Cervical Cancer Screening Participation among Women of Russian, Somali, and Kurdish Origin Compared with the General Finnish Population: A Register-Based Study

 ,
,
Abstract
:
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Data Sources and Variables
2.3. Study Outcomes
2.4. Variable Definitions
2.5. Statistical Analyses
2.6. Ethical Considerations
3. Results
3.1. Characteristics
3.2. Screening Participation in the Age-Adjusted Analysis
3.3. Screening Participation in the Multiple-Adjusted Analysis
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Research Data
References
- WHO. Screening for Cervical Cancer. Available online: http://www.who.int/reproductivehealth/topics/cancers/fight-cervical-cancer/en/ (accessed on 6 June 2020).
- Landy, R.; Pesola, F.; Castañón, A.; Sasieni, P. Impact of cervical screening on cervical cancer mortality: Estimation using stage-specific results from a nested case–control study. Br. J. Cancer 2016, 115, 1140–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; Franceschi, S.; Zaridze, D.; Poljak, M.; Veerus, P.; Plummer, M.; Bray, F. Preventable fractions of cervical cancer via effective screening in six Baltic, central, and eastern European countries 2017–40: A population-based study. Lancet Oncol. 2016, 17, 1445–1452. [Google Scholar] [CrossRef] [Green Version]
- Spence, A.R.; Alobaid, A.; Drouin, P.; Goggin, P.; Gilbert, L.; Provencher, D.; Tousignant, P.; Hanley, J.A.; Franco, E.L. Screening histories and contact with physicians as determinants of cervical cancer risk in Montreal, Quebec. Curr. Oncol. 2014, 21, 294–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Cervical Cancer. Available online: https://www.who.int/health-topics/cervical-cancer#tab=tab_1 (accessed on 23 May 2020).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altobelli, E.; Lattanzi, A. Cervical carcinoma in the European Union: An update on disease burden, screening program state of activation, and coverage as of March 2014. Int. J. Gynecol. Cancer 2015, 25, 474–483. [Google Scholar] [CrossRef]
- Lonnberg, S.; Nieminen, P.; Luostarinen, T.; Anttila, A. Mortality audit of the Finnish cervical cancer screening program. Int. J. Cancer 2013, 132, 2134–2140. [Google Scholar] [CrossRef]
- Dugue, P.; Lynge, E.; Rebolj, M. Mortality of non-participants in cervical screening: Register-based cohort study. Int. J. Cancer 2014, 134, 2674–2682. [Google Scholar] [CrossRef]
- Visioli, C.B.; Crocetti, E.; Zappa, M.; Iossa, A.; Andersson, K.L.; Bulgaresi, P.; Alfieri, A.; Amunni, G. Participation and Risk of High Grade Cytological Lesions Among Immigrants and Italian-Born Women in an Organized Cervical Cancer Screening Program in Central Italy. J. Immigr. Minor. Health 2015, 17, 670–678. [Google Scholar] [CrossRef]
- Gallo, F.; Caprioglio, A.; Castagno, R.; Ronco, G.; Segnan, N.; Giordano, L. Inequalities in cervical cancer screening utilisation and results: A comparison between Italian natives and immigrants from disadvantaged countries. Health Policy 2017, 121, 1072–1078. [Google Scholar] [CrossRef]
- Azerkan, F.; Sparen, P.; Sandin, S.; Tillgren, P.; Faxelid, E.; Zendehdel, K. Cervical screening participation and risk among Swedish-born and immigrant women in Sweden. Int. J. Cancer 2012, 30, 937–947. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, A.W.; de Nooijer, P.; Hop, W.C. Screening for cervical carcinoma: Participation and results for ethnic groups and socioeconomic status. Cancer Cytopathol. 2005, 105, 270–276. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM). World Migration Report 2018. Available online: https://publications.iom.int/system/files/pdf/wmr_2018_en.pdf (accessed on 12 June 2018).
- Statistics Finland. Numbers and Shares of Persons with Immigrant Background by Area 1990–2017. Available online: http://pxnet2.stat.fi/PXWeb/pxweb/en/Maahanmuuttajat_ja_kotoutuminen/Maahanmuuttajat_ja_kotoutuminen__Maahanmuuttajat_ja_kotoutuminen/007_ulkom_osuudet.px/ (accessed on 15 August 2019).
- WHO. How Health Systems Can Address Health Inequities Linked to Migration and Ethnicity. Available online: https://www.euro.who.int/data/assets/pdf_file/0005/127526/e94497.pdf (accessed on 12 March 2017).
- Simon, J.; Kiss, N.; Łaszewska, A.; Mayer, S. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Labour Migrants in the European Region; World Health Organisation Regional Office for Europe: København, Denmark, 2015; Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/289245/WHO-HENReport-A5-1-Labour-rev1.pdf?ua=1.2015 (accessed on 1 May 2018).
