Getting Old Well in Sub Saharan Africa: Exploring the Social and Structural Drivers of Subjective Wellbeing among Elderly Men and Women in Uganda

Abstract
:1. Background
2. Aging and Subjective Wellbeing
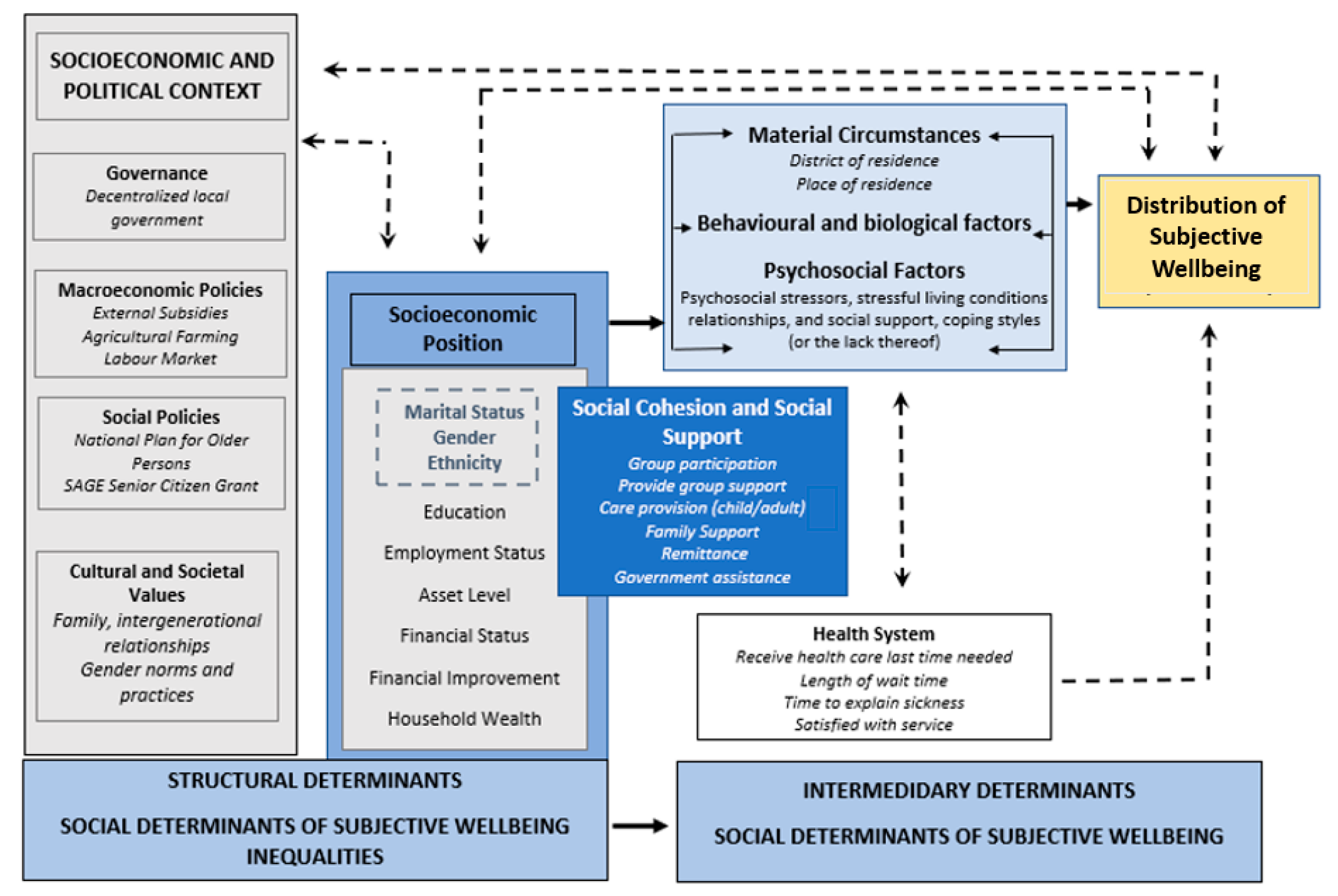
3. Framing Aging and SWB in SSA
4. Aging in Uganda
5. Research Design and Methods
6. Results
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; p. 246. [Google Scholar]
- Jivraj, S.; Nazroo, J.; Vanhoutte, B.; Chandola, T. Aging and subjective well-being in later life. J. Gerontol Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Rymkiewicz, P.D.; Heng, Y.X.; Vasudev, A.; Larbi, A. The immune system in the aging human. Immunol. Res. 2012, 53, 235–250. [Google Scholar] [CrossRef] [PubMed]
- Sargent-Cox, K.A.; Butterworth, P.; Anstey, K.J. Role of physical activity in the relationship between mastery and functional health. Gerontologist 2015, 55, 120–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadler, M.E.; Miller, C.J.; Christensen, K.; McGue, M. Subjective wellbeing and longevity: A co-twin control study. Twin Res. Hum. Genet. 2011, 14, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Blanchflower, D.G.; Oswald, A.J. Is well-being U-shaped over the life cycle? Soc. Sci. Med. 2008, 66, 1733–1749. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M.; Sörensen, S. Influences of socioeconomic status, social network, and competence on subjective well-being in later life: A meta-analysis. Psychol. Aging 2000, 15, 187–224. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. In The Lancet; Lancet Publishing Group: Amsterdam, The Netherlands, 2015; Volume 385, pp. 640–648. [Google Scholar]
- Carstensen, L.L.; Fung, H.H.; Charles, S.T. P1: IZO Motivation and Emotion [me] pp911-moem-468764 Socioemotional Selectivity Theory and the Regulation of Emotion in the Second Half of Life 1. Motiv. Emot. 2003, 27, 103–123. [Google Scholar] [CrossRef]
- Graham, C.; Ruiz Pozuelo, J. Happiness, stress, and age: How the U curve varies across people and places. J. Popul. Econ. 2017, 30, 225–264. [Google Scholar] [CrossRef]
- Deaton, A.S.; Tortora, R. People in Sub-Saharan Africa Rate Their Health and Health Care Among the Lowest in The World. Health Aff. 2015, 34, 519–527. [Google Scholar] [CrossRef] [Green Version]
- United Nations, Department of Economic and Social Affairs PD. United Nations, Department of Economic and Social Affairs PD. United nations department of economic and social affairs, population division. In World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Read, S.; Grundy, E.; Foverskov, E. Socio-economic position and subjective health and well-being among older people in Europe: A systematic narrative review. In Aging and Mental Health; Routledge: London, UK, 2016; Volume 20, pp. 529–542. [Google Scholar]
- Pinquart, M.; Sörensen, S. Gender Differences in Self-Concept and Psychological Well-Being in Old Age: A Meta-Analysis. J. Gerontol. Ser. B Psychol. Sci. Copyr. 2001, 56, P195–P213. [Google Scholar] [CrossRef]
- Diener, E.; Lucas, R.E.; Oishi, S. Subjective well-being: The science of happiness and life satisfaction. In Handbook of Positive Psychology, 2nd ed.; Amazon: North Seattle, WA, USA, 2002; pp. 63–73. [Google Scholar]
