1. Introduction
Endocrine-disrupting chemicals (EDCs) are ubiquitous exogenous chemical substances that interfere with a series of functions of endocrine system either by enzyme and receptor-mediated mechanisms or epigenetic effects, thereby adversely inducing various aspects of reproductive, metabolic, neurological, and immune problems at any stage of human life [
1,
2]. Phthalates and bisphenol A (BPA) are two prevailing EDCs that have drawn increasingly remarkable public concern globally over the past few decades.
Phthalates are a group of aromatic chemicals consisting of dialkyl esters or alkyl and aryl esters of orthophthalic acid (1,2-dicarboxylic acid) [
3], and can be commonly separated into two categories, i.e., high molecular weight (HMW) phthalates and low molecular weight (LMW) phthalates [
4]. HMW phthalates, such as di-(2-ethylhexyl) phthalate (DEHP), di-n-octyl phthalate (DOP), di-isononyl phthalate (DiNP), and butyl benzyl phthalate (BBzP), mainly function as plasticizers in plastics products, food containers, children’s toys, building materials, and medical devices (e.g., medical tubing, blood and intravenous bags, dialysis machines, and disposable surgical gloves) [
5,
6,
7]. LMW phthalates, such as di-butyl phthalate (DBP), di-isobutyl phthalates (DiBP), di-ethyl phthalate (DEP), and di-methyl phthalate (DMP), are widely used as additives in personal care products (e.g., cosmetics, lotions, and perfumes), medications and dietary supplements [
8,
9] and pesticide [
10]. In this way, it is important to notice that due to the fact that phthalates are usually physically, rather than chemically, added to the above daily products. The ease release of phthalates into the environment results in pervasive human exposure to environmental phthalates through digestive tract ingestion (dietary intake or indoor dust ingestion) [
11,
12], inhalation [
13,
14], and percutaneous absorption (by personal care products) directly or indirectly. The phenomenon occurs because phthalates are usually physically, rather than chemically, added to the above daily products.
BPA is an alkylphenol organic compound whose structure consists of two phenol functional groups connected by two carbon-containing methyl groups [
15]. BPA is extensively used in epoxy resins and polycarbonate plastics, and shares some common sources of exposure with phthalates. A range of consumer products that contain BPA can release hazardous pollutants under high temperature, strong acid, or other certain conditions. For example, a previous study has tested that the migration of BPA from polycarbonate plastics into the food occurred at 70 °C [
16], and this occurrence is consequently considered as a potential chronic threat to human health [
17,
18].
In fact, a number of EDCs have been increasingly reported to be linked with human health problems especially female reproductive disorders in recent years [
19]. Results from several literature indicated that BPA and phthalates played negative roles in thyroid function on the basis of different thyroid hormone levels [
20,
21]. In addition, two cross-sectional studies have found positive relationship between BPA and the phthalate metabolite mono-ethyl phthalate (MEP) and precocious puberty in Thai girls [
22,
23]. Some other epidemiologic studies have focused on the higher BPA level in women with polycystic ovarian syndrome (PCOS) [
24,
25] and the consistent conclusion can be also found in adolescents [
26]. In addition, various cell cultures [
27], animal models [
28], and human epidemiologic data have supplied evidences that phthalates may change the endometrial environment or are possibly associated with endometriosis [
29]. One recent study has described that BPA exposure may affect the expression of key severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection mediators such as angiotensin-converting enzyme 2 (ACE2), transmembrane serine protease 2 (TMPRSS2), and furin in human tissues. Thus, the BPA exposure may have relevant effects on the risk of severe COVID-19 [
30]. Furthermore, BPA and phthalates—as oestrogen-mimicking EDCs—are thought to be responsible for inducing the occurrence and progression of many oestrogen-dependent cancers by binding to oestrogenic receptors, which are important evolution-related transcription factors related to many critical biological processes. Such actions probably play a considerable role in human breast carcinogenesis [
19,
31]. Amongst the multitudinous hormone-dependent cancers related to BPA and phthalates exposure, breast cancer is the most important issue that should be placed more attention.
