
Association between Blood Mercury Levels and Non-Alcoholic Fatty Liver Disease in Non-Obese Populations: The Korean National Environmental Health Survey (KoNEHS) 2012–2014

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
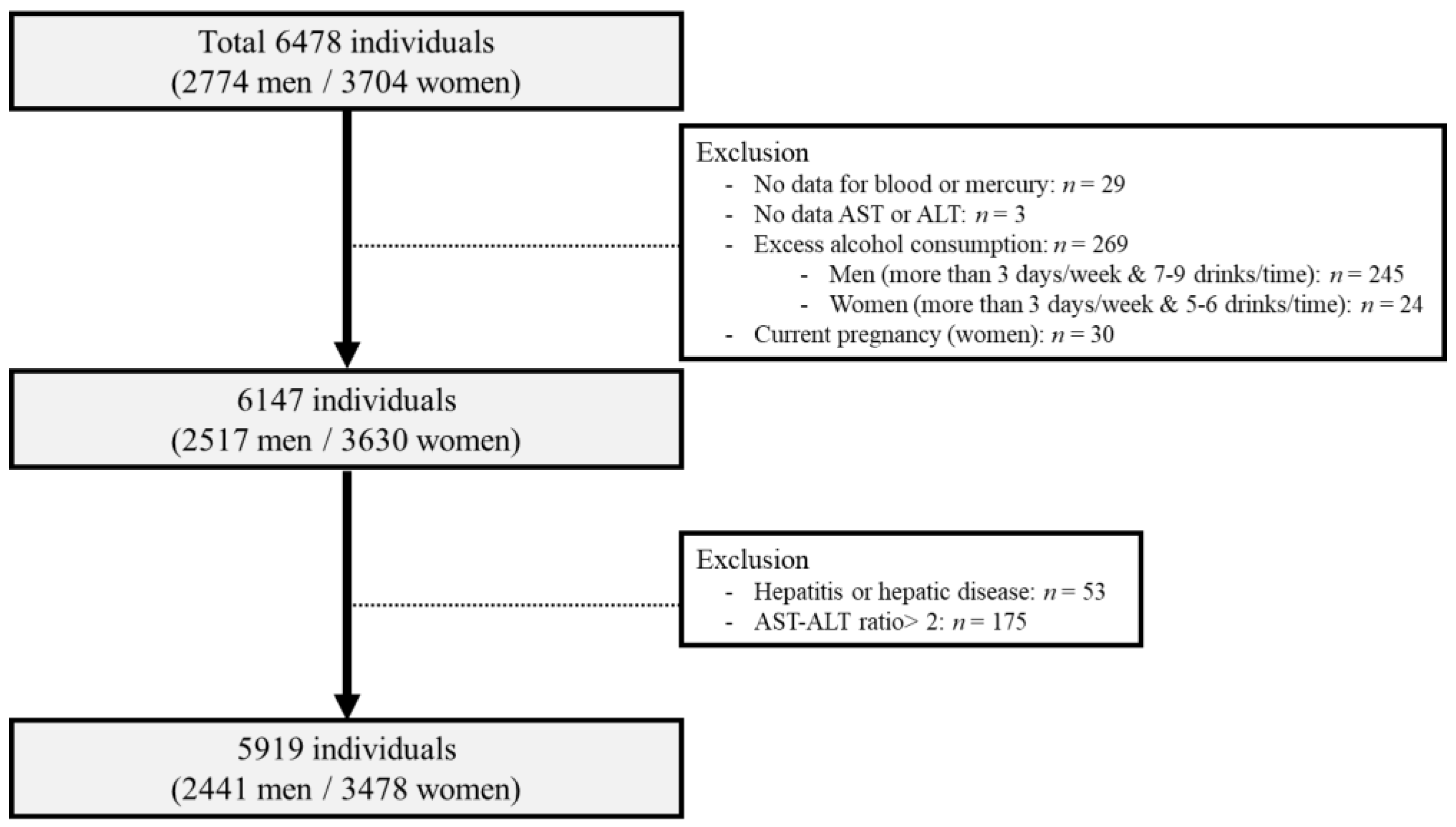
2.1. Study Population
2.2. Questionnaire and Definition of Anthrophometric and Biochemical Parameters
2.3. NAFLD Assessment
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Mercury Concentration in Blood and Urine
3.3. Prevalence of NAFLD
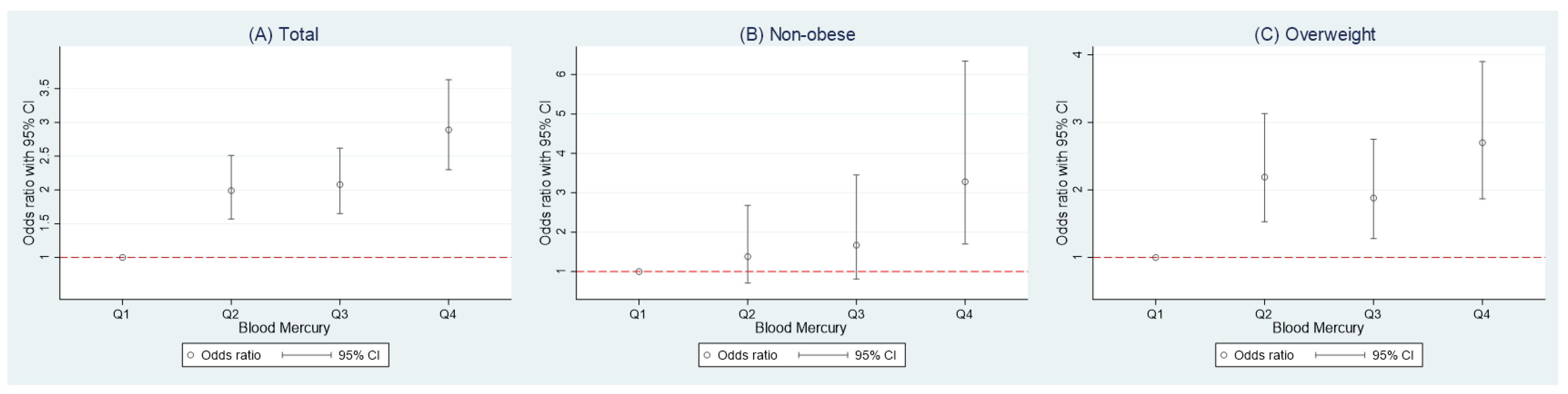
3.4. Association between Mercury and NAFLD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Mercury. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp46.pdf (accessed on 11 November 2020).
- Agency for Toxic Substances and Disease Registry (ATSDR). Substance Priority List. Available online: https://www.atsdr.cdc.gov/spl/index.html (accessed on 11 November 2020).
- Bjorkman, L.; Lundekvam, B.F.; Laegreid, T.; Bertelsen, B.I.; Morild, I.; Lilleng, P.; Lind, B.; Palm, B.; Vahter, M. Mercury in human brain, blood, muscle and toenails in relation to exposure: An autopsy study. Environ. Health 2007, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Yaginuma-Sakurai, K.; Murata, K.; Iwai-Shimada, M.; Nakai, K.; Kurokawa, N.; Tatsuta, N.; Satoh, H. Hair-to-blood ratio and biological half-life of mercury: Experimental study of methylmercury exposure through fish consumption in humans. J. Toxicol. Sci. 2012, 37, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Dart, R.C. (Ed.) Medical Toxicology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004; pp. 1437–1448. [Google Scholar]
- Kim, S.A.; Kwon, Y.; Kim, S.; Joung, H. Assessment of Dietary Mercury Intake and Blood Mercury Levels in the Korean Population: Results from the Korean National Environmental Health Survey 2012–2014. Int. J. Environ. Res. Public Health 2016, 13, 877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Lee, B.K. Strong positive associations between seafood, vegetables, and alcohol with blood mercury and urinary arsenic levels in the Korean adult population. Arch. Environ. Contam. Toxicol. 2013, 64, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Kaus, S.; Krause, C.; Lepom, P.; Schulz, C.; Seiwert, M.; Seifert, B. German Environmental Survey 1998 (GerES III): Environmental pollutants in blood of the German population. Int. J. Hyg. Environ. Health 2002, 205, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, K.L.; Mortensen, M.E.; Jones, R.L.; Caudill, S.P.; Osterloh, J.D. Total blood mercury concentrations in the U.S. population: 1999–2006. Int. J. Hyg. Environ. Health 2009, 212, 588–598. [Google Scholar] [CrossRef]
