Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy

 ,
, 
Abstract
:1. Introduction
2. Method
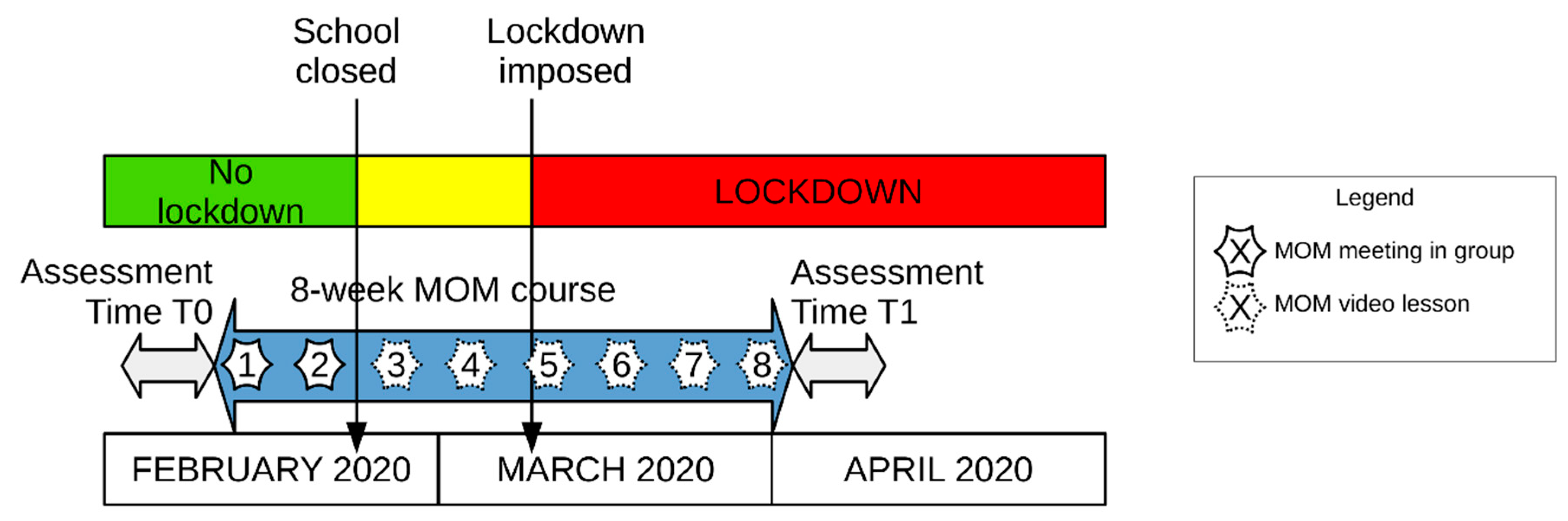
2.1. Procedure
2.2. Participants
2.3. Mindfulness Oriented Meditation (MOM) Course
2.4. Measures
2.5. Statistical Analyses
3. Results
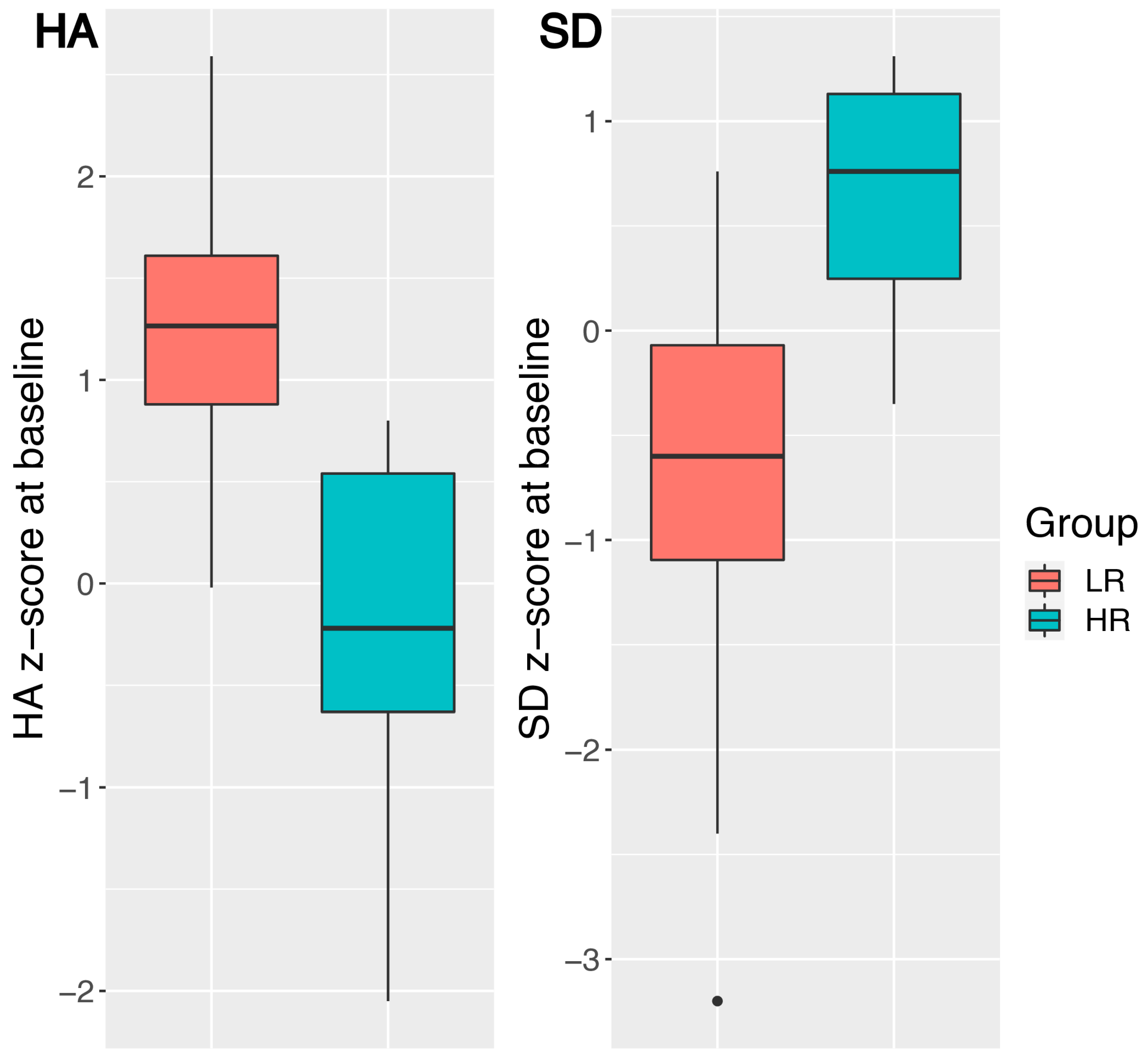
3.1. Objective 1: Baseline Differences in Teachers with LR and HR Personality Profiles
Sample Partitioning Based on Resilience Profile
3.2. Objective 2: Pre–Post MOM Changes in Teachers with LR and HR Personality Profiles
3.2.1. Mindfulness Skills
3.2.2. Empathy
3.2.3. Personality Profile
3.2.4. Interoceptive Awareness
3.2.5. Psychological Well-Being
3.2.6. Emotional Distress
3.2.7. Teacher Burnout
3.2.8. Adherence to Practice
3.3. Objective 3: Teachers’ Satisfaction with the MOM Course (in General and in the Context of the Covid-19 Outbreak)
Evaluation of the MOM Course
4. Discussion
4.1. Objective 1: Baseline Differences in Teachers with LR and HR Personality Profiles
4.2. Objective 2: Pre–Post MOM Changes in Teachers with LR and HR Personality Profiles
4.3. Objective 3: Teachers’ Satisfaction with the MOM Course (in General and in the Context of the Covid-19 Outbreak)
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19); Situation Report–51; World Health Organization: Albany, NY, USA, 11 March 2020. [Google Scholar]
- World Health Organization. Coronavirus Disease 2019 (COVID-19); Situation Report–105; World Health Organization: Albany, NY, USA, 4 May 2020. [Google Scholar]
- International Monetary Fund. Italy: 2020 Article IV Consultation-Press Release; Staff Report; and Statement by the Executive Director for Italy; IMF Country Report No. 20/79; International Monetary Fund: Washington, DC, USA, 20 March 2020. [Google Scholar]
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Di Nicola, M. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Favieri, F.; Forte, G.; Tambelli, R.; Casagrande, M. The Italians in the time of coronavirus: Psychosocial aspects of unexpected COVID-19 pandemic. Lancet 2020. preprint. [Google Scholar] [CrossRef]
- Davico, C.; Ghiggia, A.; Marcotulli, D.; Ricci, F.; Amianto, F.; Vitiello, B. Psychological impact of the COVID-19 pandemic on adults and their children in Italy. Lancet 2020. preprint. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Sun, L.; Sun, Z.; Wu, L.; Zhu, Z.; Zhang, F.; Shang, Z.; Liu, W. Prevalence and risk factors of acute posttraumatic stress symptoms during the COVID-19 outbreak in Wuhan, China. MedRxiv 2020. preprint. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Gentilini, U.; Almenfi, M.; Orton, I.; Dale, P. Social Protection and Jobs Responses to Covid-19: A Real-Time Review of Country Measures; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Logie, C.H.; Turan, J.M. How do we balance tensions between COVID-19 public health responses and stigma mitigation? Learning from HIV research. AIDS Behav. 2020, 24, 2003–2006. [Google Scholar] [CrossRef] [Green Version]
- Geoffroy, P.A.; Le Goanvic, V.; Sabbagh, O.; Richoux, C.; Weinstein, A.; Dufayet, G.; Lejoyeux, M. Psychological support system for hospital workers during the COVID-19 outbreak: Rapid design and implementation of the Covid-psy hotline. Front. Psychiatry 2020, 11, 511. [Google Scholar] [CrossRef]
