Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population

 , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Self-Report Measures
2.2.1. Study Presentation and Informed Consent
2.2.2. Personal History
2.2.3. Food Habits
2.2.4. Physical Activity Patterns
2.3. Data Analyses
3. Results
3.1. Sociodemographic Characteristics of the Study Sample
3.2. Physical Activity and Food Habits
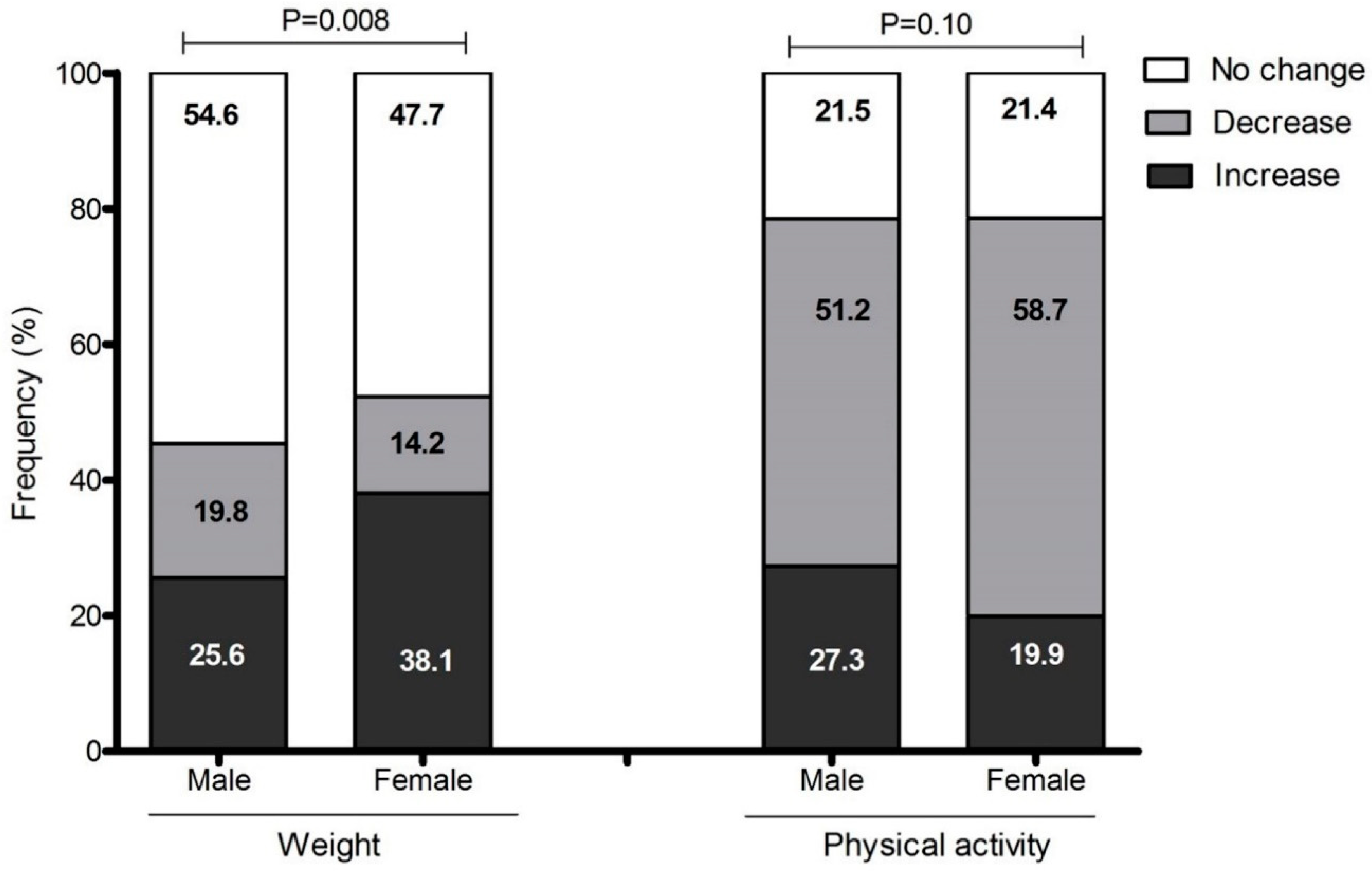
3.3. Body Weight Changes
3.4. Association of Variables with Bodyweight Increase and PA Decrease
4. Discussion
5. Strengths and Limitations
6. Contributions of this Study
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Pandemic Statement by World Health Organization. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 22 June 2020).