- Apaydin, F.G.; Bas, H.; Kalender, S.; Kalender, Y. Subacute effects of low dose lead nitrate and mercury chloride exposure on kidney of rats. Environ. Toxicol. Pharmacol. 2016, 41, 219–224. [Google Scholar] [CrossRef]
- Chen, C.; Qu, L.; Li, B.; Xing, L.; Jia, G.; Wang, T.; Gao, Y.; Zhang, P.; Li, M.; Chen, W.; et al. Increased oxidative DNA damage, as assessed by urinary 8-hydroxy-2’-deoxyguanosine concentrations, and serum redox status in persons exposed to mercury. Clin. Chem. 2005, 51, 759–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinkov, A.A.; Ajsuvakova, O.P.; Skalnaya, M.G.; Popova, E.V.; Sinitskii, A.I.; Nemereshina, O.N.; Gatiatulina, E.R.; Nikonorov, A.A.; Skalny, A.V. Mercury and metabolic syndrome: A review of experimental and clinical observations. Biometals 2015, 28, 231–254. [Google Scholar] [CrossRef]
- Lebeaupin, C.; Vallee, D.; Hazari, Y.; Hetz, C.; Chevet, E.; Bailly-Maitre, B. Endoplasmic reticulum stress signalling and the pathogenesis of non-alcoholic fatty liver disease. J. Hepatol. 2018, 69, 927–947. [Google Scholar] [CrossRef]
- Chen, R.; Xu, Y.; Xu, C.; Shu, Y.; Ma, S.; Lu, C.; Mo, X. Associations between mercury exposure and the risk of nonalcoholic fatty liver disease (NAFLD) in US adolescents. Environ. Sci. Pollut. Res. Int. 2019, 26, 31384–31391. [Google Scholar] [CrossRef]
- Cave, M.; Appana, S.; Patel, M.; Falkner, K.C.; McClain, C.J.; Brock, G. Polychlorinated biphenyls, lead, and mercury are associated with liver disease in American adults: NHANES 2003–2004. Environ. Health Perspect 2010, 118, 1735–1742. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.M.; Moon, J.S.; Yoon, J.S.; Won, K.C.; Lee, H.W. The sex-specific effects of blood lead, mercury, and cadmium levels on hepatic steatosis and fibrosis: Korean nationwide cross-sectional study. J. Trace Elem. Med. Biol. 2020, 62, 126601. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Priyadarshi, R.N.; Anand, U. Non-alcoholic Fatty Liver Disease: Growing Burden, Adverse Outcomes and Associations. J. Clin. Transl. Hepatol. 2020, 8, 76–86. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Sarwar, R.; Pierce, N.; Koppe, S. Obesity and nonalcoholic fatty liver disease: Current perspectives. Diabetes Metab. Syndr. Obes. 2018, 11, 533–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, K.; Das, K.; Mukherjee, P.S.; Ghosh, A.; Ghosh, S.; Mridha, A.R.; Dhibar, T.; Bhattacharya, B.; Bhattacharya, D.; Manna, B.; et al. Nonobese population in a developing country has a high prevalence of nonalcoholic fatty liver and significant liver disease. Hepatology 2010, 51, 1593–1602. [Google Scholar] [CrossRef]
- Cho, H.C. Prevalence and Factors Associated with Nonalcoholic Fatty Liver Disease in a Nonobese Korean Population. Gut Liver 2016, 10, 117–125. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.J.; Lee, K.E.; Kim, D.J.; Kim, S.K.; Ahn, C.W.; Lim, S.K.; Kim, K.R.; Lee, H.C.; Huh, K.B.; et al. Metabolic significance of nonalcoholic fatty liver disease in nonobese, nondiabetic adults. Arch. Intern. Med. 2004, 164, 2169–2175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, A.; Eder, S.K.; Felder, T.K.; Kedenko, L.; Paulweber, B.; Stadlmayr, A.; Huber-Schonauer, U.; Niederseer, D.; Stickel, F.; Auer, S.; et al. Clinical and Metabolic Characterization of Lean Caucasian Subjects With Non-alcoholic Fatty Liver. Am. J. Gastroenterol. 2017, 112, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.N.; Park, S.J.; Choi, B.; Joo, N.S. Blood Mercury and Insulin Resistance in Nondiabetic Koreans (KNHANES 2008–2010). Yonsei Med. J. 2015, 56, 944–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, T.G.; Clarkson, T.W.; Dhahir, P.H. The relationship between blood levels and dose of methylmercury in man. Arch. Environ. Health 1980, 35, 28–36. [Google Scholar] [CrossRef]
- Lee, S.; Yoon, J.H.; Won, J.U.; Lee, W.; Lee, J.H.; Seok, H.; Kim, Y.K.; Kim, C.N.; Roh, J. The Association Between Blood Mercury Levels and Risk for Overweight in a General Adult Population: Results from the Korean National Health and Nutrition Examination Survey. Biol. Trace Elem. Res. 2016, 171, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Ha, K.H.; He, K.; Kim, D.J. Association between Blood Mercury Level and Visceral Adiposity in Adults. Diabetes Metab J. 2017, 41, 113–120. [Google Scholar] [CrossRef]
- Vahter, M.E.; Mottet, N.K.; Friberg, L.T.; Lind, S.B.; Charleston, J.S.; Burbacher, T.M. Demethylation of methyl mercury in different brain sites of Macaca fascicularis monkeys during long-term subclinical methyl mercury exposure. Toxicol. Appl. Pharmacol. 1995, 134, 273–284. [Google Scholar] [CrossRef]