Breast cancer is the most frequent cancer and the second leading cause of cancer death amongst American women [
32] and accounts for almost a quarter of all types of cancer in women worldwide. The incidence of breast cancer is on the rise in many countries over the last few decades [
33]. Over time, emerging literature from laboratory works and human epidemiological studies have focused on the relationship of BPA and phthalates exposure with breast cancer [
34,
35,
36]. However, the results still remain inconsistent although several recent laboratory findings have supplied valuable evidence that BPA or di(2-ethylhexyl) phthalate (DEHP) exposure is responsible for the development and progression of breast cancer [
17,
37]. An Alaska case-control study has revealed that the phthalate metabolite MEHP was associated with breast cancer [
38]. Similarly, another study has demonstrated the correlation between urinary MEP concentrations and increased breast cancer risk, whereas MBzP and mono(3-carboxypropyl) phthalate (MCPP) were negatively linked with breast cancer [
39]. However, in a recent study conducted in America, the researchers have not observed any relationship between phthalates or BPA and breast cancer [
40].
Therefore, given the controversial conclusion of current epidemiological studies, we aim to perform a meta-analysis to assess systematically the association of BPA and eight phthalate metabolites, including mono-benzyl phthalate (MBzP), mono-ethyl phthalate (MEP), mono-(2-ethyl-5-hydroxyhexyl) phthalate (MEHHP), mono-2-ethylhexyl phthalate (MEHP), mono-(2-ethyl-5-oxohexyl) phthalate (MEOHP), mono (3-carboxypropyl) phthalate (MCPP), mono-butyl phthalate (MBP), and mono-2-isobutyl phthalate (MiBP) with the risk of breast cancer.