- Zhou, X. Psychological crisis interventions in Sichuan Province during the 2019 novel coronavirus outbreak. Psychiatry Res. 2020, 286, 112895. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Yang, L.; Yin, J.; Wang, D.; Rahman, A.; Li, X. Urgent need to develop evidence-based self-help interventions for mental health of healthcare workers in COVID-19 pandemic. Psychol. Med. 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The role of telehealth in reducing the mental health burden from COVID-19. Telemed. E Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Fischer, R.; Karl, J.A.; Bortolini, T.; Zilberberg, M.; Robinson, K.; Rabelo, A.L.A.; Mattos, P. Rapid review and meta-meta-analysis of self-guided interventions to address anxiety, depression and stress during COVID-19 social distancing. PsyArXiv 2020. preprint. [Google Scholar] [CrossRef]
- Chiesa, A.; Malinowski, P. Mindfulness-based approaches: Are they all the same? J. Clin. Psychol. 2011, 67, 404–424. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. J. Altern. Complement. Med. 2006, 15, 593–600. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Goldberg, S.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef]
- Luken, M.; Sammons, A. Systematic review of mindfulness practice for reducing job burnout. Am. J. Occup. Ther. 2016, 70, p1–p7002250020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gawande, R.; To, M.N.; Pine, E.; Griswold, T.; Creedon, T.B.; Brunel, A.; Schuman-Olivier, Z. Mindfulness training enhances self-regulation and facilitates health behavior change for primary care patients: A randomized controlled trial. J. Gen. Intern. Med. 2019, 34, 293–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matiz, A.; Guzzon, D.; Crescentini, C.; Paschetto, A.; Fabbro, F. The role of self body brushing vs mindfulness meditation on interoceptive awareness: A non-randomized pilot study on healthy participants with possible implications for body image disturbances. Eur. J. Integr. Med. 2020, 37, 101168. [Google Scholar] [CrossRef]
- Birnie, K.; Speca, M.; Carlson, L.E. Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Stress Health 2010, 26, 359–371. [Google Scholar] [CrossRef]
- Lamothe, M.; Rondeau, E.; Malboeuf-Hurtubise, C.; Duval, M.; Sultan, S. Outcomes of MBSR or MBSR-based interventions in health care providers: A systematic review with a focus on empathy and emotional competencies. Complement. Ther. Med. 2016, 24, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Campanella, F.; Crescentini, C.; Urgesi, C.; Fabbro, F. Mindfulness-oriented meditation improves self-related character scales in healthy individuals. Compr. Psychiatry 2014, 55, 1269–1278. [Google Scholar] [CrossRef]
- Crescentini, C.; Matiz, A.; Fabbro, F. Improving personality/character traits in individuals with alcohol dependence: The influence of mindfulness-oriented meditation. J. Addict. Dis. 2015, 34, 75–87. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- Carmody, J.; Baer, R.A. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. J. Behav. Med. 2008, 31, 23–33. [Google Scholar] [CrossRef]
- Mantzios, M.; Giannou, K. Group vs. single mindfulness meditation: Exploring avoidance, impulsivity, and weight management in two separate mindfulness meditation settings. Appl. Psychol. Health Well Being 2014, 6, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Matiz, A.; Fabbro, F.; Crescentini, C. Single vs. group mindfulness meditation: Effects on personality, religiousness/spirituality, and mindfulness skills. Mindfulness 2017, 9, 1236–1244. [Google Scholar] [CrossRef]
