Healthy People 2020: Social Determinants of Cigarette Smoking and Electronic Cigarette Smoking among Youth in the United States 2010–2018



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Data and Sample
2.2. Measurements
2.3. Analyses
3. Results
3.1. Descriptive Statistics of Demographics
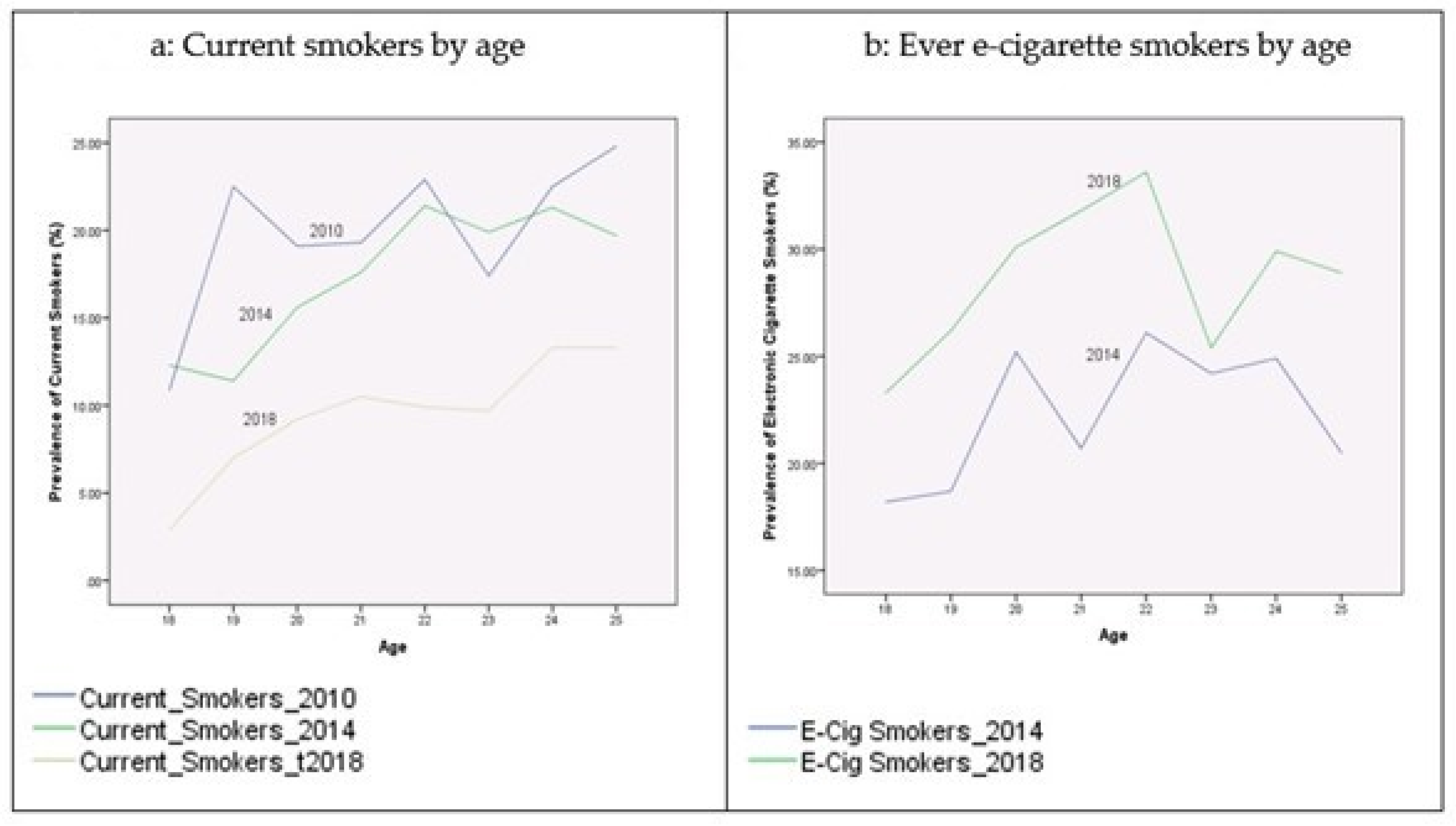
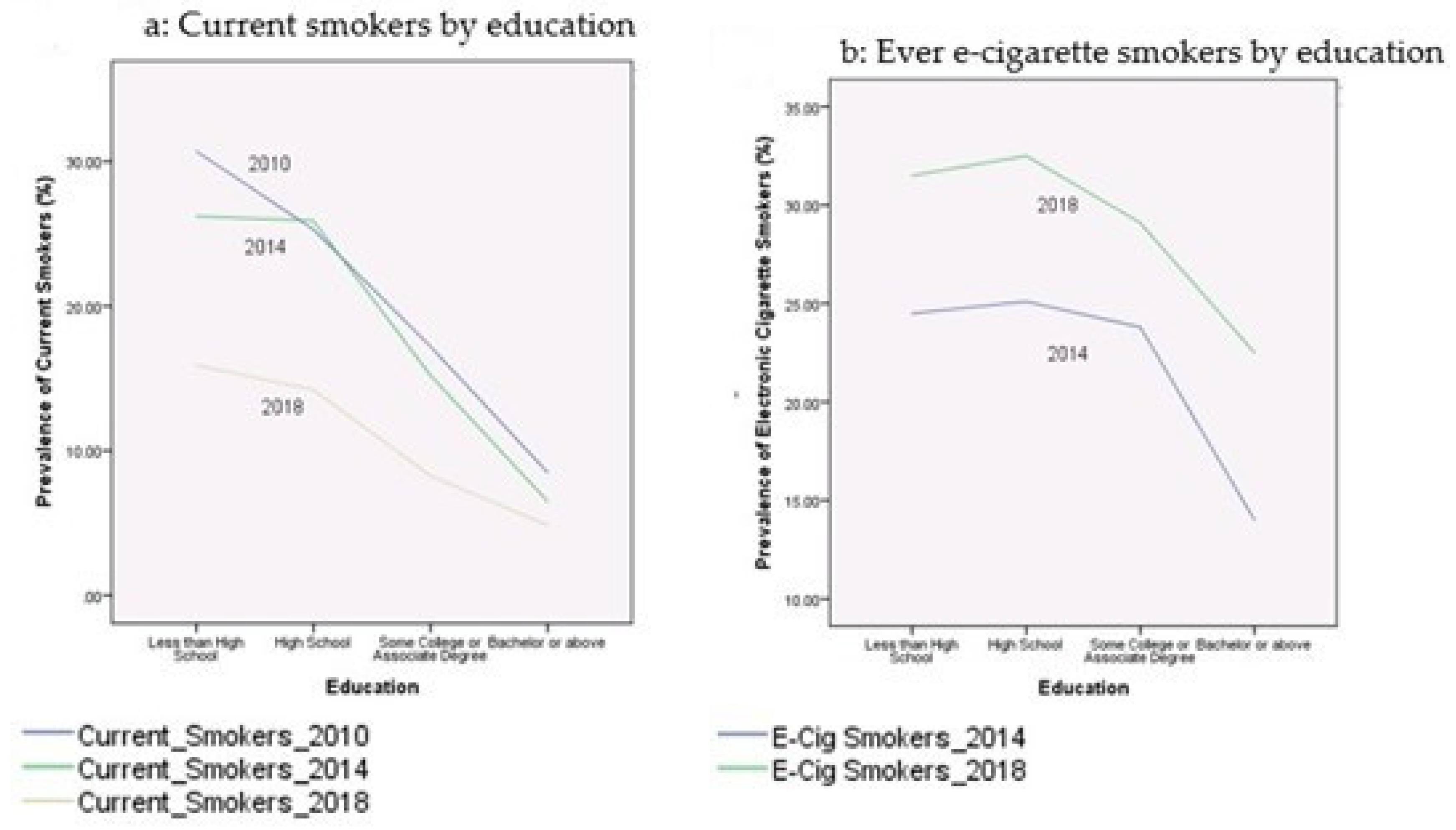
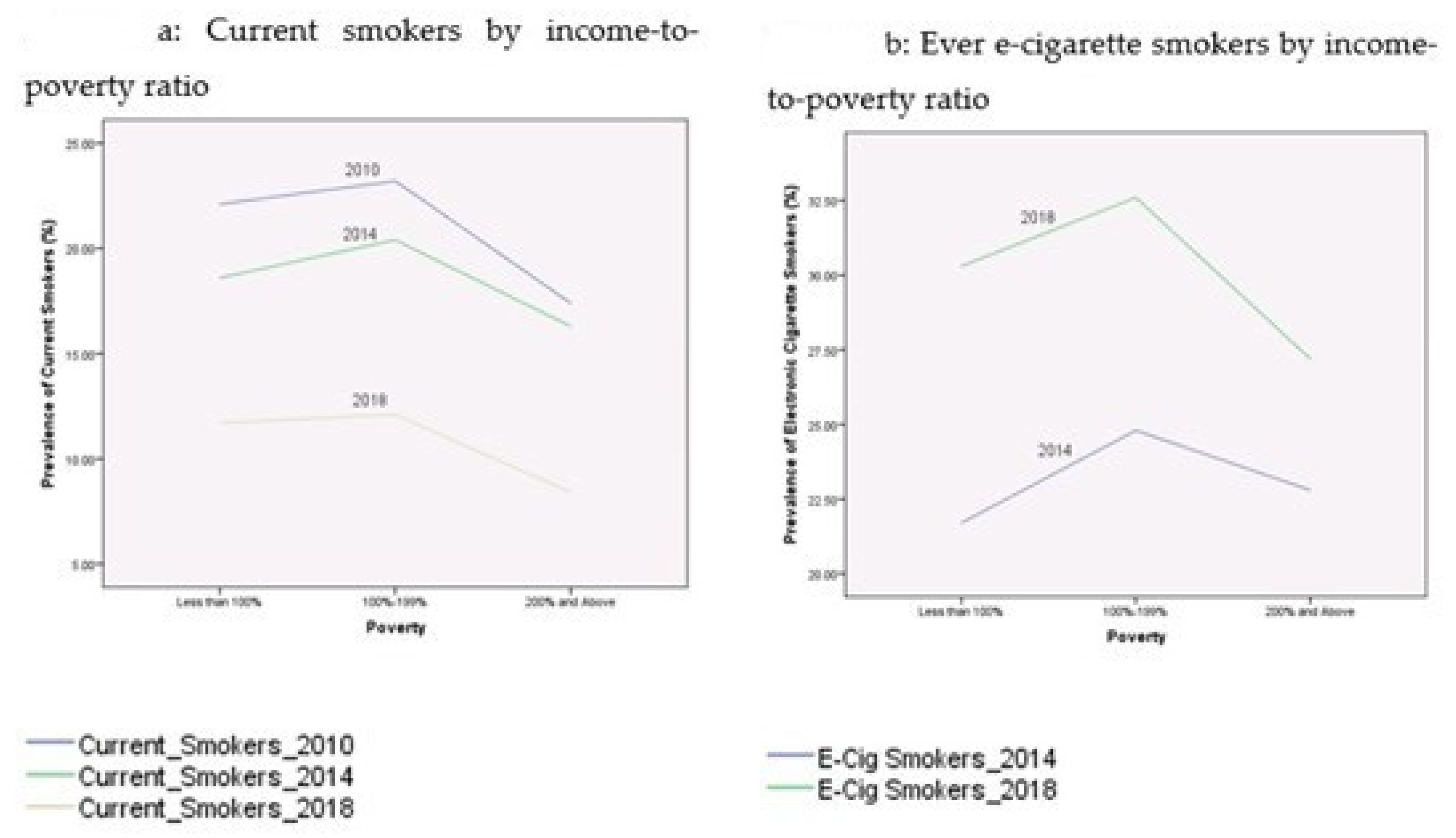
3.2. Prevalence of Current Cigarette Smoking and Electronic Cigarette Smoking
3.3. Predicting the Likelihood of Smoking Behaviors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Cigarette Smoking among U.S. Adults Lowest Ever Recorded: 14% in 2017. Available online: https://www.cdc.gov/media/releases/2018/p1108-cigarette-smoking-adults.html (accessed on 1 September 2020).
- Office of the Surgeon General; U.S. Department of Health and Human Services. Health Consequences of Smoking, Surgeon General Fact Sheet. Available online: https://www.hhs.gov/surgeongeneral/reports-and-publications/tobacco/consequences-smoking-factsheet/index.html (accessed on 10 August 2020).
- Centers for Disease Control and Prevention. Current Cigarette Smoking among Adults in the United States. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/ (accessed on 1 September 2020).
- Office of Disease Prevention and Health Promotion (ODPHP); U.S. Department of Health and Human Services. Healthy People 2020 Brochure. Available online: https://www.healthypeople.gov/sites/default/files/HP2020_brochure_with_LHI_508_FNL.pdf (accessed on 10 August 2020).