- Chilean Health Ministry. Coronavirus-COVID-19 Action Plan, Chile 2020. Available online: https://www.gob.cl/coronavirus/plandeaccion/ (accessed on 18 July 2020).
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Bermúdez, C.; Pereira, F.J.; Trejos-Gallego, D.; Pérez, A.; Puentes, M.; López, L.M.; García, C.P.; Parada, E.M.; Peláez, M.E.M.; Ramírez, J.O.; et al. Recomendaciones nutricionales de la Asociación Colombiana de Nutrición Clínica para pacientes hospitalizados con infección por SARS-CoV-2. Rev. Nutr. Clin. Metab. 2020, 3, 74–85. [Google Scholar] [CrossRef]
- Bhutani, S.; A Cooper, J. COVID-19 related home confinement in adults: Weight gain risks and opportunities. Obesity 2020. [Google Scholar] [CrossRef]
- Dietz, W.; Santos-Burgoa, C. Obesity and its Implications for COVID-19 Mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef] [Green Version]
- OCDE. Overweight and Obese Population in Chile 2019. Available online: https://www.oecd.org/health/health-systems/Revisi%C3%B3n-OCDE-de-Salud-P%C3%BAblica-Chile-Evaluaci%C3%B3n-y-recomendaciones.pdf (accessed on 23 June 2020).
- Dietitians-Nutritionist CG. Food and Nutrition Recommendations for the Spanish Population in the Face of the COVID-19 Health Crisis. 2020. Available online: https://academianutricionydietetica.org/NOTICIAS/alimentacioncoronavirus.pdf (accessed on 20 June 2020).
- Butler, M.J.; Barrientos, R.M. The impact of nutrition on COVID-19 susceptibility and long-term consequences. Brain Behav. Immun. 2020, 87, 53–54. [Google Scholar] [CrossRef]
- Green, W.D.; Beck, M.A. Obesity Impairs the Adaptive Immune Response to Influenza Virus. Ann. Am. Thorac. Soc. 2017, 14, S406–S409. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Healthy at Home-Physical Activity. WHO: Switzerland. 2020. Available online: https://www.who.int/news-room/campaigns/connecting-the-world-to-combat-coronavirus/healthyathome/healthyathome---physical-activity (accessed on 20 July 2020).
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B.; Miranda, C.; Stein, M. Impact of Home Quarantine on Physical Activity Among Older Adults Living at Home During the COVID-19 Pandemic: Qualitative Interview Study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Alles, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M. Diet and physical activity during the COVID-19 lockdown period (March-May 2020): Results from the French NutriNet-Sante cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Olivares, S.; Zacarías, I. Study to Review and Update the Dietary Guidelines for the Chilean Population. Santiago: Chilean Ministry of Health 2013. Available online: https://www.minsal.cl/portal/url/item/dde0bc471a56a001e040010165012224.pdf (accessed on 19 June 2020).
- McCrory, M.A.; Hamaker, B.R.; Lovejoy, J.C.; Eichelsdoerfer, P.E. Pulse Consumption, Satiety, and Weight Management1. Adv. Nutr. 2010, 1, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramdath, D.; Renwick, S.; Duncan, A.M. The Role of Pulses in the Dietary Management of Diabetes. Can. J. Diabetes 2016, 40, 355–363. [Google Scholar] [CrossRef] [PubMed]
- USDA. Dietary Guidelines for Americans. US Department of Health and Human Services and US Department of Agriculture. 2015. Available online: https://health.gov/sites/default/files/2019-09/2015-2020_Dietary_Guidelines.pdf (accessed on 19 June 2020).