- Spijkerman, M.P.J.; Pots, W.T.M.; Bohlmeijer, E.T. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sevilla-Llewellyn-Jones, J.; Santesteban-Echarri, O.; Pryor, I.; McGorry, P.; Alvarez-Jimenez, M. Web-based mindfulness interventions for mental health treatment: Systematic review and meta-analysis. JMIR Ment. Health 2018, 5, e10278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Broche-Pérez, Y.; Fernández-Fleites, Z.; Jiménez-Puig, E.; Fernández-Castillo, E.; Rodríguez-Martin, B.C. Gender and fear of COVID-19 in a Cuban population sample. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Liu, W. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Southwick, S.M.; Charney, D.S. Resilience: The Science of Mastering Life’s Greatest Challenges; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Karreman, A.; Vingerhoets, A.J. Attachment and well-being: The mediating role of emotion regulation and resilience. Personal. Individ. Differ. 2012, 53, 821–826. [Google Scholar] [CrossRef]
- Simeon, D.; Yehuda, R.; Cunill, R.; Knutelska, M.; Putnam, F.W.; Smith, L.M. Factors associated with resilience in healthy adults. Psychoneuroendocrinology 2007, 32, 1149–1152. [Google Scholar] [CrossRef]
- Davydov, D.M.; Stewart, R.; Ritchie, K.; Chaudieu, I. Resilience and mental health. Clin. Psychol. Rev. 2010, 30, 479–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Personal. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Sagone, E.; De Caroli, M.E. A correlational study on dispositional resilience, psychological well-being, and coping strategies in university students. Am. J. Educ. Res. 2014, 2, 463–471. [Google Scholar] [CrossRef]
- Morice-Ramat, A.; Goronflot, L.; Guihard, G. Are alexithymia and empathy predicting factors of the resilience of medical residents in France? Int. J. Med. Educ. 2018, 9, 122. [Google Scholar] [CrossRef] [Green Version]
- Keye, M.D.; Pidgeon, A.M. Investigation of the relationship between resilience, mindfulness, and academic self-efficacy. Open J. Soc. Sci. 2013, 1, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Haase, L.; Stewart, J.L.; Youssef, B.; May, A.C.; Isakovic, S.; Simmons, A.N.; Paulus, M.P. When the brain does not adequately feel the body: Links between low resilience and interoception. Biol. Psychol. 2016, 113, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Hjemdal, O.; Vogel, P.A.; Solem, S.; Hagen, K.; Stiles, T.C. The relationship between resilience and levels of anxiety, depression, and obsessive-compulsive symptoms in adolescents. Clin. Psychol. Psychother. 2010, 18, 314–321. [Google Scholar] [CrossRef]
- Cooke, G.P.; Doust, J.A.; Steele, M.C. A survey of resilience, burnout, and tolerance of uncertainty in Australian general practice registrars. BMC Med. Educ. 2013, 2, 13. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Lee, H.K.; Lee, K. Influence of temperament and character on resilience. Compr. Psychiatry 2013, 54, 1105–1110. [Google Scholar] [CrossRef]
- Eley, D.S.; Cloninger, C.R.; Walters, L.; Laurence, C.; Synnott, R.; Wilkinson, D. The relationship between resilience and personality traits in doctors: Implications for enhancing well being. PeerJ 2013, 1, e216. [Google Scholar] [CrossRef] [Green Version]
