
Spatio-Temporal Dynamics of Plasmodium falciparum and Plasmodium vivax in French Guiana: 2005–2019

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Area
2.3. Case Definition
2.4. Meteorological Data
2.5. Statistical Analyses
2.6. Legal and Ethical Considerations
3. Results
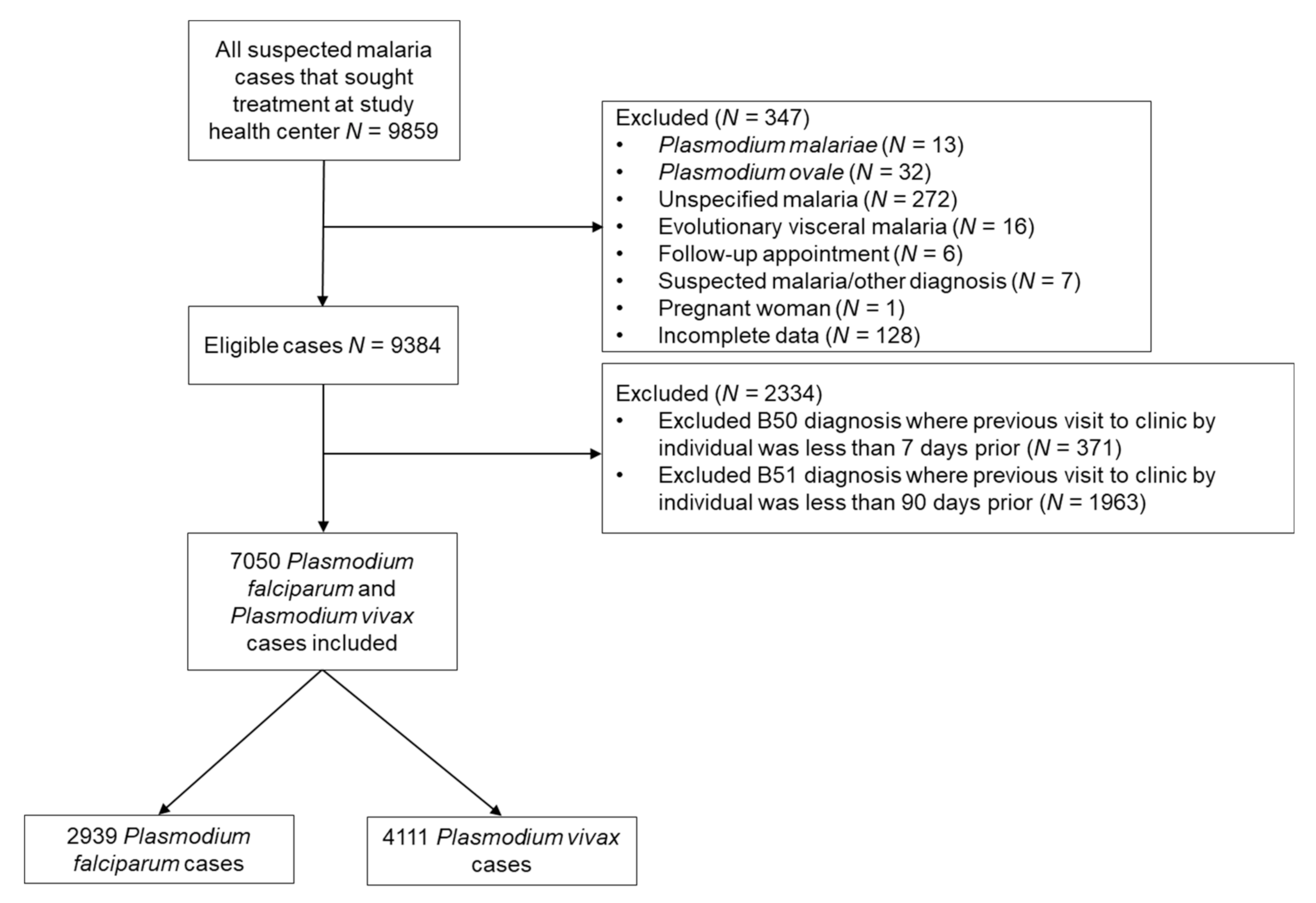
3.1. Study Population
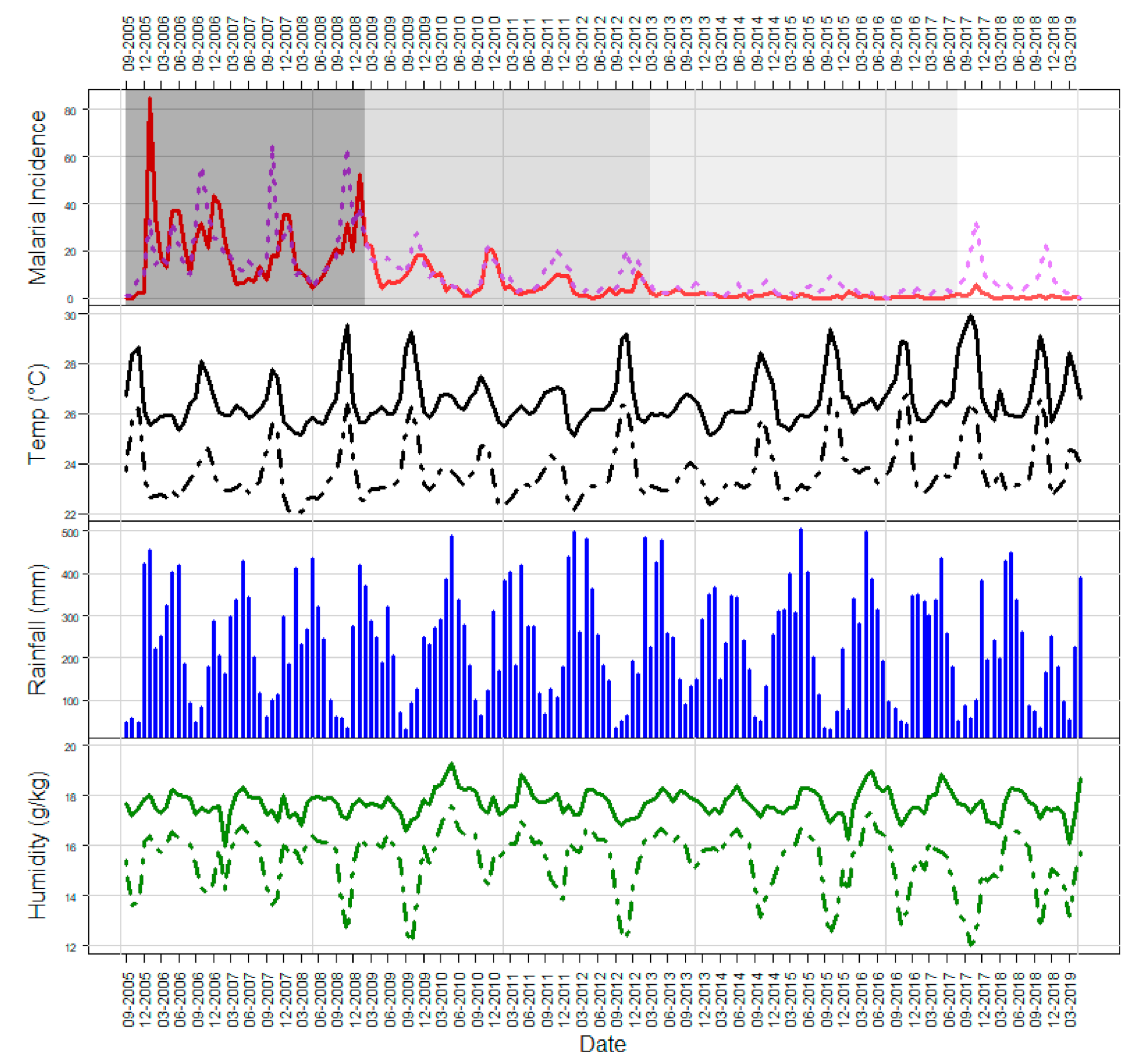
3.2. Overview of the Time Series
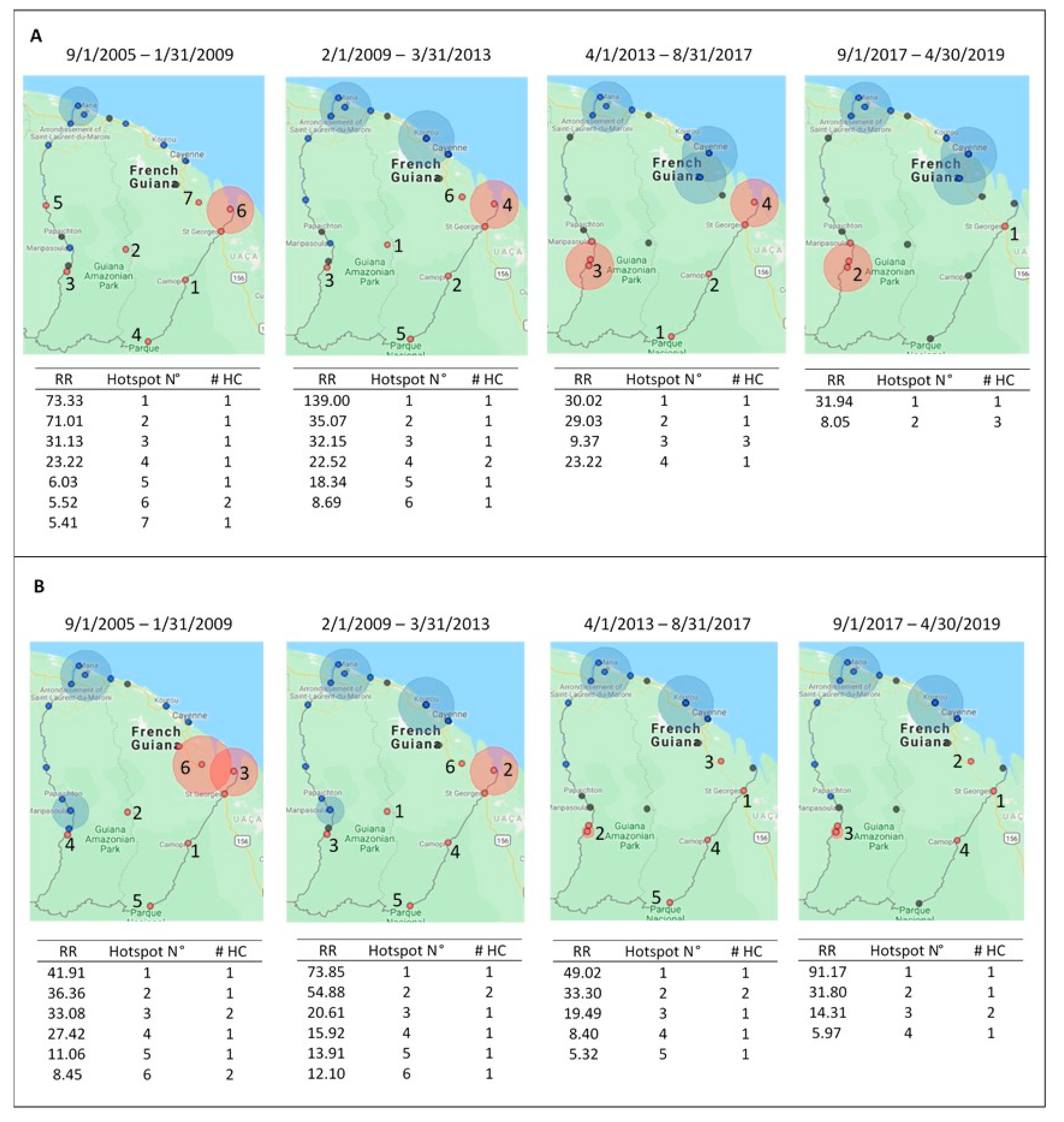
3.3. Malaria Transmission Periods
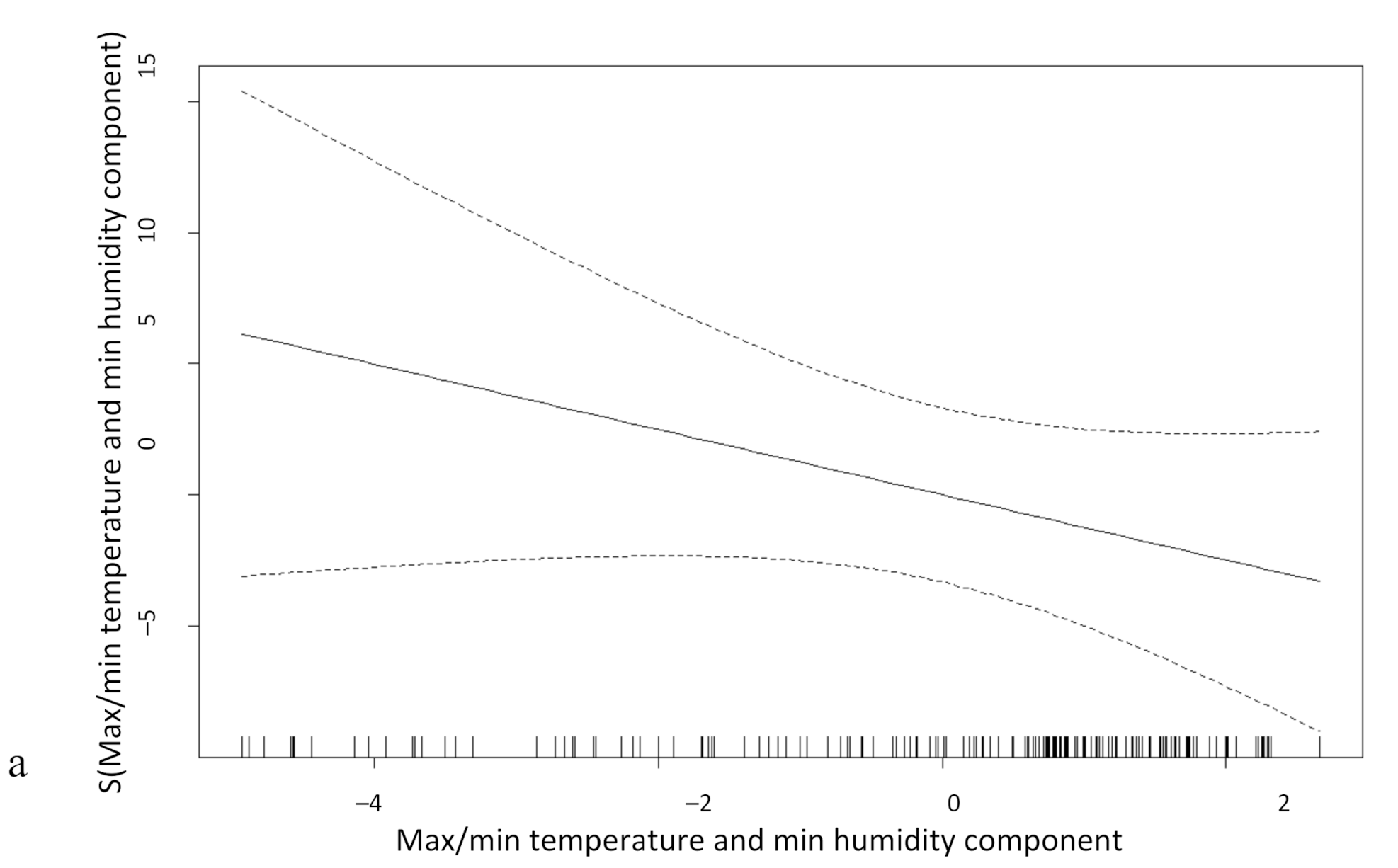
