
Correlation between Handgrip Strength and Depression in Older Adults—A Systematic Review and a Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
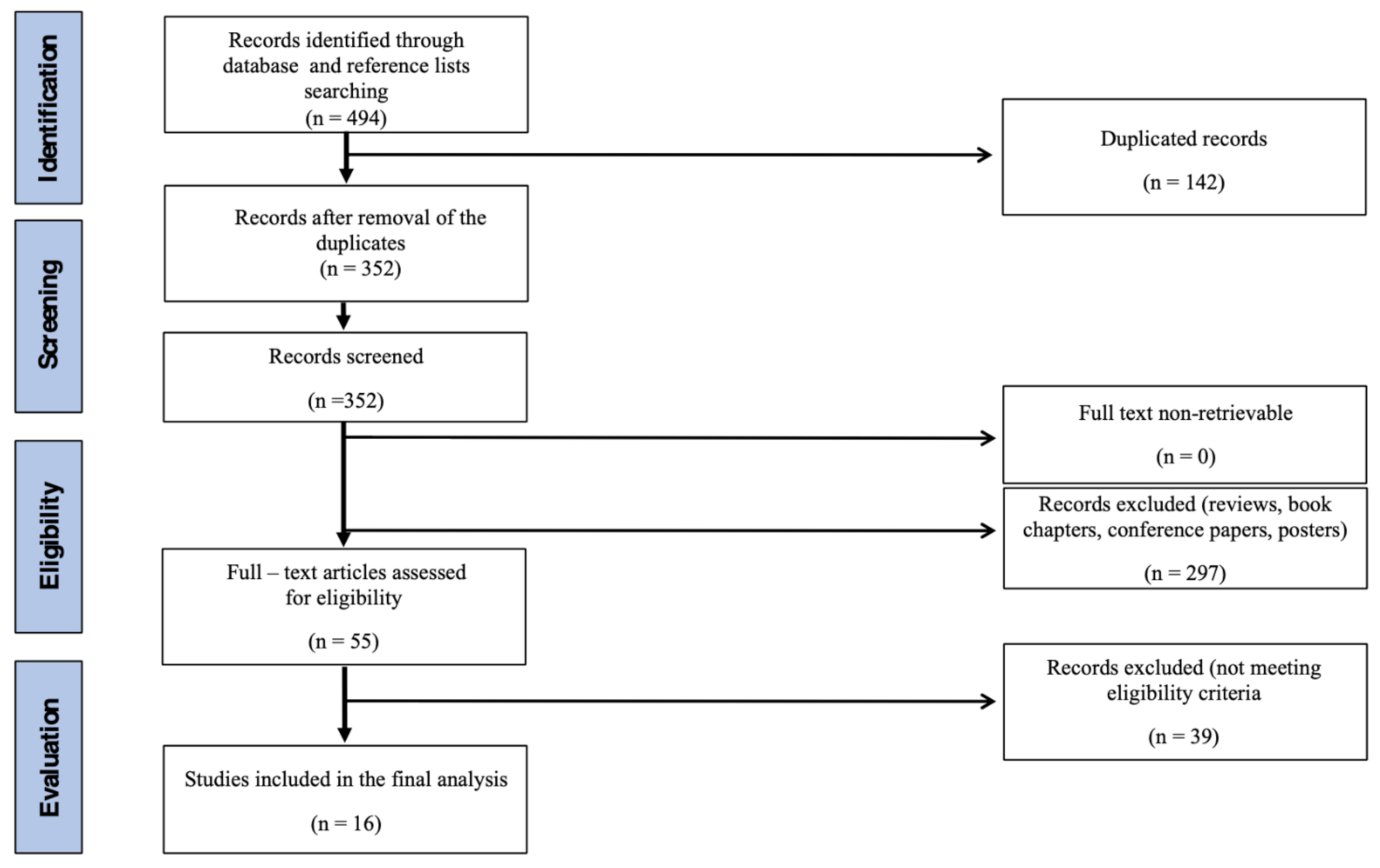
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
2.4. Measures of Effect Sizes
