
Musculoskeletal Disorders, Pain Medication, and in-Hospital Mortality among Patients with COVID-19 in South Korea: A Population-Based Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Statement
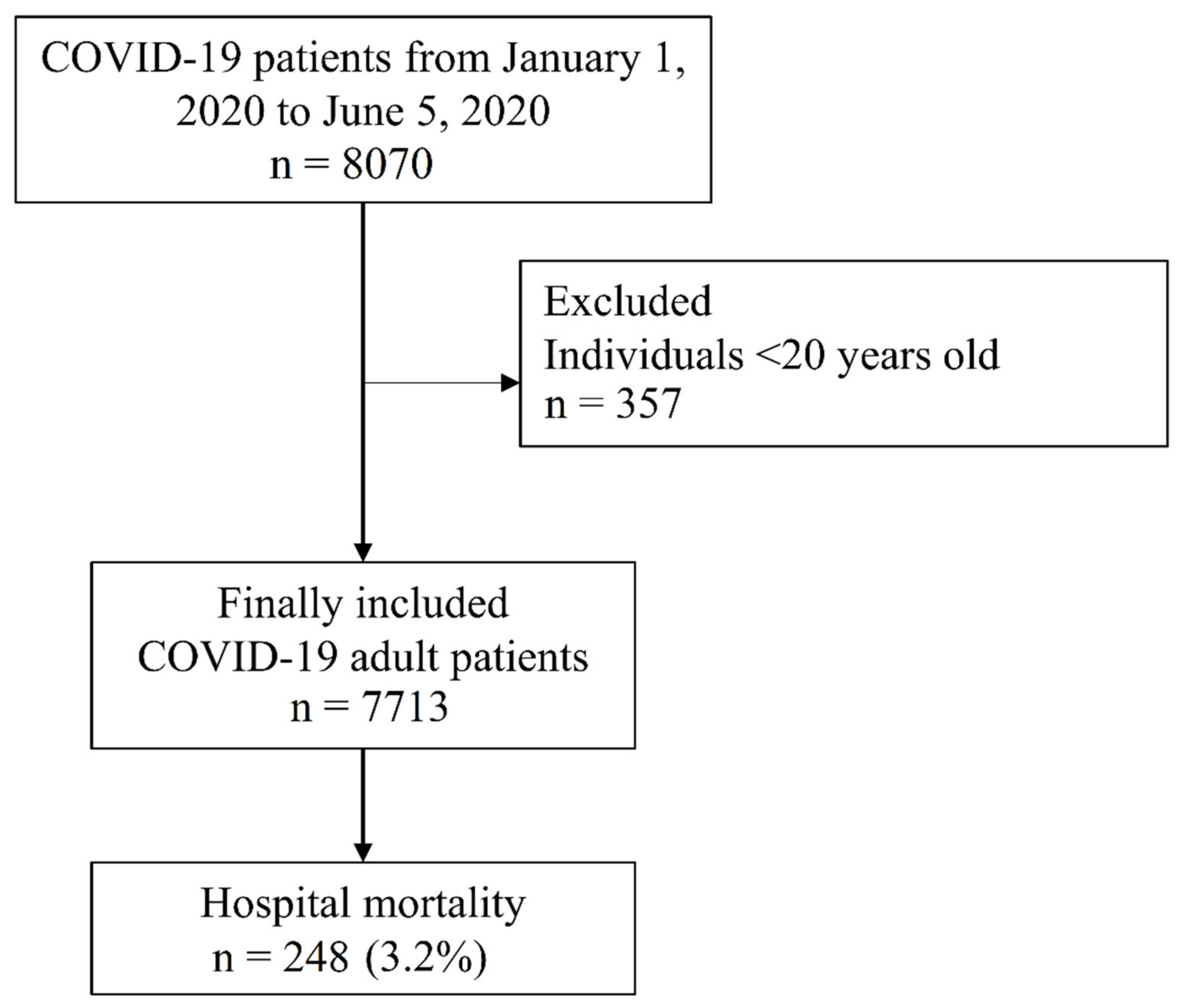
2.2. NHIS-COVID-19 Cohort Database and Study Population
2.3. Exposure Variables: Musculoskeletal Disease and Pain Medication
2.4. Endpoints
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. In-Hospital Mortality among Patients with COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.D.; Schuchat, A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Coronavirus Research Center. Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Global Map of Cases and Deaths by Country/Region/Sovereignty. 2020. Available online: https://coronavirus.jhu.edu/map.html (accessed on 6 April 2021).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford–AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Haberman, R.; Axelrad, J.; Chen, A.; Castillo, R.; Yan, D.; Izmirly, P.; Neimann, A.; Adhikari, S.; Hudesman, D.; Scher, J.U. Covid-19 in Immune-Mediated Inflammatory Diseases—Case Series from New York. N. Engl. J. Med. 2020, 383, 85–88. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manuel, O.; Estabrook, M.; The American Society of Transplantation Infectious Diseases Community of Practice. RNA respiratory viral infections in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waghmare, A.; Englund, J.A.; Boeckh, M. How I treat respiratory viral infections in the setting of intensive chemotherapy or hematopoietic cell transplantation. Blood 2016, 127, 2682–2692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, M.; Babik, J.M. COVID-19 in Immunocompromised Hosts: What We Know So Far. Clin. Infect. Dis. 2021, 72, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Generaal, E.; Vogelzangs, N.; Macfarlane, G.; Geenen, R.; Smit, J.H.; Dekker, J.; Penninx, B.W. Basal inflammation and innate immune response in chronic multisite musculoskeletal pain. Pain 2014, 155, 1605–1612. [Google Scholar] [CrossRef]
- Wolfe, F.; Caplan, L.; Michaud, K. Treatment for rheumatoid arthritis and the risk of hospitalization for pneumonia: Associations with prednisone, disease-modifying antirheumatic drugs, and anti-tumor necrosis factor therapy. Arthritis Rheum. 2006, 54, 628–634. [Google Scholar] [CrossRef]
- Flint, T.R.; Janowitz, T.; Connell, C.M.; Roberts, E.W.; Denton, A.; Coll, A.P.; Jodrell, D.I.; Fearon, D.T. Tumor-Induced IL-6 Reprograms Host Metabolism to Suppress Anti-tumor Immunity. Cell Metab. 2016, 24, 672–684. [Google Scholar] [CrossRef] [PubMed]