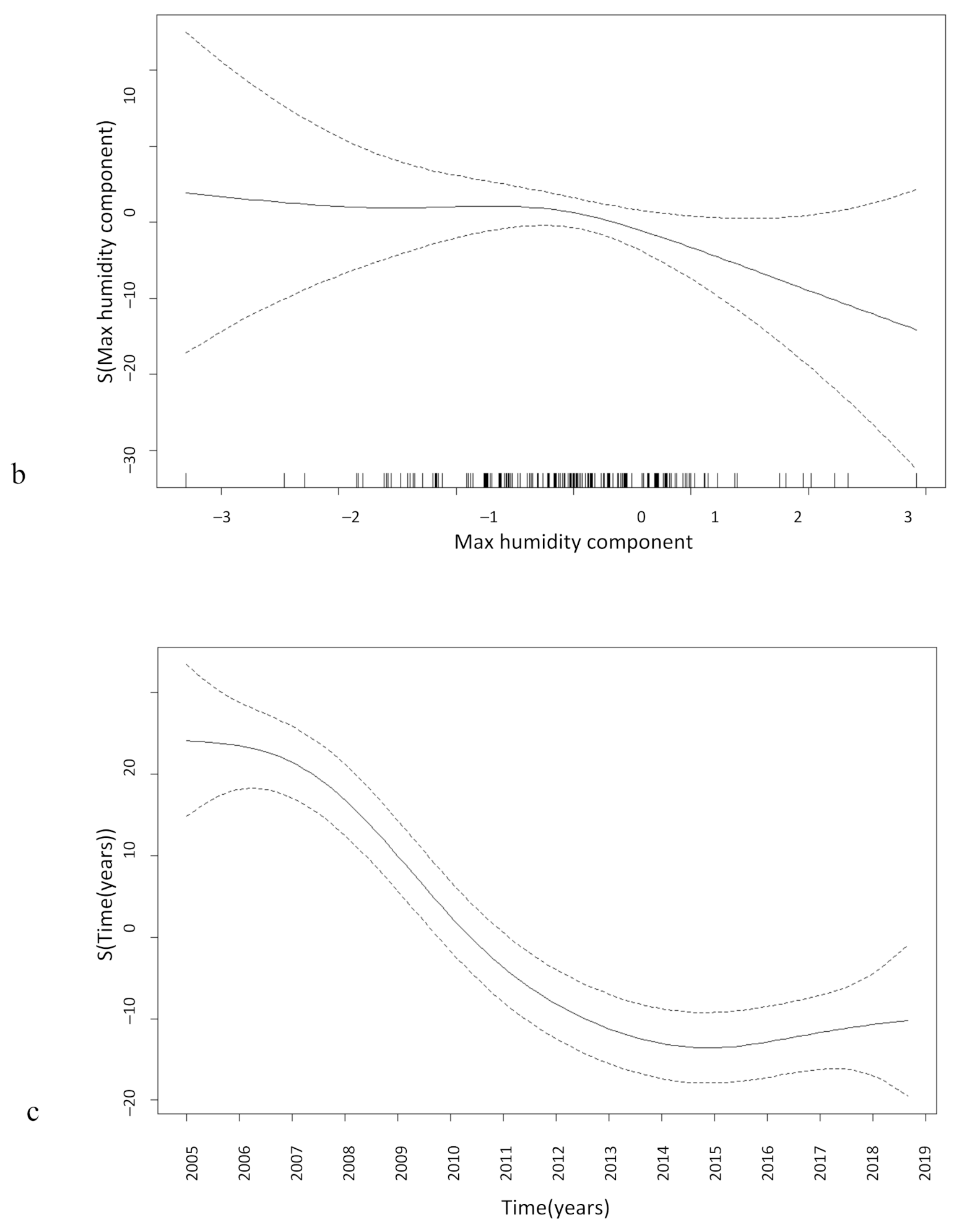
3.4. Meteorological Data and Malaria Incidence Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Malaria Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Institut National de la Statistique et des Études Économiques (INSEE). National Institute of Statistics and Economic Studies. Available online: https://www.insee.fr (accessed on 11 June 2019).
- Epelboin, Y.; Chaney, S.; Guidez, A.; Habchi-Hanriot, N.; Talaga, S.; Wang, L.; Dusfour, I. Successes and failures of sixty years of vector