- Uganda Bureau of Statistics the Republic of Uganda 2015 Statistical Abstract Website. 2015. Available online: www.ubos.org (accessed on 3 January 2020).
- Mugisha, J.; Scholten, F.; Owilla, S.; Naidoo, N.; Seeley, J.; Chatterji, S.; Boerma, T. Caregiving responsibilities and burden among older people by HIV status and other determinants in Uganda. AIDS Care 2013, 25, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Nzabona, A.; Ntozi, J.; Rutaremwa, G. Loneliness among older persons in Uganda: Examining social, economic and demographic risk factors. Ageing Soc. 2016, 36, 860–888. [Google Scholar] [CrossRef]
- Maniragaba, F.; Nzabona, A.; Asiimwe, J.B.; Bizimungu, E.; Mushomi, J.; Ntozi, J.; Kwagala, B. Factors associated with older persons’ physical health in rural Uganda. PLoS ONE 2019, 14. [Google Scholar] [CrossRef] [PubMed]
- Golaz, V.; Wandera, S.O.; Rutaremwa, G. Understanding the vulnerability of older adults: Extent of and breaches in support systems in Uganda. Ageing Soc. 2017, 37, 63–89. [Google Scholar] [CrossRef]
- Wandera, S.O.; Golaz, V.; Kwagala, B.; Ntozi, J. Factors associated with self-reported ill health among older Ugandans: A cross sectional study. Arch. Gerontol. Geriatr. 2015, 61, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Kinyanda, E.; Kuteesa, M.; Scholten, F.; Mugisha, J.; Baisley, K.; Seeley, J. Risk of major depressive disorder among older persons living in HIV-endemic central and southwestern Uganda. AIDS Care 2016, 28, 1516–1521. [Google Scholar] [CrossRef]
- Kahneman, D.; Krueger, A.B.; Schkade, D.A.; Schwarz, N.; Stone, A.A. A survey method for characterizing daily life experience: The day reconstruction method. Science 2004, 306, 1776–1780. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B.H.; Love, G.D. Positive health: Connecting well-being with biology. In Philosophical Transactions of the Royal Society B: Biological Sciences; Royal Society: London, UK, 2004; pp. 1383–1394. [Google Scholar]
- Lau, D.T.; Machizawa, S.; Doi, M. Informal and Formal Support among Community-Dwelling Japanese American Elders Living Alone in Chicagoland: An In-Depth Qualitative Study. J. Cross Cult. Gerontol. 2012, 27, 149–161. [Google Scholar] [CrossRef]
- Taniguchi, H.; Potter, D.A. Who are your Neighbors? Neighbor Relationships and Subjective Well-Being in Japan. Appl. Res. Qual. Life 2016, 11, 1425–1443. [Google Scholar] [CrossRef]
- Caron, J. Predictors of Quality of Life in Economically Disadvantaged Populations in Montreal. Soc. Indic. Res. 2012, 107, 411–427. [Google Scholar] [CrossRef]
- Kloos, B.; Townley, G. Investigating the relationship between neighborhood experiences and psychiatric distress for individuals with serious mental illness. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 105–116. [Google Scholar] [CrossRef] [Green Version]
- Kim, J. Neighborhood disadvantage and mental health: The role of neighborhood disorder and social relationships. Soc. Sci. Res. 2010, 39, 260–271. [Google Scholar] [CrossRef]
- Diener, E.D.; Gohm, C.L.; Suh, E.; Oishi, S. Similarity of the relations between marital status and subjective well-being across cultures. J. Cross Cult. Psychol. 2000, 31, 419–436. [Google Scholar] [CrossRef]
