Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing


 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Sample
2.2. Body Composition Measurement Procedure
2.3. Variables
2.3.1. Primary Body Composition Variables
- FFM—fat-free body mass, expressed in kg;
- PM—total body protein mass, expressed in kg;
- SMM—skeletal muscle mass, expressed in kg;
2.3.2. Longitudality-Independent Body Composition Variables
- FFMI—fat-free mass index, expressed in kg/m2;
- SMMI—body skeletal muscle mass index, expressed in kg/m2;
- PMI—body protein mass index, expressed in kg/m2.
2.3.3. Voluminosity-Independent Body Composition Variables
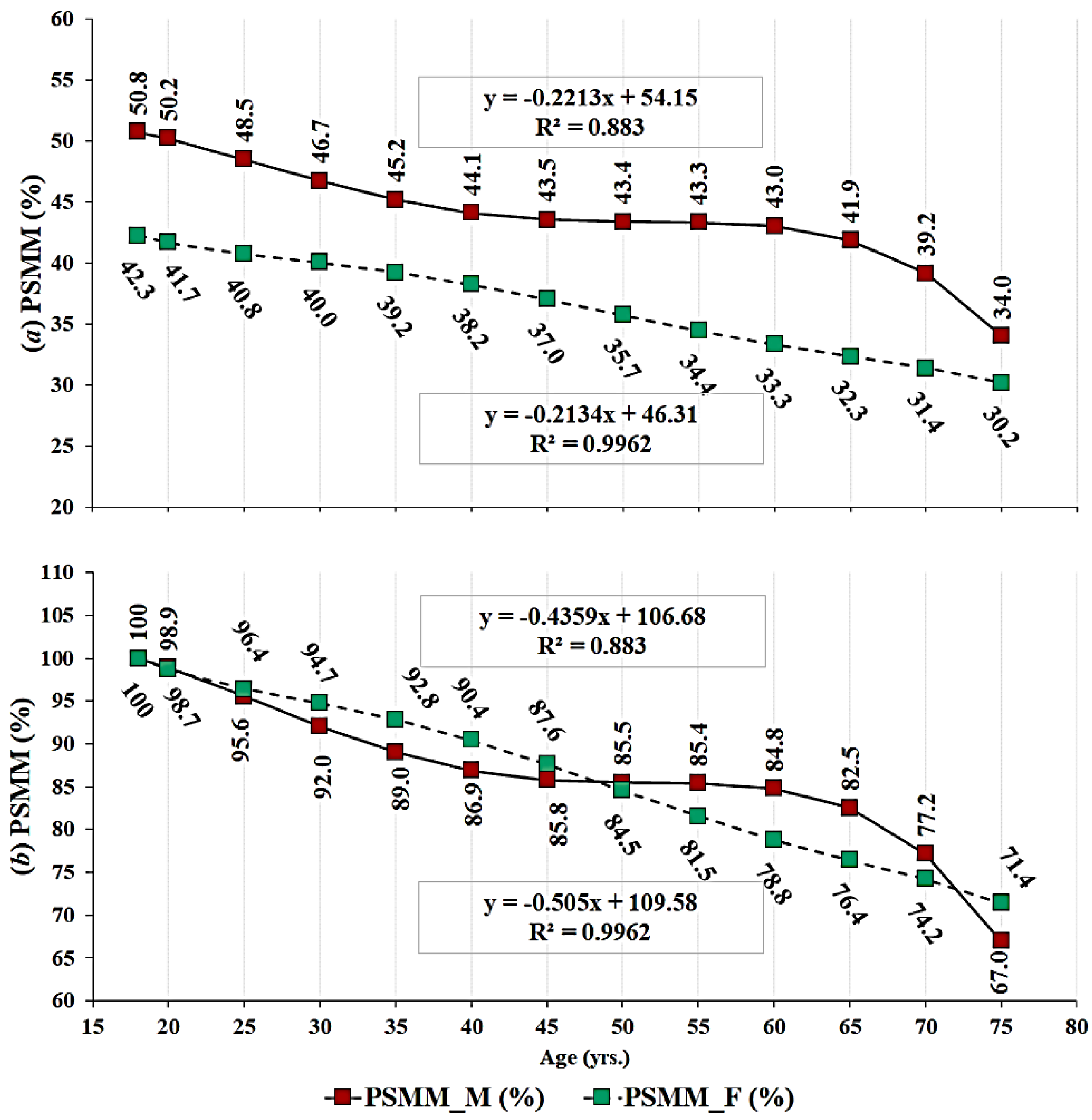
- PSMM—percent skeletal muscle mass, expressed in %;
- PP—percent protein mass, expressed in %.