- Kimmons, J.E.; Gillespie, C.; Seymour, J.; Serdula, M.; Blanck, H.M. Fruit and Vegetable Intake among Adolescents and Adults in the United States: Percentage Meeting Individualized Recommendations. Medscape J. Med. 2009, 11, 26. [Google Scholar] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruiz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Nutritional recommendations for CoVID-19 quarantine. Eur. J. Clin. Nutr. 2020, 74, 850–851. [Google Scholar] [CrossRef]
- Carr, K.A.; Daniel, T.O.; Lin, H.; Epstein, L.H. Reinforcement pathology and obesity. Curr. Drug Abus. Rev. 2011, 4, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oginsky, M.F.; Goforth, P.B.; Nobile, C.W.; Lopez-Santiago, L.F.; Ferrario, C.R. Eating ’Junk-Food’ Produces Rapid and Long-Lasting Increases in NAc CP-AMPA Receptors: Implications for Enhanced Cue-Induced Motivation and Food Addiction. Neuropsychopharmacology 2016, 41, 2977–2986. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Bhutani, S.A.; Cooper, J.; Vandellen, M.R. Self-reported changes in energy balance behaviors during COVID-19 related home confinement: A Cross-Sectional Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Zheng, M.; Rangan, A.; Olsen, N.J.; Andersen, L.B.; Wedderkopp, N.; Kristensen, P.; Grøntved, A.; Ried-Larsen, M.; Lempert, S.M.; Allman-Farinelli, M.; et al. Substituting sugar-sweetened beverages with water or milk is inversely associated with body fatness development from childhood to adolescence. Nutrients 2015, 31, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Salari-Moghaddam, A.; Aslani, N.; Saneei, P.; Keshteli, A.H.; Daneshpajouhnejad, P.; Esmaillzadeh, A.; Adibi, P. Water intake and intra-meal fluid consumption in relation to general and abdominal obesity of Iranian adults. Nutr. J. 2020, 19, 39–48. [Google Scholar] [CrossRef]
- Stookey, J.D.; Constant, F.; Popkin, B.M.; Gardner, C.D. Drinking Water Is Associated With Weight Loss in Overweight Dieting Women Independent of Diet and Activity. Obesisty 2008, 16, 2481–2488. [Google Scholar] [CrossRef]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Bulló, M.; Lamuela-Raventós, R.M.; Salas-Salvadó, J. Mediterranean diet and oxidation: Nuts and olive oil as important sources of fat and antioxidants. Curr. Top. Med. Chem. 2011, 11, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.P.; Aggarwal, K.K.; Zhang, P.-Y. Omega-3 fatty acids and cardiovascular disease. Eur. Rev. Med Pharmacol. Sci. 2015, 19, 441–445. [Google Scholar] [PubMed]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Jakobsson, J.; Malm, C.; Furberg, M.; Ekelund, U.; Svensson, M. Physical Activity During the Coronavirus (COVID-19) Pandemic: Prevention of a Decline in Metabolic and Immunological Functions. Front. Sports Act. Living 2020, 2, 57. [Google Scholar] [CrossRef]
- Fallon, K. Exercise in the time of COVID-19. Aust. J. Gen. Pr. 2020, 49, 49. [Google Scholar] [CrossRef]