- Mroczek, D.K.; Spiro, A. Change in life satisfaction during adulthood: Findings from the veterans affairs normative aging study. J. Pers. Soc. Psychol. 2005, 88, 189–202. [Google Scholar] [CrossRef] [Green Version]
- Chipperfield, J.G.; Havens, B. Gender Differences in the Relationship Between Marital Status Transitions and Life Satisfaction in Later Life. J. Gerontol. Psychol. Sci. 2001, 56, P176–P186. [Google Scholar] [CrossRef] [Green Version]
- Lucas, R.E.; Clark, A.E.; Georgellis, Y.; Diener, E. Reexamining Adaptation and the Set Point Model of Happiness: Reactions to Changes in Marital Status. J. Personal. Soc. Psychol. 2003, 84, 527. [Google Scholar] [CrossRef]
- Amato, P.R. Research on divorce: Continuing trends and new developments. J. Marriage Fam. 2010, 72, 650–666. [Google Scholar] [CrossRef]
- Bowen, G.L.; Jensen, T.M. Late-Life Divorce and Postdivorce Adult Subjective Well-Being. J. Fam. Issues 2017, 38, 1363–1388. [Google Scholar] [CrossRef]
- Uganda Bureau of Statistics (UBS); ICF. Uganda Demographic and Health Survey 2016; UBOS: Kampala, Uganda; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Jivraj, S.; Nazroo, J. Determinants of socioeconomic inequalities in subjective well-being in later life: A cross-country comparison in England and the USA. Qual. Life Res. 2014, 23, 2545–2558. [Google Scholar] [CrossRef]
- Cheung, C.K.; Ngan, R.M.H. Filtered Life Satisfaction and Its Socioeconomic Determinants in Hong Kong. Soc. Indic. Res. 2012, 109, 223–242. [Google Scholar] [CrossRef]
- Netuveli, G.; Wiggins, R.D.; Hildon, Z.; Montgomery, S.M.; Blane, D. Quality of life at older ages: Evidence from the English longitudinal study of aging (wave 1). J. Epidemiol. Community Health 2006, 60, 357–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y. Social inequalities in happiness in the United States, 1972 to 2004: An age-period-cohort analysis. Am. Sociol. Rev. 2008, 73, 204–226. [Google Scholar] [CrossRef] [Green Version]
- Graham, C.; Chattopadhyay, S. Gender and well-being around the world. Int. J. Happiness Dev. 2013, 1, 212–232. [Google Scholar] [CrossRef] [Green Version]
- Meggiolaro, S.; Ongaro, F. Life satisfaction among older people in Italy in a gender approach. Ageing Soc. 2015, 35, 1481–1504. [Google Scholar] [CrossRef]
- Stone, A.A.; Schwartz, J.E.; Broderick, J.E.; Deaton, A. A snapshot of the age distribution of psychological well-being in the United States. Proc. Natl. Acad. Sci. USA 2010, 107, 9985–9990. [Google Scholar] [CrossRef] [Green Version]
- Dahlberg, L.; McKee, K.J. Social exclusion and well-being among older adults in rural and urban areas. Arch. Gerontol. Geriatr. 2018, 79, 176–184. [Google Scholar] [CrossRef]
- Tobiasz-Adamczyk, B.; Zawisza, K. Urban-rural differences in social capital in relation to self-rated health and subjective well-being in older residents of six regions in Poland. Ann. Agric. Environ. Med. 2017, 24, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Alcañiz, M.; Riera-Prunera, M.-C.; Sole-Auró, A. Do Elderly People Living in Rural Areas Enjoy Better Mental Well-Being? Evidence from Catalonia, Spain. Available online: www.ub.edu/irea/ (accessed on 10 December 2019).