- Eley, D.S.; Leung, J.; Hong, B.A.; Cloninger, K.M.; Cloninger, C.R. Identifying the dominant personality profiles in medical students: Implications for their well-being and resilience. PLoS ONE 2016, 11, e0160028. [Google Scholar] [CrossRef] [Green Version]
- Oshio, A.; Taku, K.; Hirano, M.; Saeed, G. Resilience and big five personality traits: A meta-analysis. Personal. Individ. Differ. 2018, 127, 54–60. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Przybeck, T.R.; Svrakic, D.M.; Wetzel, R.D. The Temperament and Character Inventory (TCI): A guide to Its Development and Use; Center for Psychobiology of Personality: St Louis, MO, USA, 1994. [Google Scholar]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Fabbro, A.; Fabbro, F.; Capurso, V.; D’Antoni, F.; Crescentini, C. Effects of mindfulness training on school teachers’ self-reported personality traits as well as stress and burnout levels. Percept. Mot. Skills 2020, 127, 515–532. [Google Scholar] [CrossRef]
- OECD. TALIS 2018 Results (Volume II): Teachers and School Leaders as Valued Professionals; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Crescentini, C.; Urgesi, C.; Campanella, F.; Eleopra, R.; Fabbro, F. Effects of an 8-week meditation program on the implicit and explicit attitudes toward religious/spiritual self-representations. Conscious. Cogn. 2014, 30, 266–280. [Google Scholar] [CrossRef]
- Crescentini, C.; Matiz, A.; Cimenti, M.; Pascoli, E.; Eleopra, R.; Fabbro, F. Effect of mindfulness meditation on personality and psychological well-being in patients with multiple sclerosis. Int. J. MS Care 2018, 20, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabbro, F.; Crescentini, C. La meditazione orientata alla mindfulness (MOM) nella ricerca psicologica. Ricerche. Psicologia. 2017, 4, 457–472. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. Full Catastrophe Living; Deltacorte: New York, NY, USA, 1990. [Google Scholar]
- Thera, N. The Heart of Buddhist Meditation: The Buddha’s Way of Mindfulness; Weiser Book: San Francisco, CA, USA, 2014. [Google Scholar]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [Green Version]
- Giovannini, C.; Giromini, L.; Bonalume, L.; Tagini, A.; Lang, M.; Amadei, G. The Italian five facet mindfulness questionnaire: A contribution to its validity and reliability. J. Psychopathol. Behav. Assess. 2014, 36, 415–423. [Google Scholar] [CrossRef]
- Reniers, R.L.E.P.; Corcoran, R.; Drake, R.; Shryane, N.M.; Völlm, B.A. The QCAE: A questionnaire of cognitive and affective empathy. J. Personal. Assess. 2011, 93, 84–95. [Google Scholar] [CrossRef]
- Di Girolamo, M.; Giromini, L.; Winters, C.L.; Serie, C.M.B.; de Ruiter, C. The questionnaire of cognitive and affective empathy: A comparison between paper-and-pencil versus online formats in Italian samples. J. Personal. Assess. 2017, 101, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Delvecchio, G.; Garzitto, M.; Fagnani, C.; Fornasari, L.; Stazi, M.A.; Picardi, A.; Brambilla, P. Normative data and effects of age and gender on temperament and character dimensions across the lifespan in an Italian population: A cross-sectional validation study. J. Affect. Disord. 2016, 204, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calì, G.; Ambrosini, E.; Picconi, L.; Mehling, W.E.; Committeri, G. Investigating the relationship between interoceptive accuracy, interoceptive awareness, and emotional susceptibility. Front. Psychol. 2015, 6, 1202. [Google Scholar] [CrossRef] [Green Version]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Sirigatti, S.; Stefanile, C.; Giannetti, E.; Iani, L.; Penzo, I.; Mazzeschi, A. Assessment of factor structure of Ryff’s psychological well-being scales in Italian adolescents. Boll. Psicol. Appl. 2009, 259, 30–50. [Google Scholar]