- Luzi, L.; Radaelli, M.G. Influenza and obesity: Its odd relationship and the lessons for COVID-19 pandemic. Acta Diabetol. 2020, 57, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Phillipou, A.; Meyer, D.; Neill, E.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Eating and exercise behaviors in eating disorders and the general population during the COVID -19 pandemic in Australia: Initial results from the COLLATE project. Int. J. Eat. Disord. 2020, 53, 1158–1165. [Google Scholar] [CrossRef]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pr. 2020, 14, 210–216. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 1–15. [Google Scholar] [CrossRef]
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical Activity and Coronavirus Disease 2019 (COVID-19): Specific Recommendations for Home-Based Physical Training. Manag. Sport Leis. 2020, 1–6. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020. [Google Scholar] [CrossRef]
- Stanton, R.; To, G.Q.; Khalesi, S.; Williams, S.L.; Alley, S.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Chodkiewicz, J.; Talarowska, M.; Miniszewska, J.; Nawrocka, N.; Biliński, P. Alcohol Consumption Reported during the COVID-19 Pandemic: The Initial Stage. Int. J. Environ. Res. Public Health 2020, 17, 4677. [Google Scholar] [CrossRef]
- Jurak, G.; Morrison, S.A.; Leskošek, B.; Kovač, M.; Hadžić, V.; Vodičar, J.; Truden, P.; Starc, G. Physical activity recommendations during the coronavirus disease-2019 virus outbreak. J. Sport Health. Sci. 2020. [Google Scholar] [CrossRef]
- Niedermeier, M.; Frühauf, A.; Kopp-Wilfling, P.; Rumpold, G.; Kopp, M. Alcohol Consumption and Physical Activity in Austrian College Students—A Cross-Sectional Study. Subst. Use Misuse 2018, 53, 1581–1590. [Google Scholar] [CrossRef]
- Buscemi, J.; Martens, M.P.; Murphy, J.G.; Yurasek, A.M.; Smith, A.E. Moderators of the Relationship Between Physical Activity and Alcohol Consumption in College Students. J. Am. Coll. Health 2011, 59, 503–509. [Google Scholar] [CrossRef]
- Graupensperger, S.; Wilson, O.W.A.; Bopp, M.; Evans, M.B. Longitudinal association between alcohol use and physical activity in US college students: Evidence for directionality. J. Am. Coll. Health 2018, 68, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Smothers, B.; Bertolucci, D. Alcohol consumption and health-promoting behavior in a U.S. household sample: Leisure-time physical activity. J. Stud. Alcohol 2001, 62, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.K.; Barry, E.A. Examining Physical Activity Levels and Alcohol Consumption: Are People Who Drink More Active? Am. J. Health Promot. 2012, 26, e95–e104. [Google Scholar] [CrossRef]
- Probst, C.; Kilian, C.; Sanchez, S.; Lange, S.; Rehm, J. The role of alcohol use and drinking patterns in socioeconomic inequalities in mortality: A systematic review. Lancet Public Health 2020, 5, e324–e332. [Google Scholar] [CrossRef]
- Ricci, C.; Schutte, A.E.; Schutte, R.; Smuts, C.M.; Pieters, M. Trends in alcohol consumption in relation to cause-specific and all-cause mortality in the United States: A report from the NHANES linked to the US mortality registry. Am. J. Clin. Nutr. 2020, 111, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Sobal, J.; Rauschenbach, B.A.; Frongillo, E. Marital status changes and body weight changes: A US longitudinal analysis. Soc. Sci. Med. 2003, 56, 1543–1555. [Google Scholar] [CrossRef]