- Yamamoto, M.; Yanagisawa, R.; Motomura, E.; Nakamura, M.; Sakamoto, M.; Takeya, M.; Eto, K. Increased methylmercury toxicity related to obesity in diabetic KK-Ay mice. J. Appl. Toxicol. 2014, 34, 914–923. [Google Scholar] [CrossRef]
- Lee, B.K.; Kim, Y. Blood cadmium, mercury, and lead and metabolic syndrome in South Korea: 2005–2010 Korean National Health and Nutrition Examination Survey. Am. J. Ind. Med. 2013, 56, 682–692. [Google Scholar] [CrossRef]
- Rothenberg, S.E.; Korrick, S.A.; Fayad, R. The influence of obesity on blood mercury levels for U.S. non-pregnant adults and children: NHANES 2007–2010. Environ. Res. 2015, 138, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzunhisarcikli, M.; Aslanturk, A.; Kalender, S.; Apaydin, F.G.; Bas, H. Mercuric chloride induced hepatotoxic and hematologic changes in rats: The protective effects of sodium selenite and vitamin E. Toxicol. Ind. Health 2016, 32, 1651–1662. [Google Scholar] [CrossRef] [PubMed]
- Grotto, D.; Valentini, J.; Fillion, M.; Passos, C.J.; Garcia, S.C.; Mergler, D.; Barbosa, F., Jr. Mercury exposure and oxidative stress in communities of the Brazilian Amazon. Sci. Total Environ. 2010, 408, 806–811. [Google Scholar] [CrossRef]
- Paschos, P.; Paletas, K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia 2009, 13, 9–19. [Google Scholar] [PubMed]
- Chen, C.H.; Huang, M.H.; Yang, J.C.; Nien, C.K.; Yang, C.C.; Yeh, Y.H.; Yueh, S.K. Prevalence and risk factors of nonalcoholic fatty liver disease in an adult population of Taiwan: Metabolic significance of nonalcoholic fatty liver disease in nonobese adults. J. Clin. Gastroenterol. 2006, 40, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.M.; Brancati, F.L.; Diehl, A.M. The prevalence and etiology of elevated aminotransferase levels in the United States. Am. J. Gastroenterol. 2003, 98, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kim, Y.; Sim, C.S.; Ham, J.O.; Kim, N.S.; Lee, B.K. Associations between blood mercury levels and subclinical changes in liver enzymes among South Korean general adults: Analysis of 2008–2012 Korean national health and nutrition examination survey data. Environ. Res. 2014, 130, 14–19. [Google Scholar] [CrossRef]
- Choi, J.; Bae, S.; Lim, H.; Lim, J.-A.; Lee, Y.-H.; Ha, M.; Kwon, H.-J. Mercury Exposure in Association With Decrease of Liver Function in Adults: A Longitudinal Study. J. Prev. Med. Public Health 2017, 50, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, Y.; Park, J.; Youn, K. Association between urinary phthalate metabolites and obesity in adult Korean population: Korean National Environmental Health Survey (KoNEHS), 2012–2014. Ann. Occup. Environ. Med. 2019, 31, e23. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 5919) | Non-Obese (n = 3614) | Overweight (n = 2305) | p-Value | |
