
A Validation Study of the Revised Caregiving Burden Instrument in Korean Family Caregivers of Stroke Survivors


Abstract
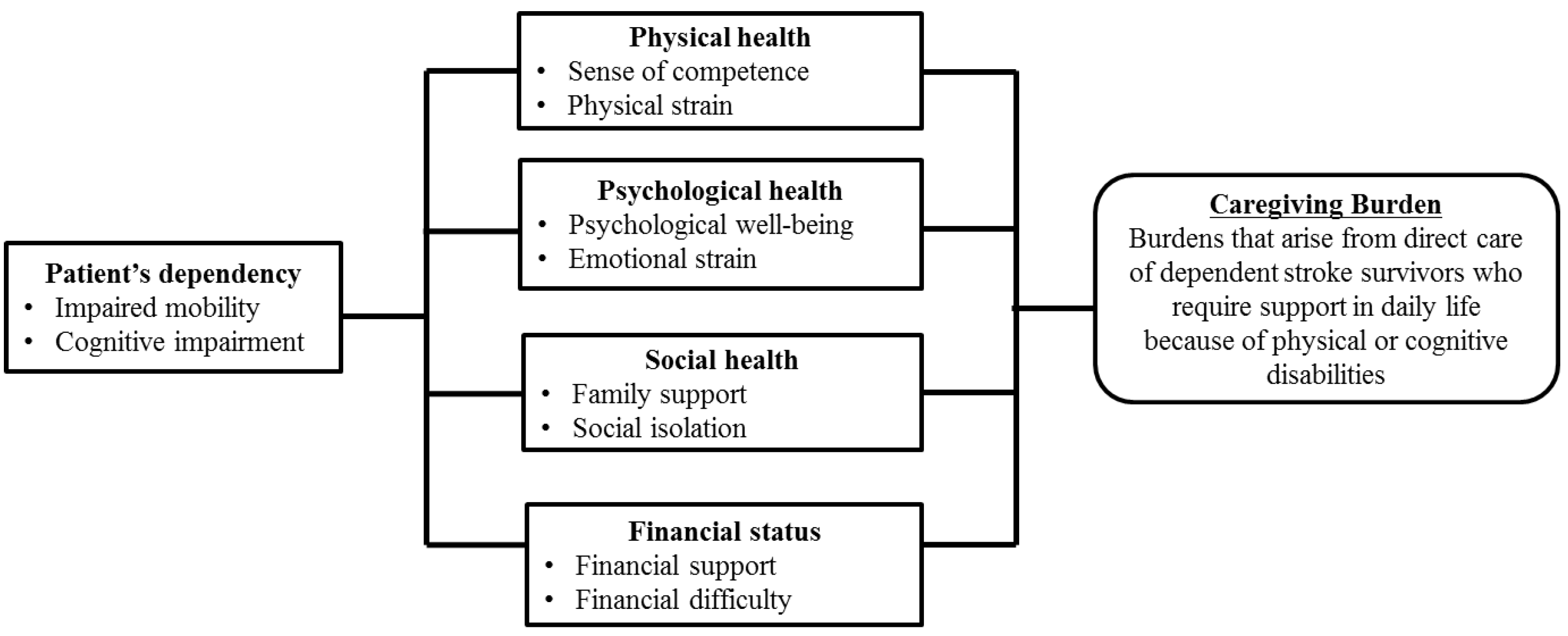
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measurements
2.3.1. Demographics of Caregivers and Stroke Survivors
2.3.2. Caregiver Burden
2.4. Ethical Considerations
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. General Characteristics
3.2. Psychometric Testing of the Scale
3.2.1. Item Analysis
3.2.2. Examination of Factor Independence and Reliability
3.2.3. Exploratory Factor Analysis
3.2.4. Construct Validity: Known-Group Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Camicia, M.; Lutz, B.J.; Markoff, N.; Catlin, A. Determining the needs of family caregivers of stroke patients during inpatient rehabilitation using interview, art, and survey. Rehabil. Nurs. 2019, 44, 328–337. [Google Scholar] [CrossRef]
- Pont, W.; Groeneveld, I.; Arwert, H.; Meesters, J.; Mishre, R.R.; Vliet Vlieland, T.; Goossens, P.; SCORE-Study Group. Caregiver burden after stroke: Changes over time? Disabil. Rehabil. 2020, 42, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.I.; Naglie, G.; Silver, F.L.; Gignac, M.A. Stroke family caregivers’ support needs change across the care continuum: A qualitative study using the timing it right framework. Disabil. Rehabil. 2013, 35, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Lutz, B.J.; Young, M.E.; Cox, K.J.; Martz, C.; Creasy, K.R. The crisis of stroke: Experiences of patients and their family caregivers. Top. Stroke Rehabil. 2011, 18, 786–797. [Google Scholar] [CrossRef]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Arkan, G.; Beser, A.; Ozturk Haney, M.; Ozturk, V. Psychometric testing of the Turkish version of the Stroke Self-Efficacy Questionnaire. J. Nurs. Res. 2019, 27, e35. [Google Scholar] [CrossRef]
- Jaracz, K.; Grabowska-Fudala, B.; Górna, K.; Jaracz, J.; Moczko, J.; Kozubski, W. Burden in caregivers of long-term stroke survivors: Prevalence and determinants at 6 months and 5 years after stroke. Patient Educ. Couns. 2015, 98, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Jaracz, K.; Grabowska-Fudala, B.; Górna, K.; Kozubski, W. Consequences of stroke in the light of objective and subjective indices: A review of recent literature. Neurol. Neurochir. Pol. 2014, 48, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Kruithof, W.J.; Post, M.W.; van Mierlo, M.L.; van den Bos, G.A.; de Man-van Ginkel, J.M.; Visser-Meily, J.M. Caregiver burden and emotional problems in partners of stroke patients at two months and one year post-stroke: Determinants and prediction. Patient Educ. Couns. 2016, 99, 1632–1640. [Google Scholar] [CrossRef]
- Pucciarelli, G.; Ausili, D.; Galbussera, A.A.; Rebora, P.; Savini, S.; Simeone, S.; Alvaro, R.; Vellone, E. Quality of life, anxiety, depression and burden among stroke caregivers: A longitudinal, observational multicentre study. J. Adv. Nurs. 2018. [Google Scholar] [CrossRef] [PubMed]