control in French Guiana. Mem. Inst. Oswaldo Cruz 2018, 113, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douine, M.; Musset, L.; Corlin, F.; Pelleau, S.; Pasquier, J.; Mutricy, L.; Adenis, A.; Djossou, F.; Brousse, P.; Perotti, F.; et al. Prevalence of Plasmodium spp. in illegal gold miners in French Guiana in 2015: A hidden but critical malaria reservoir. Malar. J. 2016, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanf, M.; Stephani, A.; Basurko, C.; Nacher, M.; Carme, B. Determination of the Plasmodium vivax relapse pattern in Camopi, French Guiana. Malar. J. 2009, 8, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosnier, E.; Roux, E.; Cropet, C.; Lazrek, Y.; Moriceau, O.; Gaillet, M.; Mathieu, L.; Nacher, M.; Demar, M.; Odonne, G.; et al. Prevalence of Plasmodium spp. in the Amazonian Border Context (French Guiana–Brazil): Associated factors and spatial distribution. Am. J. Trop. Med. Hyg. 2020, 102, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Pommier de Santi, V.P.; Dia, A.; Adde, A.; Hyvert, G.; Galant, J.; Mazevet, M.; Nguyen, C.; Vezenegho, S.; Dusfour, I.; Girod, R.; et al. Malaria in French Guiana linked to illegal gold mining. Emerg. Infect. Dis. 2016, 22, 344–346. [Google Scholar] [CrossRef] [Green Version]
- Reiner, R.C.; Geary, M.; Atkinson, P.M.; Smith, D.L.; Gething, P.W. Seasonality of Plasmodium falciparum transmission: A systematic review. Malar. J. 2015, 14, 343. [Google Scholar] [CrossRef] [Green Version]
- Climate—French Guiana. Available online: https://www.climatestotravel.com/climate/french-guiana (accessed on 3 June 2019).