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Puchner, K.; Karamagioli, E.; Pikouli, A.; Tsiamis, C.; Kalogeropoulos, A.; Kakalou, E.; Pavlidou, E.; Pikoulis, E. Time to rethink refugee and migrant health in Europe: Moving from emergency response to integrated and individualized health care provision for migrants and refugees. Int. J. Environ. Res. Public Health 2018, 15, 1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idehen, E.E.; Koponen, P.; Härkänen, T.; Kangasniemi, M.; Pietilä, A.-M.; Korhonen, T. Disparities in cervical screening participation: A comparison of Russian, Somali and Kurdish immigrants with the general Finnish population. Int. J. Equity Health 2018, 17, 56. [Google Scholar] [CrossRef] [Green Version]
- Idehen, E.E.; Korhonen, T.; Castaneda, A.; Juntunen, T.; Kangasniemi, M.; Pietilä, A.-M.; Koponen, P. Factors associated with cervical cancer screening participation among immigrants of Russian, Somali and Kurdish origin: A population-based study in Finland. BMC Women’s Health 2017, 17, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertzum-Larsen, R.; Kjær, S.K.; Frederiksen, K.; Thomsen, L.T. Participation in cervical cancer screening among immigrants and Danish-born women in Denmark. Prev. Med. 2019, 123, 55–64. [Google Scholar] [CrossRef]
- Brzoska, P.; Aksakal, T.; Yilmaz-Aslan, Y. Utilization of cervical cancer screening among migrants and non-migrants in Germany: Results from a large-scale population survey. BMC Public Health 2020, 20, 5. [Google Scholar] [CrossRef] [PubMed]
- Marlow, L.A.V.; Wardle, J.; Walle, J. Understanding cervical screening non-attendance among ethnic minority women in England. Br. J. Cancer 2015, 113, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leinonen, M.K.; Campbell, S.; Ursin, G.; Tropé, A.; Nygård, M. Barriers to cervical cancer screening faced by immigrants: A registry-based study of 1.4 million women in Norway. Eur. J. Public Health 2017, 27, 873–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crampe-Casnabet, C.; Franck, J.; Ringa, V.; Coeuret-Pellicer, M.; Chauvin, P.; Menvielle, G. Role of obesity in differences in cervical cancer screening rates by migration history. The CONSTANCES survey. Cancer Epidemiol. 2019, 58, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Downs, L.S.; Smith, J.S.; Scarinci, I.; Flowers, L.; Parham, G. The disparity of cervical cancer in diverse populations. Gynecol. Oncol. 2008, 109, S22–S30. [Google Scholar] [CrossRef]
- Leinonen, M.K.; Campbell, S.; Klungsøyr, O.; Lönnberg, S.; Hansen, B.T.; Nygård, M. Personal and provider level factors influence participation to cervical cancer screening: A retrospective register-based study of 1.3 million women in Norway. Prev. Med. 2017, 94, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Olesen, S.C.; Butterworth, P.; Jacomb, P.; Tait, R.J. Personal factors influence use of cervical cancer screening services: Epidemiological survey and linked administrative data address the limitations of previous research. Health Serv. Res. 2012, 12, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idehen, E.; Pietilä, A.-M.; Kangasniemi, M. Barriers and Facilitators to Cervical Screening among Migrant Women of African Origin: A Qualitative Study in Finland. Int. J. Environ. Res. Public Health 2020, 17, 7473. [Google Scholar] [CrossRef] [PubMed]
- Hulme, J.; Moravac, C.; Ahmad, F.; Cleverly, S.; Lofters, A.; Ginsburg, O.; Dunn, S. “I want to save my life”: Conceptions of cervical and breast cancer screening among urban immigrant women of South Asian and Chinese origin. BMC Public Health 2016, 16, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, H.; Sherman, S.M.; Tincello, D.; Moss, E.L. Awareness of and attitudes towards cervical cancer prevention among migrant Eastern European women in England. J. Med. Screen. 2020, 27, 40–47. [Google Scholar] [CrossRef]
- Adunlin, G.; Cyrus, J.W.; Asare, M.; Sabik, L.M. Barriers and facilitators to breast and cervical cancer screening among immigrants in the United States. J. Immigr. Minor. Health 2019, 21, 606–658. [Google Scholar] [CrossRef]
- Poudel, K.; Sumi, N. Analyzing Awareness on Risk Factors, Barriers and Prevention of Cervical Cancer among Pairs of Nepali High School Students and Their Mothers. Int. J. Environ. Res. Public Health 2019, 16, 4382. [Google Scholar] [CrossRef] [Green Version]
- Gele, A.A.; Qureshi, S.A.; Kour, P.; Kumar, B.; Diaz, E. Barriers and facilitators to cervical cancer screening among Pakistani and Somali immigrant women in Oslo: A qualitative study. Int. J. Women’s Health 2017, 9, 487–496. [Google Scholar] [CrossRef] [Green Version]