4. Discussion
The widespread sources of exposure to BPA and phthalates are unavoidable and unintentional in daily life. Moreover, BPA and phthalates all exist as immanent EDCs that play a major role in adverse reproductive system damages [
49,
50,
51], metabolic disorders [
52], grip strength [
53], and hormone-sensitive cancers [
54,
55] in males and females. Previous studies have shown that exposure during preconception and prenatal stages may cause adverse health consequences for pregnant women and their offspring [
18,
56,
57,
58]. An earlier review includes examples that showing how several EDCs are identified and affect the development of mammary glands in animal models [
59]. Fabiana and Kalpana’s recent studies conducted in rat models report that exposure to low-dose diethyl phthalate (DEP) and phenol at critical windows lead to changes in histology and transcriptome in rat mammary glands [
60,
61]. However, very few epidemiological studies are conducted on the correlation between certain EDCs, especially BPA and phthalates and human breast cancer risk. Some studies have even yielded inconsistent results.
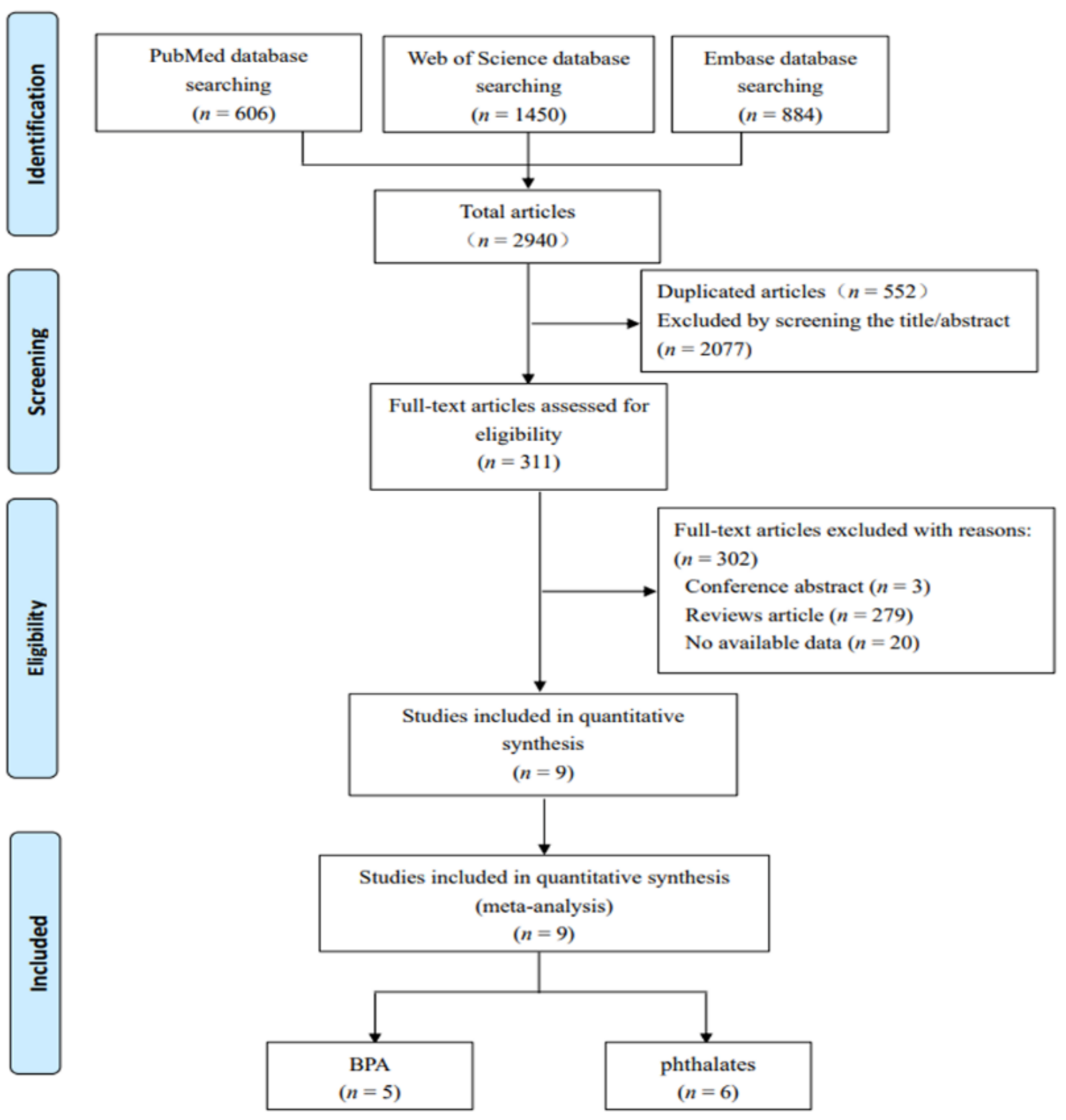
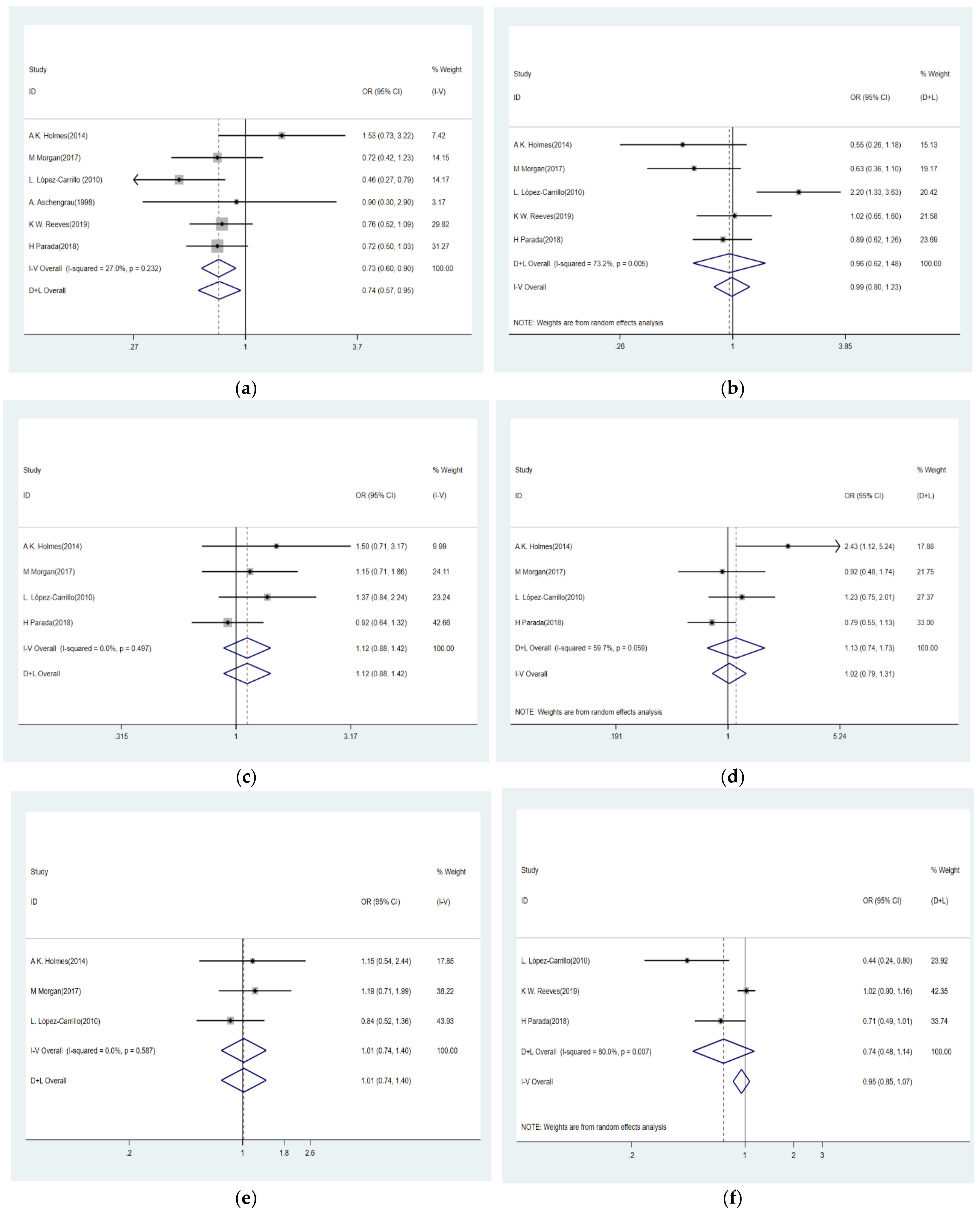
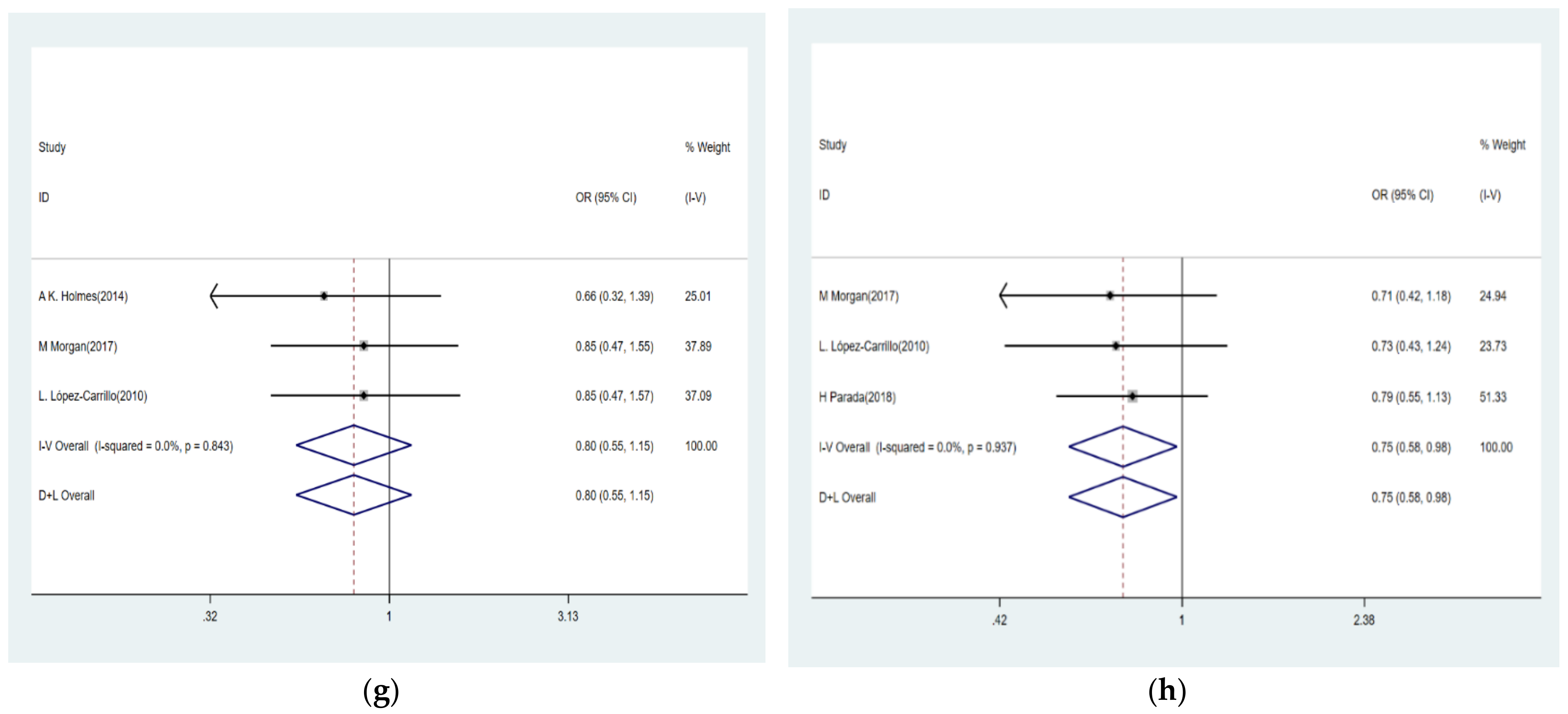