- Viola, M.M.; Musso, P.; Inguglia, C.; Lo Coco, A. Psychological well-being and career indecision in emerging adulthood: The moderating role of hardiness. Career Dev. Q. 2016, 64, 387–396. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Costantini, M.; Musso, M.; Viterbori, P.; Bonci, F.; Del Mastro, L.; Garrone, O.; Morasso, G. Detecting psychological distress in cancer patients: Validity of the Italian version of the hospital anxiety and depression scale. Support. Care Cancer 1999, 7, 121–127. [Google Scholar] [CrossRef]
- Brennan, C.; Worrall-Davies, A.; McMillan, D.; Gilbody, S.; House, A. The hospital anxiety and depression scale: A diagnostic meta-analysis of case-finding ability. J. Psychosom. Res. 2010, 69, 371–378. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the hospital anxiety and depression scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Schwab, R.L. Maslach Burnout Inventory—Educators Survey (MBI-ES). In MBI Study, 3rd ed.; Maslach, C., Jackson, S.E., Leiter, M.P., Eds.; Consulting Psychologists Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Hartigan, J.A.; Wong, M.A. Algorithm AS 136: A K-Means clustering algorithm. Appl. Stat. 1979, 28, 100. [Google Scholar] [CrossRef]
- Urgesi, C.; Aglioti, S.M.; Skrap, M.; Fabbro, F. The spiritual brain: Selective cortical lesions modulate human self-transcendence. Neuron 2010, 65, 309–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, L.; Atchley, R.M.; Oken, B.S. Adherence to practice of mindfulness in novice meditators: Practices chosen, amount of time practiced, and long-term effects following a mindfulness-based intervention. Mindfulness 2017, 9, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Forbes, L.; Gutierrez, D.; Johnson, S.K. Investigating adherence to an online introductory mindfulness program. Mindfulness 2017, 9, 271–282. [Google Scholar] [CrossRef]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: A systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Ho, C.S.; Chee, C.; Ho, R. Mental health strategies to combat the psychological impact of coronavirus disease 2019 (COVID-19) beyond paranoia and panic. Ann. Acad. Med. Singapore 2020, 49, 1–6. [Google Scholar]
- Fessell, D.; Cherniss, C. Coronavirus disease 2019 (COVID-19) and beyond: Micropractices for burnout prevention and emotional wellness. J. Am. Col. Radiol. 2020, 17, 746–748. [Google Scholar] [CrossRef]
- Shaw, S.C. Hopelessness, helplessness and resilience: The importance of safeguarding our trainees’ mental wellbeing during the COVID-19 pandemic. Nurse Educ. Pract. 2020, 44, 102780. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.Y.; Kwak, H.Y.; Kim, J.W. Using mind–body modalities via telemedicine during the COVID-19 crisis: Cases in the Republic of Korea. Int. J. Environ. Res. Public Health 2020, 17, 4477. [Google Scholar] [CrossRef]
- Szcześniak, D.; Gładka, A.; Misiak, B.; Cyran, A.; Rymaszewska, J. The SARS-CoV-2 and mental health: From biological mechanisms to social consequences. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2020, 104, 110046. [Google Scholar] [CrossRef] [PubMed]
