Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus

 ,
, 
 and
and 
Abstract
:1. Introduction
Objectives: Peak Question
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Selection of Studies and Collection of Data
2.5. Assessment of the Quality of Studies: Detection of Possible Bias
2.6. Analysis of Data and Levels of Evidence
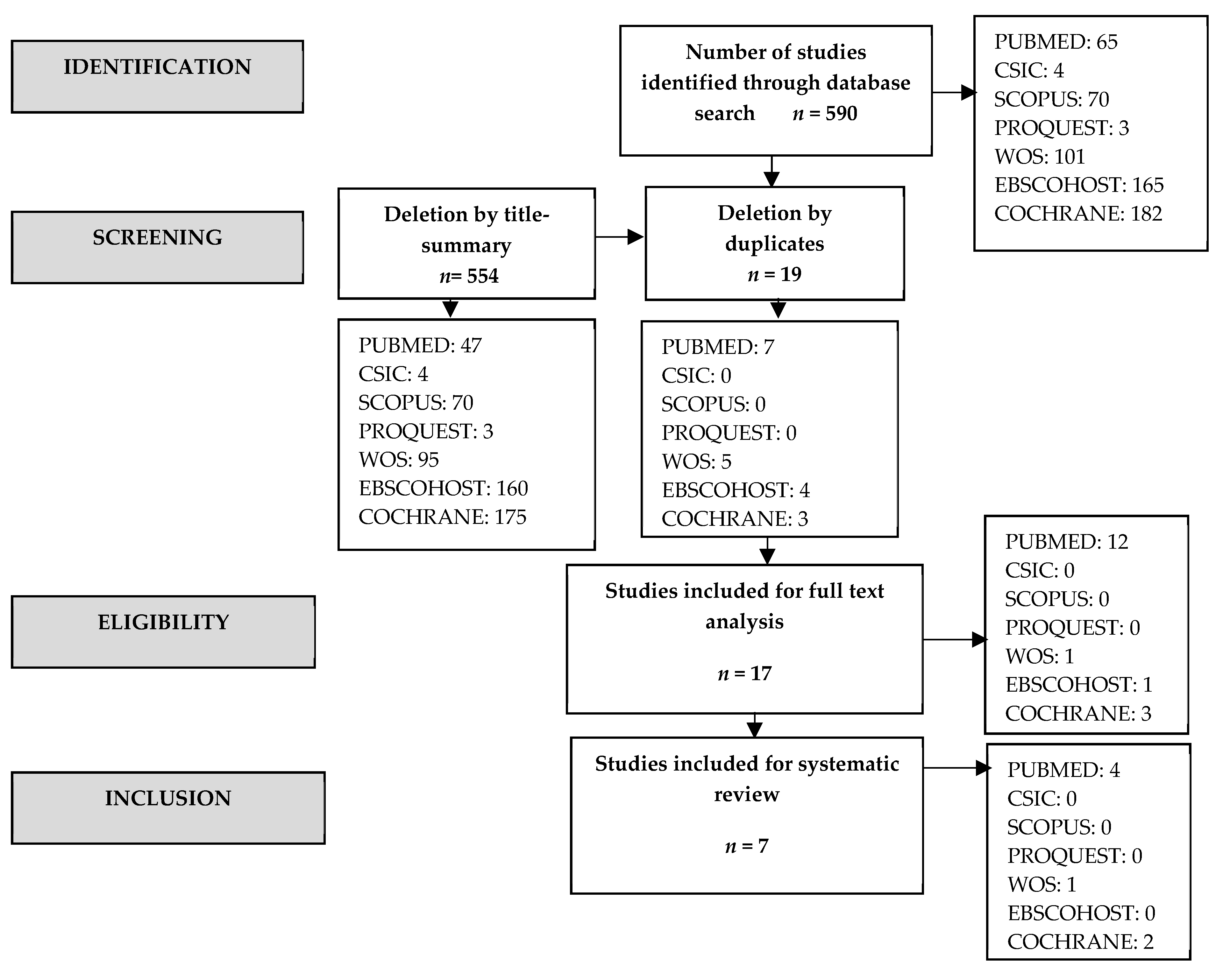
3. Results
4. Discussion
4.1. Physical Activity and Psychological Factors in Pregnant Women
4.2. Physical Activity and GDM Prevention
4.3. Strengths and Limitations
4.4. Implications for Clinical Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kassebaum, N.J.; Arora, M.; Barber, R.M.; Bhuttaq, Z.A.; Brow, J.; Carter, A.; Casey, D.C.; Charlson, F.J.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef] [Green Version]
- Andes, L.J.; Cheng, Y.J.; Rolka, D.B.; Gregg, E.W.; Imperatore, G. Prevalence of Prediabetes Among Adolescents and young adults in the United States, 2005–2016. JAMA Pediatr. 2020, 174, e194498. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Report on Diabetes. Available online: https://www.who.int/publications/i/item/global-report-on-diabetes (accessed on 20 January 2020).