- Marlow, L.; McBride, E.; Varnes, L.; Waller, J. Barriers to cervical screening among older women from hard-to-reach groups: A qualitative study in England. BMC Women’s Health 2019, 19, 38. [Google Scholar] [CrossRef]
- Ekechi, C.; Olaitan, A.; Ellis, R.; Koris, J.; Amajuoyi, A.; Marlow, L.A.V. Knowledge of cervical cancer and attendance at cervical cancer screening: A survey of Black women in London. BMC Public Health 2014, 14, 1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addawe, M.A.; Mburu, C.; Madar, A.A. Barriers to cervical cancer screening: A qualitative study among Somali women in Oslo Norway. Health Prim. Care 2018, 2, 1–5. [Google Scholar] [CrossRef]
- Salad, J.; Verdonk, P.; de Boer, F.; Abma, T.A. “A Somali girl is Muslim and does not have premarital sex. Is vaccination really necessary?” A qualitative study into the perceptions of Somali women in the Netherlands about the prevention of cervical cancer. Int. J. Equity Health 2015, 14, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, M.Z.; Hughes, T.L.; Sommers, M.S.; Hanlon, A.; Meghani, S.H. Association of pregnancy history and cervical cancer screening in a community sample of sexual minority women. J. Women’s Health 2019, 28, 526–534. [Google Scholar] [CrossRef]
- Grange, G.; Malvy, D.; Lancon, F.; Gaudin, A.; El Hasnaoui, A. Factors associated with regular cervical cancer screening. Int. J. Gynaecol. Obstet. 2008, 102, 28–33. [Google Scholar] [CrossRef]
- Cerigo, H.; Coutlee, F.; Franco, E.L.; Brassard, P. Factors associated with cervical cancer screening uptake among Inuit women in Nunavik, Quebec, Canada. BMC Public Health 2013, 13, 438. [Google Scholar] [CrossRef] [Green Version]
- Lofters, A.K.; Moineddin, R.; Hwang, S.W.; Glazier, R.H. Predictors of low cervical cancer screening among immigrant women in Ontario, Canada. BMC Women’s Health 2011, 11, 20. [Google Scholar] [CrossRef] [Green Version]
- Finnish Cancer Registry. Screening Statistics. 2020. Available online: https://cancerregistry.fi/statistics/screening-statistics/ (accessed on 19 October 2020).
- Salo, H.; Nieminen, P.; Kilpi, T.; Auranen, K.; Leino, T.; Vänskä, S.; Tiihonen, P.; Lehtinen, M.; Anttila, A. Divergent coverage, frequency and costs of organised and opportunistic Pap testing in Finland. Int. J. Cancer 2014, 135, 204–213. [Google Scholar] [CrossRef]
- Pankakoski, M.; Heinävaara, S.; Anttila, A.; Sarkeala, T. Differences in cervical test coverage by age, socioeconomic status, ethnic origin and municipality type–A nationwide register-based study. Prev. Med. 2020, 139, 106219. [Google Scholar] [CrossRef]
- Virtanen, A.; Anttila, A.; Luostarinen, T.; Malila, N.; Nieminen, P. Improving cervical cancer screening attendance in F inland. Int. J. Cancer 2015, 1, E677–E684. [Google Scholar] [CrossRef]
- Virtanen, A.; Anttila, A.; Luostarinen, T.; Nieminen, P. Self-sampling versus reminder letter: Effects on cervical cancer screening attendance and coverage in Finland. Int. J. Cancer 2011, 128, 2681–2687. [Google Scholar] [CrossRef]
- Castaneda, A.; Rask, S.; Härkänen, T.; Juntunen, T.; Skogberg, N.; Mölsä, M.; Tolonen, H.; Koskinen, S.; Koponen, P. Enhancing Survey Participation among Foreign-Born Populations. Finn. Yearb. Popul. Res. 2018, 53, 89–110. Available online: https://journal.fi/fypr (accessed on 5 June 2019). [CrossRef] [Green Version]
- Lundqvist, A.; Mäki-Opas, T. Health 2011 Survey–Methods. National Institute for Health and Welfare, Report 58-6. 2016. Available online: http://urn.fi/URN:ISBN:978-952-302-669-8,8/2016 (accessed on 5 June 2019).
- Population Finland. Population Information System. Available online: https://vrk.fi/en/population-information-system (accessed on 5 June 2019).
- Finnish Cancer Registry. Mass Screening-Cervical Cancer Screening. Available online: https://cancerregistry.fi/research/research-themes/cervical-cancer-screening/ (accessed on 5 June 2019).
- Finnish Institute for Health & Welfare. Care Register for Health Care. Available online: https://thl.fi/en/web/thlfi-en/statistics/information-on-statistics/register-descriptions/care-register-for-health-care (accessed on 5 June 2019).
- Finnish Institute for Health & Welfare. Medical Birth Register. Available online: https://thl.fi/en/web/thlfi-en/statistics/information-on-statistics/register-descriptions/newborns (accessed on 5 June 2019).
- Finnish Institute for Health & Welfare. Description of Statistics-New-Born. Available online: https://thl.fi/en/web/thlfi-en/statistics/information-on-statistics/description-of-statistics/newborns (accessed on 5 June 2019).
- Statistics Finland. Statistics. Available online: https://www.stat.fi/til/index_en.html (accessed on 5 June 2019).