|---|---|---|---|---|
| Gender, n (% men) | 2441 (41.24) | 1409 (38.99) | 1032 (44.77) | <0.001 |
| Age (years) | 51.37 ± 0.19 | 49.89 ± 0.25 | 53.70 ± 0.30 | <0.001 |
| Drinking Status, n (%) | 0.151 | |||
| Never | 2121 (35.83) | 1304 (36.08) | 817 (35.44) | |
| Former | 315 (5.32) | 176 (4.87) | 139 (6.03) | |
| Current | 3483 (58.84) | 2134 (59.05) | 1349 (58.52) | |
| Smoking Status, n (%) | <0.001 | |||
| Never | 4005 (67.66) | 2510 (69.45) | 1495 (64.86) | |
| Former | 910 (15.37) | 508 (14.06) | 402 (17.44) | |
| Current | 1004 (16.96) | 596 (16.49) | 408 (17.70) | |
| Physical activity, n (%) | 0.596 | |||
| No | 3772 (63.73) | 2320 (64.19) | 1452 (62.99) | |
| Moderate | 1169 (19.75) | 709 (19.62) | 460 (19.96) | |
| Vigorous | 978 (16.52) | 585 (16.19) | 393 (17.05) | |
| Monthly household income, n (%) | <0.001 | |||
| <Low | 1632 (27.57) | 901 (24.93) | 731 (31.71) | |
| Low-Mid | 2722 (45.99) | 1716 (47.48) | 1006 (43.64) | |
| Mid-High | 1512 (25.54) | 964 (26.67) | 548 (23.77) | |
| >High | 53 (0.90) | 33 (0.91) | 20 (0.87) | |
| Education, n (%) | <0.001 | |||
| <High school | 2115 (35.95) | 1100 (30.87) | 1006 (43.93) | |
| High school | 2025 (34.42) | 1290 (35.90) | 735 (32.10) | |
| College and more | 1743 (29.63) | 1194 (33.23) | 549 (23.97) | |
| Marital status, n (%) | <0.001 | |||
| Single | 610 (10.31) | 441 (12.20) | 169 (7.33) | |
| Married | 4675 (78.98) | 2839 (78.56) | 1836 (79.65) | |
| Divorced | 634 (10.71) | 334 (9.24) | 300 (10.71) | |
| AST | 24.71 ± 0.15 | 23.74 ± 0.20 | 26.22 ± 0.23 | <0.001 |
| ALT | 24.03 ± 0.22 | 20.95 ± 0.24 | 28.86 ± 0.40 | <0.001 |
| GGT | 31.69 ± 0.56 | 27.37 ± 0.70 | 38.45 ± 0.92 | <0.001 |
| Comorbidity, n (%) | ||||
| Hypertension | 1210 (20.44) | 530 (14.67) | 680 (29.50) | <0.001 |
| Diabetes mellitus | 493 (8.33) | 218 (6.03) | 275 (11.93) | <0.001 |
| Hyperlipidemia | 1925 (35.52) | 924 (25.57) | 1001 (43.43) | <0.001 |
| Blood Mercury (ug/L) | Total (n = 5919) | Non-Obese (n = 3614) | Overweight (n = 2305) | p-Value | |
|---|---|---|---|---|---|
| GM ± GSE | 1.15 ± 0.01 | 1.08 ± 0.01 | 1.25 ± 0.01 | <0.001 | |
| Percentile | Min | 0.07 | 0.07 | 0.50 | |
| 25th | 2.05 | 1.93 | 2.28 | ||
| 50th | 3.07 | 2.87 | 3.42 | ||
| 75th | 4.7 | 4.36 | 5.25 | ||