- Adde, A.; Roux, E.; Mangeas, M.; Dessay, N.; Nacher, M.; Dusfour, I.; Girod, R.; Briolant, S. Dynamical mapping of Anopheles darlingi densities in a residual malaria transmission area of French Guiana by using remote sensing and meteorological data. PLoS ONE 2016, 11, e0164685. [Google Scholar] [CrossRef]
- Adde, A.; Dusfour, I.; Roux, E.; Girod, R.; Briolant, S. Anopheles fauna of coastal Cayenne, French Guiana: Modelling and mapping of species presence using remotely sensed land cover data. Mem. Inst. Oswaldo Cruz 2016, 111, 750–756. [Google Scholar] [CrossRef]
- Roux, E.; Gaborit, P.; Romaña, C.A.; Girod, R.; Dessay, N.; Dusfour, I. Objective sampling design in a highly heterogeneous landscape—characterizing environmental determinants of malaria vector distribution in French Guiana, in the Amazonian region. BMC Ecol. 2013, 13, 45. [Google Scholar] [CrossRef] [Green Version]
- Chaves, L.S.M.; Conn, J.E.; López, R.V.M.; Sallum, M.A.M. Abundance of impacted forest patches less than 5 km2 is a key driver of the incidence of malaria in Amazonian Brazil. Sci. Rep. 2018, 8, 7077. [Google Scholar] [CrossRef]
- Souza, P.F.; Xavier, D.R.; Suarez Mutis, M.C.; da Mota, J.C.; Peiter, P.C.; de Matos, V.P.; de Avelar Figueiredo Mafra Magalhães, M.; Barcellos, C. Spatial spread of malaria and economic frontier expansion in the Brazilian Amazon. PLoS ONE 2019, 14, e0217615. [Google Scholar] [CrossRef] [PubMed]
- Gaudart, J.; Poudiougou, B.; Dicko, A.; Ranque, S.; Toure, O.; Sagara, I.; Diallo, M.; Diawara, S.; Ouattara, A.; Diakite, M.; et al. Space-time clustering of childhood malaria at the household level: A dynamic cohort in a Mali village. BMC Public Health 2006, 6, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, D.I.; Gething, P.W.; Kabaria, C.W.; Temperley, W.H.; Noor, A.M.; Okiro, E.A.; Shanks, G.D.; Snow, R.W.; Hay, S.I. Temperature and malaria trends in highland East Africa. PLoS ONE 2011, 6, e24524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okunlola, O.A.; Oyeyemi, O.T. Spatio-temporal analysis of association between incidence of malaria and environmental predictors of malaria transmission in Nigeria. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amy McNally NASA; GSFC; HSL. FLDAS Noah Land Surface Model L4 Global Monthly 0.1 × 0.1 Degree (MERRA-2 and CHIRPS); Goddard Earth Sciences Data and Information Services Center (GES DISC): Greenbelt, MD, USA, 2018. [Google Scholar] [CrossRef]
- Huffman, G.J.; Stocker, E.F.; Bolvin, D.T.; Nelkin, E.J.; Tan, J. GPM IMERG Final Precipitation L3 1 Month 0.1 Degree × 0.1 Degree V06; Goddard Earth Sciences Data and Information Services Center (GES DISC): Greenbelt, MD, USA, 2019. [Google Scholar] [CrossRef]
- Messagier, A.L.; Blaizot, R.; Couppié, P.; Delaigue, S. Teledermatology use in remote areas of French Guiana: Experience from a long-running system. Front. Public Health 2019, 7, 387. [Google Scholar] [CrossRef]
