat, Ainoa Roldán, Mari Carmen Gómez-Cabrera, Caterina Pesce, and Cristina Blasco-Lafarga. 2021. "Exploring Potential Benefits of Accumulated Multicomponent-Training in Non-Active Older Adults: From Physical Fitness to Mental Health" International Journal of Environmental Research and Public Health 18, no. 18: 9645. https://doi.org/10.3390/ijerph18189645