- Office of Disease Prevention and Health Promotion (ODPHP); U.S. Department of Health and Human Services. Social Determinants of Health. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health (accessed on 10 August 2020).
- Garrett, B.E.; Dube, S.R.; Babb, S.; McAfee, T. Addressing the social determinants of health to reduce tobacco-related disparities. Nicotine TOB Res. 2015, 17, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Office of the Surgeon General; U.S. Department of Health and Human Services. E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538680/pdf/Bookshelf_NBK538680.pdf (accessed on 10 August 2020).
- Ramoa, C.P.; Hiler, M.M.; Spindle, T.R.; Lopez, A.A.; Karaoghlanian, N.; Lipato, T.; Breland, A.B.; Shihadeh, A.; Eissenberg, T. Electronic cigarette nicotine delivery can exceed that of combustible cigarettes: A preliminary report. TOB Control 2016, 25, e6–e9. [Google Scholar] [CrossRef] [PubMed]
- St. Helen, G.; Havel, C.; Dempsey, D.; Jacob, P.; Benowitz, N.L. Nicotine delivery, retention, and pharmacokinetics from various electronic cigarettes. Addiction 2016, 111, 535–544. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; The National Academies Press: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. 2014 Surgeon General’s Report: The Health Consequences of Smoking-50 Years of Progress. Available online: https://www.cdc.gov/tobacco/data_statistics/sgr/50th-anniversary/index.htm (accessed on 1 September 2020).
- Centers for Disease Control and Prevention. National Health Interview Survey. Available online: https://www.cdc.gov/nchs/nhis/index.htm (accessed on 10 August 2020).
- Centers for Disease Control and Prevention. Youth and Tobacco Use. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/youth_data/tobacco_use/index.htm (accessed on 1 September 2020).
- Malta, D.C.; Vieira, M.L.; Szwarcwald, C.L.; Caixeta, R.; Brito, S.M.F.; Reis, A. Smoking trends among brazilian population- national household survey, 2008 and the national health survey, 2013. Rev. Bras. Epidemiol. 2015, 18 (Suppl. 2), 45–56. [Google Scholar] [CrossRef] [PubMed]
- Santero, M.; Melendi, S.; Hernandez-Vasquez, A.; Irazola, V. Socio-economic inequalities in smoking prevalence and involuntary exposure to tobacco smoke in Argentina: Analysis of three cross-sectional nationally representative surveys in 2005, 2009 and 2013. PLoS ONE 2019, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Cigarette Smoking and Tobacco Use among People of Low Socioeconomic Status. Available online: https://www.cdc.gov/tobacco/disparities/low-ses/index.htm (accessed on 1 September 2020).
- Carlson, S.; Widome, R.; Fabian, L.; Luo, X.; Forster, J. Barriers to quitting smoking among young adults: The role of socioeconomic status. Am. J. Health Promot 2018. [Google Scholar] [CrossRef] [PubMed]
- Tobacco Free Kids. U.S. State and Local Issues: Smoke-Free Laws. Available online: https://www.tobaccofreekids.org/what-we-do/us/smoke-free-laws (accessed on 1 September 2020).
- American Heart Association. Smoking in America: Why More Americans Are Kicking the Habit. Available online: https://www.heart.org/en/news/2018/08/29/smoking-in-america-why-more-americans-are-kicking-the-habit (accessed on 10 August 2020).