- The Social Insurance Institution of Finland (Kela). Statistics by Topic. Available online: https://www.kela.fi/web/en/statistics-by-topic (accessed on 5 June 2019).
- Population Finland. Personal Identity Code. Available online: https://vrk.fi/en/personal-identity-code1 (accessed on 5 June 2019).
- Research Triangle Institute: SUDAAN Language Manual, Volumes 1 and 2, Release 11; Research Triangle Institute: Research Triangle Park, NC, USA, 2012.
- Akaike, H. Information theory as an extension of the maximum likelihood principle. In Second International Symposium on Information Theory; Csáki, F., Petrov, B.N., Eds.; BNPBF Csaki Budapest Akademiai Kiado: Budapest, Hungary, 1973; pp. 267–281. [Google Scholar]
- Graubard, B.; Korn, E. Predictive margins with survey data. Biometrics 1999, 55, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, R.; Pahkinen, E. Practical Methods for Design and Analyses of Complex Surveys, 2nd ed.; John Wiley and Sons: Chichester, UK, 2004. [Google Scholar]
- Regulation GDP. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data and repealing Directive 95/46. J. Eur. Union 2016, 59, 294. [Google Scholar]
- Moen, K.A.; Kumar, B.; Qureshi, S.; Diaz, E. Differences in cervical cancer screening between immigrants and nonimmigrants in Norway: A primary healthcare register-based study. Eur. J. Cancer Prev. 2017, 26, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Finnish Ministry of Social Affairs and Health. Health Services. Available online: http://stm.fi/en/health-services (accessed on 9 September 2017).
- Team, V.; Manderson, L.H.; Markovic, M. From state care to self-care: Cancer screening behaviours among Russian-speaking Australian women. Aust. J. Prim. Health 2013, 19, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Carballo, M.; Nerukar, A. Migration, refugees, and health risks. Emerg Infect Dis. 2001, 7 (Suppl. S3), 556–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sanjosé, S.; Serrano, B.; Castellsagué, X.; Brotons, M.; Muñoz, J.; Bruni, L.; Bosch, F.X. Human papillomavirus (HPV) and related cancers in the global Alliance for vaccines and immunization (GAVI) countries: A WHO/ICO HPV information Centre report. Vaccine 2012, 30 (Suppl. S4). [Google Scholar] [CrossRef]
- Anttila, A.; Nieminen, P. Cervical cancer screening programme in Finland with an example on implementing alternative screening methods. Coll. Antropol. 2007, 31, 17–22. [Google Scholar]
- Chang, H.K.; Seo, S.; Myong, J.; Koo, J.; Jeong, J. Factors Associated with Cervical Cancer Screening among Married Female Immigrants with Korean Husbands in South Korea. Int. J. Environ. Res. Public Health 2018, 15, 2528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaneda, A.; Rask, S.; Koponen, P.; Mölsä, M.; Koskinen, S.; Migrant Health and Wellbeing. A Study on Persons of Russian, Somali and Kurdish Origin in Finland. Report 61. (In Finnish, English abstract). Helsinki, Finland. Finnish Institute for Health & Welfare (THL). Available online: http://urn.fi/URN:ISBN:978-952-245-739-4 (accessed on 1 May 2018).
- Willems, B.; Bracke, P. The education gradient in cancer screening participation: A consistent phenomenon across Europe? Int. J. Public Health 2018, 63, 93–103. [Google Scholar] [CrossRef]
- Lorini, C.; Caini, S.; Ierardi, F.; Bachini, L.; Gemmi, F.; Bonaccorsi, G. Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants? Int. J. Environ. Res. Public Health 2020, 17, 1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Social Insurance Institution of Finland (Kela). Old-Age Pension. Available online: https://www.kela.fi/web/en/old-age-pension?inheritRedirect=true) (accessed on 8 October 2019).