- Diasso, P.D.K.; Birke, H.; Nielsen, S.D.; Main, K.M.; Højsted, J.; Sjøgren, P.; Kurita, G.P. The effects of long-term opioid treatment on the immune system in chronic non-cancer pain patients: A systematic review. Eur. J. Pain 2019, 24, 481–496. [Google Scholar] [CrossRef]
- Oh, T.K.; Jeon, Y.-T.; Choi, J.W. Trends in chronic opioid use and association with five-year survival in South Korea: A population-based cohort study. Br. J. Anaesth. 2019, 123, 655–663. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.-A. Trends in long-term glucocorticoid use and risk of 5-year mortality: A historical cohort study in South Korea. Endocrine 2020, 69, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.R.; Kuo, Y.-F.; Baillargeon, J.; Raji, M.A. The impact of long-term opioid use on the risk and severity of COVID-19. J. Opioid Manag. 2020, 16, 401–404. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, J.; Lawlor, P.; Vigano, A.; Dorgan, M.; Bruera, E. Equianalgesic Dose Ratios for Opioids: A Critical Review and Proposals for Long-Term Dosing. J. Pain Symptom Manag. 2001, 22, 672–687. [Google Scholar] [CrossRef]
- Salas, M.; Hotman, A.; Stricker, B.H. Confounding by Indication: An Example of Variation in the Use of Epidemiologic Terminology. Am. J. Epidemiol. 1999, 149, 981–983. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S.; Mansournia, M.A.; Altman, D.G. Sparse data bias: A problem hiding in plain sight. BMJ 2016, 352, i1981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, W.A.; Chung, C.P.; Murray, K.T.; Hall, K.; Stein, C.M. Prescription of Long-Acting Opioids and Mortality in Patients with Chronic Noncancer Pain. JAMA 2016, 315, 2415–2423. [Google Scholar] [CrossRef] [Green Version]
- Gomes, T.; Tadrous, M.; Mamdani, M.M.; Paterson, J.M.; Juurlink, D.N. The Burden of Opioid-Related Mortality in the United States. JAMA Netw. Open 2018, 1, e180217. [Google Scholar] [CrossRef]
- Pierce, M.; Bird, S.M.; Hickman, M.; Millar, T. National record linkage study of mortality for a large cohort of opioid users ascertained by drug treatment or criminal justice sources in England, 2005–2009. Drug Alcohol Depend. 2015, 146, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Schwetz, T.A.; Calder, T.; Rosenthal, E.; Kattakuzhy, S.; Fauci, A.S. Opioids and Infectious Diseases: A Converging Public Health Crisis. J. Infect. Dis. 2019, 220, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Fine, D.R.; Li, L.; Kimmel, S.D.; Ngo, L.H.; Suzuki, J.; Price, C.N.; Ronan, M.V.; Herzig, S.J. Disparities in United States hospitalizations for serious infections in patients with and without opioid use disorder: A nationwide observational study. PLoS Med. 2020, 17, e1003247. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, D.F.; Gordon, K.S.; Barry, D.T.; Becker, W.C.; Crystal, S.; Edelman, E.J.; Gaither, J.; Gordon, A.J.; Goulet, J.; Kerns, R.D.; et al. Long-term Prescription of Opioids and/or Benzodiazepines and Mortality Among HIV-Infected and Uninfected Patients. J. Acquir. Immune Defic. Syndr. 2015, 69, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Schimmel, J.; Manini, A.F. Opioid Use Disorder and COVID-19: Biological Plausibility for Worsened Outcomes. Subst. Use Misuse 2020, 55, 1900–1901. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.Q.; Kaelber, D.C.; Xu, R.; Volkow, N.D. COVID-19 risk and outcomes in patients with substance use disorders: Analyses from electronic health records in the United States. Mol. Psychiatry 2021, 26, 30–39. [Google Scholar] [CrossRef]
- MacKinnon, L.; Socías, M.E.; Bardwell, G. COVID-19 and overdose prevention: Challenges and opportunities for clinical practice in housing settings. J. Subst. Abus Treat. 2020, 119, 108153. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.G.; Ramage, M.; Fagan, E.B. A Primary Care Response to COVID-19 for Patients with an Opioid Use Disorder. J. Rural. Heal. 2021, 37, 169–171. [Google Scholar] [CrossRef] [Green Version]
- Fredi, M.; Cavazzana, I.; Moschetti, L.; Andreoli, L.; Franceschini, F.; Airò, P.; Bazzani, C.; Crisafulli, F.; Filippini, M.; Frassi, M.; et al. COVID-19 in patients with rheumatic diseases in northern Italy: A single-centre observational and case–control study. Lancet Rheumatol. 2020, 2, e549–e556. [Google Scholar] [CrossRef]
- Haberman, R.H.; Castillo, R.; Chen, A.; Yan, D.; Ramirez, D.; Sekar, V.; Lesser, R.; Solomon, G.; Neimann, A.L.; Blank, R.B.; et al. COVID-19 in Patients with Inflammatory Arthritis: A Prospective Study on the Effects of Comorbidities and Disease-Modifying Antirheumatic Drugs on Clinical Outcomes. Arthritis Rheumatol. 2020, 72, 1981–1989. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; Woolf, A.D.; Dreinhöfer, K.; Homb, N.; Hoy, D.G.; Kopansky-Giles, D.; Åkesson, K.; March, L. Reducing the global burden of musculoskeletal conditions. Bull. World Heal. Organ. 2018, 96, 366–368. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Number (%) | Mean (SD) |
|---|---|---|
| Sex, male | 3048 (39.5%) | |
| Age | ||
| 20–29 | 2057 (26.7%) | |
| 30–39 | 832 (10.8%) | |
| 40–49 | 1036 (13.4%) | |
| 50–59 | 1567 (20.3%) | |
| 60–69 | 1199 (15.5%) | |