- Byun, E.; Evans, L.K. Concept analysis of burden in caregivers of stroke survivors during the early poststroke period. Clin. Nurs. Res. 2015, 24, 468–486. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lee, D.T. Meaning in stroke family caregiving: A literature review. Geriatr. Nurs. 2017, 38, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lee, D.T.F. Meaning in stroke family caregiving in China: A phenomenological study. J. Fam. Nurs. 2019, 25, 260–286. [Google Scholar] [CrossRef]
- Kramer, B.J. Gain in the caregiving experience: Where are we? what next? Gerontologist 1997, 37, 218–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmstahl, S.; Malmberg, B.; Annerstedt, L. Caregiver’s burden of patients 3 years after stroke assessed by a Novel caregiver burden scale. Arch. Phys. Med. Rehabil. 1996, 77, 177–182. [Google Scholar] [CrossRef]
- Scholte op Reimer, W.J.; de Haan, R.J.; Pijnenborg, J.M.; Limburg, M.; van den Bos, G.A. Assessment of burden in partners of stroke patients with the sense of competence questionnaire. Stroke 1998, 29, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Bakas, T.; Champion, V.; Perkins, S.M.; Farran, C.J.; Williams, L.S. Psychometric testing of the revised 15-item Bakas Caregiving Outcomes Scale. Nurs. Res. 2006, 55, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Thomas, P.; Cheng, Q.; Clement, N.; McDougall, A.; Hodgkinson, S.; Cordato, D. Trends in acute stroke presentations to an emergency department: Implications for specific communities in accessing acute stroke care services. Postgrad. Med. J. 2019, 95, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, N.; Holley, J.; Ellmers, T.; Mein, G.; Cloud, G. Qualitative focus group study investigating experiences of accessing and engaging with social care services: Perspectives of carers from diverse ethnic groups caring for stroke survivors. BMJ Open 2016, 6, e009498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jessup, N.M.; Bakas, T.; McLennon, S.M.; Weaver, M.T. Are there gender, racial or relationship differences in caregiver task difficulty, depressive symptoms and life changes among stroke family caregivers? Brain Inj. 2015, 29, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Mårtensson, J.; Zhao, Y.; Johansson, L. Living on the edge: Family caregivers’ experiences of caring for post-stroke family members in China: A qualitative study. Int. J. Nurs. Stud. 2019, 94, 1–8. [Google Scholar] [CrossRef]
- Qiu, X.; Sit, J.W.H.; Koo, F.K. The influence of Chinese culture on family caregivers of stroke survivors: A qualitative study. J. Clin. Nurs. 2018, 27, e309–e319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastawrous, M. Caregiver burden-A critical discussion. Int. J. Nurs. Stud. 2013, 50, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Roh, Y.S. Development of an instrument measuring caregiving consequences for the family of stroke patients. Clin. Nurs. Res. 2005, 10, 33–44. [Google Scholar]
- Kang, H. A guide on the use of factor analysis in the assessment of construct validity. J. Korean Acad. Nurs. 2013, 43, 587–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pett, M.A.; Lackey, N.R.; Sullivan, J.J. Making Sense of Factor Analysis: The Use of Factor Analysis for Instrument Development in Health Care Research; Sage Publications: London, UK, 2003. [Google Scholar]