- Sund, R. Quality of the Finnish Hospital Discharge Register: A systematic review. Scand. J. Public Health 2012, 40, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Gissler, M.; Haukka, J. Finnish health and social welfare registers in epidemiological research. Nor. Epidemiol. 2004, 14, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Pukkala, E.; Engholm, G.; Højsgaard Schmidt, L.K.; Storm, H.; Khan, S.; Lambe, M.; Pettersson, D.; Ólafsdóttir, E.; Tryggvadóttir, L.; Hakanen, T.; et al. Nordic Cancer Registries–An overview of their procedures and data comparability. Acta Oncol. 2018, 57, 440–455. [Google Scholar] [CrossRef] [Green Version]
- Lofters, A.; Vahabi, M.; Glazier, R.H. The validity of self-reported cancer screening history and the role of social disadvantage in Ontario, Canada. BMC Public Health 2015, 15, 28. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristics (n = 2644) | Russian (n = 837) | Somali (n = 532) | Kurdish (n = 454) | Finns (n = 821) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mass screening participation | |||||||||
| Variable/description | % | 95%CI 1 | % | 95%CI | % | 95%CI | % | 95%CI | |
| No invitation | 2.6 | 1.7–4.1 | 2.1 | 1.3–3.4 | 0.9 | 0.4–1.8 | 3.5 | 2.5–4.9 | |
| Invited, not participated | 34.0 | 30.8–37.4 | 79.0 | 76.2–81.6 | 30.2 | 28.1–32.4 | 29.9 | 26.8–33.1 | |
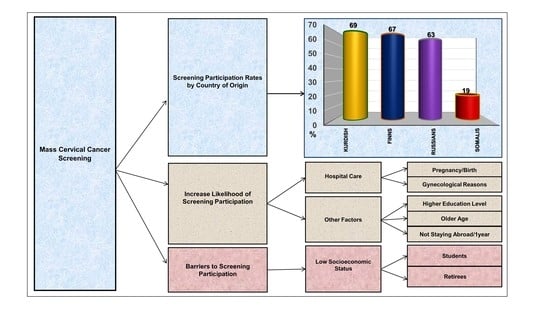
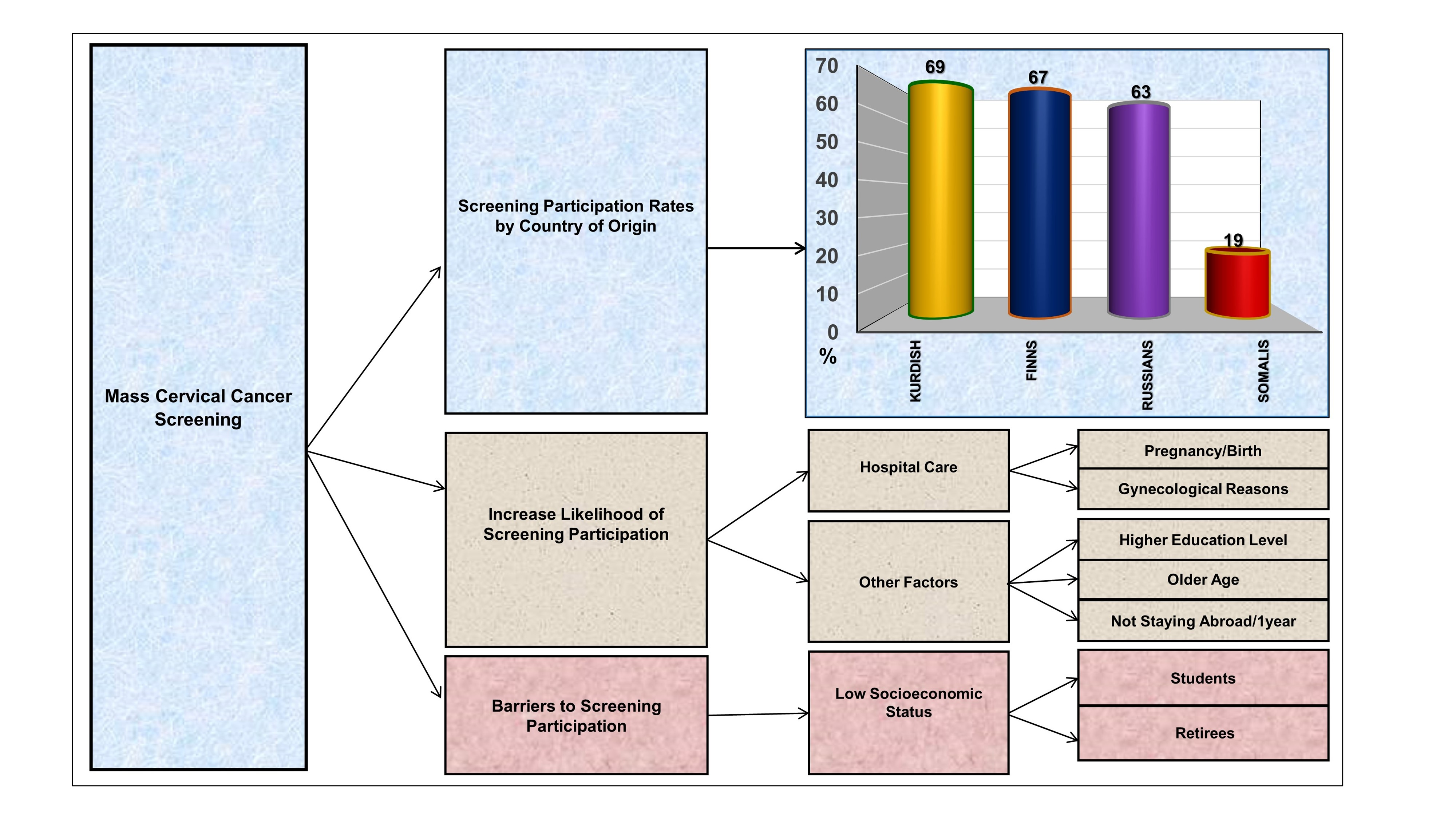
| Invited, participated | 63.3 | 59.9–66.6 | 18.9 | 16.4–21.6 | 68.9 | 66.6–71.1 | 66.6 | 63.3–69.8 | |
| Age | |||||||||
| 30–39 | 29.1 | 26.0–32.3 | 44.0 | 40.8–47.3 | 43.5 | 41.0–45.9 | 28.7 | 25.8–31.9 | |
| 40–49 | 34.3 | 31.0–37.6 | 36.2 | 33.1–39.4 | 39.9 | 37.5–42.4 | 28.5 | 25.5–31.7 | |
| 50–64 | 36.7 | 33.4–40.1 | 19.7 | 17.3–22.4 | 16.6 | 14.9–18.5 | 42.8 | 39.4–46.2 | |
| Education 2 | |||||||||
| High school or higher | 78.7 | 75.7–81.4 | 18.8 | 16.4–21.4 | 33.0 | 30.7–35.3 | 87.0 | 84.7–89.1 | |
| Less than high school/unknown | 21.3 | 18.6–24.3 | 81.2 | 78.6–83.6 | 67.0 | 64.7–69.3 | 13.0 | 10.9–15.3 | |
| Marital status | |||||||||
| Married or in a civil union | 53.7 | 50.1–57.1 | 65.4 | 62.2–68.5 | 76.5 | 74.4–78.6 | 48.5 | 45.0–51.9 | |
| Other/Unknown | 46.3 | 42.9–49.9 | 34.6 | 31.5–37.8 | 23.5 | 21.4–25.6 | 51.5 | 48.1–55.0 | |
| Employment status | |||||||||
| Employed | 60.1 | 56.6–63.5 | 26.0 | 23.2–29.0 | 32.1 | 29.9–34.5 | 81.1 | 78.3–83.5 | |
| Childcare at home | 5.6 | 4.2–7.4 | 5.3 | 4.0–6.9 | 5.8 | 4.8–7.1 | 1.7 | 1.0–2.9 | |
| Student | 6.1 | 4.6–8.2 | 22.1 | 19.8–24.5 | 11.9 | 10.6–13.4 | 2.5 | 1.5–3.9 | |
| Retired | 3.7 | 2.6–5.2 | 6.6 | 5.0–8.5 | 13.2 | 11.5–15.2 | 5.1 | 3.9–6.7 | |