- Umberson, D.; Liu, H.; Powers, D. Marital status, marital transitions, and body weight. J. Health Soc. Behav. 2009, 50, 327–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Total n = 700 | Male n = 172 (24.6%) | Female n = 528 (75.4%) | p-Value |
|---|---|---|---|---|
| Age (years) a | 31 (18–62) | 28 (18–61) | 31 (19–62) | <0.001 |
| Members per household (n) a | 3 (0.5–5.5) | 2.5 (0–5) | 3 (1–6) | 0.179 |
| Education level n (%) b | 0.189 | |||
| Primary | 5 (0.71) | 0 | 5 (0.95) | |
| Secondary | 92 (13.14) | 26 (15.12) | 66 (12.5) | |
| University | 427 (61) | 106 (61.63) | 321 (60.8) | |
| Technical education | 85 (12.14) | 14 (8.14) | 71 (13.45) | |
| Postgraduate | 91 (13) | 26 (15.12) | 65 (12.31) | |
| Marital status n (%) b | 0.016 | |||
| Single | 396 (56.57) | 116 (67.44) | 280 (53.03) | |
| Married | 185 (26.43) | 35 (20.35) | 150 (28.41) | |
| Common law married | 73 (10.43) | 14 (8.14) | 59 (11.17) | |
| Separated | 40 (5.71) | 7 (4.07) | 33 (6.25) | |
| Widowed | 6 (0.86) | 0 | 6 (1.14) | |
| Socioeconomic level b | 0.041 | |||
| Low | 47 (6.71) | 10 (5.81) | 37 (7.01) | |
| Middle–low | 147 (21.00) | 30 (17.44) | 117 (22.16) | |
| Middle | 388 (55.43) | 93 (54.07) | 295 (55.87) | |
| Middle–high | 99 (14.14) | 36 (20.93) | 63 (11.93) | |
| High | 19 (2.71) | 3 (1.74) | 16 (3.03) |
| Variable | Total n = 700 | Male n = 172 (24.6%) | Female n = 528 (75.4%) | p-Value |
|---|---|---|---|---|
| Anthropometric parameters | ||||
| Size (m) a | 1.63 (1.5–1.8) | 1.75 (1.6–1.82) | 1.6 (1.5–1.72) | <0.001 |
| Body weight (kg) a | 68 (52–96) | 76.5 (60–105) | 66 (51–92) | <0.001 |
| BMI (kg/m2) a | 25.3 (20.2–34.95) | 25.85 (20.4–31.6) | 25.1 (20.2–34.95) | 0.720 |
| BMI category n (%) b | 0.029 | |||
| Normal weight | 334 (47.71) | 76 (44.19) | 258 (48.86) | |
| Overweight | 251 (35.86) | 75 (43.6) | 176 (33.3) | |
| Obesity | 115 (16.43) | 21 (12.2) | 94 (17.8) | |
| Physical activity patterns | ||||
| Physical activity (times/week) a | 2 (0–7) | 3 (0–7) | 2 (0–7) | <0.001 |
| Physical activity (min/session) a | 30 (0–90) | 45 (0–120) | 30 (0–90) | <0.001 |
| Types of physical activity (%) b | <0.001 | |||
| None | 198 (28.3) | 30 (17.44) | 168 (31.82) | |
| Combined/mixed | 136 (19.43) | 37 (21.51) | 99 (18.75) | |
| Yoga/Pilates | 77 (11) | 12 (6.98) | 65 (12.31) | |
| Aerobic/jogging | 118 (16.86) | 25 (14.53) | 93 (17.61) | |
| Calisthenics | 118 (16.86) | 43 (25) | 75 (14.2) | |
| Resistance training | 53 (7.57) | 25 (14.53) | 28 (5.3) | |
| Review social network n (%Yes) b | 407 (58.14) | 91 (52.9) | 316 (59.85) | 0.101 |
| Active breaks n (%Yes) b | 285 (40.71) | 86 (50.0) | 199 (37.69) | 0.004 |
| Sedentary lifestyle n (Yes%) b | 407 (58.14) | 91 (52.9) | 316 (59.85) | 0.100 |
| Sedentary lifestyle (hours/day) | 0.039 | |||
| <2 | 85 (12.1) | 17 (9.9) | 68 (12.9) | |
| 3–5 | 234 (33.4) | 71 (41.3) | 163 (30.9) | |
| ≥6 | 381 (54.4) | 84 (48.8) | 297 (56.2) |
| Variable | Total n = 700 | Male n = 172 (24.6%) | Female n = 528 (75.4%) | p-Value |
|---|---|---|---|---|
| Positive Nutritional parameters | ||||