- Duncan, M. On puerperal diabetes. Trans. Obs. Soc. Lond. 1882, 24, 256–285. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standard of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Pellonperä, O.; Mokkala, K.; Houttu, N.; Vahlberg, T.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Efficacy of fish oil and/or probiotic intervention on the incidence of gestational diabetes mellitus in an at-risk group of overweight and obese women: A randomized, placebo-controlled, double-blind clinical trial. Diabetes Care 2019, 42, 1009–1017. [Google Scholar] [CrossRef]
- Lipscombe, L.L.; Delos-Reyes, F.; Glenn, A.J.; Liang, X.; Grant, S.; Thorpe, K.E.; Price, J.A.D. The avoiding diabetes after pregnancy trial in moms program: Feasibility of a diabetes prevention program for women with recent gestational diabetes mellitus. Can. J. Diabetes 2019, 43, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Xu, S.; Li, P.; Li, L. Predictors of insulin treatment during pregnancy and abnormal postpartum glucose metabolism in patients with gestational diabetes mellitus. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2655–2665. [Google Scholar] [CrossRef] [Green Version]
- Salat, D.; Aguilera, C. Current treatment for gestational diabetes. Med. Clin. (Barc.) 2015, 145, 269–272. [Google Scholar] [CrossRef]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [Green Version]
- Trout, K.K.; Ellis, K.K.; Bratschie, A. Prevention of obesity and diabetes in childbearing women. J. Midwifery Womens Health 2013, 58, 297–302. [Google Scholar] [CrossRef]
- Márquez-Pardo, R.; Torres-Barea, I.; Córdoba-Doña, J.-A.; Cruzado-Begines, C.; García-García-Doncel, L.; Aguilar-Diosdado, M.; Baena-Nieto, M.G. Continuous glucose monitoring and glycemic patterns in pregnant women with gestational diabetes mellitus. Diabetes Technol. Ther. 2020, 22, 271–277. [Google Scholar] [CrossRef]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise, or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, E.G.; Reynolds, C.M.E.; Killalea, A.; O’Kelly, R.; Sheehan, S.R.; Turner, M.J. Maternal obesity and dyslipidemia associated with gestational diabetes mellitus (GDM). Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Ruchat, S.-M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- Song, C.; Li, J.; Leng, J.; Ma, R.C.; Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: A meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 960–969. [Google Scholar] [CrossRef]
- Sinclair, I.; St-Pierre, M.; Elgbeili, G.; Bernard, P.; Vaillancourt, C.; Gagnon, S.; Dancause, K.N. Psychosocial stress, sedentary behavior, and physical activity during pregnancy among Canadian women: Relationships in a diverse cohort and a nationwide sample. Int. J. Environ. Res. Public Health 2019, 16, 5150. [Google Scholar] [CrossRef] [Green Version]
- Dipietro, L.; Evenson, K.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E. Benefits of physical activity during pregnancy and postpartum. Med. Sci. Sport Exerc. 2019, 51, 1292–1302. [Google Scholar] [CrossRef]
- Collings, P.J.; Farrar, D.; Gibson, J.; West, J.; Barber, S.E.; Wright, J. associations of pregnancy physical activity with maternal cardiometabolic health, neonatal delivery outcomes and body composition in a biethnic cohort of 7305 mother–child pairs: The born in bradford study. Sport Med. 2020, 50, 615–628. [Google Scholar] [CrossRef] [Green Version]