- Behan, C. The benefits of meditation and mindfulness practices during times of crisis such as Covid-19. Irish J. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Polizzi, C.; Lynn, S.J.; Perry, A. Stress and coping in the time of Covid-19: Pathways to resilience and recovery. Clin. Neuropsychiatry 2020, 17, 59–62. [Google Scholar]
- Baiano, C.; Zappullo, I.; Conson, M. Tendency to worry and fear of mental health during Italy’s COVID-19 lockdown. Int. J. Environ. Res. Public Health 2020, 17, 5928. [Google Scholar] [CrossRef]
- Galbraith, N.; Boyda, D.; McFeeters, D.; Hassan, T. The mental health of doctors during the Covid-19 pandemic. BJPsych Bull. 2020, 1–4. [Google Scholar] [CrossRef]
- Van Agteren, J.; Bartholomaeus, J.; Fassnacht, D.B.; Iasiello, M.; Ali, K.; Lo, L.; Kyrios, M. Using Internet-based psychological measurement to capture the deteriorating community mental health profile during COVID-19: Observational study. JMIR Ment. Health 2020, 7, e20696. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 30954–30955. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Wang, H. The psychological and mental impact of Coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Tan, H. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open. 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Dong, L.; Wang, T.; Yuan, C.; Fu, R.; Zhang, L.; Bouey, J. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen. Hosp. Psychiatry 2020, S0163-8343(20), 30045-300451. [Google Scholar]
- Hayes, S.C.; Plumb, J.C. Mindfulness from the bottom up: Providing an inductive framework for understanding mindfulness processes and their application to human suffering. Psychol. Inq. 2007, 18, 242–248. [Google Scholar] [CrossRef]
- Bandura, A. Self-regulation of motivation through anticipatory and self-reactive mechanisms. In Nebraska Symposium on Motivation; Dienstbier, R.A., Ed.; University of Nebraska Press: Lincoln, MO, USA, 1990; pp. 69–164. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef]
- Abbott, R.A.; Whear, R.; Rodgers, L.R.; Bethel, A.; Thompson, C.J.; Kuyken, W.; Dickens, C. Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: A systematic review and meta-analysis of randomised controlled trials. J. Psychosom. Res. 2014, 76, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Nam, S.; Toneatto, T. The influence of attrition in evaluating the efficacy and effectiveness of mindfulness-based interventions. Int. J. Ment. Health Addict. 2016, 14, 969–981. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Carmody, J.; Reed, G.; Kristeller, J.; Merriam, P. Mindfulness, spirituality, and health-related symptoms. J. Psychosom. Res. 2008, 64, 393–403. [Google Scholar] [CrossRef]
- Cobb, M.; Puchalski, C.M.; Rumbold, B. (Eds.) Oxford Textbook of Spirituality in Healthcare; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Ferrell, B.R.; Handzo, G.; Picchi, T.; Puchalski, C.; Rosa, W.E. The urgency of spiritual care: COVID-19 and the critical need for whole-person palliation. J. Pain Symptom Manag. 2020, 60, e7–e11. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID-19 and physical distancing: The need for prevention and early intervention. JAMA Int. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Question | Course Evaluation |
|---|---|
