1. Introduction
There are still quite a few economically underdeveloped regions in China, which include 5 provinces in northwest China, 4 provinces in the southwest, and 8 in the central region. The population of those regions accounts for 58.19% of China’s total population, of which the rural population accounts for 41.43% [
1]. There is a certain economical gap between these less developed regions and the eastern coastal areas, with low per capita income and poor infrastructure construction. Thus, the less developed region is the main focus in this phase. How to improve the health level of rural residents in less developed areas and achieve equalization of medical and health services have been a major concern [
2,
3,
4].
In rural areas of economically underdeveloped areas, the industrial structure is dominated by agriculture, labor productivity is low, per capita income is low, and a large number of people flow to cities and developed areas for employment. Young people leave rural areas for better employment opportunities. A larger percentage of middle-aged and elderly females live in rural areas. Due to their older age and lower education level, middle-aged and older females find it difficult to find jobs in cities and developed areas, and thus, most of them stay in rural areas. More and more middle-aged and elderly females (MAEF) appear to lack the care of their families and become a vulnerable group that needs attention. They are vulnerable due to several reasons, including their frail age and low economic income. Many elderly women are in poverty and living alone with the extension of life expectancy and gender mortality [
5]. The traditional joint family is gradually replaced by the nuclear family, which leads to the weakening of family relations. Women live longer than their male counterparts and may no longer have a built-in caregiver [
6].
The proportion of middle-aged and elderly, those aged 45 or older, is increasing in China, often with more chronic conditions than their predecessors. While the change in the age profile of the population will be accompanied by a decline in communicable diseases, an increasing number of middle-aged and elderly will raise the incidence of non-communicable diseases, placing new burdens on health care provision into the future [
7]. Thus, the demand for health care services has increased, especially middle-aged and elderly females (MAEF) in rural areas. Rural females are also having lower life expectancy, compared to urban females [
8,
9]. Previous research has demonstrated gender differences in health care utilization, with females using more both outpatient and inpatient utilization of health care services compared to males [
10].
The challenge of population health is gradually shifting away from traditional infectious diseases to non-communicable diseases related to an aging population, such as chronic non-communicable diseases. Most middle-aged and older women have lower levels of health, high proportion of chronic non-communicable diseases, long-duration illnesses, and high demand for inpatient services. Thus, high pressure on hospitalization expenses makes it very prone to poverty due to due to illness, which places tremendous pressure on the medical security of middle-aged and elderly women in rural China. In the United States, about three-quarters of total health care costs are related to the treatment of chronic diseases, and chronic diseases is an important factor that impacts the use of inpatient services [
11].
The economic income of MAEF in economically underdeveloped areas is generally lower than that of men, and their social status is also relatively low. Any catastrophic medical expenses will cause serious illness and poverty due to illness in the middle-aged and elderly women, which will inevitably affect their use of inpatient services and limit their needs for inpatient service [
12]. In 2003, the new rural cooperative medical system (NCMS) was launched by the Chinese central government in order to provide health insurance for China’s rural population. The NCMS is characterized by voluntary enrollment, individual and governmental co-financing, and pooled resources at the county level [
13]. NCMS policy was also found to increase the utilization of health care services [
14].
One important factor in this choice of focus is that middle-aged and elderly females is the key group whose utilization of inpatient services needs more attention as their health decays with age. The middle-aged and elderly female demographic faces a great disease burden. Maintaining this age-based separation in this study is thus a logical step to take.
This paper examines the utilization of inpatient services and its influencing factors for middle-aged and elderly rural females in underdeveloped regions. This study analyzes whether the utilization of inpatient service is influenced by demographic or socioeconomic factors or not, such as medical insurance (NCMS), age, gender, marital status, education, occupation, labor force, chronic disease, and income level. The findings from this study form a certain scientific basis for further modulation of the medical security system, which will allow for the development of effective corresponding countermeasures to improve the utilization of medical care, elevate health statuses, and impel the equality and accessibility of health service utilization.