2.5. Statistical Analysis
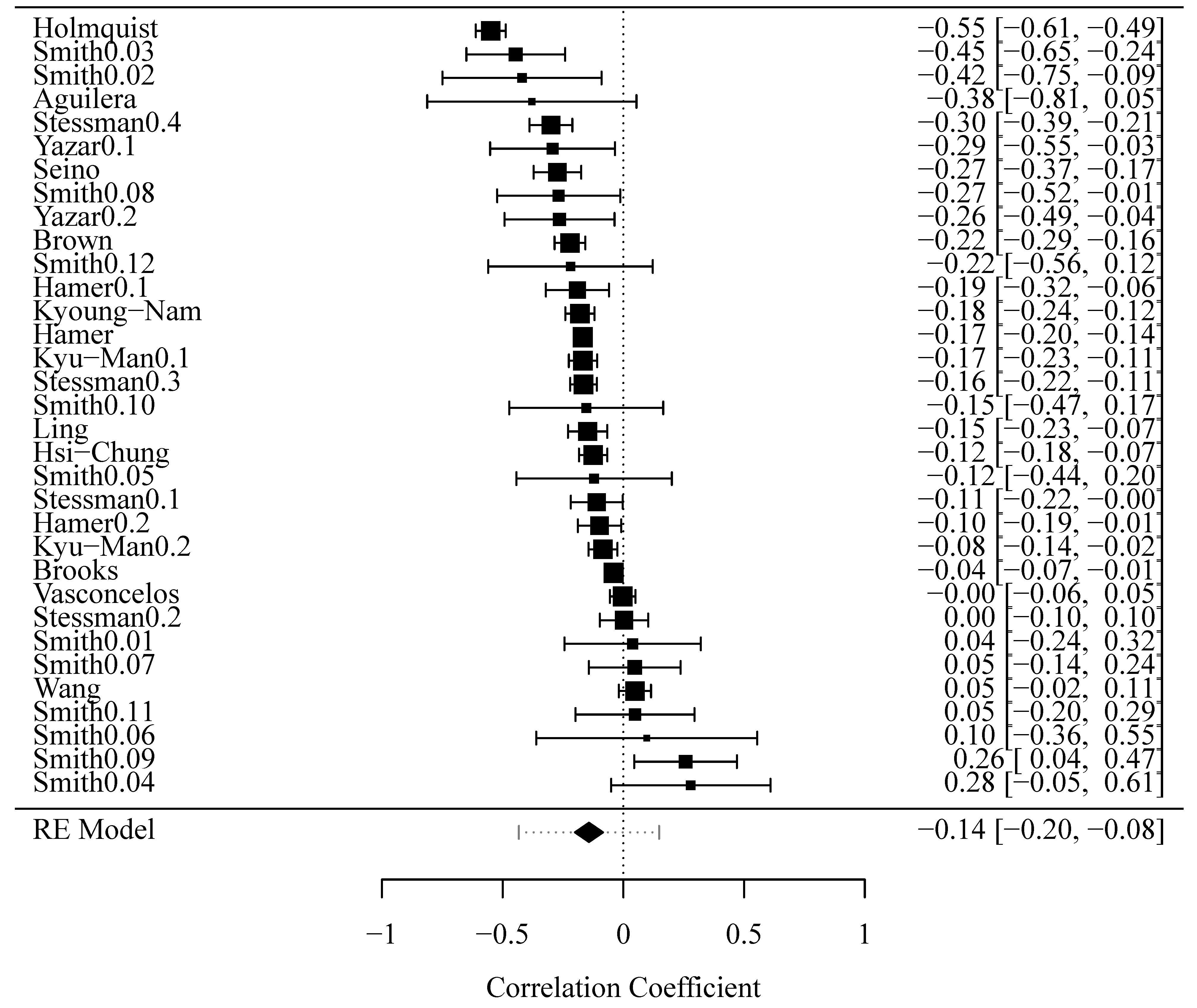
3. Results
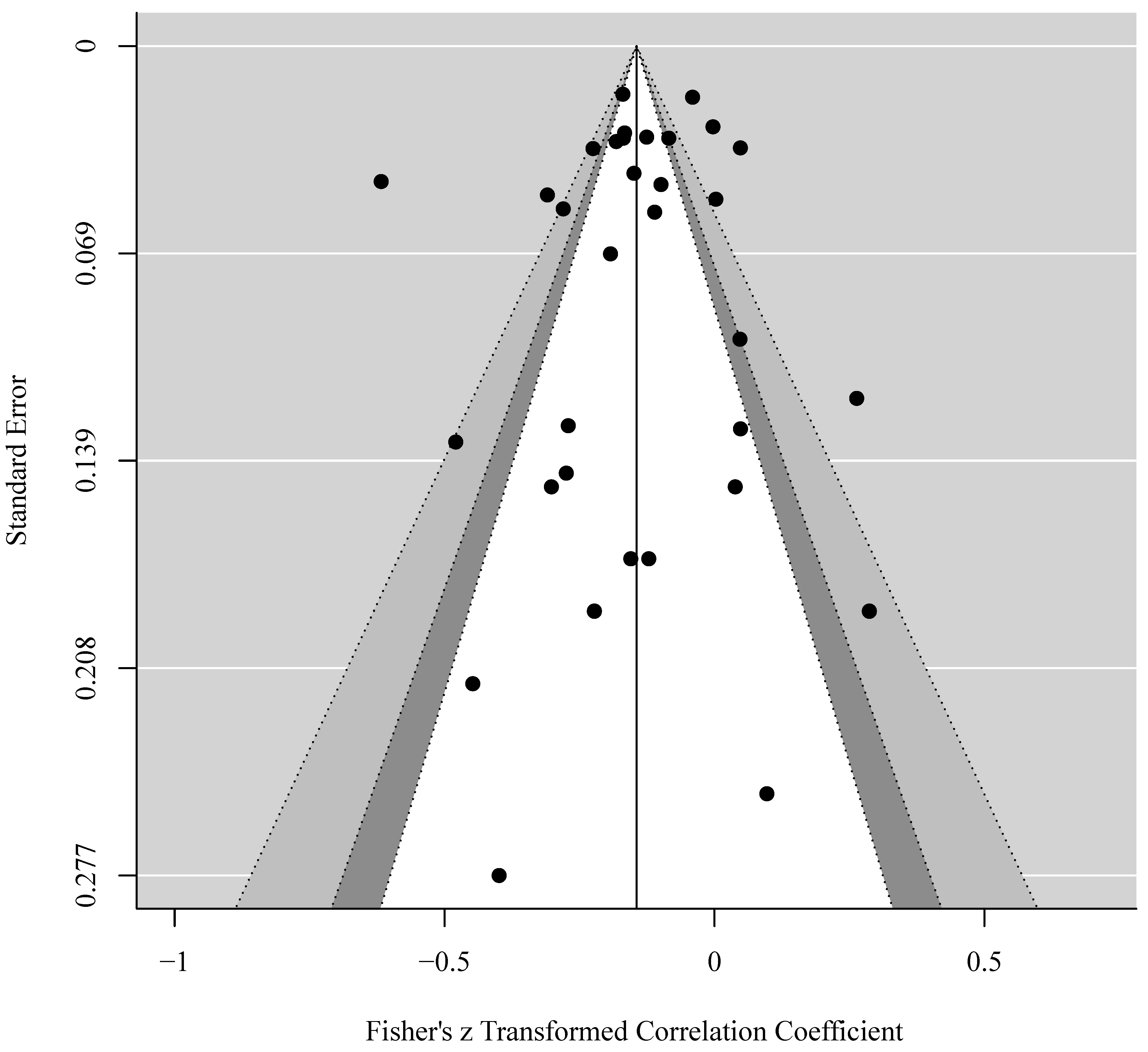
3.1. Publication Bias Analysis
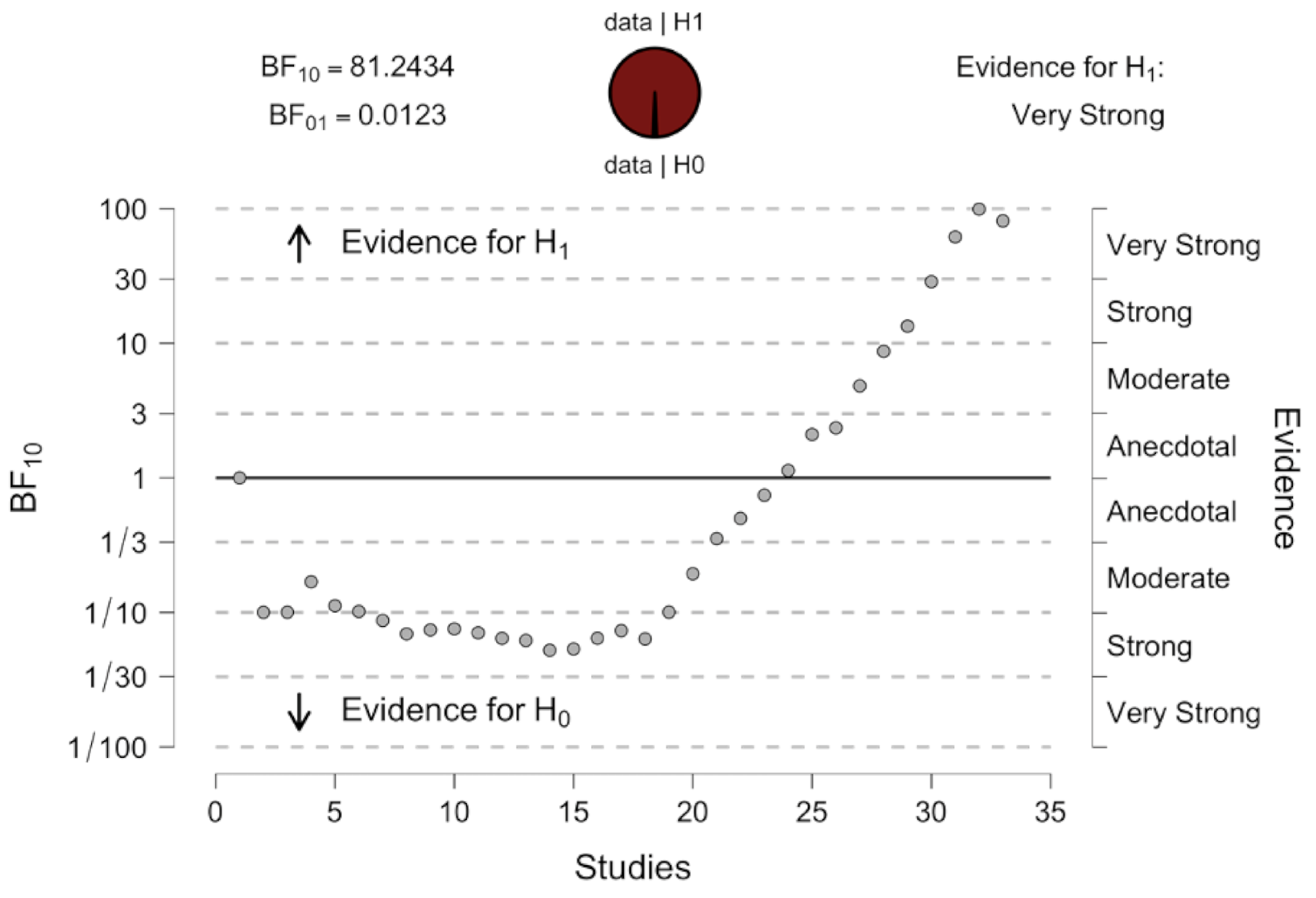
3.2. Sensitivity Analysis
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, S.Y.; Lim, J.; Park, H.S. Relationship between low handgrip strength and quality of life in Korean men and women. Qual. Life Res. 2018, 27, 2571–2580. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health of Older Adults. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults (accessed on 11 August 2020).