- Elliott, S.J.; Dixon, J.; Bisung, E.; Kangmennaang, J. A Glowing footprint: Developing an index of wellbeing for low to middle income countries. Int. J. Wellbeing 2017, 7. [Google Scholar] [CrossRef]
- Adebowale, S.A.; Atte, O.; Ayeni, O. Elderly Well-being in a Rural Community in North Central Nigeria, sub-Saharan Africa. Public Health Res. 2012, 2, 92–101. [Google Scholar]
- Gureje, O.; Kola, L.; Afolabi, E.; Olley, B.O. Determinants of quality of life of elderly Nigerians: Results from the Ibadan Study of Ageing. Afr. J. Med. Med Sci. 2008, 37, 239. [Google Scholar]
- Ralston, M. The Role of Older Persons’ Environment in Aging Well: Quality of Life, Illness, and Community Context in South Africa. Gerontologist 2018, 58, 111–120. [Google Scholar] [CrossRef]
- Calys-Tagoe, B.N.L.; Hewlett, S.A.; Dako-Gyeke, P.; Yawson, A.E.; Baddoo, N.A.; Seneadza, N.A.H.; Kowal, P. Predictors of subjective well-being among older Ghanaians. Ghana Med. J. 2014, 48, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Sadana, R.; Blas, E.; Budhwani, S.; Koller, T.; Paraje, G. Healthy Ageing: Raising awareness of inequalities, determinants, and what could be done to improve health equity. Gerontologist 2016, 56, S178–S193. [Google Scholar] [CrossRef] [Green Version]
- National Policy for Older Persons The Republic of Uganda National Policy for Older Persons Ageing with Security and Dignity Ministry of Gender Labour and Social Development, P.O Box 7136 Kampala Uganda. 2009. Available online: http://www.mglsd.go.ug (accessed on 10 January 2020).
- Rentfrow, P.J. Geographical variation in subjective well-being. In Handbook of Well-Being; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- World Health Organization. A Conceptual Framework for Action on the Social Determinants of Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs Sustainable Development Goals; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Social Determinants of Health; Marmot, M., Wilkinson, R., Eds.; OUP Oxford: Oxford, UK, 2005. [Google Scholar]
- World Health Organization. Social Determinants of Health: The Solid Facts; Wilkinson, R.G., Marmot, M., Eds.; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Moore, S.; Haines, V.; Hawe, P.; Shiell, A. Lost in translation: A genealogy of the “social capital” concept in public health. J. Epidemiol. Community Health 2006, 60, 729–734. [Google Scholar] [CrossRef] [Green Version]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Åslund, C.; Larm, P.; Starrin, B.; Nilsson, K.W. The buffering effect of tangible social support on financial stress: Influence on psychological well-being and psychosomatic symptoms in a large sample of the adult general population. Int. J. Equity Health 2014, 13, 85. [Google Scholar] [CrossRef] [Green Version]
- Robinette, J.W.; Charles, S.T.; Mogle, J.A.; Almeida, D.M. Neighborhood cohesion and daily well-being: Results from a diary study. Soc. Sci. Med. 2013, 96, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Seeley, J.; Dercon, S.; Barnett, T. The effects of HIV/AIDS on rural communities in East Africa: A 20-year perspective. Trop. Med. Int. Health 2010, 15, 329–335. [Google Scholar] [CrossRef]
- Hickey, S.; Bukenya, B. The politics of promoting social cash transfers in Uganda: The potential and pitfalls of ‘thinking and working politically’. Dev. Policy Rev. 2019. [Google Scholar] [CrossRef]
- Kowal, P.; Chatterji, S.; Naidoo, N.; Biritwum, R.; Fan, W.; Ridaura, R.L.; Snodgrass, J.J. Data resource profile: The world health organization study on global ageing and adult health (SAGE). Int. J. Epidemiol. 2012, 41, 1639–1649. [Google Scholar] [CrossRef]
- Kowal, P.; Kahn, K.; Ng, N.; Naidoo, N.; Abdullah, S.; Bawah, A.; Xavier Gómez-Olivé, F. Ageing and adult health status in eight lower-income countries: The INDEPTH WHO-SAGE collaboration. Glob. Health Action 2010, 3 (Suppl. 2), 11–22. [Google Scholar] [CrossRef]
- Africa Human Development Report 2016 Accelerating Gender Equality and Women’s Empowerment in Africa. 2016. Available online: http://hdr.undp.org/sites/default/files/afhdr_2016_lowres_en.pdf (accessed on 15 December 2019).
