Is Rescuer Cardiopulmonary Resuscitation Jeopardised by Previous Fatiguing Exercise?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
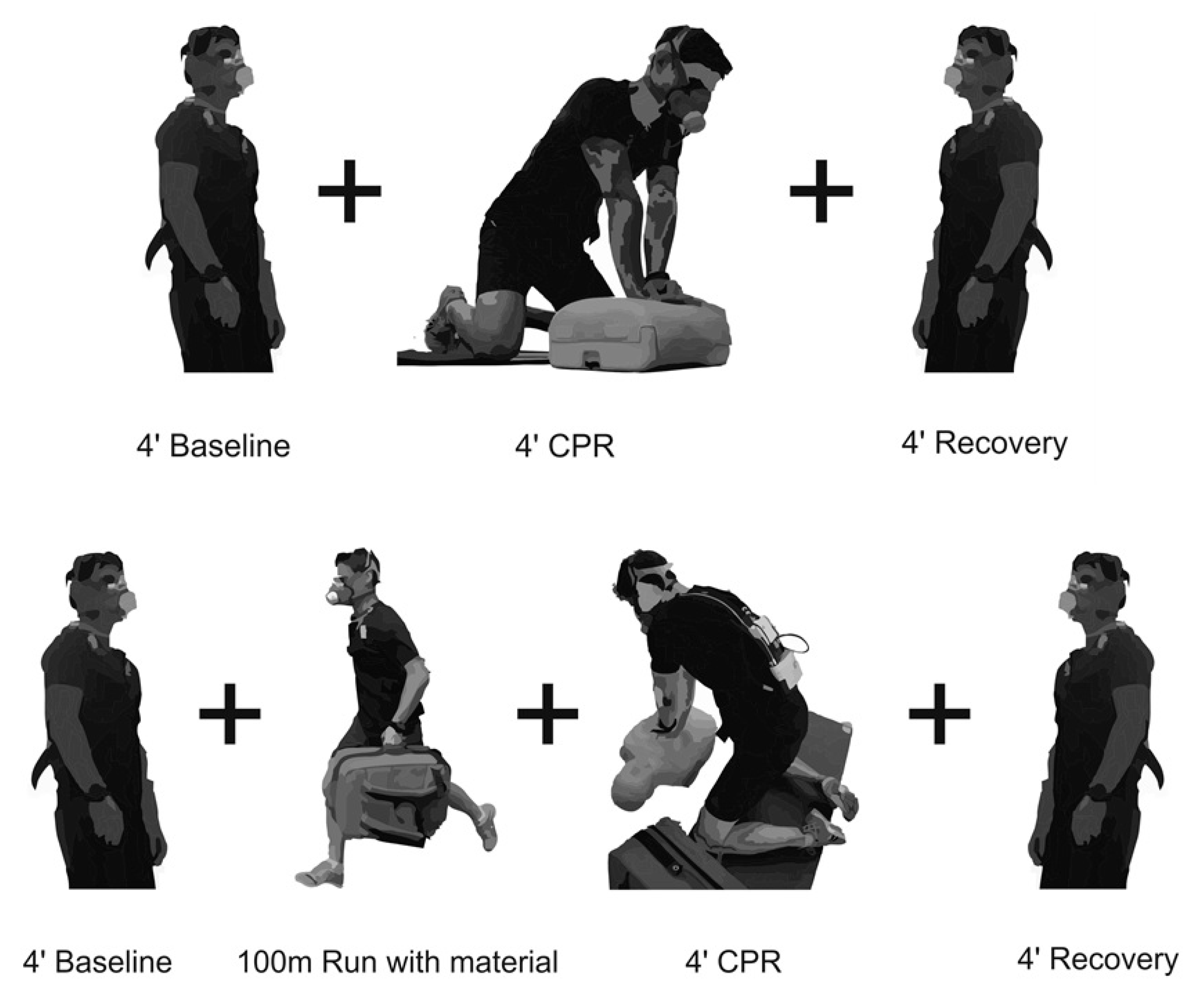
2.2. Design
2.3. Methodology
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sugerman, T.; Edelson, P.; Leary, M.; Weidman, K.; Herzberg, L.; Hoek, L.V.; Becker, B.; Abella, S. Rescuer fatigue during actual in-hospital cardiopulmonary resuscitation with audiovisual feedback: A prospective multicenter study. Resuscitation 2009, 80, 981–984. [Google Scholar] [CrossRef] [Green Version]
- Vadeboncoeur, T.; Stolz, U.; Panchal, A.; Silver, A.; Venuti, M.; Tobin, J.; Smith, G.; Nunez, M.; Karamooz, M.; Spaite, D. Chest compression depth and survival in out-of-hospital cardiac arrest. Resuscitation 2014, 85, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Stiell, I.G.; Brown, S.P.; Nichol, G.; Cheskes, S.; Vaillancourt, C.; Callaway, C.W.; Morrison, L.J.; Christenson, J.; Aufderheide, T.P.; Davis, D.P. What is the optimal chest compression depth during out-of-hospital cardiac arrest resuscitation of adult patients? Circulation 2014, 130, 1962–1970. [Google Scholar] [CrossRef] [Green Version]
- Idris, A.H.; Guffey, D.; Pepe, P.E.; Brown, S.P.; Brooks, S.C.; Callaway, C.W.; Christenson, J.; Davis, D.P.; Daya, M.R.; Gray, R. Chest compression rates and survival following out-of-hospital cardiac arrest. Crit. Care Med. 2015, 43, 840–848. [Google Scholar] [CrossRef]
- Christenson, J.; Andrusiek, D.; Everson-Stewart, S.; Kudenchuk, P.; Hostler, D.; Powell, J.; Callaway, C.W.; Bishop, D.; Vaillancourt, C.; Davis, D. Chest compression fraction determines survival in patients with out-of-hospital ventricular fibrillation. Circulation 2009, 120, 1241–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumar, R.; Shuster, M.; Callaway, C.; Gent, L.; Atkins, D.; Bhanji, F.; Brooks, S.; Caen, A. 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 115, S315–S367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.-T.; Wenzel, V. European resuscitation council guidelines for resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talikowska, M.; Tohira, H.; Bailey, P.; Finn, J. Cardiopulmonary resuscitation quality: Widespread variation in data intervals used for analysis. Resuscitation 2016, 102, 25–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochoa, F.J.; Ramalle-Gomara, E.; Lisa, V.; Saralegui, I. The effect of rescuer fatigue on the quality of chest compressions. Resuscitation 1998, 37, 149–152. [Google Scholar] [CrossRef]