Therefore, we conducted an updated meta-analysis by extracting and summarizing the data from nine selected case-control studies, which involves 7820 participants across four different countries, to assess the relationship of BPA and eight phthalate metabolites with the risk of breast cancer accurately and comprehensively. We found that only phthalate metabolites MBzP and MiBP were passively associated with breast cancer risk. One of the possible mechanisms leading to the negative relationship is the ability of MBzP to activate human peroxisome proliferator-activated receptor (PPAR) α and γ [
62], and the ligand activation of PPARγ is relative to adipocyte differentiation, lipid accumulation, and decreased growth of breast cancer cell [
63,
64]. Another potential speculation is that phthalates metabolites are related to increased intron 1 methylation level and upregulated disintegrin and metalloproteinase domain 33 (ADAM33) expression, which play an important role in reducing breast cancer risk [
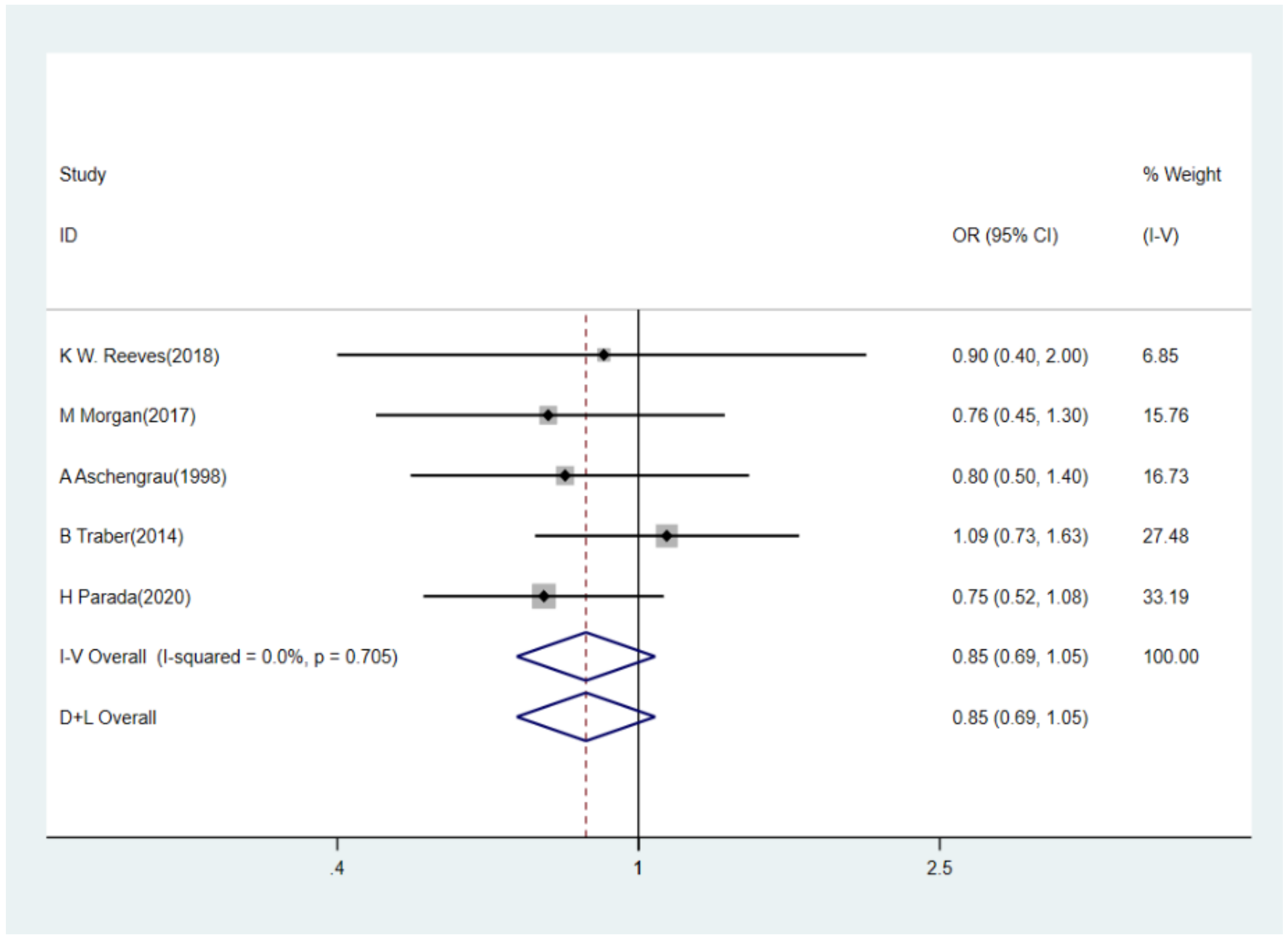
35]. Besides, results did not provide sufficient evidence of the correlations of BPA and other phthalate metabolites MEP, MEHHP, MEHP, MEOHP, MCPP, and MBP with breast cancer. However, when we conducted subgroup analyses, a marginally negative association between BPA exposure and breast cancer risk was observed in America but not in Non-America; for MCPP, we found a negative association in Non-America and general population subgroups and for MBzP, the passive association between urinary MBzP and breast cancer remained in subgroups of America