
Afghan Women’s Use of Violence against Their Children and Associations with IPV, Adverse Childhood Experiences and Poverty: A Cross-Sectional and Structural Equation Modelling Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Ethical Considerations
2.3. Measurement Tools
2.3.1. Corporal Punishment
2.3.2. Co-Variates
2.4. Statistical Analysis
3. Results
3.1. Demographic Description of the Sample
3.2. Bivariate Analysis
3.3. Multivariable Regression Analysis
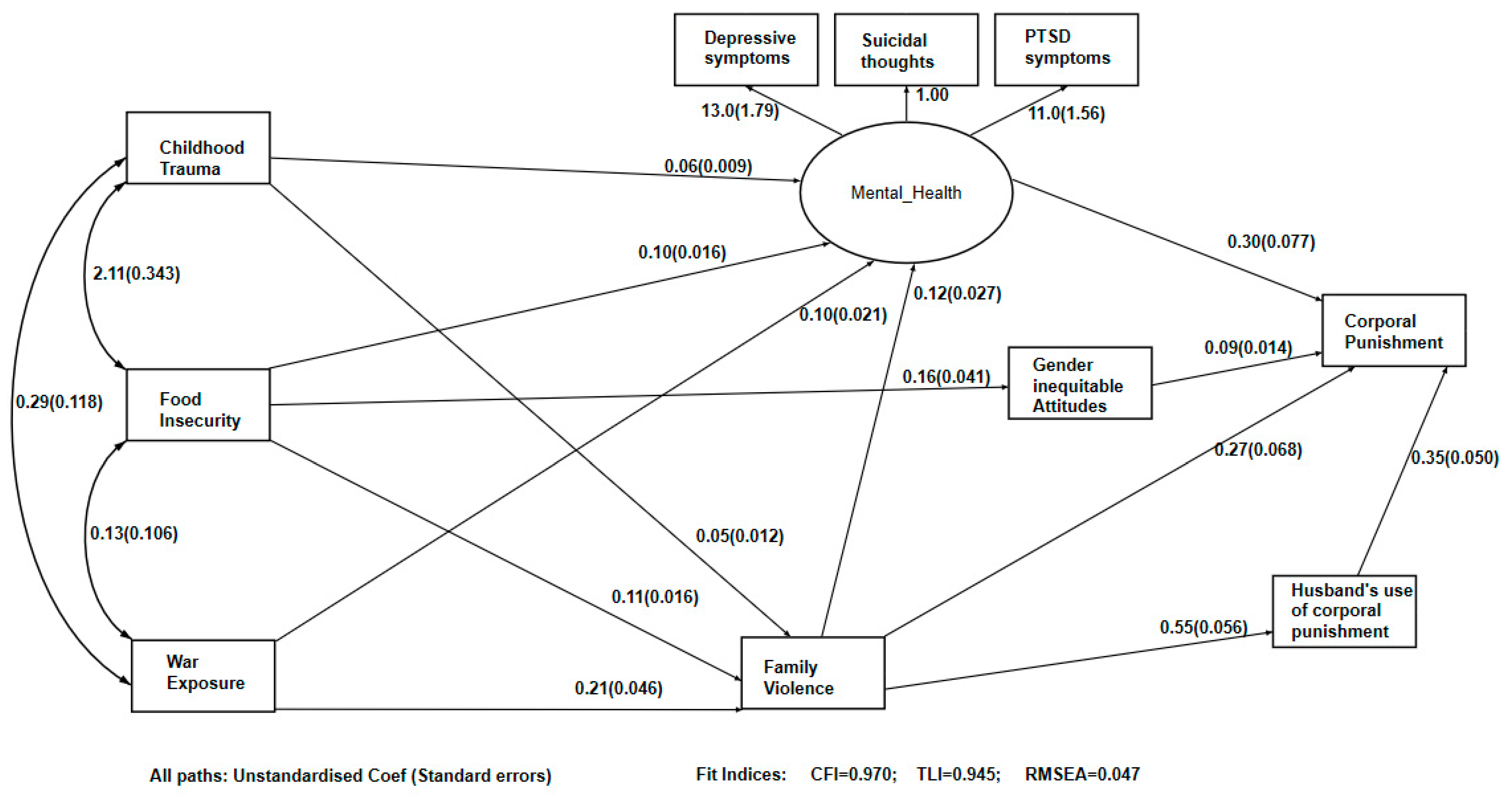
3.4. Structural Equation Model
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hillis, S.; Mercy, J.; Amobi, A.; Kress, H. Global Prevalence of Past-year Violence Against Children: A Systematic Review and Minimum Estimates. Pediatrics 2016, 137, e20154079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, L.; Bellis, M.A.; Wood, S.; Hughes, K.; McCoy, E.; Eckley, L.; Bates, G.; Mikton, C.; Shakespeare, T.; Officer, A. Prevalence and risk of violence against children with disabilities: A systematic review and meta-analysis of observational studies. Lancet 2012, 380, 899–907. [Google Scholar] [CrossRef]
- Stark, L.; Landis, D. Violence against children in humanitarian settings: A literature review of population-based approaches. Soc. Sci. Med. 2016, 152, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Saile, R.; Ertl, V.; Neuner, F.; Catani, C. Does war contribute to family violence against children? Findings from a two-generational multi-informant study in Northern Uganda. Child Abus. Negl. 2014, 38, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, B.L.; Stark, L. The impact of humanitarian emergencies on the prevalence of violence against children: An evidence-based ecological framework. Psychol. Health Med. 2017, 22, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Rubenstein, B.L.; Lu, L.Z.N.; MacFarlane, M.; Stark, L. Predictors of Interpersonal Violence in the Household in Humanitarian Settings: A Systematic Review. Trauma Violence Abus. 2017, 21, 31–44. [Google Scholar] [CrossRef]
- Cuartas, J.; Grogan-Kaylor, A.; Ma, J.; Castillo, B. Civil conflict, domestic violence, and poverty as predictors of corporal punishment in Colombia. Child Abus. Negl. 2019, 90, 108–119. [Google Scholar] [CrossRef]
- Catani, C.; Schauer, E.; Neuner, F. Beyond Individual War Trauma: Domestic Violence Against Children in Afghanistan and Sri Lanka. J. Marital Fam. Ther. 2008, 34, 165–176. [Google Scholar] [CrossRef]