- Barakat, R.; Pelaez, M.; Lopez, C.; Lucia, A.; Ruiz, J.R. Exercise during pregnancy and gestational diabetes-related adverse effects: A randomised controlled trial. Br. J. Sports Med. 2013, 47, 630–636. [Google Scholar] [CrossRef] [Green Version]
- Martis, R.; Crowther, C.A.; Shepherd, E.; Alsweiler, J.; Downie, M.R.; Brown, J. Treatments for women with gestational diabetes mellitus: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Stafne, S.N.; Salvesen, K.Å.; Romundstad, P.R.; Eggebø, T.M.; Carlsen, S.M.; Mørkved, S. Regular exercise during pregnancy to prevent gestational diabetes: A randomized controlled trial. Obstet. Gynecol. 2012, 119, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wei, Y.; Zhang, X.; Zhang, Y.; Xu, Q.; Sun, Y.; Su, S.; Zhang, L.; Liu, C.; Feng, Y.; et al. A randomized clinical trial of exercise during pregnancy to prevent gestational diabetes mellitus and improve pregnancy outcome in overweight and obese pregnant women. Am. J. Obstet. Gynecol. 2017, 216, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Middleton, P.; Crowther, C.A. Exercise for pregnant women for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; Berrington de Gonzalez, A.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality. JAMA Intern. Med. 2015, 175, 959. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee on Obstetric Practice. Committee opinion #267: Exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2002, 99, 171–173. [Google Scholar] [CrossRef]
- Gorgojo, M.J.J.; Almodóvar, R.F.; López, H.E.; Donnay, C.S. Incidence of gestational diabetes mellitus according to different diagnostic criteria in the southeast Madrid area. Influence of diagnosis on materno-fetal parameters. Rev. Clin. Esp. 2002, 202, 136–141. [Google Scholar] [CrossRef]
- Cardoso, R.C.; Gómez-Conesa, A.; Hidalgo, M.M.D. Metodología para la adaptación de instrumentos de evaluación. Fisioterapia 2010, 32, 264–270. [Google Scholar] [CrossRef]
- Cascaes, D.S.F.; Beatriz, A.V.A.T.; da Rosa, I.R.; Jose, B.G.F.P.; da Silva, R. Escalas y listas de evaluación de la calidad de estudios científicos. Rev. Cuba. Inf. Cienc. Salud 2013, 24, 295–312. [Google Scholar]
- Manterola, D.C.; Zavando, M.D. Cómo interpretar los "Niveles de Evidencia" en los diferentes escenarios clínicos. Rev. Chil. Cirugía. 2009, 61, 582–595. [Google Scholar] [CrossRef] [Green Version]
- Sklempe, K.I.; Ivanisevic, M.; Biolo, G.; Simunic, B.; Kokic, T.; Pisot, R. Combination of a structured aerobic and resistance exercise improves glycaemic control in pregnant women diagnosed with gestational diabetes mellitus. A randomised controlled trial. Women Birth 2018, 31, e232–e238. [Google Scholar] [CrossRef]
- Bo, S.; Rosato, R.; Ciccone, G.; Canil, S.; Gambino, R.; Poala, C.B.; Leone, F.; Valla, A.; Grassi, G.; Ghigo, E.; et al. Simple lifestyle recommendations and the outcomes of gestational diabetes. A 2×2 factorial randomized trial. Diabetes Obes. Metab. 2014, 16, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- De Barros, M.C.; Lopes, M.A.B.; Francisco, R.P.V.; Sapienza, A.D.; Zugaib, M. Resistance exercise and glycemic control in women with gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2010, 203, 556.e1–556.e6. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.H.; Mottola, M.F.; McManus, R.; Gratton, R. A walking intervention improves capillary glucose control in women with gestational diabetes mellitus: A pilot study. Appl. Physiol. Nutr. Metab. 2008, 33, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Youngwanichsetha, S.; Phumdoung, S.; Ingkathawornwong, T. The effects of mindfulness eating and yoga exercise on blood sugar levels of pregnant women with gestational diabetes mellitus. Appl. Nurs. Res. 2014, 27, 227–230. [Google Scholar] [CrossRef]