and general population controls. These results proved that the correlation was influenced by region and control selection, which might partly contribute to different sources or levels of BPA and phthalates exposure in different countries and control populations. The subgroup analyses for MEP, MEHHP, MEHP, MBP, and MEOHP did not reveal any significant result. Additionally, the results of sensitivity analysis suggested that the results of our meta-analysis were relatively stable, except that the conclusion was reversed after the removal of the study of K W. Reeves (2019) [
47] study in the correlation analysis for MCPP and breast cancer. One possible explanation was that the subjects of the study were recruited from postmenopausal women, which was different from two other studies. Finally, regional diversity, age differences, different detection methods, the limit of detection (LOD) and concentration classification methods for EDCs, and adjusted models produced heterogeneity to some extent and affected the data merging.
Our study had some advantages. Firstly, this study was the first meta-analysis to evaluate systematically the relationship of exposure to BPA and eight specific phthalate metabolites with breast cancer risk across four different countries to date. Secondly, we also discovered the potential sources of heterogeneity according to leaving a study each time in the sensitivity analysis. Finally, we performed the subgroup analyses by region (i.e., America and Non-America) and sources of control (i.e., clinical medical center and general population), which further verified the relationship between selected EDCs and breast cancer risk.
Our research also had several limitations. Firstly, the meta-analysis was based on relatively insufficient number of studies so that only one study was included in a certain subgroup analysis. Secondly, the sensitivity analysis suggested the presence of heterogeneity, and some of the results were not stable. In this sense, well-conducted epidemiological studies on the relationship of BPA and various phthalate metabolites with breast cancer are needed to reinforce our research results. Thirdly, although urine concentrations of BPA and phthalate metabolites are the most common methods to assess human BPA and phthalates exposures, some potential factors such as the relatively short biological half-life of above EDCs, the changes of subjects’ lifestyle after breast cancer diagnosis, the nature of retrospective case-control study, breast cancer itself, and the treatments or surgery are all likely to affect the measurement of EDCs exposure. Therefore, the time of urine collection, the inconsistency of the assessment and classification of exposure levels of the same EDCs in different original articles and the evaluation of long-term exposure based on short-term biomarker levels measured in urine led to a degree of bias. More sensitive and accurate biomarkers and better designed studies are needed to explore this possible effect in the future.







{kind=link}
{kind=link}
{kind=link}
{kind=link}