- Ng, N.; Kowal, P.; Kahn, K.; Naidoo, N.; Abdullah, S.; Bawah, A.; Xavier Gómez-Olivé, F. Health inequalities among older men and women in Africa and Asia: Evidence from eight Health and Demographic Surveillance System sites in the INDEPTH WHO-SAGE Study. Glob. Health Action 2010, 3, 5420. [Google Scholar] [CrossRef]
- Mugisha, J.O.; Schatz, E.J.; Randell, M.; Kuteesa, M.; Kowal, P.; Negin, J.; Seeley, J. Chronic disease, risk factors and disability in adults aged 50 and above living with and without HIV: Findings from the Wellbeing of Older People Study in Uganda. Glob. Health Action 2016, 9, 31098. [Google Scholar] [CrossRef]
- Phaswana-Mafuya, N.; Peltzer, K.; Chirinda, W.; Kose, Z.; Hoosain, E.; Ramlagan, S.; Davids, A. Self-rated health and associated factors among older South Africans: Evidence from the study on global ageing and adult health. Glob. Health Action 2013, 6, 19880. [Google Scholar] [CrossRef]
- Van Biljon, L.; Nel, P.; Roos, V. A partial validation of the WHOQOL-OLD in a sample of older people in South Africa. Glob. Health Action 2015, 8, 28209. [Google Scholar] [CrossRef]
- Chachamovich, E.; Trentini, C.; Fleck, M.P. Assessment of the psychometric performance of the WHOQOL-BREF instrument in a sample of Brazilian older adults. Int. Psychogeriatr. 2007, 19, 635–646. [Google Scholar] [CrossRef]
- Guttman, L. An Outline of Some New Methodology for Social Research*. 1954. Available online: https://academic.oup.com/poq/article-abstract/18/4/395/1925139 (accessed on 5 January 2020).
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis 1. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Bentler, P.M.; Weeks, D.G. Linear structural equations with latent variables. Psychometrika 1980, 45, 289–308. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Assessing Mediation in Communication Research; The Sage Sourcebook of Advanced Data Analysis Methods for Communication Research; Sage: London, UK, 2008. [Google Scholar]
- Perkins, J.M.; Subramanian, S.V.; Christakis, N.A. Social networks and health: A systematic review of sociocentric network studies in low- and middle-income countries. Soc. Sci. Med. 2015, 125, 60–78. [Google Scholar] [CrossRef] [Green Version]
- Thoits, P.A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [Green Version]
- Narayan, D. Bonds and bridges: Social capital and poverty. In Social Capital and Economic Development: Well-Being in Developing Countries; Edward Elgar: Northampton, MA, USA, 2002; pp. 58–81. [Google Scholar]
- Knodel, J.; Watkins, S.; Van Landingham, M. AIDS and Older Persons: An International Perspective. JAIDS Hagerstown MD 2003, 33, S153–S165. [Google Scholar] [CrossRef] [Green Version]
- Ice, G.H.; Yogo, J.; Heh, V.; Juma, E. The impact of caregiving on the health and well-being of Kenyan Luo grandparents. Res. Aging 2010, 32, 40–66. [Google Scholar] [CrossRef]