| Unemployed/unknown | 24.5 | 21.7–27.6 | 40.0 | 36.9–43.2 | 36.9 | 34.4–39.4 | 9.6 | 7.9–11.7 | |
| Year of migration | |||||||||
| 1970–1997 | 52.0 | 48.5–55.4 | 66.2 | 63.0–69.2 | 43.7 | 41.3–46.2 | |||
| 1998–2007 | 48.0 | 44.6–51.5 | 33.8 | 30.8–37.0 | 56.3 | 53.8–58.7 | |||
| Had moved from one municipality to another | Na 3 | ||||||||
| No | 94.6 | 92.5–96.1 | 97.0 | 95.4–98.0 | 95.8 | 94.9–96.6 | |||
| Yes | 5.4 | 3.9–7.5 | 3.0 | 2.0–4.6 | 4.2 | 3.4–5.1 | |||
| Had stayed abroad for over one-year 4 | |||||||||
| No | 97.4 | 96.0–98.3 | 92.3 | 90.2–94.0 | 93.1 | 91.5–94.4 | 97.7 | 96.4–98.6 | |
| Yes | 2.6 | 1.7–4.0 | 7.7 | 6.0–9.8 | 6.9 | 5.6–8.5 | 2.3 | 1.4–3.6 | |
| Number of births given in Finland | |||||||||
| None | 56.3 | 53.1–59.5 | 36.8 | 34.0–39.7 | 42.2 | 40–44.5 | 42.4 | 39.2–45.8 | |
| 1–2 | 40.8 | 37.6–44.0 | 15.5 | 13.4–18.0 | 47.3 | 44.9–49.6 | 45.3 | 41.9–48.8 | |
| 3 or more | 2.9 | 2.0–4.4 | 47.7 | 44.7–50.7 | 10.5 | 9.3–11.8 | 12.2 | 10.1–14.8 | |
| Number of abortions in Finland | |||||||||
| None | 81.1 | 78.2–83.7 | 90.3 | 88.3–92.0 | 77.2 | 75.1–79.2 | 82.1 | 79.2–84.6 | |
| 1 or more | 18.9 | 16.3–21.8 | 9.7 | 8.0–11.7 | 22.8 | 20.8–24.9 | 17.9 | 15.4–20.8 | |
| Hospital care in Finland 5 | |||||||||
| None | 20.1 | 17.4–23.0 | 4.7 | 3.4–6.5 | 4.6 | 3.5–6.1 | 14.8 | 12.5–17.3 | |
| Pregnancy/birth-related care | 41.8 | 38.6–45.0 | 61.3 | 58.4–64.2 | 59.3 | 57.0–61.6 | 38.6 | 35.4–41.9 | |
| Other gynecological reason | 10.2 | 8.3–12.5 | 10.0 | 8.1–12.4 | 9.4 | 8.0–11.0 | 11.7 | 9.7–14.0 | |
| Other reason | 28.0 | 25.1–31.1 | 23.9 | 21.4–26.7 | 26.7 | 24.4–29.1 | 35.0 | 31.9–38.2 | |
| Total Women (n = 2579) | Russian (n = 816) | Somali (n = 523) | Kurdish (n = 451) | Finns (n = 789) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mass screening participation Invited, participated | % | 95% CI 1 | % | 95% CI | % | 95% CI | % | 95% CI | |||||
| 63.3 | 59.9–66.6 | 18.9 | 16.4–21.6 | 68.9 | 66.6–71.1 | 66.6 | 63.3–69.8 | ||||||
| Variable/description | % | OR 2 (95%CI) | p | % | OR (95%CI) | p | % | OR (95%CI) | p | % | OR (95%CI) | p | |
| Age | |||||||||||||
| 30–39 | 60.1 | 1.00 | 0.120 | 16.8 | 1.00 | 0.027 | 63.9 | 1.00 | <0.001 | 62.2 | 1.00 | 0.001 | |
| 40–49 | 67.0 | 1.35 (0.93–1.96) | 23.1 | 1.49 (1.03–2.16) | 74.4 | 1.64 (1.30–2.06) | 67.5 | 1.26 (0.86–1.85) | |||||
| 50–64 | 68.4 | 1.44 (1.00–2.07) | 14.7 | 0.85 (0.53–1.37) | 67.5 | 1.17 (0.89–1.54) | 76.3 | 1.96 (1.35–2.83) | |||||
| Education 3 | |||||||||||||
| Upper secondary/less | 57.9 | 1.00 | 0.023 | 19.4 | 1.00 | 0.300 | 66.1 | 1.00 | 0.002 | 57.4 | 1.00 | 0.005 | |