| Max | 115.62 | 62.74 | 115.62 | ||
| Quartile 1 (n = 1467) | Quartile 2 (n = 1471) | Quartile 3 (n = 1492) | Quartile 4 (n = 1489) | p-Value for Trend | ||
|---|---|---|---|---|---|---|
| Total | ||||||
| NAFLD | Number | 268 | 368 | 395 | 462 | <0.001 |
| Weighted frequency (95% CI) | 16.33 (14.09–18.84) | 25.09 (22.08–28.36) | 26.13 (23.35–29.12) | 31.63 (28.73–34.69) | ||
| Abnormal ALT | Number | 103 | 142 | 139 | 198 | <0.001 |
| Weighted frequency (95% CI) | 8.74 (6.84–11.11) | 11.46 (9.41–13.90) | 11.25 (9.21–13.68) | 16.32 (13.94–19.00) | ||
| Abnormal AST | Number | 92 | 124 | 121 | 184 | <0.001 |
| Weighted frequency (95% CI) | 5.63 (4.21–7.48) | 9.60 (7.64–12.00) | 8.77 (7.07–10.82) | 12.94 (10.70–15.55) | ||
| Abnormal GGT | Number | 99 | 146 | 177 | 240 | <0.001 |
| Weighted frequency (95% CI) | 5.81 (4.28–7.84) | 9.92 (8.15–12.02) | 10.56 (8.78–12.65) | 15.10 (13.10–17.33) | ||
| Non-obese (n = 3614) | ||||||
| NAFLD | Number | 29 | 36 | 36 | 49 | <0.001 |
| Weighted frequency (95% CI) | 2.98 (1.79–4.91) | 3.41 (2.21–5.21) | 4.17 (2.62–6.57) | 7.15 (5.13–9.89) | ||
| Abnormal ALT | Number | 51 | 55 | 45 | 63 | 0.020 |
| Weighted frequency (95% CI) | 6.46 (4.59–9.01) | 6.92 (5.00–9.49) | 6.37 (4.28–9.36) | 9.19 (6.67–12.53) | ||
| Abnormal AST | Number | 49 | 49 | 51 | 74 | <0.001 |
| Weighted frequency (95% CI) | 4.51 (3.02–6.67) | 5.63 (3.79–8.30) | 5.83 (3.99–8.46) | 8.77 (6.39–11.92) | ||
| Abnormal GGT | Number | 51 | 62 | 73 | 96 | 0.020 |
| Weighted frequency (95% CI) | 4.46 (3.06–6.46) | 6.22 (4.44–8.63) | 6.65 (4.93–8.92) | 11.51 (9.01–14.58) | ||
| Overweight (n = 2305) | ||||||
| NAFLD | Number | 239 | 332 | 359 | 413 | 0.523 |
| Weighted frequency (95% CI) | 52.34 (46.20–58.40) | 63.18 (57.07–68.89) | 58.44 (53.57–63.15) | 60.91 (56.18–65.44) | ||
| Abnormal ALT | Number | 52 | 87 | 94 | 135 | 0.003 |
| Weighted frequency (95% CI) | 14.92 (10.81–20.23) | 19.45 (14.95–24.91) | 18.44 (14.66–22.93) | 24.84 (20.69–29.52) | ||
| Abnormal AST | Number | 43 | 75 | 70 | 110 | 0.022 |
| Weighted frequency (95% CI) | 8.65 (5.87–12.59) | 16.57 (12.43–21.75) | 13.09 (10.08–16.83) | 17.92 (14.22–22.33) | ||
| Abnormal GGT | Number | 48 | 84 | 104 | 144 | 0.003 |
| Weighted frequency (95% CI) | 9.44 (6.07–14.38) | 16.42 (12.81–20.81) | 16.32 (12.85–20.50) | 19.39 (15.79–23.58) | ||
| Crude | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Total | ||||||||
| Quartile 1 | 1 | <0.001 * | 1 | <0.001 * | 1 | <0.001 * | 1 | <0.001 * |