- Akintola, O. A Gendered Analysis of the Burden of Care on Family and Volunteer Caregivers in Uganda and South Africa; University of KwaZulu-Natal, United States Agency for International Development (USAID): Durban, South Africa, 2004; p. 47. [Google Scholar]
- Kasedde, S.; Doyle, A.M.; Seeley, J.A.; Ross, D.A. They are not always a burden: Older people and child fostering in Uganda during the HIV epidemic. Soc. Sci. Med. 2014, 113, 161–168. [Google Scholar] [CrossRef] [Green Version]
- Carmel, S. Health and well-being in late life: Gender differences worldwide. Front. Med. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Mudege, N.N.; Ezeh, A.C. Gender, aging, poverty and health: Survival strategies of older men and women in Nairobi slums. J. Aging Stud. 2009, 23, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Harling, G.; Payne, C.F.; Davies, J.I.; Gomez-Olive, F.X.; Kahn, K.; Manderson, L.; Witham, M.D. Impairment in Activities of Daily Living, Care Receipt, and Unmet Needs in a Middle-Aged and Older Rural South African Population: Findings from the HAALSI Study. J. Aging Health 2019. [Google Scholar] [CrossRef]
- Luy, M.; Minagawa, Y. Gender gaps-Life expectancy and proportion of life in poor health. Health Rep. 2014, 25, 12. [Google Scholar]
- Oksuzyan, A.; Petersen, I.; Stovring, H.; Bingley, P.; Vaupel, J.W.; Christensen, K. The Male-Female Health-Survival Paradox: A Survey and Register Study of the Impact of Sex-Specific Selection and Information Bias. Ann. Epidemiol. 2009, 19, 504–511. [Google Scholar] [CrossRef] [Green Version]
- Nyanzi, S. Ambivalence surrounding elderly widows’ sexuality in urban Uganda. Ageing Int. 2011, 36, 378–400. [Google Scholar] [CrossRef]
- Nyirenda, M.; Chatterji, S.; Falkingham, J.; Mutevedzi, P.; Hosegood, V.; Evandrou, M.; Newell, M.L. An investigation of factors associated with the health and well-being of HIV-infected or HIV-affected older people in rural South Africa. BMC Public Health 2012, 12, 259. [Google Scholar] [CrossRef] [Green Version]
- Galdas Bsc, P.M.; Certed, R.N.; Ma, F.C.; Marshall, P.; Galdas, P. Integrative literature reviews and meta-analyses. Men and health help-seeking behaviour: Literature review. J. Adv. Nurs. 2005, 49, 616–623. [Google Scholar] [CrossRef]
- Fantahun, M.; Berhane, Y.; Högberg, U.; Wall, S.; Byass, P. Ageing of a rural Ethiopian population: Who are the survivors? Public Health 2009, 123, 326–330. [Google Scholar] [CrossRef]
- Cesari, M.; De Carvalho, I.A.; Thiyagarajan, J.A.; Cooper, C.; Martin, F.C.; Reginster, J.Y.; Beard, J.R. Evidence for the domains supporting the construct of intrinsic capacity. J. Gerontol. Ser. A 2018, 73, 1653–1660. [Google Scholar] [CrossRef] [Green Version]
- Deaton, A. The Great Escape: Health, Wealth, and the Origins of Inequality; Princeton University Press: Princeton, NJ, USA, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Codes | Men | Women |
|---|---|---|---|