| 70–79 | 617 (8.0%) | |
| ≥80 | 405 (5.3%) | |
| Income in qurtile | ||
| Q1 (Lowest) | 2439 (31.6%) | |
| Q2 | 1445 (18.7%) | |
| Q3 | 1577 (20.4%) | |
| Q4 (Highest) | 2135 (27.7%) | |
| unknown | 117 (1.5%) | |
| Underlying disability | ||
| Mild degree | 318 (4.1%) | |
| Moderate to severe degree | 293 (3.8%) | |
| Residence | ||
| Seoul | 510 (6.6%) | |
| Gyeonggi-do | 431 (5.6%) | |
| Daegu | 5036 (65.3%) | |
| Gyeongsangbukdo | 933 (12.1%) | |
| Other area | 803 (10.4%) | |
| Charlson comorbidity index | 2.7 (2.7) | |
| Any cancer | 602 (7.8%) | |
| 70 (0.9%) | ||
| Metastatic solid tumour | 3641 (47.2%) | |
| Neck pain | 1971 (25.6%) | |
| Lower back pain | 4836 (62.7%) | |
| Rheumatoid arthritis | 739 (9.6%) | |
| Other musculoskeletal disease | 4908 (63.6%) | |
| Major depressive disorder | 1450 (18.8) | |
| Pain medication | ||
| Paracetamol | 58 (0.8%) | |
| Gabapentin or pregabalin | 148 (1.9%) | |
| Glucocorticoid | 63 (0.8%) | |
| NSAIDs | 1 (0.0%) | |
| Strong opoioid | 9 (0.1%) | |
| Weak opioid | 240 (3.1%) | |
| Benzodiazepine | 259 (3.4%) |
| Variable | Univariate Analysis | p-Value |
|---|---|---|
| OR (95% CI) | ||
| Age, 10 year increase | 3.56 (3.13, 4.05) | <0.001 |
| Sex, male (vs. female) | 1.90 (1.47, 2.45) | <0.001 |
| Annual income level in 2020 | ||
| Q1 (Lowest) | 1 | |
| Q2 | 0.63 (0.42, 0.95) | 0.026 |
| Q3 | 0.87 (0.61, 1.25) | 0.446 |
| Q4 (Highest) | 1.08 (0.79, 1.47) | 0.636 |
| Unknown | 0.73 (0.23, 2.34) | 0.595 |
| Residence at 2010 | ||
| Seoul | 1 | |
| Gyeonggi-do | 5.19 (1.73, 15.56) | 0.003 |
| Daegu | 3.94 (1.45, 10.67) | 0.007 |
| Gyeongsangbukdo | 7.92 (2.86, 21.99) | <0.001 |
| Other area | 3.23 (1.10, 9.51) | 0.033 |
| Underlying disability | ||
| Mild degree (vs. no disability) | 5.05 (3.46, 7.37) | <0.001 |
| Moderate to severe (vs. no disability) | 5.72 (3.93, 8.33) | <0.001 |
| Charlson comorbidity index, 1 point increase | 1.40 (1.35, 1.45) | <0.001 |
| Any cancer | 3.70 (2.71, 5.04) | <0.001 |
| Metastatic solid tumour | 4.57 (2.24, 9.31) | <0.001 |
| Major depressive disorder | 4.18 (3.23, 5.40) | <0.001 |
| Osteoarthritis | 3.26 (2.45, 4.35) | <0.001 |
| Neck pain | 0.99 (0.74, 1.33) | 0.956 |
| Lower back pain | 1.94 (1.44, 2.61) | <0.001 |
| Rheumatoid arthritis | 1.69 (1.18, 2.42) | 0.004 |
| Other musculoskeletal disease | 1.63 (1.23, 2.18) | <0.001 |
| Pain medication | ||
| Paracetamol | 0.99 (0.35, 2.52) | 0.921 |
| Gabapentin or pregabalin | 4.42 (2.65, 7.35) | <0.001 |
| Glucocorticoid | 2.63 (1.04, 6.61) | 0.040 |
| NSAIDs | 0.00 (0.00-) | 0.978 |
| Strong opoioid | 38.38 (10.24, 143.81) | <0.001 |