- Ashton, A.; McCluskey, A.; Gwinnutt, C.; Keenan, A. Effect of rescuer fatigue on performance of continuous external chest compressions over 3 min. Resuscitation 2002, 55, 151–155. [Google Scholar] [CrossRef]
- Hightower, D.; Thomas, S.; Stone, C.; Dunn, K.; March, J. Decay in quality of closed-chest compressions over time. Ann. Emerg. Med. 1995, 26, 300–303. [Google Scholar] [CrossRef]
- Kalenda, Z. The capnogram as a guide to the efficacy of cardiac massage. Resuscitation 1978, 6, 259–263. [Google Scholar] [CrossRef]
- Kern, K.B.; Sanders, A.B.; Voorhees, W.D.; Babbs, C.F.; Tacker, W.A.; Ewy, G.A. Changes in expired end-tidal carbon dioxide during cardiopulmonary resuscitation in dogs: A prognostic guide for resuscitation efforts. J. Am. Coll. Cardiol. 1989, 13, 1184–1189. [Google Scholar] [CrossRef] [Green Version]
- Sutton, R.M.; French, B.; Meaney, P.A.; Topjian, A.A.; Parshuram, C.S.; Edelson, D.P.; Schexnayder, S.; Abella, B.S.; Merchant, R.M.; Bembea, M. Physiologic monitoring of CPR quality during adult cardiac arrest: A propensity-matched cohort study. Resuscitation 2016, 106, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.-Y.; Huang, C.-H.; Chang, W.-T.; Tsai, M.-S.; Wang, C.-H.; Chen, W.-J. Initial end-tidal CO2 partial pressure predicts outcomes of in-hospital cardiac arrest. Am. J. Emerg. Med. 2016, 34, 2367–2371. [Google Scholar] [CrossRef] [PubMed]
- Grmec, Š.; Križmarič, M.; Mally, Š.; Koželj, A.; Špindler, M.; Lešnik, B. Utstein style analysis of out-of-hospital cardiac arrest—Bystander CPR and end expired carbon dioxide. Resuscitation 2007, 72, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Kolar, M.; Križmarić, M.; Klemen, P.; Grmec, Š. Partial pressure of end-tidal carbon dioxide successful predicts cardiopulmonary resuscitation in the field: A prospective observational study. Critical Care 2008, 12, R115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iserbyt, P.; Schouppe, G.; Charlier, N. A multiple linear regression analysis of factors affecting the simulated Basic Life Support (BLS) performance with Automated External Defibrillator (AED) in Flemish lifeguards. Resuscitation 2015, 89, 70–74. [Google Scholar] [CrossRef]
- Guidelines 2000 for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2000, 102, 2135–2302.