- Halse, R.E.; Wallman, K.E.; Newnham, J.P.; Guelfi, K.J. Home-based exercise training improves capillary glucose profile in women with gestational diabetes. Med. Sci. Sport Exerc. 2014, 46, 1702–1709. [Google Scholar] [CrossRef]
- Daniel, D.; Ibrahim, W. Aerobic dance exercise improves blood glucose level in pregnant women with gestational diabetes mellitus. Afr. J. Phys. Health Educ. Recreat. Danc. 2014, 20, 273–279. [Google Scholar]
- Peláez, P.M.; Casla, S.; Perales, M.; Cordero, R.Y.; Barakat, C.R. El ejercicio físico supervisado durante el embarazo mejora la percepción de la salud. Ensayo clínico aleatorizado. Retos: Nuevas Tendencias en Eductión Física, Deport y Recreación 2013, 2041, 36–38. [Google Scholar]
- Nakamura, A.; van der Waerden, J.; Melchior, M.; Bolze, C.; El-Khoury, F.; Pryor, L. Physical activity during pregnancy and postpartum depression: Systematic review and meta-analysis. J. Affect Disord. 2019, 246, 29–41. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Yin, H.; Zügel, M.; Sun, Z.; Steinacker, J.M.; Schumann, U. Association between circulating irisin and insulin resistance in non-diabetic adults: A meta-analysis. Metabolism 2016, 65, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, A.; Hedderson, M.M.; Albright, C.L.; Brown, S.D.; Ehrlich, S.F.; Caan, B.J.; Sternfeld, B.; Gordon, N.P.; Schmittdiel, J.A.; Gunderson, E.P.; et al. A pragmatic cluster randomized clinical trial of diabetes prevention strategies for women with gestational diabetes: Design and rationale of the gestational diabetes’ effects on moms (GEM) study. BMC Pregnancy Childbirth 2014, 14, 21. [Google Scholar] [CrossRef] [Green Version]
- Sanabria-Martínez, G.; García-Hermoso, A.; Poyatos-León, R.; Álvarez-Bueno, C.; Sánchez-López, M.; Martínez-Vizcaíno, V. Effectiveness of physical activity interventions on preventing gestational diabetes mellitus and excessive maternal weight gain: A meta-analysis. BJOG An. Int. J. Obstet. Gynaecol. 2015, 122, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, S.A.; Artal, R. The role of exercise in reducing the risks of gestational diabetes mellitus. Women’s Health 2013, 9, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Nobles, C.; Marcus, B.H.; Stanek, E.J.; Braun, B.; Whitcomb, B.W.; Solomon, C.G.; Manson, J.E.; Markenson, G.; Chasan-Taber, L. Effect of an exercise intervention on gestational diabetes mellitus. Obstet. Gynecol. 2015, 125, 1195–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Ma, H.; Hou, X.; Song, L.; Song, X.; Zhang, J. Reduced plasma level of irisin in first trimester as a risk factor for the development of gestational diabetes mellitus. Diabetes Res. Clin. Pract. 2018, 142, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Alka, P.; Kulandaivelan, S.; Savant, S.; Yadav, V.S. Home based exercise intervention in pregnant indian women: Effects on weight and obesity markers. Rom. J. Diabetes Nutr. Metab. Dis. 2018, 25, 131–139. [Google Scholar]