2.3.4. Combined Body Tissue Index Variables
- PFI—protein and total body fat ratio index.
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Malina, R.M.; Bouchard, C. Growth, Maturation, and Physical Activity; Human Kinetics Academic: Champaign, IL, USA, 1991; ISBN 978-0-87322-321-8. [Google Scholar]
- Kirchengast, S. Gender differences in body composition from childhood to old age: An evolutionary point of view. J. Life Sci. 2010, 2, 1–10. [Google Scholar] [CrossRef]
- Kukic, F.; Koropanovski, N.; Jankovic, R.; Cvorovic, A.; Dawes, J.J.; Lockie, G.R.; Orr, R.M.; Dopsaj, M. Association of sex-related differences in body composition to change of direction speed in police officers while carrying load. Int. J. Morphol. 2020, 38, 731–736. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukic, F.; Scekic, A.; Koropanovski, N.; Cvorovic, A.; Dawes, J.J.; Dopsaj, M. Age-related body composition differences in female police officers. Int. J. Morphol. 2019, 37, 302–307. [Google Scholar] [CrossRef] [Green Version]
- Sillanpää, E.; Cheng, S.; Häkkinen, K.; Finni, T.; Walker, S.; Pesola, A.; Ahtiainen, J.; Stenroth, L.; Selänne, H.; Sipilä, S. Body composition in 18- to 88-year-old adults—Comparison of multifrequency bioimpedance and dual-energy X-ray absorptiometry. Obesity 2014, 22, 101–109. [Google Scholar] [CrossRef]
- Candow, D.G.; Chilibeck, P.D.; Abeysekara, S.; Zello, G.A. Short-term heavy resistance training eliminates age-related deficits in muscle mass and strength in healthy older males. J. Strength Cond. Res. 2011, 25, 326–333. [Google Scholar] [CrossRef]
- Dopsaj, M.; Markovic, M.; Kasum, G.; Jovanovic, S.; Koropanovski, N.; Vukovic, M.; Mudric, M. Discrimination of different body structure indexes of elite athletes in combat sports measured by multi frequency bioimpedance method. Int. J. Morphol. 2017, 35, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Čvorović, A.; Kukić, F.; Orr, R.M.; Dawes, J.J.; Jeknić, V.; Stojković, M. Impact of a 12-week postgraduate training course on the body composition and physical abilities of police trainees. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef]
- Vuković, M.; Kukić, F.; Čvorović, A.; Janković, D.; Prćić, I.; Dopsaj, M. Relations between frequency and volume of leisure-time physical activity and body composition in police officers. Res. Quart. Exerc. Sport 2020, 91, 47–54. [Google Scholar] [CrossRef]
- Wang, Z.; Pierson, R.N.; Heymsfield, S.B. The five-level model: A new approach to organizing body-composition research. Am. J. Clin. Nutr. 1992, 56, 19–28. [Google Scholar] [CrossRef]
- Hu, F.B. Obesity Epidemiology; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Wang, Z.; St-Onge, M.-P.; Lecumberri, B.; Pi-Sunyer, F.X.; Heshka, S.; Wang, J.; Kotler, D.P.; Gallagher, D.; Wielopolski, L.; Pierson, R.N.; et al. Body cell mass: Model development and validation at the cellular level of body composition. Am. J. Physiol. Endocrinol. Metab. 2004, 286, E123–E128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on sarcopenia in older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aandstad, A.; Holtberget, K.; Hageberg, R.; Holme, I.; Anderssen, S.A. Validity and reliability of bioelectrical impedance analysis and skinfold thickness in predicting body fat in military personnel. Military Med. 2014, 179, 208–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemble, C.D.; Mun, J.; Rowe, D.A.; DuBose, K.D.; Raedeke, T.D.; Mahar, M.T. Accuracy of bioelectrical impedance analyzers in college athletes: Does hydration matter? J. Strength Cond. Res. 2010, 24. [Google Scholar] [CrossRef]
- Laskey, M.A. Dual-energy X-ray absorptiometry and body composition. Nutrition 1996, 12, 45–51. [Google Scholar] [CrossRef]
- Biaggi, R.R.; Vollman, M.W.; Nies, M.A.; Brener, C.E.; Flakoll, P.J.; Levenhagen, D.K.; Sun, M.; Karabulut, Z.; Chen, K.Y. Comparison of air-displacement plethysmography with hydrostatic weighing and bioelectrical impedance analysis for the assessment of body composition in healthy adults. Am. J. Clin. Nutr. 1999, 69, 898–903. [Google Scholar] [CrossRef] [Green Version]
- Walowski, C.O.; Braun, W.; Maisch, M.J.; Jensen, B.; Peine, S.; Norman, K.; Müller, M.J.; Bosy-Westphal, A. Reference values for skeletal muscle mass—Current concepts and methodological considerations. Nutrients 2020, 12, 755. [Google Scholar] [CrossRef] [Green Version]