- Christie, H.; Hamilton-Giachritsis, C.; Alves-Costa, F.; Tomlinson, M.; Halligan, S.L. The impact of parental posttraumatic stress disorder on parenting: A systematic review. Eur. J. Psychotraumatol. 2019, 10, 1550345. [Google Scholar] [CrossRef] [Green Version]
- Huang, K.-Y.; Abura, G.; Theise, R.; Nakigudde, J. Parental Depression and Associations with Parenting and Children’s Physical and Mental Health in a Sub-Saharan African Setting. Child Psychiat. Hum. Dev. 2017, 48, 517–527. [Google Scholar] [CrossRef]
- Miller, K.E.; Rasmussen, A. War exposure, daily stressors, and mental health in conflict and post-conflict settings: Bridging the divide between trauma-focused and psychosocial frameworks. Soc. Sci. Med. 2010, 70, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Hynes, M.E.; Sterk, C.E.; Hennink, M.; Patel, S.; DePadilla, L.; Yount, K.M. Exploring gender norms, agency and intimate partner violence among displaced Colombian women: A qualitative assessment. Glob. Public Health 2016, 11, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Namy, S.; Carlson, C.; O’Hara, K.; Nakuti, J.; Bukuluki, P.; Lwanyaaga, J.; Namakula, S.; Nanyunja, B.; Wainberg, M.L.; Naker, D.; et al. Towards a feminist understanding of intersecting violence against women and children in the family. Soc. Sci. Med. 2017, 184, 40–48. [Google Scholar] [CrossRef]
- Fulu, E.; Miedema, S.; Roselli, T.; McCook, S.; Chan, K.L.; Haardörfer, R.; Jewkes, R.; Fulu, E.; Jewkes, R.; Warner, X.; et al. Pathways between childhood trauma, intimate partner violence, and harsh parenting: Findings from the UN Multi-country Study on Men and Violence in Asia and the Pacific. Lancet Glob. Health 2017, 5, e512–e522. [Google Scholar] [CrossRef] [Green Version]
- Mootz, J.J.; Stark, L.; Meyer, E.; Asghar, K.; Roa, A.H.; Potts, A.; Poulton, C.; Marsh, M.; Ritterbusch, A.; Bennouna, C. Examining intersections between violence against women and violence against children: Perspectives of adolescents and adults in displaced Colombian communities. Confl. Health 2019, 13, 25. [Google Scholar] [CrossRef]
- UNICEF. Child Disciplinary Practices at Home: Evidence from a Range of Low- and Middle-Income Countries; UNICEF: New York, NY, USA, 2010. [Google Scholar]
- Akinola, A.; Olusegun, O.; Okunade, O. Effects of corporal punishment on learning behaviour and student’s academic performance in public secondary schools in Ibarapa east local govenment, Oyo State. Int. J. Adv. Acad. Res. 2017, 3, 14–20. [Google Scholar]