- Galliano, L.M.; Del Vecchio, A.H.M.; Silvani, J.; Façanha, C.; Del Vecchio, F.B. Physical activity level in women with gestational diabetes mellitus: Lifestyle INtervention for diabetes prevention after pregnancy (LINDA-Brasil) study. J. Diabetes 2019, 11, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Tobias, D.K.; Bowers, K.; Chavarro, J.; Vaag, A.; Grunnet, L.G.; Strøm, M.; Mills, J.; Liu, A.; Kiely, M.; et al. Physical activity and sedentary behaviors associated with risk of progression from gestational diabetes mellitus to type 2 diabetes mellitus. JAMA Intern. Med. 2014, 174, 1047. [Google Scholar] [CrossRef] [Green Version]
- Artal, R. The role of exercise in reducing the risks of gestational diabetes mellitus in obese women. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 123–132. [Google Scholar] [CrossRef]


{kind=link}
| Criterion (PICO) | Keywords |
|---|---|
| Population (P) | (pregnant) and (“gestational diabetes” or “type one diabetes” or “type i diabetes” or “type 1 diabetes” or “type two diabetes” or “type ii diabetes” or “type 2 diabetes”) |
| Intervention (I) | (“physical activity” or exercise or “exercise training” or “aerobic training” or “cardiorespiratory fitness” or “resistance training” or “resistance exercise” or “training intervention” or sport) |
| Outcome (O) | (“woman benefits” or “women benefits” or “woman effects” or “women effects”) |
| Author—Year | Type of Study | Type of Intervention | Sample Size | Results | Conclusions | Quality |
|---|---|---|---|---|---|---|
| Sklempe et al., 2017 [31] | ECA Randomization method: it is based on the web in two groups (experimental and control) Place: 2 university hospitals in Zagreb (Croatia). Participants were not blinded. Laboratory personnel and doctors were blinded. | EG: exercises twice a week → 50–55′ session + 30′ walking/day. 20′ aerobic activity (static tape with individualized intensity) + 20–25 resistance exercises (6 exercises in 3 sets of 10 to 15 repetitions with weight and elastic band) + pelvic exercises and stretching + 10’ relaxation. CG: standard care + unsupervised exercise. Program duration: 6 w minimum. Nutrition therapy for women with GDM at the beginning: 1800 kcal per day: 20% protein (90 g), 30% fat (60 g) and 50% carbohydrates (225 g), distributed in three main meals and three snacks. Postprandial and fasting glucose levels were measured 1 or 2 times a month during pregnancy. | N = 38 (18 EG, 20 CG) Inclusion criteria: pregnant women with GDM between 20 and 40 years. Characteristics: age (EG: 32.78 ± 3.83; CG: 31.95 ± 4.91); upper limit gestational age (30 w); diabetic family history (EG: 7; CG: 8); gestational age of diagnosis (EG: 22.44 ± 6.55; CG: 20.80 ± 6.05); sedentary lifestyle (EG: 25.16 ± 13.2; CG: 24.36 ± 17.09) | 365 exercise sessions. Intensity exercise between 3 and 14 in the Borg rating. 4.42% of maximum heart rate. Walking compliance > 70%. Moderate physical activity and transport levels during the 30th to 36th week of pregnancy > EG. No pharmacological treatment. Average fasting glucose < EG (p = 0.367). Postprandial glucose < EG (p < 0.001) No differences in weight gain or fat mass between both groups. No significant correlation was found between glycemic parameters and the duration of the intervention, adherence to the protocol or the number of assisted exercise sessions. | Aerobic exercises + resistance exercises → benefits for women with GDM. The EG had lower postprandial glucose levels at the end of pregnancy (p < 0.001). There was no significant difference between groups in the level of fasting glucose at the end of pregnancy. | 10/11 |