- Lynch, B.S.; Bonnie, R.J. Growing Up Tobacco Free: Preventing Nicotine Addition in Children and Youths; National Academies Press: Washington, DC, USA, 1994. [Google Scholar]
- Centers for Disease Control and Prevention. Quick Facts on the Risks of E-Cigarettes for Kids, Teens, and Young Adults. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/Quick-Facts-on-the-Risks-of-E-cigarettes-for-Kids-Teens-and-Young-Adults.html (accessed on 1 September 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | 2010 | 2010 | 2014 | 2014 | 2018 | 2018 |
|---|---|---|---|---|---|---|
| Frequency | Proportion | Frequency | Proportion | Frequency | Proportion | |
| Age | ||||||
| 18 | 311 | 9.50% | 373 | 9.40% | 210 | 9.60% |
| 19 | 355 | 10.80% | 396 | 9.90% | 215 | 9.80% |
| 20 | 361 | 11.00% | 437 | 11.00% | 250 | 11.40% |
| 21 | 383 | 11.70% | 482 | 12.10% | 256 | 11.70% |
| 22 | 442 | 13.50% | 509 | 12.80% | 292 | 13.30% |
| 23 | 482 | 14.70% | 574 | 14.40% | 319 | 14.50% |
| 24 | 467 | 14.20% | 582 | 14.60% | 315 | 14.40% |
| 25 | 480 | 14.60% | 628 | 15.80% | 338 | 15.40% |
| Gender | ||||||
| Male | 1532 | 46.70% | 1955 | 49.10% | 1103 | 50.30% |
| Female | 1749 | 53.30% | 2026 | 50.90% | 1092 | 49.70% |
| Race/Ethnicity | ||||||
| Non-Hispanic White | 1619 | 49.30% | 2241 | 56.30% | 1251 | 57.00% |
| Non-Hispanic Black | 576 | 17.60% | 573 | 14.40% | 274 | 12.50% |
| Hispanic | 844 | 25.70% | 840 | 21.10% | 453 | 20.60% |
| Other race group | 242 | 7.40% | 327 | 8.20% | 217 | 9.90% |
| Education | ||||||
| Less than high school | 535 | 16.40% | 478 | 12.00% | 239 | 10.90% |
| High school/GED | 905 | 27.70% | 1085 | 27.30% | 584 | 26.60% |
| Some college | 1335 | 40.80% | 1751 | 44.00% | 896 | 40.90% |
| Bachelor and above | 497 | 15.20% | 664 | 16.70% | 474 | 21.60% |
| Income-to-Poverty ratio | ||||||
| Less than 100% | 1057 | 34.90% | 1309 | 34.20% | 488 | 22.90% |
| 100–199% | 725 | 23.90% | 923 | 24.10% | 480 | 22.60% |
| 200% and greater | 1249 | 41.20% | 1599 | 41.70% | 1160 | 54.50% |
| Reported health status | ||||||
| Excellent | 1319 | 40.20% | 1676 | 42.10% | 935 | 42.60% |
| Very good | 1098 | 33.50% | 1330 | 33.40% | 723 | 32.90% |
| Good | 696 | 21.20% | 788 | 19.80% | 436 | 19.90% |
| Fair/Poor | 165 | 5.00% | 187 | 4.70% | 90 | 4.10% |
| Citizenship status | ||||||
| Yes | 2883 | 88.10% | 3603 | 90.60% | 2011 | 91.60% |
| No | 390 | 11.90% | 376 | 9.40% | 184 | 8.40% |
| Observations | 3281 | 3281 | 3981 | 3981 | 2195 | 2195 |
| Variables | Current Smokers 2010 (95% CI) | Current Smokers 2014 (95% CI) | Current Smokers 2018 (95% CI) | Ever Electronic Smokers 2014 (95% CI) | Ever Electronic Smokers 2018 (95% CI) |
|---|---|---|---|---|---|
| Age | |||||
| 18 | 10.9% | 12.3% | 2.90% | 18.20% | 23.30% |
| (7% to 14%) | (9% to 16%) | (1% to 5%) | (14% to 22%) | (18% to 29%) | |
| 19 | 22.5% | 11.4% | 7.00% | 18.70% | 26.20% |
| (18% to 27%) | (8% to 15%) | (4% to 10%) | (15% to 26%) | (20% to 32%) | |
| 20 | 19.1% | 15.6% | 9.20% | 25.20% | 30.10% |
| (15% to 23%) | (12% to 19%) | (6% to 13%) | (21% to 29%) | (24% to 36%) | |
| 21 | 19.3% | 17.6% | 10.50% | 20.70% | 31.80% |
| (15% to 23%) | (14% to 21%) | (7% to 14%) | (17% to 24%) | (26% to 38%) | |