- Gershoff, E.T.; Lansford, J.E.; Sexton, H.R.; Davis-Kean, P.; Sameroff, A.J. Longitudinal Links Between Spanking and Children’s Externalizing Behaviors in a National Sample of White, Black, Hispanic, and Asian American Families. Child Dev. 2012, 83, 838–843. [Google Scholar] [CrossRef] [Green Version]
- Lansford, J.E.; Chang, L.; Dodge, K.A.; Malone, P.S.; Oburu, P.; Palmérus, K.; Bacchini, D.; Pastorelli, C.; Bombi, A.S.; Zelli, A.; et al. Physical discipline and children’s adjustment: Cultural normativeness as a moderator. Child Dev. 2005, 76, 1234–1246. [Google Scholar] [CrossRef]
- McLoyd, V.C.; Smith, J. Physical Discipline and Behavior Problems in African American, European American, and Hispanic Children: Emotional Support as a Moderator. J. Marriage Fam. 2002, 64, 40–53. [Google Scholar] [CrossRef]
- Gershoff, E.T.; Grogan-Kaylor, A. Spanking and child outcomes: Old controversies and new meta-analyses. J. Fam. Psychol. 2016, 30, 453–469. [Google Scholar] [CrossRef] [Green Version]
- Corboz, J.; Siddiq, W.; Hemat, O.; Chirwa, E.D.; Jewkes, R. What works to prevent violence against children in Afghanistan? Findings of an interrupted time series evaluation of a school-based peace education and community social norms change intervention in Afghanistan. PLoS ONE 2019, 14, e0220614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D. Love, Fear and Discipline: Everyday Violence toward Children in Afghan Families; Afghanistan Research and Evaluation Unit: Kabul, Afghanistan, 2008. [Google Scholar]
- Gibbs, A.; Corboz, J.; Shafiq, M.; Marofi, F.; Mecagni, A.; Mann, C.; Karim, F.; Chirwa, E.; Maxwell-Jones, C.; Jewkes, R. An individually randomized controlled trial to determine the effectiveness of the Women for Women International Programme in reducing intimate partner violence and strengthening livelihoods amongst women in Afghanistan: Trial design, methods and baseline findings. BMC Public Health 2018, 18, 164. [Google Scholar]
- OCHA. Afghanistan Population: Population Estimate for 2015; OCHA: Afghanistan, 2015. Available online: https://www.refworld.org/docid/55eedf694.html (accessed on 6 February 2020).
- Islamic Republic of Afghanistan. Provincial Profile: Nangarhar. Available online: https://president.gov.af/en/nangarhar/ (accessed on 16 November 2020).