| Q1 | How much did you enjoy the course? |
| Q2 | How challenging was it? |
| Q3 | How useful was it for you? |
| Q4 | How much did you engage in it? |
| Q5 | In relation to training needs and your professional role, to what extent has it met your needs? |
| Q6 | How adequate do you think the instructor’s competence is with regards to content and teaching methods? |
| Context of the course (COVID-19 lockdown) | |
| Q7 | How often have you been distracted by thinking about Covid-19 during practice sessions? |
| Q8 | How much do you think the practice of meditation helped you during this particular period of isolation related to the emergency? |
| Q9 | How do you think you would have lived through this period without the practice? |
| Q10 | How do you think the distance learning methods of the last 6 meetings have conditioned the effectiveness of the course? |
| Test | Scale | Baseline Score | Difference between Groups | ||
|---|---|---|---|---|---|
| LR Group | HR Group | t | p | ||
| FFMQ | OBS | 26.47 (4.81) | 28.15 (4.31) | −1.41 | 0.17 |
| DES | 25.53 (5.00) | 27.58 (6.45) | −1.33 | 0.19 | |
| AWA | 23.16 (5.16) | 28.08 (5.99) | −3.31 | <0.01 * | |
| NJU | 24.19 (5.23) | 29.12 (5.71) | −3.39 | <0.01 * | |
| NRE | 18.25 (3.72) | 22.00 (3.78) | −3.78 | <0.01 * | |
| QCAE | CE | 57.81 (5.44) | 58.54 (6.75) | −0.44 | 0.66 |
| AE | 39.06 (3.56) | 34.62 (4.61) | 4.03 | <0.01 * | |
| TCI | NS | −0.21 (1.18) | 0.24 (1.04) | −1.52 | 0.13 |
| HA | 1.25 (0.56) | −0.26 (0.82) | 7.97 | <0.01 * | |
| RD | 0.18 (0.97) | −0.25 (1.06) | 1.57 | 0.12 | |
| P | −0.08 (1.00) | −0.09 (0.91) | −0.44 | 0.66 | |
| SD | −0.77 (0.93) | 0.64 (0.51) | −7.31 | <0.01 * | |
| C | 0.30 (0.65) | 0.38 (0.91) | −1.22 | 0.23 | |
| ST | 0.33 (0.83) | 0.64 (1.09) | −1.19 | 0.24 | |
| MAIA | NOT | 3.30 (0.93) | 3.55 (0.88) | −1.02 | 0.31 |
| NDI | 2.12 (0.68) | 2.13 (0.81) | −0.02 | 0.99 | |
| NWO | 2.08 (0.95) | 2.81 (1.06) | −2.71 | 0.01 * | |
| ARE | 2.15 (0.59) | 2.50 (0.85) | −1.79 | 0.08 | |
| EAW | 3.60 (0.94) | 3.62 (0.85) | −0.10 | 0.92 | |
| SRE | 2.38 (0.98) | 3.03 (0.70) | −2.93 | <0.01 * | |
| BLI | 2.30 (1.03) | 2.51 (0.91) | −0.82 | 0.41 | |
| TRU | 2.82 (1.20) | 3.23 (1.25) | −1.26 | 0.21 | |
| PWB | SA | 11.38 (3.10) | 13.88 (2.12) | −3.65 | <0.01 * |
| AU | 9.69 (2.93) | 12.73 (2.74) | −4.08 | <0.01 * | |
| EM | 9.91 (2.68) | 12.08 (3.16) | −2.78 | 0.01 * | |
| PG | 14.94 (1.98) | 16.23 (1.82) | −3.02 | 0.01 * | |
| PR | 12.06 (2.69) | 14.12 (3.12) | −2.65 | 0.01 * | |
| PL | 12.09 (3.00) | 14.73 (2.71) | −3.52 | <0.01 * | |
| HADS | Anxiety | 9.69 (3.41) | 6.12 (3.98) | 3.62 | <0.01 * |
| Depression | 5.19 (2.47) | 3.00 (1.88) | 3.83 | <0.01 * | |
| Total Score | 14.88 (5.25) | 9.12 (4.89) | 4.31 | <0.01 * | |
| MBI | EE | 25.69 (11.63) | 16.04 (9.44) | 3.49 | <0.01 * |
| DP | 3.53 (3.75) | 1.81 (2.65) | 2.12 | 0.04 * | |
| PA | 35.78 (5.51) | 40.62 (5.40) | −3.36 | <0.01 * | |
| Test | Scale | Pre-Post Change | 2-Way Mixed Model ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| LR Group | HR Group | Group | Time | Group: Time | |||||
| F | p | F | p | F | p | ||||
| FFMQ | OBS | 3.78 (4.20) | 2.69 (3.03) | 1.2 | 0.28 | 43.3 | <0.01 * | 1.2 | 0.27 |
| DES | 1.84 (5.16) | 0.69 (3.07) | 0.9 | 0.33 | 4.9 | 0.03 * | 1.0 | 0.32 | |
| AWA | 3.06 (4.70) | 1.08 (3.88) | 8.4 | 0.01 * | 13.0 | <0.01 * | 3.0 | 0.09 | |