| Glasses of water drunk per day a | 3 (1–7) | 4 (1–7) | 3 (0–7) | 0.016 |
| Vitamin supplementation (yes %) b | 186 (26.6) | 36 (20.9) | 150 (28.4) | 0.054 |
| Glasses of water per day b | 0.041 | |||
| 0–2 | 138 (19.7) | 41 (23.8) | 97 (18.4) | |
| 3–5 | 317 (45.3) | 84 (48.9) | 233 (44.1) | |
| 6–7 | 245 (35) | 47 (27.3) | 198 (37.5) | |
| Vegetables per day (portions) b | 0.671 | |||
| None | 117 (16.7) | 32 (18.6) | 85 (16.1) | |
| 1–2 | 484 (69.1) | 118 (68.6) | 366 (69.3) | |
| ≥3 | 99 (14.1) | 22 (12.8) | 77 (14.6) | |
| Legumes, times per week b | 0.060 | |||
| None | 68 (9.7) | 12 (7) | 56 (10.6) | |
| 1–2 | 586 (83.7) | 143 (83.1) | 443 (83.9) | |
| ≥3 | 46 (6.7) | 17 (9.9) | 29 (5.5) | |
| Fruits per day (portion) b | 0.491 | |||
| None | 48 (6.9) | 15 (8.7) | 33 (6.3) | |
| 1–3 | 373 (53.3) | 92 (53.5) | 281 (53.2) | |
| ≥4 | 279 (39.9) | 65 (37.8) | 214 (40.5) | |
| Change consumption vegetables and fruits b | 0.301 | |||
| Less than before | 145 (20.7) | 33 (19.2) | 112 (21.2) | |
| Same than before | 339 (48.4) | 92 (53.5) | 247 (46.8) | |
| More than before | 216 (30.9) | 47 (7.3) | 169 (32) | |
| Red meat, time per week | 0.018 | |||
| None | 122 (17.4) | 20 (11.6) | 102 (19.3) | |
| 1–2 | 388 (55.5) | 94 (54.7) | 294 (55.7) | |
| ≥3 | 190 (27.1) | 58 (33.7) | 132 (25) | |
| White meat, times per week b | 0.191 | |||
| None | 85 (12.1) | 15 (8.7) | 70 (13.3) | |
| 1–2 | 455 (65.1) | 112 (65.1) | 343 (64.9) | |
| ≥3 | 160 (22.9) | 45 (26.2) | 115 (21.8) | |
| Fish, times per week b | 0.590 | |||
| None | 150 (21.4) | 36 (20.9) | 114 (21.6) | |
| 1 to 2 | 526 (75.1) | 128 (74.4) | 398 (75.4) | |
| ≥3 | 24 (3.5) | 8 (4.6) | 16 (3.0) | |
| Dairy products, times per day b | 0.019 | |||
| None | 76 (10.9) | 18 (10.5) | 58 (11) | |
| 1–2 | 530 (75.7) | 120 (69.8) | 410 (77.7) | |
| ≥3 | 94 (13.4) | 34 (19.8) | 60 (11.4) | |
| Cook at home b | 0.004 | |||
| Less than before | 40 (5.7) | 12 (7) | 28 (5.3) | |
| Same than before | 243 (34.7) | 76 (44.2) | 167 (31.6) | |
| More than before | 417 (59.6) | 84 (48.8) | 333 (67.1) | |
| Feeding style perception | 0.161 | |||
| Less healthy than before | 187 (26.7) | 48 (27.9) | 139 (26.3) | |
| Same than before | 277 (39.6) | 76 (44.19) | 201 (38.1) | |
| Healthier than before | 236 (33.7) | 48 (27.9) | 188 (35.6) | |
| Among of consumption food, perception | 0.189 | |||
| Less than before | 104 (14.9) | 32 (18.6) | 72 (13.7) | |
| Same than before | 237 (33.8) | 60 (34.9) | 177 (33.5) | |
| More than before | 359 (51.3) | 80 (46.5) | 279 (52.8) | |
| Negative Nutritional parameters | ||||
| Alcohol b | 0.159 | |||
| None | 428 (61.1) | 95 (55.2) | 333 (63.1) | |
| 1–3 times/day | 210 (30) | 61 (35.5) | 149 (28.2) | |
| 1–2 times/week | 62 (8.9) | 16 (9.3) | 46 (8.7) | |
| Sausages, times per week b | <0.001 | |||
| None | 285 (40.7) | 44 (25.6) | 241 (45.6) | |
| 1–2 | 359 (51.3) | 107 (62.2) | 252 (47.7) | |
| ≥3 | 56 (8) | 21 (12.2) | 35 (6.6) | |
| Junk food, times per week b | 0.038 | |||
| None | 175 (25) | 50 (29) | 125 (23.7) | |
| 1–2 | 440 (62.9) | 110 (64) | 330 (62.5) | |
| ≥3 times per week | 85 (12.1) | 12 (7) | 73 (13.8) | |