| Quartile 2 | 1.71 (1.37–2.15) | <0.001 | 1.70 (1.36–2.13) | <0.001 | 1.78 (1.43–2.21) | <0.001 | 1.99 (1.58–2.52) | <0.001 |
| Quartile 3 | 1.81 (1.43–2.28) | <0.001 | 1.76 (1.40–2.23) | <0.001 | 1.91 (1.53–2.38) | <0.001 | 2.09 (1.66–2.64) | <0.001 |
| Quartile 4 | 2.37 (1.92–2.92) | <0.001 | 2.27 (1.83–2.81) | <0.001 | 2.52 (2.04–3.11) | <0.001 | 2.89 (2.30–3.62) | <0.001 |
| Non-obese (n = 3614) | ||||||||
| Quartile 1 | 1 | 0.004 * | 1 | 0.016 * | 1 | 0.002 * | 1 | <0.001 * |
| Quartile 2 | 1.14 (0.59–2.22) | 0.681 | 1.11 (0.57–2.16) | 0.738 | 1.24 (0.65–2.38) | 0.507 | 1.38 (0.71–2.68) | 0.330 |
| Quartile 3 | 1.41 (0.68–2.91) | 0.343 | 1.31 (0.63–2.71) | 0.460 | 1.48 (0.74–2.97) | 0.265 | 1.67 (0.81–3.47) | 0.161 |
| Quartile 4 | 2.50 (1.33–4.72) | 0.005 | 2.23 (1.16–4.30) | 0.016 | 2.68 (1.39–5.14) | 0.003 | 3.28 (1.69–6.35) | <0.001 |
| Overweight (n = 2305) | ||||||||
| Quartile 1 | 1 | 0.118 * | 1 | 0.001 * | 1 | <0.001 * | 1 | <0.001 * |
| Quartile 2 | 1.56 (1.13–2.14) | 0.006 | 1.68 (1.21–2.34) | 0.002 | 1.85 (1.32–2.59) | <0.001 | 2.19 (1.53–3.13) | <0.001 |
| Quartile 3 | 1.28 (0.92–1.77) | 0.134 | 1.48 (1.05–2.09) | 0.024 | 1.69 (1.18–2.42) | 0.004 | 1.88 (1.28–2.75) | 0.001 |
| Quartile 4 | 1.41 (1.03–1.94) | 0.030 | 1.86 (1.35–2.58) | <0.001 | 2.21 (1.56–3.11) | <0.001 | 2.69 (1.86–3.87) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.-J.; Yang, E.-J.; Park, K.; Oh, S.; Kim, T.; Hong, Y.-P. Association between Blood Mercury Levels and Non-Alcoholic Fatty Liver Disease in Non-Obese Populations: The Korean National Environmental Health Survey (KoNEHS) 2012–2014. Int. J. Environ. Res. Public Health 2021, 18, 6412. https://doi.org/10.3390/ijerph18126412
Yang Y-J, Yang E-J, Park K, Oh S, Kim T, Hong Y-P. Association between Blood Mercury Levels and Non-Alcoholic Fatty Liver Disease in Non-Obese Populations: The Korean National Environmental Health Survey (KoNEHS) 2012–2014. International Journal of Environmental Research and Public Health. 2021; 18(12):6412. https://doi.org/10.3390/ijerph18126412
Chicago/Turabian StyleYang, Yun-Jung, Eun-Jung Yang, Kyongjin Park, Subin Oh, Taehyen Kim, and Yeon-Pyo Hong. 2021. "Association between Blood Mercury Levels and Non-Alcoholic Fatty Liver Disease in Non-Obese Populations: The Korean National Environmental Health Survey (KoNEHS) 2012–2014" International Journal of Environmental Research and Public Health 18, no. 12: 6412. https://doi.org/10.3390/ijerph18126412