- Deitchler, M.; Ballard, T.; Swindale, A.; Coates, J. Introducing a Simple Measure of Household Hunger for Cross-Cultural Use; USAID: Washington, DC, USA, 2011. [Google Scholar]
- Mollica, R.F.; Caspi-Yavin, Y.; Bollini, P.; Truong, T.; Tor, S.; Lavelle, J. The Harvard Trauma Questionnaire. Validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees. J. Nerv. Ment. Dis. 1992, 180, 111–116. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar]
- Garcia-Moreno, C.; Jansen, H.A.F.M.; Ellsberg, M.; Heise, L.; Watts, C.H. Prevalence of intimate partner violence: Findings from the WHO multi-country study on women’s health and domestic violence. Lancet 2006, 368, 1260–1269. [Google Scholar] [CrossRef]
- Muthen, B.; du Toit, S.; Spisic, D. Robust Inference Using Weighted Least Squares and Quadratic Estimating Equations in Latent Variable Modeling with Categorical and Continous Outcomes. Psychometrika 1997. Available online: https://www.statmodel.com/download/Article_075.pdf (accessed on 16 November 2020).
- Renner, L.M.; Slack, K.S. Intimate partner violence and child maltreatment: Understanding intra- and intergenerational connections. Child Abus. Negl. 2006, 30, 599–617. [Google Scholar] [CrossRef] [PubMed]
- Jewkes, R.; Corboz, J.; Gibbs, A. Violence against Afghan women by husbands, mothers-in-law and siblings-in-law/siblings: Risk markers and health consequences in an analysis of the baseline of a randomised controlled trial. PLoS ONE 2019, 14, e0211361. [Google Scholar] [CrossRef]
- Boydell, N.; Nalukenge, W.; Siu, G.; Seeley, J.; Wight, D. How Mothers in Poverty Explain Their Use of Corporal Punishment: A Qualitative Study in Kampala, Uganda. Eur. J. Dev. Res. 2017, 29, 999–1016. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C.M.; Green, A.J. Parenting stress and anger expression as predictors of child abuse potential. Child Abus. Negl. 1997, 21, 367–377. [Google Scholar] [CrossRef] [Green Version]
- Lowell, A.; Renk, K. Predictors of Child Maltreatment Potential in a National Sample of Mothers of Young Children. J. Aggress. Maltreatment Trauma 2017, 26, 335–353. [Google Scholar] [CrossRef]
- Gibbs, A.; Jewkes, R.; Willan, S.; Washington, L. Associations between poverty, mental health and substance abuse, gender power, and intimate partner violence amongst young (18–30) women and men in urban informal settlements in South Africa: A cross-sectional study and structural equation model. PLoS ONE 2018, 13, e0204956. [Google Scholar]
- Gibbs, A.; Dunkle, K.; Ramsoomar, L.; Willan, S.; Jama Shai, N.; Chatterji, S.; Naved, R.; Jewkes, R. New learnings on drivers of men’s physical and/or sexual violence against their female partners, and women’s experiences of this, and the implications for prevention interventions. Glob. Health Action 2020, 13, 1739845. [Google Scholar] [CrossRef] [Green Version]
- Pittner, K.; van Ijzendoorn, M.H.; Alink, L.R.A.; Buisman, R.S.M.; Compier-de Block, L.H.C.G.C.; van den Berg, L.J.M.; Elzinga, B.M.; Lindenberg, J.; Tollenaar, M.S.; Diego, V.P.; et al. The genetic and environmental etiology of child maltreatment in a parent-based extended family design. Dev. Psychopathol. 2019, 31, 157–172. [Google Scholar] [CrossRef] [Green Version]
- Ammerman, R.T.; Putnam, F.W.; Chard, K.M.; Stevens, J.; Van Ginkel, J.B. PTSD in Depressed Mothers in Home Visitation. Psychol. Trauma 2012, 4, 186. [Google Scholar] [CrossRef] [Green Version]
- van Ee, E.; Kleber, R.J.; Jongmans, M.J. Relational Patterns Between Caregivers With PTSD and Their Nonexposed Children: A Review. Trauma Violence Abus. 2016, 17, 186–203. [Google Scholar] [CrossRef]
- Santini, P.M.; Williams, L.C.A. A randomized controlled trial of an intervention program to Brazilian mothers who use corporal punishment. Child Abus. Negl. 2017, 71, 80–91. [Google Scholar] [CrossRef]
- Hornor, G.; Bretl, D.; Chapman, E.; Chiocca, E.; Donnell, C.; Doughty, K.; Houser, S.; Marshall, B.; Morris, K.; Quinones, S.G. Corporal Punishment: Evaluation of an Intervention by PNPs. J. Pediatric Health Care 2015, 29, 526–535. [Google Scholar] [CrossRef]
- Mastonshoeva, S.; Myrttinen, H.; Chirwa, E.; Shonasimova, S.; Gulyamova, P.; Shai, N.; Jewkes, R. Evaluation of Zindagii Shoista (Living with Dignity), an Intervention to Prevent Violence against Women in Tajikistan: Impact after 30 Months. What Works to Prevent Violence against Women and Girls. 2020. Available online: https://www.whatworks.co.za/resources/reports/item/687-evaluation-of-zindagii-shoista-living-with-dignity-an-intervention-to-prevent-violence-against-women-in-tajikistan-impact-after-30-months (accessed on 6 February 2020).