- Cole, M.G.; Dendukuri, N. Risk factors for depression among elderly community subjects: A systematic review and meta-analysis. Am. J. Psychiatry 2003, 160, 1147–1156. [Google Scholar] [CrossRef]
- Hölzel, L.; Härter, M.; Reese, C.; Kriston, L. Risk factors for chronic depression—A systematic review. J. Affect. Disord. 2011, 129, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Conde-Sala, J.L.; Garre-Olmo, J.; Calvó-Perxas, L.; Turró-Garriga, O.; Vilalta-Franch, J. Course of depressive symptoms and associated factors in people aged 65+ in Europe: A two-year follow-up. J. Affect. Disord. 2019, 245, 440–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, D.; Savva, G.M.; Kenny, R.; Lawlor, B.A. What predicts persistent depression in older adults across Europe? Utility of clinical and neuropsychological predictors from the SHARE study. J. Affect. Disord. 2013, 147, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Veronese, N.; Solmi, M.; Cadore, E.L.; Stubbs, B. Exercise for depression in older adults: A meta-analysis of randomized controlled trials adjusting for publication bias. Braz. J. Psychiatry 2016, 38, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO|Physical Activity and Older Adults. Available online: https://www.who.int/dietphysicalactivity/factsheet_olderadults/en/ (accessed on 11 August 2020).
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Leurgans, S.E.; Bennett, D.A. Association of muscle strength with the risk of Alzheimer disease and the rate of cognitive decline in community-dwelling older persons. Arch. Neurol. 2009, 66, 1339–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volaklis, K.; Mamadjanov, T.; Meisinger, C.; Linseisen, J. Assoziation zwischen Muskelkraft und depressiven Symptomen: Ein narrativer Review. Wien. Klin. Wochenschr. 2019, 131, 255–264. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.-K.; Lee, W.-J.; Peng, L.-N.; Liu, L.-K.; Arai, H.; Akishita, M. Recent Advances in Sarcopenia Research in Asia: 2016 Update From the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2016, 17, 767.e1-7. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hsu, T.-H.; Wu, W.-T.; Huang, K.-C.; Han, D.-S. Is sarcopenia associated with depression? A systematic review and meta-analysis of observational studies. Age Ageing 2017, 46, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 2, 495–503. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 11 August 2020).
- MacDermid, J.; Solomon, G.; Valdes, K.; American Society of Hand Therapists. Clinical Assessment Recommendations, 3rd ed.; American Society of Hand Therapists: Mount Laurel, NJ, USA, 2015; ISBN 0692525157. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Soft. 2010, 36. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Hai, S.; Liu, Y.; Cao, L.; Liu, Y.; Liu, P.; Zhou, J.; Yang, Y.; Dong, B. Association between depressive symptoms and sarcopenia in older Chinese community-dwelling individuals. Clin. Interv. Aging 2018, 13, 1605–1611. [Google Scholar] [CrossRef] [Green Version]
- Brooks, J.M.; Titus, A.J.; Bruce, M.L.; Orzechowski, N.M.; Mackenzie, T.A.; Bartels, S.J.; Batsis, J.A. Depression and Handgrip Strength Among U.S. Adults Aged 60 Years and Older from NHANES 2011-2014. J. Nutr. Health Aging 2018, 22, 938–943. [Google Scholar] [CrossRef]
- Brown, P.J.; Roose, S.P.; Fieo, R.; Liu, X.; Rantanen, T.; Sneed, J.R.; Rutherford, B.R.; Devanand, D.P.; Avlund, K. Frailty and depression in older adults: A high-risk clinical population. Am. J. Geriatr. Psychiatry 2014, 22, 1083–1095. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Batty, G.D.; Kivimaki, M. Sarcopenic obesity and risk of new onset depressive symptoms in older adults: English Longitudinal Study of Ageing. Int. J. Obes. 2015, 39, 1717–1720. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Bates, C.J.; Mishra, G.D. Depression, physical function, and risk of mortality: National Diet and Nutrition Survey in adults older than 65 years. Am. J. Geriatr. Psychiatry 2011, 19, 72–78. [Google Scholar] [CrossRef]
- Han, K.-M.; Chang, J.; Yoon, H.-K.; Ko, Y.-H.; Ham, B.-J.; Kim, Y.-K.; Han, C. Relationships between hand-grip strength, socioeconomic status, and depressive symptoms in community-dwelling older adults. J. Affect. Disord. 2019, 252, 263–270. [Google Scholar] [CrossRef]