- Kukic, F.; Dopsaj, M.; Dawes, J.; Orr, R.; Cvorovic, A. Use of human body morphology as an indicator of physical fitness: Implications for police officers. Int. J. Morphol. 2018, 36, 1407–1412. [Google Scholar] [CrossRef]
- Rakic, S.; Dopsaj, M.; Djordjevic-Nikic, M.; Vasiljevic, N.; Dopsaj, V.; Maksimovic, M.; Tomanic, S.M.; Miljus, D. Profile and reference values for body fat and skeletal muscle mass percent at females, aged from 18.0 to 69.9, measured by multichannel segmental bioimpedance method: Serbian population study. Int. J. Morphol. 2019, 37, 1286–1293. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzolino, D.; Arosio, B.; Marzetti, E.; Calvani, R.; Cesari, M. Nutritional status as a mediator of fatigue and its underlying mechanisms in older people. Nutrients 2020, 12, 444. [Google Scholar] [CrossRef] [Green Version]
- Buffa, R.; Floris, G.U.; Putzu, P.F.; Marini, E. Body composition variations in ageing. Coll. Antropol. 2011, 35, 259–265. [Google Scholar] [PubMed]
- Demontis, F.; Piccirillo, R.; Goldberg, A.L.; Perrimon, N. The influence of skeletal muscle on systemic aging and lifespan. Aging Cell 2013, 12, 943–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlier, R.; Mertens, E.; Lefevre, J.; Thomis, M. Muscle mass and muscle function over the adult life span: A cross-sectional study in Flemish adults. Arch. Gerontol. Geriatr. 2015, 61, 161–167. [Google Scholar] [CrossRef]
- Kukic, F.; Cvorovic, A.; Dawes, J.; Orr, R.M.; Dopsaj, M. Relations of body voluminosity and indicators of muscularity with physical performance of police employees: Pilot study. Balt. J. Sport Health Sci. 2018, 4, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cut points associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef]
- Jackson, A.S.; Janssen, I.; Sui, X.; Church, T.S.; Blair, S.N. Longitudinal changes in body composition associated with healthy ageing: Men, aged 20–96 years. Br. J. Nutr. 2012, 107, 1085–1091. [Google Scholar] [CrossRef] [Green Version]
- Vadala, M. Energy restoration by an original fruits & vegetables juice intake in a cohort of elderly people affected by Sarcopenia. Int. J. Sports Exerc. Med. 2016, 2, 46. [Google Scholar] [CrossRef]
- Schaap, L.A.; Pluijm, S.M.F.; Deeg, D.J.H.; Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Williams, J.R. The declaration of Helsinki and public health. Bull. World Health Organ. 2008, 86, 650–652. [Google Scholar] [CrossRef]
- Estimates of Population. Statistical Office of the Republic of Serbia. Available online: https://www.stat.gov.rs/en-US/oblasti/stanovnistvo/procene-stanovnistva (accessed on 28 April 2020).
- Ling, C.H.Y.; de Craen, A.J.M.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.M.; Westendorp, R.G.J.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukić, F.; Todorović, N.; Cvijanović, N. Effects of a 6-week controled exercise program and semi-controled diet on body fat and skeletal muscle mass in adults. Hum. Sport. Med. 2019, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Dopsaj, M.; Mijalkovski, Z.; Ćopić, N.; Brzaković, M.; Marković, M. Morphological parameters and handgrip muscle force contractile characteristics in the first selection level in water polo: Differences between U15 water polo players and the control group. Hum. Sport. Med. 2018, 18, 5–15. [Google Scholar] [CrossRef]
- Saraykin, D.A.; Khusnutdinova, A.A.; Pavlova, V.I.; Kamskova, Y.G.; Yushkov, B.G. Adaptation of professional athletes to various physical loads by means of body composition changes. Hum. Sport. Med. 2018, 18, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Dopsaj, M.; Ilic, V.; Djordjevic-Nikic, M.; Vukovic, M.; Eminovic, F.; Macura, M.; Ilic, D. Descriptive model and gender dimorphism of body structure of physically active students of Belgrade University: Pilot Study. Anthropologist 2015, 19, 239–248. [Google Scholar] [CrossRef]
- Wells, J.C.K. Sexual dimorphism of body composition. Best Prac. Res. Clin. Endocrinol. Metab. 2007, 21, 415–430. [Google Scholar] [CrossRef]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Megal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- WHO. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 24 March 2019).