| Weak opioid | 3.06 (1.92, 4.88) | <0.001 |
| Benzodiazepine | 3.64 (2.37, 5.57) | <0.001 |
| Variable | Multivariate Model | p-Value |
|---|---|---|
| OR (95% CI) | ||
| Age, 10 year increase | 3.21 (2.75, 3.75) | <0.001 |
| Sex, male (vs. female) | 2.13 (1.57, 2.88) | <0.001 |
| Annual income level in 2020 | ||
| Q1 (Lowest) | 1 | |
| Q2 | 1.11 (0.69, 1.79) | 0.666 |
| Q3 | 1.01 (0.67, 1.54) | 0.949 |
| Q4 (Highest) | 0.86 (0.59, 1.24) | 0.411 |
| Unknown | 0.82 (0.22, 3.10) | 0.773 |
| Residence at 2010 | ||
| Seoul | 1 | |
| Gyeonggi-do | 2.82 (0.83, 9.54) | 0.096 |
| Daegu | 1.76 (0.59, 5.20) | 0.308 |
| Gyeongsangbookdo | 2.08 (0.68, 6.37) | 0.199 |
| Other area | 2.34 (0.72, 7.61) | 0.157 |
| Underlying disability | ||
| Mild degree (vs. no disability) | 0.91 (0.59, 1.40) | 0.653 |
| Moderate to severe (vs. no disability) | 2.88 (1.81, 4.60) | <0.001 |
| Charlson comorbidity index, 1 point increase | 1.19 (1.12, 1.26) | <0.001 |
| Any cancer | 1.00 (0.66, 1.52) | 0.986 |
| Metastatic solid tumour | 0.79 (0.27, 2.31) | 0.665 |
| Major depressive disorder | 1.28 (0.93, 1.76) | 0.125 |
| Osteoarthritis | 1.11 (0.75, 1.65) | 0.589 |
| Neck pain | 0.74 (0.52, 1.05) | 0.095 |
| Lower back pain | 0.73 (0.49, 1.10) | 0.133 |
| Rheumatoid arthritis | 0.78 (0.50, 1.23) | 0.291 |
| Other musculoskeletal disease | 0.73 (0.49, 1.09) | 0.129 |
| Pain medication | ||
| Paracetamol | 0.98 (0.37, 2.62) | 0.973 |
| Gabapentin or pregabalin | 0.77 (0.41, 1.45) | 0.424 |
| Glucocorticoid | 1.26 (0.43, 3.63) | 0.673 |
| NSAIDs | 0.00 (0.00-) | 0.979 |
| Strong opoioid | 12.73 (2.44, 16.64) | 0.002 |
| Weak opioid | 0.96 (0.55, 1.67) | 0.876 |
| Benzodiazepine | 0.77 (0.46, 1.29) | 0.324 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.-K.; Song, I.-A.; Lee, J.; Eom, W.; Jeon, Y.-T. Musculoskeletal Disorders, Pain Medication, and in-Hospital Mortality among Patients with COVID-19 in South Korea: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 6804. https://doi.org/10.3390/ijerph18136804
Oh T-K, Song I-A, Lee J, Eom W, Jeon Y-T. Musculoskeletal Disorders, Pain Medication, and in-Hospital Mortality among Patients with COVID-19 in South Korea: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(13):6804. https://doi.org/10.3390/ijerph18136804
Chicago/Turabian StyleOh, Tak-Kyu, In-Ae Song, Joon Lee, Woosik Eom, and Young-Tae Jeon. 2021. "Musculoskeletal Disorders, Pain Medication, and in-Hospital Mortality among Patients with COVID-19 in South Korea: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 13: 6804. https://doi.org/10.3390/ijerph18136804