- Ling, C.H.Y.; Taekema, D.; de Craen, A.J.M.; Gussekloo, J.; Westendorp, R.G.J.; Maier, A.B. Handgrip strength and mortality in the oldest old population: The Leiden 85-plus study. CMAJ 2010, 182, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-C.; Hsu, N.-W.; Chou, P. The Association Between Sleep Duration and Hand Grip Strength in Community-Dwelling Older Adults: The Yilan Study, Taiwan. Sleep 2017, 40. [Google Scholar] [CrossRef]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; García-Pinillos, F.; Latorre-Román, P.Á. Handgrip Strength is Associated with Psychological Functioning, Mood and Sleep in Women over 65 Years. Int. J. Environ. Res. Public Health 2019, 16, 873. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-N.; Lee, M.-R.; Choi, Y.-H.; Lee, B.-E.; Hong, Y.-C. Associations of Blood Cadmium Levels With Depression and Lower Handgrip Strength in a Community-Dwelling Elderly Population: A Repeated-Measures Panel Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1525–1530. [Google Scholar] [CrossRef]
- Seino, S.; Yabushita, N.; Kim, M.-J.; Nemoto, M.; Jung, S.; Osuka, Y.; Okubo, Y.; Figueroa, R.; Matsuo, T.; Tanaka, K. Physical performance measures as a useful indicator of multiple geriatric syndromes in women aged 75 years and older. Geriatr. Gerontol. Int. 2013, 13, 901–910. [Google Scholar] [CrossRef]
- Smith, L.; White, S.; Stubbs, B.; Hu, L.; Veronese, N.; Vancampfort, D.; Hamer, M.; Gardner, B.; Yang, L. Depressive symptoms, handgrip strength, and weight status in US older adults. J. Affect. Disord. 2018, 238, 305–310. [Google Scholar] [CrossRef]
- Stessman, J.; Rottenberg, Y.; Fischer, M.; Hammerman-Rozenberg, A.; Jacobs, J.M. Handgrip Strength in Old and Very Old Adults: Mood, Cognition, Function, and Mortality. J. Am. Geriatr. Soc. 2017, 65, 526–532. [Google Scholar] [CrossRef]
- Vasconcelos, K.S.d.S.; Dias, J.M.D.; Bastone, A.d.C.; Vieira, R.A.; Andrade, A.C.d.S.; Perracini, M.R.; Guerra, R.O.; Dias, R.C. Handgrip Strength Cutoff Points to Identify Mobility Limitation in Community-dwelling Older People and Associated Factors. J. Nutr. Health Aging 2016, 20, 306–315. [Google Scholar] [CrossRef]
- Holmquist, S.; Mattsson, S.; Schele, I.; Nordström, P.; Nordström, A. Low physical activity as a key differentiating factor in the potential high-risk profile for depressive symptoms in older adults. Depress. Anxiety 2017, 34, 817–825. [Google Scholar] [CrossRef]
- Olgun Yazar, H.; Yazar, T. Prevalence of sarcopenia in patients with geriatric depression diagnosis. Ir. J. Med. Sci. 2019, 188, 931–938. [Google Scholar] [CrossRef]
- Friedman, B.; Heisel, M.J.; Delavan, R.L. Psychometric properties of the 15-item geriatric depression scale in functionally impaired, cognitively intact, community-dwelling elderly primary care patients. J. Am. Geriatr. Soc. 2005, 53, 1570–1576. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.C.; Pignone, M.P. Screening accuracy for late-life depression in primary care: A systematic review. J. Fam. Pract. 2003, 52, 956–964. [Google Scholar] [PubMed]
- Sivertsen, H.; Bjørkløf, G.H.; Engedal, K.; Selbæk, G.; Helvik, A.-S. Depression and Quality of Life in Older Persons: A Review. Dement. Geriatr. Cogn. Disord. 2015, 40, 311–339. [Google Scholar] [CrossRef] [PubMed]
- Gatt, I.; Smith-Moore, S.; Steggles, C.; Loosemore, M. The Takei Handheld Dynamometer: An Effective Clinical Outcome Measure Tool for Hand and Wrist Function in Boxing. Hand 2018, 13, 319–324. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Amaral, J.F.; Mancini, M.; Novo Júnior, J.M. Comparison of three hand dynamometers in relation to the accuracy and precision of the measurements. Rev. Bras. Fisioter. 2012, 16, 216–224. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Cavero-Redondo, I.; Ramírez-Vélez, R.; Ruiz, J.R.; Ortega, F.B.; Lee, D.-C.; Martínez-Vizcaíno, V. Muscular Strength as a Predictor of All-Cause Mortality in an Apparently Healthy Population: A Systematic Review and Meta-Analysis of Data From Approximately 2 Million Men and Women. Arch. Phys. Med. Rehabil. 2018, 99, 2100–2113.e5. [Google Scholar] [CrossRef]
- Bohannon, R.W. Muscle strength: Clinical and prognostic value of hand-grip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef]
- Wilkinson, P.; Ruane, C.; Tempest, K. Depression in older adults. BMJ 2018, 363, k4922. [Google Scholar] [CrossRef]