- Bédard, M.; Molloy, D.W.; Squire, L.; Dubois, S.; Lever, J.A.; O’Donnell, M. The Zarit Burden Interview: A new short version and screening version. Gerontologist 2001, 41, 652–657. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Sage Publications: London, UK, 2014. [Google Scholar]
- Lin, L.N.; Wu, S.C. Measurement structure of the caregiver burden scale: Findings from a national community survey in Taiwan. Geriatr. Gerontol. Int. 2014, 14, 176–184. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F. Scale Development: Theory and Applications, 3rd ed.; Sage Publications: Los Angeles, CA, USA, 2012. [Google Scholar]
- Deeken, J.F.; Taylor, K.L.; Mangan, P.; Yabroff, K.R.; Ingham, J.M. Care for the caregivers: A review of self-report instruments developed to measure the burden, needs, and quality of life of informal caregivers. J. Pain Symptom Manag. 2003, 26, 922–953. [Google Scholar] [CrossRef]
- Gbiri, C.A.; Olawale, O.A.; Isaac, S.O. Stroke management: Informal caregivers’ burdens and strians of caring for stroke survivors. Ann. Phys. Rehabil. Med. 2015, 58, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Category | n (%)/Mean ± SD | |
|---|---|---|---|
| Stroke survivors | Age (years) | 65.85 ± 15.86 | |
| ≤30 | 8(3.8) | ||
| 31–40 | 8(3.8) | ||
| 41–50 | 16(7.7) | ||
| 51–60 | 31(14.9) | ||
| 61–70 | 57(27.4) | ||
| 71–80 | 57(27.4) | ||
| ≥81 | 31(14.9) | ||
| Gender (men) | 134(64.4) | ||
| Marital status | Single | 29(13.9) | |
| Married | 146(70.2) | ||
| Others | 33(15.9) | ||
| Caregivers | Age (years) | 57.77 ± 13.20 | |
| ≤30 | 7(3.4) | ||
| 31–40 | 18(8.7) | ||
| 41–50 | 32(15.4) | ||
| 51–60 | 56(26.9) | ||
| 61–70 | 64(30.8) | ||
| 71–80 | 27(13.0) | ||
| ≥81 | 4(1.9) | ||
| Gender (women) | 172(82.7) | ||
| Marital status | Single | 25(12.0) | |
| Married | 176(84.6) | ||
| Others | 7(3.4) | ||
| Education | ≤High school | 102(49.0) | |
| College | 95(45.7) | ||
| Graduate school | 11(5.3) | ||
| Religion | None | 42(20.2) | |
| Yes | 166(79.8) | ||
| Relationship | Spouse | 93(44.7) | |
| Son | 25(12.0) | ||
| Daughter | 41(19.7) | ||
| Daughter-in-law | 2(1.0) | ||
| Granddaughter | 5(2.4) | ||
| Others | 42(20.2) | ||
| Monthly income ($) | <2500 | 80(38.5) | |
| 2500–4499 | 63(30.3) | ||
| 4500–5999 | 34(16.3) | ||
| ≥6000 | 31(14.9) | ||
| Caregiving duration (months) | 71.55 ± 79.67 | ||
| ≤12 | 62(29.8) | ||
| 13–24 | 27(13.0) | ||
| 25–36 | 13(6.3) | ||
| 37–48 | 17(8.2) | ||
| ≥49 | 89(42.8) |
| Item (Number of Items) | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 |
|---|---|---|---|---|---|
| Factor 1. Family support (7) | |||||
| Q1. I feel like a victim of my family. | 0.81 | 0.11 | 0.12 | 0.11 | 0.13 |
| Q2. My family does not know about my effort or hard work. | 0.78 | 0.13 | 0.16 | 0.09 | −0.03 |
| Q3. Families are not interested in caring for patients. | 0.78 | 0.23 | −0.05 | 0.01 | −0.07 |
| Q4. I am frustrated with families who do not care for patients. | 0.77 | 0.16 | 0.06 | 0.07 | 0.09 |