| Youngwanichsetha et al., 2014 [35] | ECA Randomization method: computer program and opaque envelopes. Place: tertiary hospital in southern Thailand. | CG: standard diabetes care. EG: standard diabetes care+ diet+ yoga during 8 w. 2 exercise sessions of 50’. Measures: fasting, postprandial glucose, and HbcA1. | 180 (90 CG; 90 EG) Inclusion criteria: pregnant women with GDM between 24–30 w (no insulin). Pregnant women who have no more complications in their pregnancy. Characteristics: mean age 32.58 (SD = 5.01) CG; 31.24 (SD = 4.54) EG. Plasma glucose after 100g test CG = 89.18 (SD = 12.84) and EG = 89.36 (SD = 13.19). | Fasting glucose average: EG: 83.39 mg/dL (SD = 17.69). CG: 85.85 mg/dL (SD = 17.94). (p = 0.012) Postprandial glucose average: EG: 105.67 mg/dL (SD = 12.93). CG: 112.36 mg/dL (SD = 13.15). (p = 0.001) HbA1C average: EG: 5.23% (SD = 0.72). CG: 5.68% (SD = 0.68). (p = 0.038) EG < fasting, postprandial glucose, and HbcA1. | The exercise intervention program is effective in improving glycemic control. | 10/11 |
| Bo et al., 2014 [32] | ECA Randomization method: web (www.epiclin.it) Place: hospital Sant’Anna (Torino) | Multiple interventions: GD, GB, GBE, GE Diet: carbohydrates 48–50%; protein 18–20%; fat 30–35%; fiber 20–25 g/day, not alcohol. GD → diet. GB: diet + behavior→oral or written recommendations. GBE: diet +exercise → walk 20’/da slightly. GE2: diet +recommendations + exercise → walk 20’ vigorously every day + group b recommendations. Duration: until the end of pregnancy (approx. 16 w). | 400 participants Inclusion criteria: pregnant women with GDM between 18–50 years and 24–26 w of gestation. | Weight, BMI, insulin, and dietary values (triglycerides and CPR concentration) → < in all groups. Postprandial glucose (p < 0.001) and HbA1c (p < 0.001) → < in the E/BE groups. Groups that do exercise (n = 101): Fasting glucose: 72.4 ± 10.3. Postprandial glucose: 106.1 ± 19.0. HbAc1: 4.6 ± 0.5. Groups that do not exercise (n = 99): Fasting glucose: 74.1 ± 10.7 Postprandial glucose: 117.2 ± 16.5 HbAc1: 4.9 ± 0.4. Groups that do exercise + diet + not recommendations (n = 101): Fasting glucose: 73.3 ± 10.1 Postprandial glucose: 113.0 ± 20.0 HbAc1: 4.8 ± 0.5 Groups that do exercise + diet + recommendations (n = 99): Fasting glucose: 73.2 ± 11.0 Postprandial glucose: 110.2 ± 17.1 HbAc1: 4.8 ± 0.4 | Exercise → ↓ postprandial glucose, triglycerides and CRP concentrations. Exercise + recommendations→ no significance (p > 0.3). Group D → > maternal/neonatal complications. Exercise + diet → ↓ maternal/neonatal complications. Recommendations or recommendations + exercise→ no ↓ maternal/neonatal complications. | 10/11 |
| Halse et al., 2014 [36] | ECNA Place: King Edward Memorial Hospital, Perth, Western Australia | Analyze fasting, postprandial glucose levels, HbA1c and glucose and insulin response to an oral glucose load of 75 g. Conventional care based on glycemic control 2 h after breakfast, lunch and dinner + educator advice + dietitian + food and beverage daily in the 1st and last. GE → 3 sessions of supervised exercise (exercise bike at home: 5’ low intensity 55-65% warm-up + 20–30’ pedalling of > intensity with intervals between 15–60’ higher intensity every 2’. The intensity was individualized for each woman The duration of the session was increased up to 45’ in the last + 5–10’ of low intensity and gentle stretching) + 2 sessions without the supervision of 30’ until s 34 + conventional care. Supervision: TA, pre and post-exercise glucose and intake of the last meal before exercise. GC→ 35 ± 8, → walking (52%), exercise bike (40%), water exercise (5%) and yoga (3%) + conventional care. | 40 participants (20 EG; 20 CG) Inclusion criteria: women with GDM, between 26–30 w of gestation, who had had an exploration of the normal anatomy in w 18, with a BMI < 45, non-smokers and not enrolled in any exercise program and who could perform physical activity. Characteristics: age (32 ± 3 → CG; 34 ± 5 → EG). | W 34 → glucose measurement and insulin response at 30, 60, 90, 120’ fasting according to GTT, HbcA1, physical activity level and nutritional status. EG → glucose response to exercise was 6.3 ± 08.mM pre-exercise at 4.9 ± 0.7mM post-exercise (p < 0.001). 62% of participants → capillary glucose was 1.0 mM pre to post. Half cc fasting blood glucose EG → more than the CG (p = 0.083) → No significance. CC postprandial glucose < in EG than in CG (p = 0.046). Glucose after breakfast < EG (p = 0.036); dinner (p = 0.054); lunch (p = 0.312) Post-intervention glucose not significant differences between EG and CG, insulin response CG (4.2 ± 2.3) and EG (5.0 ± 3.0) →(p > 0.05). HbcA1 → % > in post-intervention values in CG than in EG (p = 0.012) compared with pre-intervention values, without differences between groups (p > 0.05). Physical activity → EG > number of hours/w vs. CG. Feeding → CG > protein intake in the 1st s (p = 0.033) and last w (p = 0.009). HC > intake in EG in the last w (p = 0.035). | Cycling at home helps control postprandial glucose levels in women with GDM along with a proper diet. Supervision helps > adherence to exercise and change the lifestyle of these women. + research with + population and + exercise variety | 8/11 |
| De Barros et al., 2010 [33] | ECA Randomization method: web and opaque envelopes. Place: obstetric clinic, the university hospital of Sao Paulo (Brazil). | Diet: 7 servings → 35 cal/Kg per day + 300 Kcal/day in the day 2nd and 3rd quarter. CG → usual care. EG → wait for 90’ after eating and perform blood glucose. Exercise: resistance circuit of 8 exercises with an elastic band with 15 repetitions each exercise with a minimum of 30’ of rest and a maximum of 1’. 2nd quarter → 2 series of the circuit and 3rd quarter → 3 series. 3 times in w (1 under supervision). Moderate Intensity Glycemic profile every w. Insulin if > 30% glucose measurements > recommended value, hyperglycemia or baby weight > 75th percentile. | 64 participants (32 CG; 32 EG) Inclusion criteria: women with GDM, non-smokers, sedentary between 18–45 years, without the disease, gestational age between 24–34 w. Characteristics: age CG → 32.4 ± 5.40; EG → 31.81 ± 4.87. | Insulin requirement: CG → 18 (56,3%) EG→ 7 (21.9%) Amount of insulin required IU/kg: CG → 0.49 ± 0.14 EG → 0.44 ± 0.11 Average glucose levels: CG → 102.89 ± 7.88 EG→ 100.30 ± 9.37 | The resistenace exercise program with elastic band was effective in reducing the number of patients requiring insulin and to control glucose levels in women with GDM | 11/11 |