- Kwon, J.; Yoshida, Y.; Iwasa, H.; Yoshida, H.; Kim, H.; Sugiura, M.; Furuna, T.; Suzuki, T. Health status of community-dwelling elderly with geriatric syndrome. Nihon Ronen Igakkai Zasshi 2007, 44, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Buckley, M.R.; Lachman, V.D. Depression in older patients: Recognition and treatment. JAAPA 2007, 20, 34–41. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Selection | Comparability | Outcome | Total Score | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Sample | Sample Size | Non- Respondents | Ascertainment of Exposure | Score | Based on Design and Analysis | Score | Assessment of the Outcome | Statistical Test | Score | ||
| Wang 2018 [19] | * | - | * | ** | **** | ** | ** | * | * | ** | 8 * |
| Brooks 2018 [20] | * | * | * | ** | ***** | ** | ** | * | - | * | 8 * |
| Brown 2012 [21] | * | - | * | ** | **** | ** | ** | * | * | ** | 8 * |
| Hammer 2015 [22] | * | - | * | ** | **** | ** | ** | * | * | ** | 8 * |
| Hammer 2011 [23] | * | - | - | * | ** | ** | ** | * | * | ** | 6 * |
| Han 2019 [24] | * | * | * | ** | ***** | ** | ** | * | * | ** | 9 * |
| Ling 2010 [25] | * | - | - | ** | *** | ** | ** | * | * | ** | 7 * |
| Chen 2017 [26] | * | - | - | ** | *** | ** | ** | * | * | ** | 7 * |
| Laredo-Aguilera 2019 [27] | - | - | * | * | ** | ** | ** | * | - | * | 5 * |
| Kim 2016 [28] | * | - | * | ** | **** | ** | ** | * | * | ** | 8 * |
| Seino 2013 [29] | * | - | * | * | *** | * | * | * | * | ** | 6 * |
| Smith 2018 [30] | * | - | * | * | *** | ** | ** | * | * | ** | 7 * |
| Stessman 2017 [31] | * | - | * | ** | **** | ** | ** | * | * | ** | 8 * |
| Vasconcelos 2016 [32] | * | * | * | ** | ***** | ** | ** | * | * | ** | 9 * |
| Holmquist 2017 [33] | * | - | - | ** | *** | ** | ** | * | - | * | 6 * |
| Yazar 2019 [34] | * | - | - | ** | *** | * | * | * | - | * | 5 * |
| Author and Year of Publication | Participants | Type of Dynamometer; Unit | Depression Scale | Inclusion/Exclusion Criteria | Relationships between HGS and Depressive Symptoms |
|---|---|---|---|---|---|
| Vasconcelos 2016 [32] | 1374 subjects, women and men, age 73.4 ± 6.4 | Jamar; kgf | GDS-15 | Inclusion criteria: age ≥65 years, living in the community in the urban areas of Brazil. Exclusion criteria: score of <17 in the Mini Mental State Examination-MMSE), inability to walk, being bedridden, inability to hold a handheld dynamometer due to pain or hand deformities, hemiparesis caused by a stroke, severe Parkinson’s disease, cancer treatment (except for skin cancer) and terminal illness. | Incidence of depressive symptoms in the group with MW-muscle weakness (HGS ≤17.4 kgf for women and ≤25.8 kgf for men)-16.8% and NONE = no muscle weakness and no mobility limitation-11.4% |
| Smith 2018 [30] | 587 subjects, women and men, age 69.2 ± n/d | Takei Digital Grip Strength Dynamometer; kg | PHQ-9 | Inclusion criterion: age ≥ 60 years | Relationship between depressive symptoms and HGS by weight status from multiple linear regression models among adults aged ≥ 60 years |
| Wang 2018 [19] | 865 subjects, women and men, age 68.68 ± 6.46 | EH 101, Camry, Zhongshan, China; kg | GDS-15 | Inclusion criterion: age ≥60 years Exclusion criteria: reported the presence of disease (including hyperthyroidism, hypothyroidism, or chronic heart or renal failure), physical disabilities (e.g., loss of a hand, foot, or multiple limbs), implanted electronic devices or orthopedic metal implantations, and those taking prescribed medications which could affect body composition (e.g., long-term systemic corticosteroids), severe hearing or eye problems, missing data | Comparison of HGS in the group with no depression = 30.1 ± 8.9 kg and with depression 29.2 ± 9.4 kg |
| Laredo-Aguilera 2019 [27] | 16 subjects, only women, age 72.29 ± 5.21 | TKK 5101 Grip D, Takey, Tokyo, Japan; kg | GDS-15 | Inclusion criteria: not institutionalized; active women and above the age of 65; not suffering from mental and/or intellectual disorders; free of cardiovascular and neuromuscular disorders; considered physically independent according to the Spanish version of the Barthel Index. Exclusion criteria: participation in other training programs; artificial prosthesis; any disease requiring daily intake of drugs affecting the athletic performance, in order to avoid any influence on fitness measures; any disease that contraindicated the exercise program; any symptom that a medical professional deemed as warranting exclusion. | Pearson correlation analysis adjusted for age showed significant correlations between HGS and depression (r = 0.379, p = 0.021) |