- Guyane. Available online: https://www.guyane.ars.sante.fr/ (accessed on 4 November 2020).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Hiwat, H.; Hardjopawiro, L.S.; Takken, W.; Villegas, L. Novel strategies lead to pre-elimination of malaria in previously high-risk areas in Suriname, South America. Malar. J. 2012, 11. [Google Scholar] [CrossRef] [Green Version]
- Plan de lute Contre le Paludisme en Guyane. Controle du Paludisme sur L’ensemble du Territoire 2015–2018; Agence Regionale de Sante Guyane: Cayenne, French Guiana, 2015. [Google Scholar]
- Douine, M.; Mosnier, E.; Le Hingrat, Q.; Charpentier, C.; Corlin, F.; Hureau, L.; Adenis, A.; Lazrek, Y.; Niemetsky, F.; Aucouturier, A.; et al. Illegal gold miners in French Guiana: A neglected population with poor health. BMC Public Health 2017, 18. [Google Scholar] [CrossRef] [Green Version]
- Douine, M.; Sanna, A.; Galindo, M.; Musset, L.; De Santi, V.P.; Marchesini, P.; Magalhaes, E.D.; Suarez-Mutis, M.; Hiwat, H.; Nacher, M.; et al. Malakit: An innovative pilot project to self-diagnose and self-treat malaria among illegal gold miners in the Guiana Shield. Malar. J. 2018, 17, 1–8. [Google Scholar] [CrossRef]
- Mosnier, E.; Dusfour, I.; Lacour, G.; Saldanha, R.; Guidez, A.; Gomes, M.S.; Sanna, A.; Epelboin, Y.; Restrepo, J.; Davy, D.; et al. Resurgence risk for malaria, characterization of a recent outbreak in a Amazonian border area—French Guiana/Brazil. BMC Infect. Dis. 2020. in review. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization. Epidemiological Alert: Increase of Malaria in the Americas; PAHO/WHO2018: Washington, DC, USA, 2018. [Google Scholar]
- Laneri, K.; Bhadra, A.; Ionides, E.L.; Bouma, M.; Dhiman, R.C.; Yadav, R.S.; Pascual, M. Forcing versus feedback: Epidemic malaria and monsoon rains in northwest India. PLoS Comput. Biol. 2010, 6, e1000898. [Google Scholar] [CrossRef] [PubMed]
- Odongo-Aginya, E.; Ssegwanyi, G.; Kategere, P.; Vuzi, P.C. Relationship between malaria infection intensity and rainfall pattern in Entebbe peninsula, Uganda. Afr. Health Sci. 2005, 5, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Krefis, A.C.; Schwarz, N.G.; Krüger, A.; Fobil, J.; Nkrumah, B.; Acquah, S.; Loag, W.; Sarpong, N.; Adu-Sarkodie, Y.; Ranft, U.; et al. Modeling the relationship between precipitation and malaria incidence in children from a holoendemic area in Ghana. Am. J. Trop. Med. Hyg. 2011, 84, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Christiansen-Jucht, C.; Parham, P.E.; Saddler, A.; Koella, J.C.; Basáñez, M.-G. Temperature during larval development and adult maintenance influences the survival of Anopheles gambiae s.s. Parasites Vectors 2014, 7, 489. [Google Scholar] [CrossRef]
- Abiodun, G.J.; Maharaj, R.; Witbooi, P.; Okosun, K.O. Modelling the influence of temperature and rainfall on the population dynamics of Anopheles arabiensis. Malar. J. 2016, 15, 364. [Google Scholar] [CrossRef] [Green Version]
- Adimi, F.; Soebiyanto, R.P.; Safi, N.; Kiang, R. Towards malaria risk prediction in Afghanistan using remote sensing. Malar. J. 2010, 9, 125. [Google Scholar] [CrossRef] [Green Version]