| Davenport et al., 2008 [34] | Case-control study Place: London. | 2 groups were established: CG: conventional treatment: nutritionist advice every 2 w. Objectives: 2000 Kcal/day. 200 g CH in 3 meals and 3 drinks + glucose measurement + regular monitoring with your doctor. EG: hike (3–4 times at w increasing from 2’ to reach 40’ the last w. Duration: 6 w) + conventional treatment. Inclusion criteria: women with GDM, without pathology in pregnancy, and with follow-up from their doctor. | 30 women → 10 EG and 20 CG. Characteristics: age → CG: 33.3 ± 5.3; EG: 33.48 ± 7.1. BMI before pregnancy → CG: 32.8 ± 5.9; EG: 32.92 ± 7.1.; Weight gained during pregnancy → CG: 12.7 ± 8.4. EG: 12.0 ± 9.7 | Participants that require insulin: CG: 70%. EG: 70%. Glucose values at treatment: EG: < at the end of pregnancy tan the CG. CG capillary glucose 1 h after dinner increased at the end of the arm compared to the beginning. Amount of insulin: EG: 0.16 ± 0.13 U/kg → required less frequently. CG: 0.5 ± 0.37 U/kg. | Glucose concentration can be improved, as well as reducing the amount and frequency of insulin injection in women with GDM who walk. | 7/9 |
| Daniel et al., 2014 [37] | ECA Randomization method: random assignment to the GE/GC. Place: Owerri, Nigeria. | EG: dance exercises for 8 w. Warm-up (low-intensity aerobic exercises) and 5–10’ stretching + Dance: 10–20’ cardio-respiratory exercises (low-moderate intensity) such as fast walking. The duration increased from 40 to 60’ after 4 w + strengthening exercises (pelvic floor and abdominal muscle exercise)+ stretching and cooling 5–10’. CG: no exercise program. Fasting glucose level at the beginning. 4 and 8 w. | 30 participants (15 EG; 15 CG) Inclusion criteria: women with > 24 w of gestation diagnosed with GDM suitable for exercise. Charactristics: age → EG 32 ± 3.42; CG 32.93 ± 4.61. Gestational age (weeks) → EG: 26.8 ± 0.94; CG 26.33 ± 0.98. | Fasting glucose: Start: EG(144.53; SD: 6.96); CG (145.07; SD: 8.19), (p = 0.85). S 4: EG (118.63; SD:10.73); CG (142.73; SD: 6.96) (p = 0.001) S 8: EG (87.67; SD: 11.84); CG (141.53; SD: 6.82) (p = 0.001) | Significant effect of the exercise program. Exercises 3 times per w between 40–60’ per session at moderate intensity reduces blood glucose. | 8/11 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laredo-Aguilera, J.A.; Gallardo-Bravo, M.; Rabanales-Sotos, J.A.; Cobo-Cuenca, A.I.; Carmona-Torres, J.M. Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 17, 6151. https://doi.org/10.3390/ijerph17176151
Laredo-Aguilera JA, Gallardo-Bravo M, Rabanales-Sotos JA, Cobo-Cuenca AI, Carmona-Torres JM. Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus. International Journal of Environmental Research and Public Health. 2020; 17(17):6151. https://doi.org/10.3390/ijerph17176151
Chicago/Turabian StyleLaredo-Aguilera, José Alberto, María Gallardo-Bravo, Joseba Aingerun Rabanales-Sotos, Ana Isabel Cobo-Cuenca, and Juan Manuel Carmona-Torres. 2020. "Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus" International Journal of Environmental Research and Public Health 17, no. 17: 6151. https://doi.org/10.3390/ijerph17176151
APA StyleLaredo-Aguilera, J. A., Gallardo-Bravo, M., Rabanales-Sotos, J. A., Cobo-Cuenca, A. I., & Carmona-Torres, J. M. (2020). Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus. International Journal of Environmental Research and Public Health, 17(17), 6151. https://doi.org/10.3390/ijerph17176151