| Frequency/Mean (%) | Frequency/Mean (%) | ||
| Age (Years) | 65.00 (SD = 10.30, range = 50–90) | 64.21(SD = 10.35, range = 50–101) | |
| Subjective Wellbeing | 7 (SD = 2.81, Range = 0–13.25) | 6 (SD = 2.75, Range = 0–12.40) | |
| Care Responsibilities | |||
| Care Responsibilities for Children | 103 (58%) 2.7 (SD = 2.25, Range 0–11) | 216 (73%) 3.1 (SD = 2.15, range 0–10) | |
| Provide Care for Adult | |||
| No | 0 | 159 (90) | 256 (87) |
| Yes | 1 | 17 (10) | 38 (13) |
| Receive Family Assistance | |||
| No | 0 | 96 (55) | 106 (36) |
| Yes | 1 | 80 (45) | 188 (64) |
| Provide Community Support | |||
| No | 0 | 111 (63) | 192 (65) |
| Yes | 1 | 65 (37) | 102 (35) |
| Participate in Group | |||
| No | 0 | 106 (61) | 176 (60) |
| Yes | 1 | 68 (39) | 118 (40) |
| Government Assistance | |||
| No | 0 | 166 (94) | 270 (92) |
| Yes | 1 | 10 (6) | 24 (8) |
| Receive Remittance from Children | |||
| Yes | 0 | 32 (18) | 106 (36) |
| No | 1 | 144 (82) | 188 (64) |
| Number of People Close to (children and adults) | 12 (SD = 19.68, Range 0–100) | 8 (SD = 14.45, range 0–98) | |
| Health care variables | |||
| Receive Health Care Last Time Needed | |||
| No | 0 | 11 (6) | 27 (9) |
| Yes | 1 | 165 (94) | 267 (91) |
| Length of Waiting time | |||
| Not long | 0 | 106 (60) | 145 (49) |
| Long | 1 | 70 (40) | 149 (51) |
| Time to Explain Sickness (HC) | |||
| Always | 0 | 159 (90) | 244 (83) |
| Not Always | 1 | 17 (10) | 50 (17) |
| Satisfied with Services (HC) | |||
| Satisfied | 0 | 158 (93) | 241 (88) |
| Not Satisfied | 1 | 11 (7) | 33 (12) |
| Socio-economic variables | |||
| Asset Level | |||
| Poor | 0 | 43 (24) | 114 (39) |
| Middle | 1 | 63 (36) | 93 (32) |
| Rich | 2 | 70 (40) | 87 (30) |
| Financial Status | |||
| Bad | 0 | 109 (63) | 201 (68) |
| Good | 1 | 64 (37) | 93 (32) |
| Financial Improvement (last 3yrs) | |||
| Worse | 0 | 117 (66) | 192 (65) |
| Better/same | 1 | 59 (34) | 102 (35) |
| Currently Employed/Working | |||
| No | 0 | 30 (17) | 61 (21) |
| Yes | 1 | 146 (83) | 233 (79) |
| Educational Level | |||
| None | 0 | 18 (10) | 70 (24) |
| Primary | 1 | 99 (57) | 168 (57) |
| Secondary | 2 | 47 (27) | 38 (13) |
| Higher | 3 | 9 (5) | 18 (6) |
| Demographic factors | |||
| Marital Status | |||
| Not Married | 0 | 65 (37) | 258 (88) |
| Married | 1 | 111 (63) | 36 (12) |
| Residence/Location | |||
| Urban | 0 | 55 (31) | 113 (38) |
| Rural | 1 | 121 (69) | 181 (62) |
| Religion | |||
| Catholic | 0 | 105 (60) | 182 (62) |
| Protestant | 1 | 42 (24) | 62 (21) |
| Islam | 2 | 18 (10) | 21 (8) |
| Other | 3 | 10 (6) | 29 (10) |
| Total | 176 | 294 | |
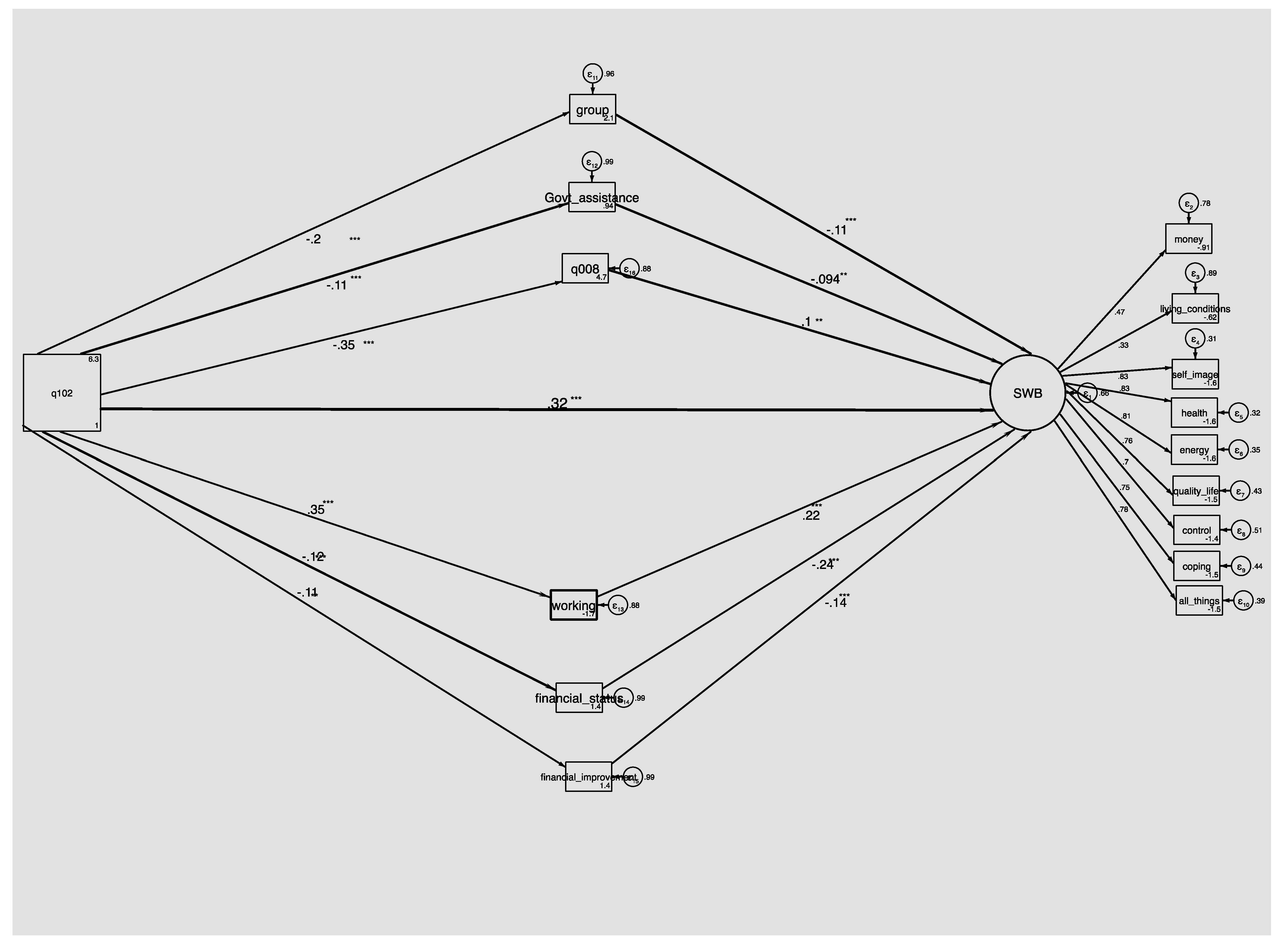
| Variables | Men only | Women only | Total sample |
|---|---|---|---|
| Age (Years) | 0.41[0.27–0.54] *** | 0.44[0.33–0.54] *** | 0.42[0.34–0.50] *** |
| Provide Community Support | −0.22[−0.39–−0.06] *** | −0.26[−0.39–−0.13] *** | −0.24[−0.34–−0.14] *** |