| 22 | 22.9% | 21.4% | 9.90% | 26.10% | 33.60% |
| (19% to 27%) | (18% to 25%) | (6% to 13%) | (22% to 30%) | (28% to 39%) | |
| 23 | 17.4% | 19.9% | 9.70% | 24.20% | 25.40% |
| (14% to 21%) | (17% to 23%) | (6% to 13%) | (21% to 28%) | (21% to 30%) | |
| 24 | 22.5% | 21.3% | 13.30% | 24.90% | 29.90% |
| (19% to 26%) | (18% to 25%) | (10% to 17%) | (21% to 28%) | (35% to 28%) | |
| 25 | 24.8% | 19.7% | 13.30% | 20.50% | 28.90% |
| (21% to 29%) | (17% to 23%) | (10% to 17%) | (17% to 24%) | (24% to 34%) | |
| Gender | |||||
| Male | 22.9% | 19.9% | 11.60% | 27.20% | 35.50% |
| (21% to 25%) | (18% to 22%) | (10% to 14%) | (25% to 29%) | (33% to 38%) | |
| Female | 18.0% | 16.1% | 8.20% | 18.10% | 22.10% |
| (16% to 20%) | (14% to 18%) | (7% to 10%) | (16% to 20%) | (20% to 25%) | |
| Race/Ethnicity | |||||
| Non-Hispanic White | 25.6% | 22.1% | 12.20% | 28.30% | 33.70% |
| (24% to 28%) | (20% to 24%) | (10% to 14%) | (26% to 30%) | (31% to 36%) | |
| Non-Hispanic Black | 18.9% | 15.2% | 8.40% | 10.60% | 16.20% |
| (16% to 22%) | (12% to 18%) | (5% to 12%) | (8% to 13%) | (12% to 21%) | |
| Hispanic | 12.1% | 11.9% | 5.10% | 18.20% | 23.70% |
| (10% to 14%) | (10% to 14%) | (3% to 7%) | (16% to 21%) | (20% to 28%) | |
| Other race group | 16.5% | 9.8% | 8.80% | 15.00% | 27.00% |
| (12% to 21%) | (7% to 13%) | (5% to 13%) | (11% to 19%) | (21% to 33%) | |
| Education | |||||
| Less than high school | 30.7% | 26.2% | 15.90% | 24.50% | 31.50% |
| (27% to 35%) | (22% to 30%) | (11% to 21%) | (21% to 28%) | (26% to 37%) | |
| High school/GED | 25.3% | 25.9% | 14.20% | 25.10% | 32.50% |
| (22% to 28%) | (23% to 29%) | (11% to 17%) | (22% to 28%) | (29% to 36%) | |
| Some college | 17.2% | 15.2% | 8.30% | 23.80% | 29.10% |
| (15% to 19%) | (14% to 17%) | (6% to 10%) | (22% to 26%) | (26% to 32%) | |
| Bachelor and above | 8.5% | 6.5% | 4.90% | 14.00% | 22.50% |
| (6% to 11%) | (5% to 8%) | (3% to 7%) | (11% to 17%) | (19% to 26%) | |
| Income-to-Poverty ratio | |||||
| Less than 100% | 22.1% | 18.6% | 11.70% | 21.70% | 30.30% |
| (20% to 25%) | (17% to 21%) | (9% to 15%) | (19% to 24%) | (26.2% to 34.4%) | |
| 100%–199% | 23.2% | 20.4% | 12.10% | 24.80% | 32.60% |
| (20% to 26%) | (18% to 23%) | (9% to 15%) | (22% to 28%) | (28% to 37%) | |
| 200% and greater | 17.4% | 16.3% | 8.40% | 22.80% | 27.20% |
| (15% to 19%) | (14% to 18%) | (7% to 10%) | (21% to 25%) | (25% to 30%) | |
| Reported health status | |||||
| Excellent | 14.9% | 11.6% | 6.10% | 17.10% | 23.70% |
| (13% to 17%) | (10% to 13%) | (5% to 8%) | (15% to 19%) | (21% to 26%) | |
| Very good | 20.3% | 19.5% | 11.90% | 25.30% | 31.30% |
| (18% to 23%) | (17% to 22%) | (10% to 14%) | (23% to 28%) | (28% to 35%) | |
| Good | 26.3% | 25.1% | 13.90% | 26.60% | 32.60% |
| (23% to 30%) | (22% to 28%) | (11% to 17%) | (24% to 30%) | (28% to 37%) | |
| Fair/Poor | 38.2% | 34.2% | 13.90% | 34.80% | 42.30% |
| (31% to 46%) | (27% to 41%) | (7% to 21%) | (28% to 42%) | (32% to 52%) | |
| Citizenship status | |||||
| Yes | 21.6% | 18.7% | 10.10% | 23.80% | 29.70% |
| (20% to 23%) | (17% to 20%) | (9% to 11%) | (22% to 25%) | (28% to 32%) | |
| No | 10.8% | 10.9% | 8.20% | 10.90% | 19.00% |