| Fried food, times per week b | 0.149 | |||
| None | 223 (31.9) | 47 (27.3) | 176 (33.3) | |
| 1–2 | 419 (59.9) | 106 (61.6) | 313 (59.3) | |
| ≥3 | 58 (8.3) | 19 (11.1) | 39 (7.4) |
| Variable | OR (95% CI) p-Value |
|---|---|
| Sociodemographic parameters | |
| Separated marital status | 3.33 (1.53–7.24), 0.002 |
| Married | 1.52 (1.03–2.2), 0.030 |
| Middle socioeconomic level | 1.48 (1.04–2.1), 0.027 |
| Nutritional parameters | |
| Eating more food | 4.12 (2.9–5.9), <0.001 |
| Eating less food | 4.12 (2.52–6.72), <0.001 |
| Cook less than before | 4.06 (1.9–8.7), <0.001 |
| Eating fried foods ≥ 3 times a week | 3.36 (1.77–6.4), <0.001 |
| Perception of having a healthier diet | 2.46 (1.72–3.54), <0.001 |
| Low consumption of legumes ≤ 1 time per week | 2.27 (1.05–4.92), 0.030 |
| Sausage consumption ≥ 3 times per week | 2.16 (1.18–3.97), 0.010 |
| Junk food consumption ≥ 3 times per week | 1.76 (1.02–3.0), 0.040 |
| Low water consumption ≤ 2 glasses per day | 1.58 (1.03–2.41), 0.030 |
| Cook more than before | 1.50 (1.1–2.1), 0.010 |
| Fish consumption 1–2 times per week | 0.67 (0.46–0.97), 0.030 |
| Physical activity parameters | |
| Active breaks | 0.72 (0.53–0.99), 0.040 |
| Mixed physical activity | 0.63 (0.40–0.99), 0.048 |
| Exercise session duration 30–60 min | 0.61 (0.42–0.90), 0.011 |
| Yoga and Pilates | 0.53 (0.31–0.90), 0.021 |
| Exercise session duration > 60 min | 0.52 (0.31–0.88), 0.010 |
| Physical activity ≥ 4 times/week | 0.51 (0.34–0.75), 0.001 |
| Sedentary behavior ≥ 6 h/day | 1.85 (1.13–3.03), 0.010 |
| Variable | OR (CI 95%) p-Value |
|---|---|
| Anthropometric parameters | |
| Perception of weight increase | 2.01 (1.35–3.25), 0.001 |
| Being Overweight | 1.80 (1.17–2.76), 0.007 |
| Nutritional parameters | |
| Daily alcohol consumption | 4.77 (1.68–13.5), 0.003 |
| Decrease vegetable consumption | 3.32 (1.85–5.98), <0.001 |
| Perception of having a healthier diet | 2.11 (1.36–3.29), 0.001 |
| Eating more food than before | 1.87 (1.26–2.78), 0.002 |
| Physical parameters | |
| Sedentary ≥ 6 h | 2.12 (1.23–3.63), 0.006 |
| Exercise session duration ≤ 30 min | 1.99 (1.18–3.37), 0.01 |
| Yoga and Pilates | 1.82 (1.02–3.24), 0.04 |
| Physical activity 1–3 times per week | 1.67 (1.07–2.6), 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes-Olavarría, D.; Latorre-Román, P.Á.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population. Int. J. Environ. Res. Public Health 2020, 17, 5431. https://doi.org/10.3390/ijerph17155431
Reyes-Olavarría D, Latorre-Román PÁ, Guzmán-Guzmán IP, Jerez-Mayorga D, Caamaño-Navarrete F, Delgado-Floody P. Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population. International Journal of Environmental Research and Public Health. 2020; 17(15):5431. https://doi.org/10.3390/ijerph17155431
Chicago/Turabian StyleReyes-Olavarría, Daniela, Pedro Ángel Latorre-Román, Iris Paola Guzmán-Guzmán, Daniel Jerez-Mayorga, Felipe Caamaño-Navarrete, and Pedro Delgado-Floody. 2020. "Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population" International Journal of Environmental Research and Public Health 17, no. 15: 5431. https://doi.org/10.3390/ijerph17155431