- Ouedraogo, B.; Inoue, Y.; Kambiré, A.; Sallah, K.; Dieng, S.; Tine, R.; Rouamba, T.; Herbreteau, V.; Sawadogo, Y.; Ouedraogo, L.S.L.W.; et al. Spatio-temporal dynamic of malaria in Ouagadougou, Burkina Faso, 2011–2015. Malar. J. 2018, 17, 138. [Google Scholar] [CrossRef] [Green Version]
- Mosnier, E.; Douine, M.; Epelboin, L.; Pelleau, S.; de Santi, V.P.; Dangel, Y.; Demar, M.; Mutricy, R.; Guarmit, B.; Nacher, M.; et al. Asymptomatic Plasmodium falciparum and vivax infection in the neighborhood of Blondin, Saint-Georges-de-l’Oyapock District, French Guiana. Bull. Soc. Pathol. Exot. (1990) 2017, 110, 265–269. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Center | September 2005–January 2009 | February 2009–March 2013 | April 2013–August 2017 | September 2017–April 2019 | ||||
|---|---|---|---|---|---|---|---|---|
| Pf per 1000 | Pv per 1000 | Pf per 1000 | Pv per 1000 | Pf per 1000 | Pv per 1000 | Pf per 1000 | Pv per 1000 | |
| Apatou | 5.44 | 0.18 | 0.29 | 0.29 | 0.2 | 0 | 0 | 0 |
| Antecume Pata | 403 | 372.9 | 153.1 | 146.6 | 2.5 | 40.0 | 2.2 | 26.1 |
| Awala Yalimapo | 0 | 1.6 | 0 | 0.8 | 0 | 0 | 0 | 0 |
| Camopi | 574 | 420.1 | 131.9 | 102.1 | 13.4 | 17.4 | 1.6 | 12.3 |
| Cacao | 12.3 | 149.7 | 9.7 | 22.4 | 0 | 3.0 | 0 | 1.2 |
| Gran Santi | 71.8 | 2.7 | 0.4 | 0.7 | 0.3 | 0.4 | 0 | 0.1 |
| Iracoubo | 0 | 0 | 0 | 1.0 | 0 | 0 | 0 | 0.6 |
| Javouney | 3.6 | 0.9 | 0 | 0 | 0 | 0.7 | 0 | 0 |
| Maripa-Soula | 5.5 | 2.4 | 2.8 | 2.3 | 3.5 | 3.8 | 1.0 | 1.8 |
| Organabo | 4.4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ouanary | 46.2 | 246.2 | 82.6 | 128.4 | 16.5 | 0 | 0 | 0 |
| Papaїchton | 12.2 | 2.6 | 5.8 | 2.9 | 0.6 | 1.7 | 0.1 | 0.1 |
| Régina | 71.4 | 70.2 | 42.0 | 84.0 | 1.1 | 39.5 | 1.1 | 60.2 |
| Saül | 897 | 496.8 | 620.9 | 509.8 | 13.3 | 6.6 | 0 | 20.0 |
| Saint Georges de l’Oyapock | 67.3 | 256.0 | 73.9 | 175.4 | 2.9 | 52.5 | 3.9 | 67.6 |
| Trois Sauts | 28 | 150.7 | 86.6 | 97.6 | 15.9 | 11.6 | 2.8 | 7.0 |
| Taluen | 0 | 0 | 0 | 15.6 | 0 | 108.0 | 0 | 34.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scully, J.; Mosnier, E.; Carbunar, A.; Roux, E.; Djossou, F.; Garçeran, N.; Musset, L.; Sanna, A.; Demar, M.; Nacher, M.; et al. Spatio-Temporal Dynamics of Plasmodium falciparum and Plasmodium vivax in French Guiana: 2005–2019. Int. J. Environ. Res. Public Health 2021, 18, 1077. https://doi.org/10.3390/ijerph18031077
Scully J, Mosnier E, Carbunar A, Roux E, Djossou F, Garçeran N, Musset L, Sanna A, Demar M, Nacher M, et al. Spatio-Temporal Dynamics of Plasmodium falciparum and Plasmodium vivax in French Guiana: 2005–2019. International Journal of Environmental Research and Public Health. 2021; 18(3):1077. https://doi.org/10.3390/ijerph18031077
Chicago/Turabian StyleScully, Jenna, Emilie Mosnier, Aurel Carbunar, Emmanuel Roux, Félix Djossou, Nicolas Garçeran, Lise Musset, Alice Sanna, Magalie Demar, Mathieu Nacher, and et al. 2021. "Spatio-Temporal Dynamics of Plasmodium falciparum and Plasmodium vivax in French Guiana: 2005–2019" International Journal of Environmental Research and Public Health 18, no. 3: 1077. https://doi.org/10.3390/ijerph18031077