| High school or more | 67.6 | 1.52 (1.06–2.17) | 15.9 | 0.78 (0.50–1.24) | 73.3 | 1.41 (1.13–1.76) | 71.3 | 1.87 (1.20–2.89) | |||||
| Marital status | |||||||||||||
| Other/unknown | 64.6 | 1.00 | 0.612 | 19.3 | 1.00 | 0.736 | 61.0 | 1.00 | <0.001 | 69.3 | 1.00 | 0.848 | |
| Married/in a civil union | 66.3 | 1.08 (0.80–1.46) | 18.4 | 0.94 (0.66–1.34) | 70.9 | 1.57 (1.24–1.99) | 69.9 | 1.03 (0.76–1.40) | |||||
| Employment status | |||||||||||||
| Employed | 66.9 | 1.00 | 0.195 | 22.7 | 1.00 | 0.001 | 74.0 | 1.00 | 0.001 | 70.8 | 1.00 | 0.399 | |
| Childcare at home | 62.0 | 0.80 (0.42–1.54) | 27.4 | 1.28 (0.64–2.56) | 75.5 | 1.08 (0.7–1.68) | 71.3 | 1.02 (0.29–3.63) | |||||
| Student | 65.7 | 0.95 (0.48–1.88) | 9.9 | 0.37 (0.22–0.62) | 65.9 | 0.68 (0.48–0.95) | 51.1 | 0.42 (0.15–1.18) | |||||
| Retired | 44.1 | 0.39 (0.17–0.87) | 23.6 | 1.05 (0.48–2.31) | 60.6 | 0.54 (0.37–0.78) | 66.2 | 0.81 (0.42–1.56) | |||||
| Unemployed/unknown | 66.0 | 0.96 (0.67–1.37) | 20.7 | 0.89 (0.56–1.39) | 65.4 | 0.66 (0.51–0.86) | 64.3 | 0.74 (0.43–1.26) | |||||
| Year of migration | |||||||||||||
| 1970–1997 | 68.0 | 1.00 | 0.129 | 16.3 | 1.00 | 0.013 | 67.4 | 1.00 | 0.358 | ||||
| 1998–2007 | 62.6 | 0.79 (0.58–1.07) | 23.2 | 1.56 (1.10–2.21) | 69.6 | 1.11 (0.89–1.38) | |||||||
| Had moved from one municipality to another | Na 4 | ||||||||||||
| Yes | 60.0 | 1.00 | 0.495 | 26.2 | 1.00 | 0.371 | 55.9 | 1.00 | 0.008 | ||||
| No | 65.8 | 1.28 (0.63–2.63) | 18.5 | 0.64 (0.24–1.72) | 69.3 | 1.79 (1.16–2.75) | |||||||
| Had stayed abroad for over one-year 5 | |||||||||||||
| Yes | 45.2 | 1.00 | 0.076 | 15.8 | 1.00 | 0.560 | 60.9 | 1.00 | 0.097 | 33.4 | 1.00 | 0.005 | |
| No | 66.0 | 2.36 (0.91–6.09) | 18.9 | 1.24 (0.60–2.57) | 69.3 | 1.46 (0.93–2.27) | 70.4 | 4.86 (1.62–14.57) | |||||
| Number of births given in Finland | |||||||||||||
| None | 63.6 | 1.00 | 0.249 | 24.2 | 1.00 | 0.045 | 68.7 | 1.00 | 0.342 | 70.0 | 1.00 | 0.974 | |
| 1–2 births | 68.9 | 1.27 (0.88–1.83) | 20.6 | 0.81 (0.46–1.42) | 69.9 | 1.04 (0.80–1.35) | 69.2 | 0.96 (0.68–1.36) | |||||
| 3 births or more | 56.9 | 0.75 (0.32–1.76) | 15.6 | 0.57 (0.36–0.92) | 64.7 | 0.83 (0.59–1.17) | 69.2 | 0.96 (0.57–1.6) | |||||
| Number of abortions in Finland | |||||||||||||
| None | 64.9 | 1.00 | 0.455 | 18.9 | 1.00 | 0.736 | 68.4 | 1.00 | 0.636 | 70.1 | 1.00 | 0.491 | |
| 1 or more | 68.3 | 1.17 (0.78–1.75) | 17.2 | 0.90 (0.47–1.70) | 69.6 | 1.06 (0.84–1.33) | 67.2 | 0.87 (0.59–1.29) | |||||
| Hospital care in Finland 6 | |||||||||||||
| None | 55.0 | 1.00 | 0.010 | 14.9 | 1.00 | 0.061 | 41.5 | 1.00 | <0.001 | 62.4 | 1.00 | 0.025 | |
| Pregnancy/birth- related care | 70.5 | 1.97 (1.29–3.02) | 16.7 | 1.15 (0.50–2.66) | 71.1 | 3.54 (1.92–6.53) | 66.8 | 1.21 (0.73–2.02) | |||||