| NJU | 2.38 (4.98) | 1.54 (3.73) | 13.0 | <0.01 * | 11.0 | <0.01 * | 0.5 | 0.48 | |
| NRE | 1.72 (4.71) | 0.73 (3.79) | 21.6 | <0.01 * | 4.6 | 0.04 * | 0.7 | 0.39 | |
| QCAE | CE | −0.97 (5.20) | −0.62 (4.03) | 0.4 | 0.54 | 1.6 | 0.21 | 0.1 | 0.78 |
| AE | −2.97 (4.40) | −1.65 (3.92) | 9.9 | <0.01 * | 17.5 | <0.01 * | 1.4 | 0.24 | |
| TCI | NS | 0.05 (0.77) | −0.19 (0.57) | 1.4 | 0.23 | 0.6 | 0.43 | 1.8 | 0.19 |
| HA | −0.46 (0.33) | −0.23 (0.64) | 65.7 | <0.01 * | 28.6 | <0.01 * | 3.1 | 0.08 | |
| RD | 0.04 (0.64) | −0.22 (0.68) | 6.0 | 0.02 * | 1.1 | 0.29 | 2.3 | 0.14 | |
| P | 0.19 (0.95) | 0.05 (0.74) | <0.1 | 0.89 | 0.8 | 0.39 | 0.5 | 0.50 | |
| SD | 0.64 (0.74) | 0.12 (0.49) | 39.0 | <0.01 * | 20.1 | <0.01 * | 9.3 | <0.01 * | |
| C | 0.24 (0.63) | 0.17 (0.64) | 0.7 | 0.42 | 4.4 | 0.04 * | 2.3 | 0.14 | |
| ST | 0.36 (0.66) | 0.13 (0.47) | 0.6 | 0.44 | 10.2 | <0.01 * | 2.2 | 0.15 | |
| MAIA | NOT | 0.52 (0.77) | 0.42 (0.54) | 1.2 | 0.28 | 27.4 | <0.01 * | 0.3 | 0.61 |
| NDI | −0.08 (0.75) | −0.28 (1.00) | 0.6 | 0.44 | 2.5 | 0.12 | 0.8 | 0.39 | |
| NWO | 0.18 (1.07) | −0.22 (0.86) | 8.2 | 0.01 * | <0.1 | 0.87 | 2.3 | 0.13 | |
| ARE | 1.03 (0.71) | 0.76 (0.92) | 2.7 | 0.11 | 69.9 | <0.01 * | 1.6 | 0.21 | |
| EAW | 0.33 (0.78) | 0.27 (0.88) | <0.1 | 0.96 | 7.6 | 0.01 * | 0.1 | 0.78 | |
| SRE | 0.96 (0.94) | 0.62 (0.81) | 9.0 | <0.01 * | 46.4 | <0.01 * | 2.1 | 0.15 | |
| BLI | 0.86 (1.08) | 0.67 (0.89) | 0.3 | 0.56 | 33.5 | <0.01 * | 0.5 | 0.46 | |
| TRU | 0.74 (0.88) | 0.44 (0.88) | 1.0 | 0.32 | 25.5 | <0.01 * | 1.7 | 0.20 | |
| PWB | SA | 0.59 (2.85) | −0.35 (2.06) | 4.4 | 0.4 * | 0.2 | 0.62 | 3.0 | 0.09 |
| AU | 0.97 (3.04) | 1.00 (2.06) | 20.2 | <0.01 * | 7.9 | 0.01 * | <0.1 | 0.96 | |
| EM | 1.50 (2.26) | 1.04 (2.78) | 9.0 | <0.01 * | 14.7 | <0.01 * | 0.5 | 0.49 | |
| PG | −0.03 (3.04) | −0.08 (1.74) | 5.8 | 0.02 * | 0.1 | 0.73 | 0.9 | 0.34 | |
| PR | 1.78 (1.88) | 0.23 (2.12) | 3.1 | 0.08 | 14.6 | <0.01 * | 8.7 | <0.01 * | |
| PL | 0.72 (1.85) | −0.38 (2.56) | 9.0 | <0.01 * | 0.3 | 0.57 | 3.6 | 0.06 | |
| HADS | Anxiety | −1.53 (2.68) | −0.54 (2.63) | 14.2 | <0.01 * | 8.7 | <0.01 * | 2.0 | 0.16 |
| Depression | −1.47 (2.09) | −0.35 (1.50) | 9.1 | <0.01 * | 13.8 | <0.01 * | 5.3 | 0.03 * | |
| Total Score | −3.00 (4.13) | −0.88 (2.82) | 16.0 | <0.01 * | 16.7 | <0.01 * | 4.9 | 0.03 * | |
| MBI | EE | −2.56 (9.47) | −2.92 (5.67) | 17.7 | <0.01 * | 6.7 | 0.01 * | <0.1 | 0.87 |
| DP | −0.62 (4.09) | 1.00 (4.08) | 2.5 | 0.12 | 0.3 | 0.56 | 1.0 | 0.32 | |
| PA | −0.94 (6.44) | −1.42 (4.23) | 10.4 | <0.01 * | 2.6 | 0.11 | 0.1 | 0.74 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matiz, A.; Fabbro, F.; Paschetto, A.; Cantone, D.; Paolone, A.R.; Crescentini, C. Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy. Int. J. Environ. Res. Public Health 2020, 17, 6450. https://doi.org/10.3390/ijerph17186450
Matiz A, Fabbro F, Paschetto A, Cantone D, Paolone AR, Crescentini C. Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy. International Journal of Environmental Research and Public Health. 2020; 17(18):6450. https://doi.org/10.3390/ijerph17186450
Chicago/Turabian StyleMatiz, Alessio, Franco Fabbro, Andrea Paschetto, Damiano Cantone, Anselmo Roberto Paolone, and Cristiano Crescentini. 2020. "Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy" International Journal of Environmental Research and Public Health 17, no. 18: 6450. https://doi.org/10.3390/ijerph17186450