| Q5. I get angry when I see a patient. | 0.74 | 0.05 | 0.11 | 0.19 | 0.34 |
| Q6. Because of the patient, my relationship with my family is worse than before. | 0.59 | 0.23 | 0.25 | 0.33 | 0.08 |
| Q7. I get angry easily because I cannot tolerate things as before. | 0.56 | 0.21 | 0.17 | 0.35 | 0.24 |
| Factor 2. Patient’s dependency (5) | |||||
| Q8. The patient wants me to stay with him (her) all the time. | 0.21 | 0.74 | 0.11 | 0.14 | 0.13 |
| Q9. The patient wants me to do what they can do themselves. | 0.25 | 0.70 | 0.06 | 0.11 | 0.12 |
| Q10. Even if I go out, my mind is with the patient. | 0.09 | 0.61 | 0.36 | 0.24 | 0.26 |
| Q11. I’ve had fewer meetings recently with people than ever before. | 0.17 | 0.57 | 0.12 | 0.29 | 0.31 |
| Q12. I always live in tension because of the patient. | 0.18 | 0.55 | 0.36 | 0.13 | 0.40 |
| Factor 3. Physical health (4) | |||||
| Q13. I am sorry I cannot do for the patient as much as I want to because I am tired. | 0.09 | 0.07 | 0.77 | 0.11 | 0.04 |
| Q14. I am concerned about the future of the patient. | 0.07 | 0.29 | 0.69 | 0.14 | 0.27 |
| Q15. I am responsible for my patient beyond my ability. | 0.21 | 0.03 | 0.65 | 0.21 | 0.17 |
| Q16. I cannot sleep well enough. | 0.12 | 0.32 | 0.55 | 0.19 | 0.02 |
| Factor 4. Financial burden (4) | |||||
| Q17. I am worried about the high cost of patient care. | 0.02 | 0.05 | 0.37 | 0.76 | −0.02 |
| Q18. The cost of the patient makes it difficult for the family. | 0.21 | 0.35 | 0.16 | 0.75 | 0.17 |
| Q19. I cannot afford to spend money like I used to. | 0.28 | 0.25 | 0.12 | 0.73 | 0.21 |
| Q20. I have to do other things in the house while I look after the patient. | 0.24 | 0.19 | 0.06 | 0.43 | 0.37 |
| Factor 5. Psychological health (3) | |||||
| Q21. I am always worried about the patient. | −0.06 | 0.16 | 0.31 | 0.05 | 0.78 |
| Q22. It is painful to see the patient. | 0.39 | 0.18 | 0.10 | 0.32 | 0.57 |
| Q23. When I think about the patient, I get depressed. | 0.34 | 0.33 | 0.05 | 0.25 | 0.51 |
| Mean ± SD | 2.55 ± 0.88 | 3.75 ± 0.77 | 3.98 ± 0.67 | 3.58 ± 0.87 | 3.67 ± 0.80 |
| Cronbach’s alpha | 0.89 | 0.85 | 0.79 | 0.80 | 0.68 |
| % of variance | 17.7 | 13.5 | 11.9 | 10.6 | 9.0 |
| Cumulative % | 17.7 | 31.2 | 43.1 | 53.7 | 62.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.S.; Roh, Y.S. A Validation Study of the Revised Caregiving Burden Instrument in Korean Family Caregivers of Stroke Survivors. Int. J. Environ. Res. Public Health 2021, 18, 2960. https://doi.org/10.3390/ijerph18062960
Kim SS, Roh YS. A Validation Study of the Revised Caregiving Burden Instrument in Korean Family Caregivers of Stroke Survivors. International Journal of Environmental Research and Public Health. 2021; 18(6):2960. https://doi.org/10.3390/ijerph18062960
Chicago/Turabian StyleKim, So Sun, and Young Sook Roh. 2021. "A Validation Study of the Revised Caregiving Burden Instrument in Korean Family Caregivers of Stroke Survivors" International Journal of Environmental Research and Public Health 18, no. 6: 2960. https://doi.org/10.3390/ijerph18062960