{kind=link}
| Variable | n | % (n)/Mean, SD (95% CI) | Mother Using Corporal Punishment on Their Child | ||
|---|---|---|---|---|---|
| Socioeconomic Status | No% (n)/Mean | Yes% (n)/Mean | p-Value | ||
| Age | 855 | ||||
| 18 to 24 | 11.4 (97) | 14.2 (56) | 8.9 (41) | 0.015 | |
| 25+ | 88.7 (758) | 85.8 (338) | 91.1 (420) | ||
| Level of education | |||||
| No formal education | 853 | 86.1 (734) | 84.7 (333) | 87.2 (401) | 0.303 |
| Any formal education | 14.0 (119) | 15.3 (60) | 12.8 (59) | ||
| Food insecurity > more | 854 | 5.5, 2.85 (5.27, 5.66) | 4.8 | 6.1 | <0.001 |
| Gender attitudes > more gender inequitable attitudes | 854 | 21.8, 3.15 (21.67, 22.10) | 19.1 | 20.4 | <0.001 |
| Mental health | |||||
| Posttraumatic Stress Disorder (PTSD) > more | 857 | 25.7, 8.31 (25.11, 26.23) | 7.73 | 11.4 | <0.001 |
| Depression > more | 854 | 15.7, 10.07 (14.98, 16.33) | 13.7 | 17.4 | <0.001 |
| Suicidal ideation (past 4 weeks) | 851 | ||||
| No | 93.1 (792) | 97.5 (385) | 89.3 (407) | <0.001 | |
| Yes | 6.9 (59) | 2.5 (10) | 10.8 (49) | ||
| Childhood trauma | |||||
| Childhood physical violence | 854 | ||||
| No | 93.1 (796) | 97.2 (383) | 89.8 (413) | <0.001 | |
| Yes | 6.8 (58) | 2.8 (11) | 10.2 (47) | ||
| As a child, witnessing mother being physically abused | 855 | ||||
| No | 77.3 (661) | 87.1 (343) | 69.0 (318) | <0.001 | |
| Yes | 22.7 (194) | 12.9 (51) | 31.0 (143) | ||
| Experiencing childhood emotional violence | 855 | ||||
| No | 82.7 (707) | 89.6 (353) | 76.8 (354) | <0.001 | |
| Yes | 17.3 (148) | 10.4 (41) | 23.2 (107) | ||
| Experiencing hardship as a child | 855 | ||||
| No | 60.1 (514) | 71.3 (281) | 50.5 (233) | <0.001 | |
| Yes | 39.9 (341) | 28.7 (113) | 49.5 (228) | ||
| Experiencing neglect as a child | 854 | ||||
| No | 30.2 (258) | 21.9 (86) | 37.3 (172) | <0.001 | |
| Yes | 69.8 (596) | 78.1 (307) | 62.7 (289) | ||
| Experience of trauma in adulthood | |||||
| Family violence | 793 | ||||
| None | 71.5 (567) | 79.0 (567) | 0 | <0.001 | |
| Violence from mother-in-law | 5.2 (41) | 0 | 54.7 (41) | ||
| Intimate partner violence (IPV) | 19.0 (151) | 21.0 (151) | 0 | ||
| Both IPV and violence from mother-in-law | 4.3 (34) | 0 | 45.3 (34) | ||
| War Exposure | 886 | ||||
| None | 34.2 (268) | 35.3 (251) | 23.3 (17) | 0.09 | |
| Exposure to one or two | 56.1 (440) | 55.4 (394) | 63.0 (46) | ||
| Exposure to three or more events | 9.7 (76) | 9.3 (66) | 13.7 (10) | ||
| Corporal punishment | |||||
| Partner uses corporal punishment on the child | 854 | ||||
| No | 56.3 (481) | 71.8 (282) | 43.2 (199) | <0.001 | |
| Yes | 43.7 (373) | 28.2 (111) | 56.8 (262) | ||