- Wilson, L.A.B.; de Groote, I.; Humphrey, L.T. Sex differences in the patterning of age-related bone loss in the human hallucal metatarsal in rural and urban populations. Am. J. Phys. Anthropol. 2020, 171, 628–644. [Google Scholar] [CrossRef]
- Su, Y.; Yuki, M.; Hirayama, K.; Sato, M.; Han, T. Denture wearing and malnutrition risk among community-dwelling older adults. Nutrients 2020, 12, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinsa, G.D.; Goryakin, Y.; Fumagalli, E.; Suhrcke, M. Obesity and socioeconomic status in developing countries: A systematic review. Obes. Rev. 2012, 13, 1067–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Lee, K.; Kwan, M.-P. Environmental influences on leisure-time physical inactivity in the U.S.: An exploration of spatial non-stationarity. ISPRS Int. J. Geo. Inf. 2018, 7, 143. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Sex | Variables | 18–29.9 | 30–39.9 | 40–49.9 | 50–59.9 | 60–69.9 | 70–79.9 | ANOVA |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Males | PM (kg) ** | 14.16 ± 1.76 | 14.19 ± 1.81 | 14.06 ± 1.71 | 13.64 ± 1.65 | 13.01 ± 1.72 | 11.05 ± 1.59 | F = 14.54, PE2 = 0.01 |
| PP (%) ** | 17.14 ± 1.36 | 15.65 ± 1.46 | 15.36 ± 1.34 | 15.02 ± 1.11 | 14.32 ± 1.52 | 13.58 ± 0.89 | F = 411.46, PE2 = 0.28 | |
| PMI (kg/m2) ** | 4.22 ± 0.35 | 4.28 ± 0.38 | 4.28 ± 0.37 | 4.2 ± 0.29 | 4.05 ± 0.41 | 3.72 ± 0.31 | F = 14.59, PE2 = 0.01 | |
| SMM (kg) ** | 40.73 ± 5.31 | 40.78 ± 5.53 | 40.4 ± 5.13 | 39.12 ± 4.98 | 37.24 ± 5.19 | 30.91 ± 4.82 | F = 14.86, PE2 = 0.01 | |
| PSMM (%) ** | 49.27 ± 3.96 | 44.95 ± 4.28 | 44.12 ± 3.88 | 43.04 ± 3.17 | 40.94 ± 4.3 | 37.94 ± 2.68 | F = 409.57, PE2 = 0.28 | |
| SMMI (kg/m2) ** | 12.13 ± 1.06 | 12.3 ± 1.18 | 12.29 ± 1.13 | 12.04 ± 0.9 | 11.59 ± 1.23 | 10.39 ± 1.03 | F = 14.73, PE2 = 0.01 | |
| PFI (kg) ** | 1.596 ± 0.98 | 0.874 ± 0.46 | 0.784 ± 0.40 | 0.673 ± 0.22 | 0.599 ± 0.23 | 0.466 ± 0.08 | F = 273.55, PE2 = 0.20 | |
| FFM (kg) ** | 71.1 ± 8.95 | 71.49 ± 9.18 | 71.00 ± 8.86 | 69.01 ± 8.39 | 66.91 ± 9.43 | 57.13 ± 8.63 | F = 9.69, PE2 = 0.01 | |
| FFMI (kg/m2) ** | 21.19 ± 1.75 | 21.56 ± 1.90 | 21.6 ± 1.94 | 21.24 ± 1.46 | 20.84 ± 2.37 | 19.20 ± 1.76 | F = 14.60, PE2 = 0.01 | |
| Females | PM (kg) ** | 9.31 ± 1.37 | 9.55 ± 1.09 | 9.49 ± 1.04 | 9.02 ± 1.11 | 9.19 ± 1.54 | 7.89 ± 0.67 | F = 11.54, PE2 = 0.02 |
| PP (%) | 14.76 ± 1.56 | 13.95 ± 1.79 | 13.43 ± 1.61 | 12.54 ± 1.51 | 11.86 ± 1.48 | 11.84 ± 1.09 | F = 156.64, PE2 = 0.19 | |
| PMI (kg/m2) ** | 3.22 ± 0.31 | 3.34 ± 0.33 | 3.37 ± 0.29 | 3.33 ± 0.32 | 3.45 ± 0.48 | 3.29 ± 0.17 | F = 30.30, PE2 = 0.04 | |
| SMM (kg) | 26.09 ± 4.17 | 26.81 ± 3.31 | 26.66 ± 3.13 | 25.22 ± 3.34 | 25.73 ± 4.66 | 21.75 ± 2.05 | F = 11.61, PE2 = 0.02 | |