| Care Responsibilities for Children | |||
| Participate in Group | −0.16[−0.32–0.01] * | −0.28[−0.41–−0.16] *** | −0.23[−0.33–−0.13] *** |
| Number of People Close to | −0.13[−0.30–0.04] | −0.13[−0.27–−0.002] ** | −0.15[−0.26–−0.04] *** |
| Childcare Responsibilities | −0.12[−0.28–0.05] | −0.11[−0.24–0.03] | −0.08[−.018–0.02] |
| Provide Care to Adults | 0.05[−0.11–0.23] | −0.09[−0.23–0.04] | −0.03[−0.14–0.07] |
| Government Assistance | −0.04[−0.22–0.13] | −0.29[−0.42–−0.16] *** | −0.19[−0.29–−0.08] *** |
| Family Assistance | −0.14[−0.31–0.02] * | 0.02[−0.11–0.16] | 0.003[−0.10–0.11] |
| Receive Remittance from Children | −0.08[−0.26–0.08] | 0.01[−0.12–0.15] | 0.02[−0.08–0.13] |
| Receive Healthcare Last Time Needed | 0.10[−0.07–0.27] | −0.16[−0.29–−0.03] ** | −0.08[−0.19–0.02] |
| Length of Waiting Time | −0.05[−0.23–0.12] | 0.11[−0.03–0.24] | 0.06[−0.04–0.17] |
| Time to Explain Sickness (HC) | 0.04[−0.13–0.22] | 0.13[−0.01–0.26] * | 0.12[0.02–0.23] ** |
| Satisfied with Services (HC) | −0.09[−0.26–0.08] | 0.12[−0.01–0.25] * | 0.07[−0.03–0.18] |
| Education | −0.31[−0.48–−0.15] *** | −0.23[−0.36–−0.09] *** | −0.29[−0.39–−0.19] *** |
| Not Currently Working | 0.19[0.03–0.35] ** | 0.28[0.16–0.39] *** | 0.26[0.17–0.35] *** |
| Asset Level | −0.33[−0.49–−0.17] *** | −0.26[−0.39–−0.13] *** | −0.30[−0.40–−0.20] *** |
| Good Financial Status | −0.47[−0.61–−0.32] *** | −0.44[−0.56–−0.33] *** | −0.45[−0.54–−0.36] *** |
| Financial Improvement (last 3 y) | −0.40[−0.55–−0.25] *** | −0.46[−0.57–−0.34] *** | −0.42[−0.52–−0.33] *** |
| Gender (female) | N/A | N/A | 0.21[0.11–0.32] *** |
| Currently Married | −0.25[−0.42–−0.08] *** | −0.12[−0.25–0.02] * | −0.26[−0.36–−0.16] *** |
| Rural Residence/Location | −0.001[−0.17–0.17] | −0.04[−0.16–0.08] | −0.04[−0.14–0.06] |
| Religion | 0.09[−0.08–0.26] | 0.01[−0.13–0.14] | 0.05[−0.06–0.16] |
| RMSEA (Root mean squared error of approximation) | 0.097 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rishworth, A.; Elliott, S.J.; Kangmennaang, J. Getting Old Well in Sub Saharan Africa: Exploring the Social and Structural Drivers of Subjective Wellbeing among Elderly Men and Women in Uganda. Int. J. Environ. Res. Public Health 2020, 17, 2347. https://doi.org/10.3390/ijerph17072347
Rishworth A, Elliott SJ, Kangmennaang J. Getting Old Well in Sub Saharan Africa: Exploring the Social and Structural Drivers of Subjective Wellbeing among Elderly Men and Women in Uganda. International Journal of Environmental Research and Public Health. 2020; 17(7):2347. https://doi.org/10.3390/ijerph17072347
Chicago/Turabian StyleRishworth, Andrea, Susan J. Elliott, and Joseph Kangmennaang. 2020. "Getting Old Well in Sub Saharan Africa: Exploring the Social and Structural Drivers of Subjective Wellbeing among Elderly Men and Women in Uganda" International Journal of Environmental Research and Public Health 17, no. 7: 2347. https://doi.org/10.3390/ijerph17072347