| Mother uses corporal punishment on the child (outcome variable) | 855 | ||||
| No | 45.1 (394) | ||||
| Yes | 53.9 (461) | ||||
| Mother Uses Corporal Punishment on the Child (n = 711) | Adj. OR | p > |t| | [95% Conf. Interval] | |
|---|---|---|---|---|
| Low | High | |||
| Socioeconomic status | ||||
| Age | ||||
| 18–24 | ref | ref | ref | ref |
| 25+ | 0.98 | 0.86 | 0.76 | 1.26 |
| Level of education | ||||
| No formal education | ref | ref | ref | ref |
| Any formal education | 0.97 | 0.812 | 0.76 | 1.24 |
| Food insecurity | ||||
| >more | 1.1 | 0.017 | 1.02 | 1.19 |
| Gender attitudes | ||||
| >more gender inequitable attitudes | 1.14 | <0.001 | 1.07 | 1.21 |
| Mental health | ||||
| Posttraumatic Stress Disorder (PTSD) | ||||
| >more | 1.04 | 0.089 | 0.10 | 1.08 |
| Depression | ||||
| >more | 0.99 | 0.661 | 0.97 | 1.02 |
| Suicidal ideation (past 4 weeks) | ||||
| No | ref | ref | ref | ref |
| Yes | 1.63 | 0.327 | 0.62 | 4.30 |
| Childhood trauma | ||||
| Childhood physical violence | ||||
| No | ref | ref | ref | ref |
| Yes | 1.34 | 0.594 | 0.46 | 3.91 |
| As a child, witnessing mother being physically abused | ||||
| No | ref | ref | ref | ref |
| Yes | 2.50 | 0.001 | 1.55 | 4.04 |
| Experiencing childhood emotional violence | ||||
| No | ref | ref | ref | ref |
| Yes | 1.076 | 0.807 | 0.60 | 1.95 |
| Experiencing hardship as a child | ||||
| No | ref | ref | ref | ref |
| Yes | 1.81 | 0.003 | 1.23 | 2.67 |
| Experiencing neglect as a child | ||||
| No | ref | ref | ref | ref |
| Yes | 0.49 | 0.001 | 0.33 | 0.73 |
| Experience of trauma in adulthood | ||||
| Family violence | ||||
| None | ref | ref | ref | ref |
| Violence from mother-in-law | 1.78 | 0.158 | 0.80 | 3.95 |
| Intimate partner violence (IPV) | 3.30 | <0.001 | 1.90 | 5.73 |
| Both IPV and violence from mother-in-law | 1.66 | 0.368 | 0.55 | 5.05 |
| War exposure | ||||
| None | Ref | Ref | Ref | ref |
| Exposure to one or two event(s) | 1.24 | 0.288 | 0.84 | 1.83 |
| Exposure to three or more events | 1.02 | 0.951 | 0.47 | 2.23 |
| Corporal punishment | ||||
| Partner uses corporal punishment on the child | ||||
| No | ref | ref | ref | ref |
| Yes | 3.09 | <0.001 | 2.15 | 4.45 |
| Pathway | Unstandardised Coef. (95% CI) | Standardised Coef. (95%CI) | p-Value |
|---|---|---|---|
| Mental Health -> Corporal Punishment | 0.30 (0.15–0.45) | 0.16 (0.08–0.23) | <0.001 |
| Family Violence -> Corporal Punishment | 0.27 (0.14–0.40) | 0.23 (0.12–0.35) | <0.001 |
| Gender inequitable attitudes -> Corporal Punishment | 0.09 (0.06–0.12) | 0.22 (0.15–0.29) | <0.001 |
| Partner using Corporal Punishment on the child -> Corporal Punishment | 0.35 (0.25–0.45) | 0.32 (0.24–0.41) | <0.001 |