- Sousa, A.; Figueiredo, P.; Zamparo, P.; Pyne, D.B.; Vilas-Boas, J.P.; Fernandes, R.J. Exercise modality effect on bioenergetical performance at VO2max intensity. Med. Sci. Sports Exerc. 2015, 47, 1705–1713. [Google Scholar] [CrossRef] [Green Version]
- Sousa, A.; Fernandes, R.J.; Rodríguez, N.; Abraldes, J.A. Influence of a 100-M Simulated In-Water Rescue on Cardiopulmonary Parameters. Prehosp. Emerg. Care 2017, 21, 301–308. [Google Scholar] [CrossRef] [PubMed]
- De Jesus, K.; Guidetti, L.; de Jesus, K.; Vilas Boas, J.P.; Baldari, C.; Fernande, R. Which are the best VO2 sampling intervals to characterize low to severe swimming intensities? Int. J. Sports Physiol. Perform. 2014, 35, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, V.; Keller, C.; Ahamed, I.; Dorges, V.; Lindner, K.; Brimacombe, J. Effects of samller tidal volumes during basic life support ventilation in patients with respiratory arrest: Good ventilation, less risk? Resuscitation 1999, 43, 25–29. [Google Scholar] [CrossRef]
- Wallace, S.; Abella, S.; Becker, B. Quantifying the effect of cardiopulmonary resuscitation quality on cardiac arrest outcome. A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 148–156. [Google Scholar] [CrossRef] [Green Version]
- Sheak, K.; Douglas, W.; Leary, M.; Babaeizadeh, S.; UYuen, T.; Zive, D.; Owens, P.; Edelson, D.; Daya, M.; Idris, A.; et al. Quantitative relationship between end-tidal carbon dioxide and CPR quality during both in-hospital and out-of-hospital cardiac arrest. Resuscitation 2015, 89, 149–154. [Google Scholar] [CrossRef]
- Miles, D.; Underwood, J.P.; Nolan, D.; Frey, M.; Gotshall, R. Metabolic, hemodynamic, and respiratory responses to performing cardiopulmonary resuscitation. Can. J. Appl. Sport Sci. 1984, 9, 141–147. [Google Scholar]
- Buono, M.J.; Golding, L. The energy cost of performing cardiopulmonary resuscitation. Med. Sci. Sports Exerc. 1980, 12, 118. [Google Scholar]
- Abella, B.S.; Sandbo, N.; Vassilatos, P.; Alvarado, J.P.; O’Hearn, N.; Wigder, H.N.; Hoffman, P.; Tynus, K.; Vanden Hoek, T.L.; Becker, L.B. Chest compression rates during cardiopulmonary resuscitation are suboptimal: A prospective study during in-hospital cardiac arrest. Circulation 2005, 111, 428–434. [Google Scholar] [CrossRef]
- Gallagher, E.J.; Lombardi, G.; Gennis, P. Effectiveness of bystander cardiopulmonary resuscitation and survival following out-of-hospital cardiac arrest. JAMA 1995, 274, 1922–1925. [Google Scholar] [CrossRef]
- Gómez, C.A.; Pérez, V.R.; Furelos, R.J.B.; Palacios-Aguilar, J. Efecto de la fatiga física del socorrista en los primeros cuatro minutos de la reanimación cardiopulmonar posrescate acuático. Emerg. Rev. Soc. Española Med. Urgenc. Y Emerg. 2013, 25, 184–190. [Google Scholar]
- Perkins, G.D.C.M.; Simons, R. Training manikins. In Abc Of Resuscitation, 5th ed.; Colqu-houn, M.H.A., Evans, T.R., Eds.; BMJ Publishing Group: London, UK, 2004; pp. 97–101. [Google Scholar]