| PSMM (%) ** | 41.29 ± 4.49 | 39.14 ± 5.04 | 37.66 ± 4.55 | 35.01 ± 4.21 | 33.13 ± 4.09 | 32.63 ± 3.07 | F = 151.77, PE2 = 0.19 | |
| SMMI (kg/m2) ** | 9.03 ± 0.98 | 9.37 ± 1.01 | 9.46 ± 0.87 | 9.29 ± 0.96 | 9.67 ± 0.46 | 9.09 ± 0.54 | F = 26.12, PE2 = 0.04 | |
| PFI (kg) ** | 0.671 ± 0.31 | 0.563 ± 0.28 | 0.473 ± 0.20 | 0.378 ± 0.14 | 0.332 ± 0.15 | 0.322 ± 0.07 | F = 92.77, PE2 = 0.12 | |
| FFM (kg) ** | 47.34 ± 6.87 | 48.67 ± 5.51 | 48.43 ± 5.33 | 46.18 ± 5.82 | 47.49 ± 8.25 | 41.53 ± 4.30 | F = 10.55, PE2 = 0.02 | |
| FFMI (kg/m2) ** | 16.39 ± 1.53 | 17.02 ± 1.63 | 17.19 ± 1.46 | 17.03 ± 1.66 | 17.86 ± 2.75 | 17.34 ± 1.07 | F = 40.34, PE2 = 0.06 |
| Variables | Pearson Correlation | Fisher r-to-z Transformation | p | |
|---|---|---|---|---|
| Male | Female | |||
| PM (kg) | −0.065 ** | −0.034 | −1.413 | 0.079 |
| PP (%) | −0.517 ** | −0.443 ** | −4.378 | 0.000 |
| PMI (kg/m2) | 0.015 | 0.165 ** | −6.890 | 0.000 |
| SMM (kg) | −0.066 ** | −0.033 | −1.504 | 0.066 |
| PSMM (%) | −0.516 ** | −0.438 ** | −4.598 | 0.000 |
| SMMI (kg/m2) | 0.008 | 0.148 ** | −6.416 | 0.000 |
| PFI (kg) | −0.432 ** | −0.354 ** | −4.199 | 0.000 |
| FFM (kg) | −0.038 * | −0.010 | −1.274 | 0.101 |
| FFMI (kg/m2) | 0.055 ** | 0.200 ** | −6.716 | 0.006 |
| Variables | Component—Female | Variables | Component—Male | ||
|---|---|---|---|---|---|
| 1 | 2 | 1 | 2 | ||
| SMMI | 0.939 | −0.135 | SMMI | 0.946 | −0.040 |
| SMM | 0.935 | 0.196 | SMM | 0.944 | 0.151 |
| PM | 0.934 | 0.200 | PM | 0.943 | 0.147 |
| FFM | 0.928 | 0.175 | FFMI | 0.938 | −0.102 |
| PMI | 0.926 | −0.163 | FFM | 0.937 | 0.116 |
| FFMI | 0.919 | −0.201 | PMI | 0.934 | −0.059 |
| PSMM | 0.015 | 0.983 | PSMM | 0.041 | 0.977 |
| PP | −0.062 | 0.980 | PP | −0.018 | 0.975 |
| PFI | 0.078 | 0.930 | PFI | 0.079 | 0.897 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dopsaj, M.; Kukić, F.; Đorđević-Nikić, M.; Koropanovski, N.; Radovanović, D.; Miljuš, D.; Subošić, D.; Tomanić, M.; Dopsaj, V. Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing. Int. J. Environ. Res. Public Health 2020, 17, 5977. https://doi.org/10.3390/ijerph17165977
Dopsaj M, Kukić F, Đorđević-Nikić M, Koropanovski N, Radovanović D, Miljuš D, Subošić D, Tomanić M, Dopsaj V. Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing. International Journal of Environmental Research and Public Health. 2020; 17(16):5977. https://doi.org/10.3390/ijerph17165977
Chicago/Turabian StyleDopsaj, Milivoj, Filip Kukić, Marina Đorđević-Nikić, Nenad Koropanovski, Dragan Radovanović, Dragan Miljuš, Dane Subošić, Milena Tomanić, and Violeta Dopsaj. 2020. "Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing" International Journal of Environmental Research and Public Health 17, no. 16: 5977. https://doi.org/10.3390/ijerph17165977