| Family Violence -> Partner using Corporal Punishment on the child | 0.55 (0.43–0.66) | 0.51 (0.44–0.59) | <0.001 |
| Childhood Trauma -> Mental Health | 0.06 (0.04–0.07) | 0.28 (0.24–0.33) | <0.001 |
| War Exposure -> Mental Health | 0.10 (0.05–0.14) | 0.15 (0.10–0.20) | <0.001 |
| Food Insecurity -> Mental Health | 0.10 (0.07–0.13) | 0.42 (0.36–0.49) | <0.001 |
| Family Violence -> Mental Health | 0.12 (0.07–0.18) | 0.20 (0.13–0.27) | <0.001 |
| Childhood Trauma -> Family Violence | 0.05 (0.03–0.07) | 0.16 (0.08–0.23) | <0.001 |
| Food Insecurity -> Family Violence | 0.11 (0.08–0.14) | 0.28 (0.20–0.36) | <0.001 |
| War Exposure -> Family Violence | 0.21 (0.12–0.30) | 0.21 (0.12–0.29) | <0.001 |
| Food Insecurity -> Gender inequitable attitudes | 0.16 (0.08–0.24) | 0.15 (0.08–0.22) | <0.001 |
| Covariances | |||
| Family violence with suicidal thoughts | 0.62 (0.46–0.78) | 0.62 (0.46–0.78) | <0.001 |
| Childhood trauma with Gender inequitable attitudes | −1.36 (−2.04–−0.68) | −0.13 (−0.19–−0.06) | <0.001 |
| Childhood trauma with Food insecurity | 2.11 (1.44–2.78) | 0.21 (0.15–0.27) | <0.001 |
| Childhood trauma with war exposure | 0.29 (0.06–0.52) | 0.08 (0.02–0.14) | 0.015 |
| War exposure with Food insecurity | 0.13 (−0.08–0.34) | 0.04 (−0.03–0.11) | 0.233 |
| RMSEA = 0.047, CFI = 0.97, TLI = 0.95 | |||
| Estimator: Weighted Least Squares Mean and Variance Estimators (WLSMV) with theta Parameterization | |||
| Link function: Probit | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndungu, J.; Jewkes, R.; Ngcobo-Sithole, M.; Chirwa, E.; Gibbs, A. Afghan Women’s Use of Violence against Their Children and Associations with IPV, Adverse Childhood Experiences and Poverty: A Cross-Sectional and Structural Equation Modelling Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7923. https://doi.org/10.3390/ijerph18157923
Ndungu J, Jewkes R, Ngcobo-Sithole M, Chirwa E, Gibbs A. Afghan Women’s Use of Violence against Their Children and Associations with IPV, Adverse Childhood Experiences and Poverty: A Cross-Sectional and Structural Equation Modelling Analysis. International Journal of Environmental Research and Public Health. 2021; 18(15):7923. https://doi.org/10.3390/ijerph18157923
Chicago/Turabian StyleNdungu, Jane, Rachel Jewkes, Magnolia Ngcobo-Sithole, Esnat Chirwa, and Andrew Gibbs. 2021. "Afghan Women’s Use of Violence against Their Children and Associations with IPV, Adverse Childhood Experiences and Poverty: A Cross-Sectional and Structural Equation Modelling Analysis" International Journal of Environmental Research and Public Health 18, no. 15: 7923. https://doi.org/10.3390/ijerph18157923