- Hong, D.Y.; Park, S.O.; Lee, K.R.; Baek, K.J.; Shin, D.H. A different rescuer changing strategy between 30: 2 cardiopulmonary resuscitation and hands-only cardiopulmonary resuscitation that considers rescuer factors: A randomised cross-over simulation study with a time-dependent analysis. Resuscitation 2012, 83, 353–359. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Rf (b.min−1) | VT (l) | VE (l.min−1) | VO2 (ml/kg/min) | R | VCO2 (ml.min−1) | HR (bpm) | PetCO2 mmHg | |
|---|---|---|---|---|---|---|---|---|---|
| CPR | Base | 15.4 ± 3.7 | 1.1 ± 0.3 | 15.3 ± 3.5 | 6.2 ± 1.1 | 0.88 ± 0.1 | 0.4 ± 0.1 | 90 ± 12 | 34.4 ± 2.5 |
| 1st min | 26.3 ± 8.9 1 | 1.30 ± 0.6 1 | 30.1 ± 8.4 1 | 11.4 ± 1.8 1 | 0.97 ± 0.0 1 | 0.81 ± 0.2 1 | 115 ± 18 1 | 28.7 ± 4.4 1 | |
| 2nd min | 29.6 ± 9.8 | 1.27 ± 0.4 2 | 33.9 ± 7.4 2 | 14.9 ± 1.9 2 | 0.87 ± 0.1 2 | 0.95 ± 0.2 2 | 124 ± 15 2 | 30.8 ± 5.2 2 | |
| 3rd min | 28.5 ± 7.7 | 1.46 ± 0.4 3 | 38.3 ± 7.7 3 | 16.5 ± 2.7 3 | 0.90 ± 0.0 3 | 1.09 ± 0.2 3 | 128 ± 15 3 | 33.1 ± 4.6 | |
| 4th min | 27.1 ± 7.2 4 | 1.48 ± 0.4 4 | 37.7 ± 9.3 4 | 16.0 ± 3.2 4 | 0.92 ± 0.1 4 | 1.08 ± 0.2 4 | 130 ± 16 4 | 31.4 ± 4.4 4 | |
| 4-min | 27.1 ± 8.3 * | 1.36 ± 0.4 * | 33.9 ± 7.3 * | 14.4 ± 2.1 * | 0.92 ± 0.1 * | 0.96 ± 0.2 * | 123 ± 17 * | 32.9 ± 5.0 | |
| CPR Run | Base | 14.7 ± 1.2 | 1.1 ± 0.3 | 14.8 ± 2.5 | 7.7 ± 1.6 | 0.89 ± 0.1 | 0.4 ± 0.1 | 85 ± 10 | 33.7 ± 2.1 |
| 1st min | 29.9 ± 5.8 | 2.6 ± 0.8 | 74.9 ± 17.3 | 27.2 ± 3.0 | 1.27 ± 0.1 | 2.51 ± 0.5 | 155 ± 15 | 39.6 ± 5.3 | |
| 2nd min | 30.3 ± 5.6 | 2.48 ± 0.7 | 72.4 ± 17.7 | 22.8 ± 3.2 | 1.33 ± 0.1 | 2.24 ± 0.5 | 154 ± 13 | 37.2 ± 4.9 | |
| 3rd min | 31.1 ± 5.7 | 2.20 ± 0.7 | 66.7 ± 16.7 | 19.8 ± 2.6 | 1.27 ± 0.1 | 1.86 ± 0.4 | 148 ± 15 | 33.7 ± 4.9 | |
| 4th min | 32.1 ± 5.5 | 2.0 ± 0.5 | 62.6 ± 14.7 | 19.3 ± 2.9 | 1.16 ± 0.1 | 1.65 ± 0.3 | 144 ± 15 | 35.6 ± 5.4 | |
| 4-min | 30.5 ± 5.8 | 2.27 ± 0.6 | 67.3 ± 15.0 | 22.0 ± 2.5 | 1.25 ± 0.1 | 2.01 ± 0.4 | 148 ± 17 | 31.9 ± 5.3 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abraldes, J.A.; Fernandes, R.J.; Rodríguez, N.; Sousa, A. Is Rescuer Cardiopulmonary Resuscitation Jeopardised by Previous Fatiguing Exercise? Int. J. Environ. Res. Public Health 2020, 17, 6668. https://doi.org/10.3390/ijerph17186668
Abraldes JA, Fernandes RJ, Rodríguez N, Sousa A. Is Rescuer Cardiopulmonary Resuscitation Jeopardised by Previous Fatiguing Exercise? International Journal of Environmental Research and Public Health. 2020; 17(18):6668. https://doi.org/10.3390/ijerph17186668
Chicago/Turabian StyleAbraldes, J. Arturo, Ricardo J. Fernandes, Núria Rodríguez, and Ana Sousa. 2020. "Is Rescuer Cardiopulmonary Resuscitation Jeopardised by Previous Fatiguing Exercise?" International Journal of Environmental Research and Public Health 17, no. 18: 6668. https://doi.org/10.3390/ijerph17186668