| Ling 2010 [25] | 484 subjects, women and men, age 85–89 | Jamar; kg | GDS-15 | Data from the prospective population-based Lei-den 85-plus study, which involved all 85-year-old inhabitants of Leiden, The Netherlands. No selection criteria had been imposed for health status or demographic characteristics. | Lower HGS was significantly associated (p < 0.001) with higher GDS scores |
| Stessman 2017 [31] | 2304 subjects, women and men, age 70–90 | 5001 Grip- A, Takei, Niigata City, Japan; kg | BSI | Inclusion criterion: aged 70 to 71 at baseline in 1990–1991. | Relationship between HGS and depression measured at the ages of 70, 78, 85 and 90 years |
| Seino 2013 [29] | 340 subjects, only women, age 80.0 ± 4.6 | TKK 5401 Grip D, Takey, Tokyo, Japan; kg | CES-D | Inclusion criteria: female, aged ≥ 75 years Exclusion criteria: required a cane or other walking device, or their physical performance could not be measured by a standard method, e.g., they needed physical support from another person; could not understand the instructions of performance tests and questionnaires; or had data missing from their performance tests and geriatric syndromes. | Relationships between HGS and depressive symptoms expressed as odds ratio: adjusted for age, stroke, hypertension, diabetes mellitus, heart disease, respiratory disease, osteoporosis, dyslipidemia, low back pain and knee pain = 2.8 (1.2–6.3) |
| Olgun Yazar and Yazar 2019 [34] | 281 subjects, women and men, age W/M: control 72.40 ± 6.46/72.26 ± 6.520 experimental 75.84 ± 6.98/ 74.14 ± 7.92 | Jamar; kg | GDS-15 | Inclusion criteria: normal neurological examination, without known chronic disease history apart from hypertension or chronic medication use, with no loss of more than 10% body weight within the last 6 months, and with HDRS score below 7 (control 1) or GDS score below 10 (control 2). GD patients additionally abided by the same exclusion criteria as healthy volunteers, apart from using at least one antidepressant. Patients with pacemaker or any implant and those with diseases severely affecting mobility (cerebrovascular events causing confinement to bed, advanced muscle disease, hip dislocations, decompensated heart failure, acute and chronic renal failure with fluid load, etc.) were not included in the study. | Mean HGS in the group of older people without depression 21.70 ± 5.478 and with depression 18.71 ± 5.4 |
| Chen 2017 [26] | 1081 subjects, women and men, age 76.3 ± 6.1 | Jamar; kg | HADS | Inclusion criteria: aged ≥ 65 years and residence in Yilan City. Individuals who failed to provide a past medical history, who could not complete the interview, or who were unable to cooperate regarding the collection of anthropometric data because of physical disability or compromised cognitive function were excluded. | Individuals with depressive symptoms demonstrated weaker HGS (p < 0.001) |
| Kim 2016 [28] | 983 subjects, women and men, age 75.2 ± 6.0 | Hand Grip Meter 6103, Tanita, Tokyo, Japan; kg | GDS-15 | Inclusion criteria: age ≥ 60 years and the ability to communicate with and follow instructions from the survey staff. Exclusion criteria: lack of information on blood cadmium concentration handgrip strength, anthropometric measurement and alcohol consumption, | Relationship between GDS score and HGS using linear mixed models. Adjusted for age, sex, city of residence, monthly income, education level, smoking status, pack-years of smoking, passive smoking status, alcohol drinking, moderate physical activity, weight, height, and comorbidity status. Right hand: beta −0.18; CI 95% −0.23, −0.13 Left hand: beta −0.15; CI 95% −0.20, −0.10 |
| Brooks 2018 [20] | 3421 subjects, women and men, age 69.9 ± 6.9 | -; kg | PHQ-9 | Exclusion criteria: age <60 years, missing data. | Linear Regression Models for Depressive Symptoms by HGS Outcome −0.19 ± 0.08 |
| Brown 2012 [21] | 854 subjects, women and men, age 75 ± n/d | -; kgf siła | CES-D | Inclusion criterion: 75 years of age at the time of the evaluation. Exclusion criteria: missing baseline depression data or missing data on all of the four frailty characteristics. | Mean HGS in the non-depressed group: 35.28 (12.57) kgf and in the mildly depressed group: 29.69 (10.20) kgf and in the depressed group: 30.07 (11.75) kgf |