| Other gynecological reason | 71.7 | 2.09 (1.13–3.86) | 27.9 | 2.23 (0.88–5.70) | 67.7 | 3.01 (1.49–6.08) | 82.0 | 2.77 (1.40–5.49) | |||||
| Other reason | 62.7 | 1.38 (0.89–2.14) | 22.9 | 1.71 (0.69–4.24) | 65.3 | 2.70 (1.42–5.13) | 70.5 | 1.45 (0.87–2.41) | |||||
| Total n of Women (n = 2579) | |||
|---|---|---|---|
| Variable/Description | OR (95% CI) 2 | p | |
| Study groups | |||
| Finns | 1.00 | <0.001 | |
| Russian | 0.92 (0.74–1.16) | ||
| Somali | 0.16 (0.11–0.22) | ||
| Kurdish | 1.37 (1.02–1.83) | ||
| Age | |||
| 30–39 | 1.00 | 0.003 | |
| 40–49 | 1.30 (1.04–1.62) | ||
| 50–64 | 1.56 (1.20–2.02) | ||
| Education 3 | |||
| Upper secondary or less | 1.00 | 0.006 | |
| High school or more | 1.37 (1.10–1.70) | ||
| Employment status | |||
| Employed | 1.00 | 0.006 | |
| Childcare at home | 0.95 (0.61–1.48) | ||
| Student | 0.59 (0.43–0.83) | ||
| Retired | 0.60 (0.40–0.89) | ||
| Unemployed/unknown | 0.82 (0.65–1.03) | ||
| Year of migration | |||
| 1970–1997 | 1.00 | 0.090 | |
| 1998–2007 among Russian | 0.91 (0.66–1.26) | ||
| 1998–2007 among Somali | 1.69 (1.08–2.65) | ||
| 1998–2007 among Kurdish | 1.21 (0.82–1.77) | ||
| Had stayed abroad for over one year | |||
| Yes | 1.00 | 0.008 | |
| No | 1.87 (1.18–2.96) | ||
| Hospital care in Finland 4 | |||
| None | 1.00 | <0.001 | |
| Pregnancy and birth-related care | 1.73 (1.27–2.35) | ||
| Any other gynecological reason | 2.47 (1.65–3.68) | ||
| Any other reason | 1.53 (1.12–2.08) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idehen, E.E.; Virtanen, A.; Lilja, E.; Tuomainen, T.-P.; Korhonen, T.; Koponen, P. Cervical Cancer Screening Participation among Women of Russian, Somali, and Kurdish Origin Compared with the General Finnish Population: A Register-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 7899. https://doi.org/10.3390/ijerph17217899
Idehen EE, Virtanen A, Lilja E, Tuomainen T-P, Korhonen T, Koponen P. Cervical Cancer Screening Participation among Women of Russian, Somali, and Kurdish Origin Compared with the General Finnish Population: A Register-Based Study. International Journal of Environmental Research and Public Health. 2020; 17(21):7899. https://doi.org/10.3390/ijerph17217899
Chicago/Turabian StyleIdehen, Esther E., Anni Virtanen, Eero Lilja, Tomi-Pekka Tuomainen, Tellervo Korhonen, and Päivikki Koponen. 2020. "Cervical Cancer Screening Participation among Women of Russian, Somali, and Kurdish Origin Compared with the General Finnish Population: A Register-Based Study" International Journal of Environmental Research and Public Health 17, no. 21: 7899. https://doi.org/10.3390/ijerph17217899