| (8% to 14%) | (8% to 14%) | (4% to 12%) | (8% to 14%) | (13% to 25%) | |
| Observations (n) | 3281 | 3981 | 2195 | 3981 | 2195 |
| Being a Current Smoker | Being a Current Smoker | Being a Current Smoker | |
|---|---|---|---|
| 2010 | 2014 | 2018 | |
| Col (1) | Col (2) | Col (3) | |
| Odds Ratio | Odds Ratio | Odds Ratio | |
| (Lower to Upper 95% CI) | (Lower to Upper 95% CI) | (Lower to Upper 95% CI) | |
| Ever electronic cigarette smoker | 10.428 (8.502 to 12.790) *** | 6.666 (4.770 to 9.316) *** | |
| Age | 1.193 (1.141 to 1.248) *** | 1.191 (1.136 to 1.248) *** | 1.285 (1.188 to 1.389) *** |
| Gender | |||
| Male | 1.408 (1.162 to 1.706) *** | 1.028 (0.841 to 1.255) | 1.141 (0.828 to 1.571) |
| Female (reference) | |||
| Race/Ethnicity | |||
| Non-Hispanic White | 1.177 (0.780 to 1.778) | 1.869 (1.198 to 2.916) ** | 1.475 (0.824 to 2.643) |
| Non-Hispanic Black | 0.590 (0.373 to 0.932) * | 1.502 (0.906 to 2.492) | 1.130 (0.543 to 2.352) |
| Hispanic | 0.315 (0.199 to 0.498) *** | 0.702 (0.433 to 1.140) | 0.495 (0.245 to 1.001) * |
| Other race group (ref) | |||
| Education | |||
| Less than high school | 10.227 (6.644 to 15.742) *** | 7.540 (4.828 to 11.776) *** | 6.729 (3.560 to 12.718) *** |
| High school/GED | 6.056 (4.102 to 8.942) *** | 6.782 (4.585 to 10.031) *** | 4.416 (2.591 to 7.526) *** |
| Some college | 3.242 (2.223 to 4.728) *** | 2.339 (1.386 to 3.947) *** | |
| Bachelor and above (ref) | 2.698 (1.853 to 3.929) *** | ||
| Income-to-Poverty ratio | |||
| Less than 100% | 1.363 (1.083 to 1.716) ** | 1.173 (0.927 to 1.484) | 1.621 (1.095 to 2.400) * |
| 100%–199% | 1.428 (1.115 to 1.829) ** | 1.147 (0.892 to 1.475) | 1.466 (0.999 to 2.152) |
| 200% and greater (ref) | |||
| Reported health status | |||
| Excellent (ref) | |||
| Very good | 1.578 (1.252 to 1.988) *** | 1.654 (1.303 to 2.098) *** | 1.759 (1.202 to 2.575) * |
| Good | 1.888 (1.461 to 2.439) *** | 2.094 (1.606 to 2.730) *** | 1.618 (1.054 to 2.482) * |
| Fair/Poor | 2.883 (1.943 to 4.277) *** | 2.420 (1.606 to 3.648) *** | 1.419 (0.714 to 2.818) |
| Citizenship status | |||
| Yes | 2.135 (1.425 to 3.199) *** | 1.040 (0.683 to 1.582) | 1.236 (0.912 to 1.674) |
| No (ref) | |||
| Observations (n) | 3281 | 2195 | 3981 |
| −2 Log likelihood | 2695.38 | 2650.297 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, G.; Wu, L. Healthy People 2020: Social Determinants of Cigarette Smoking and Electronic Cigarette Smoking among Youth in the United States 2010–2018. Int. J. Environ. Res. Public Health 2020, 17, 7503. https://doi.org/10.3390/ijerph17207503
Wang G, Wu L. Healthy People 2020: Social Determinants of Cigarette Smoking and Electronic Cigarette Smoking among Youth in the United States 2010–2018. International Journal of Environmental Research and Public Health. 2020; 17(20):7503. https://doi.org/10.3390/ijerph17207503
Chicago/Turabian StyleWang, Gang, and Liyun Wu. 2020. "Healthy People 2020: Social Determinants of Cigarette Smoking and Electronic Cigarette Smoking among Youth in the United States 2010–2018" International Journal of Environmental Research and Public Health 17, no. 20: 7503. https://doi.org/10.3390/ijerph17207503