| Hamer 2011 [23] | 679 subjects, women and men, age: non-depressed 75.7 ± 7.1 depressed 79.0 ± 7.7 | hand-held dynamometer; kg | GDS-15 | Inclusion criterion: aged ≥ 65 years | Mean HGS in the non-depressed group: men 33.84 ± 10.6 kg, women 19.12 ± 10.0 kg and in the depressed group: men 29.74 ± 10.5 kg, women 17.11 ± 10.6 kg |
| Hamer 2015 [22] | 3862 subjects, women and men, age 64.6 ± 8.3 | Smedley hand-held dynamometer, Stoelting, USA; kg | CES-D | Inclusion criteria: absence of depression at baseline and availability of exposure, outcome and covariate data. For the key exposure measure, grip strength, there were no upper age limits Respondents were excluded if they had swelling or inflammation, severe pain or a recent injury or surgery to the hand in the preceding6 months. | Mean HGS in the non-depressed group: 31.2 ± 11.2 kg and in the depressed group: 27.4 ± 10.5 kg |
| Han 2019 [24] | 1056 subjects, women and men, age 69.55 ± 6.25 | THH 5401 Takei, Tokyo, Japan | PHQ-9 | Inclusion criteria: adults aged ≥ 60 years with all of the following conditions: reliable data from a handgrip dynamometer; responded to the questionnaires regarding depressive symptoms; no missing data regarding sociodemographic and health-related variables. | In logistic regression analysis, older adults in the lowest HGS tertile were more likely to have depressive symptoms compared to those in the highest HGS tertile (adjusted odds ratio [aOR] = 1.85, 95% confidence interval [CI] = 1.25–2.74). |
| Holmquist 2017 [33] | 490 subjects, women and men, age 70 ± 0 | Jamar, kg | GDS-15 | Residency in Umeå, Sweden was the only criterion for inclusion. Exclusion criteria: none | The present study provided a potential high-risk profile for depressive symptoms among elderly community-dwelling individuals, which included low levels functional performance (including HGS) combined with low levels of physical activity. |
| Author and Year of Publication | Group Size | Sex | Depression Scale | The Result Presented in the Work | The Size of the Effect Expressed in req | |
|---|---|---|---|---|---|---|
| Vasconcelos 2016 [32] | 1374 | both | GDS-15 | OR | 0.99 | −0.003 |
| Smith 2018 [30] | 49 | M | PHQ-9 | beta | 0.34 | 0.039 |
| 25 | M | beta | −3.72 | −0.420 | ||
| 60 | M | beta | −4.12 | −0.446 | ||
| 31 | M | beta | 2.01 | 0.279 | ||
| 37 | M | beta | −1.25 | −0.121 | ||
| 19 | M | beta | 1.45 | 0.100 | ||
| 107 | F | beta | 0.31 | 0.047 | ||
| 52 | F | beta | −1.83 | −0.268 | ||
| 75 | F | beta | 0.86 | 0.258 | ||
| 37 | F | beta | −0.93 | −0.154 | ||
| 64 | F | beta | 0.22 | 0.048 | ||
| 31 | F | beta | −1.1 | −0.219 | ||
| Wang 2018 [19] | 865 | both | GDS-15 | d | −0.101 | −0.050 |
| Laredo-Aguilera 2019 [27] | 16 | F | GDS-15 | r | −0.379 | −0.379 |
| Ling 2010 [25] | 484 | both | GDS-15 | req | −0.148 | −0.148 |
| Stessman 2017 [31] | 327 | both | BSI | OR | 0.668 | −0.110 |
| 384 | OR | 1.009 | 0.003 | |||
| 1187 | OR | 0.545 | −0.165 | |||
| 406 | OR | 0.320 | −0.300 | |||
| Seino 2013 [29] | 340 | F | CES-D | OR | 0.357 | −0.273 |
| Olgun 2019 [34] | 144 | M | GDS-15 | phi | 0.192 | −0.293 |
| 137 | F | phi | 0.414 | −0.264 | ||
| Chen 2017 [26] | 1081 | both | HADS | req | −0.125 | −0.125 |
| Kim 2016 [28] | 983 | both | GDS-15 | beta std. | −0.180 | −0.180 |
| Brooks 2018 [20] | 3421 | both | PHQ-9 | beta | −0.190 | −0.041 |
| Brown 2012 [21] | 854 | both | CES-D | d | −0.454 | −0.221 |
| Hamer 2011 [23] | 210 | M | GDS-15 | d | −0.388 | −0.190 |
| 469 | F | d | −0.198 | −0.099 | ||
| Hamer 2015 [12] | 3862 | both | CES-D | d | −0.341 | −0.168 |
| Han 2019 [24] | 1056 | both | PHQ-9 | OR | 0.541 | −0.167 |
| OR | 0.735 | −0.084 | ||||
| Holmquist 2017 [33] | 490 | both | GDS-15 | d | −1.315 | −0.549 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Kleka, P.; Pawlaczyk, M. Correlation between Handgrip Strength and Depression in Older Adults—A Systematic Review and a Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4823. https://doi.org/10.3390/ijerph18094823
Zasadzka E, Pieczyńska A, Trzmiel T, Kleka P, Pawlaczyk M. Correlation between Handgrip Strength and Depression in Older Adults—A Systematic Review and a Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(9):4823. https://doi.org/10.3390/ijerph18094823
Chicago/Turabian StyleZasadzka, Ewa, Anna Pieczyńska, Tomasz Trzmiel, Paweł Kleka, and Mariola Pawlaczyk. 2021. "Correlation between Handgrip Strength and Depression in Older Adults—A Systematic Review and a Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 9: 4823. https://doi.org/10.3390/ijerph18094823