2. Materials and Methods
2.1. Subjects and Methods
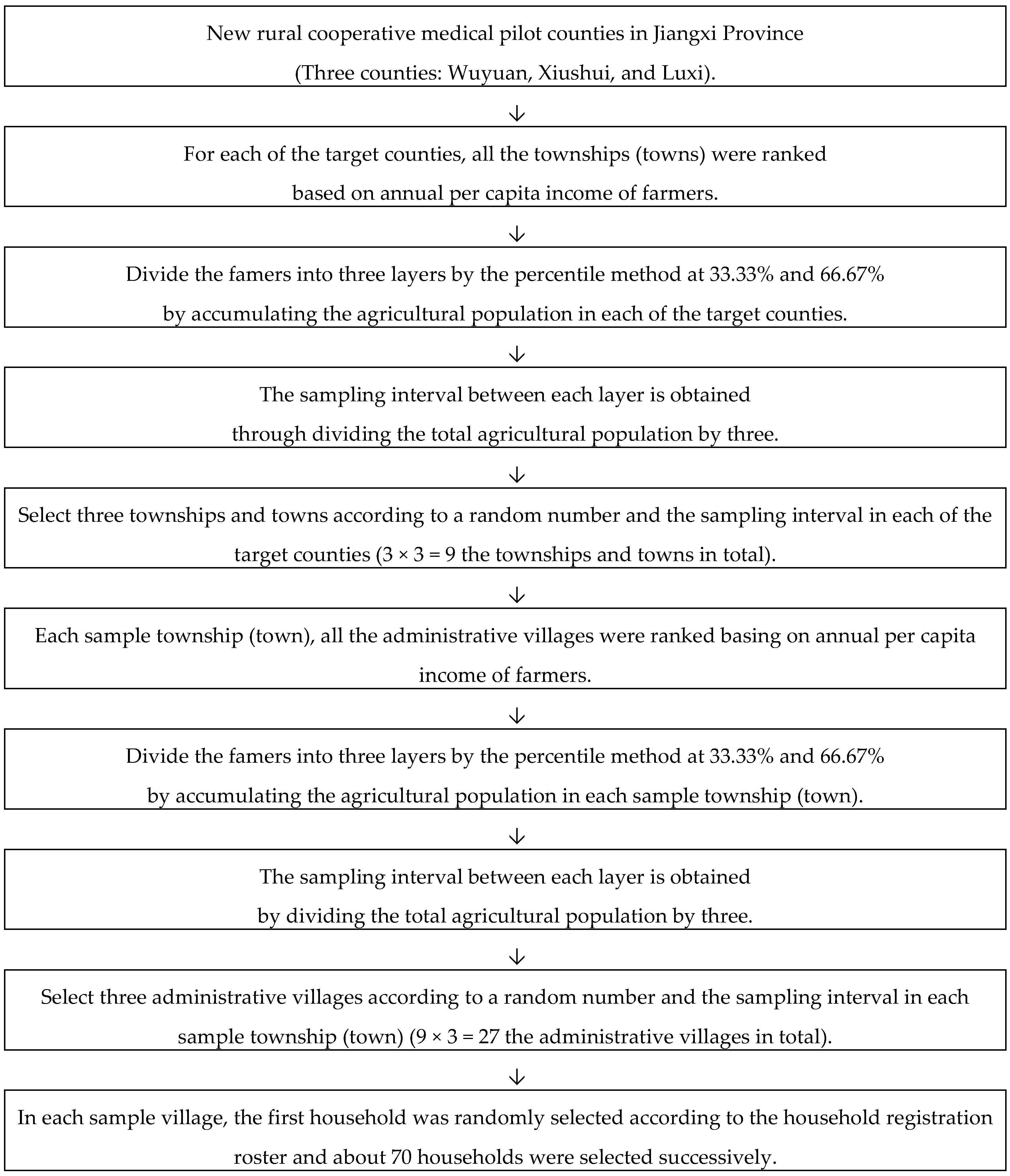
Jiangxi Province is a less developed region located in middle China. This study was initially carried out in Wuyuan, Xiushui, and Luxi—three counties of Jiangxi Province—which are the first batch and second batch of new rural cooperative medical pilot counties. Multi-stage stratified cluster random sampling method was used to randomly select the research objects in the sample counties. For each of the target counties, all the townships and towns were ranked based on annual per capita income of farmers. The three-point system is used to divide the famers into three layers by the percentile method at 33.33% and 66.67% by accumulating the agricultural population in each of the target counties. The sampling interval between each layer is obtained through calculation of the total agricultural population. A random number was extracted from the random number table, and the townships and towns in the first layer were determined according to the cumulative agricultural population. The second random number was determined according to the sampling interval, and the sample towns on the second layer were selected. The third random number was determined in turn according to the sampling interval, and the sample towns on the third layer were selected. The sampling villages were selected in accordance with the sampling method of sample towns, and a total of 9 sample townships and towns were selected. Then, three administrative villages were randomly selected for each sample township (town) and a total of 27 sample villages were selected.
In each sample village, the first household was randomly selected according to the household registration roster and about 70 households were selected successively. All household members in the family were investigated through an interview questionnaire. In this study, a number of cross-sectional surveys were conducted in 2006, 2008, 2010, 2012, and 2014. In order to ensure data comparability, the sample villages selected for the five surveys were all the same [
15]. The sampling process is shown in
Figure 1.
A one-to-one household survey method was used in this study. The investigator conducted a questionnaire by asking the head of the household. If the household head was not at home, the questionnaire was completed asking other members of the family who were over 18 years of age. The questionnaire included general demographic characteristics, health statuses of family members, and family members’ health service needs and utilization status [
16]. The subjects in this paper were the female aged 45 and above, living in rural areas for more than half a year which were adhered to classification standard of middle-aged and elderly age by the United Nations WHO.
2.2. Sample Size Calculation
The sample content required in this study is formulated as follows:
Using the previous baseline results, the hospitalization rate of rural residents within one year was π = 4.00%, , , , with the result of: people. There were 8082, 8015, 7524, 7857, and 7808 objects, respectively, in the five follow-up surveys, which were all larger than the theoretical sample size.
2.3. Weighing Methods
Complex sampling survey refers to the random sampling of research objects in each layer according to the proportion after stratification of subjects. Owing to the existence of sampling error, there is always a deviation in population conjectured by sample, which skews the result away from features of the population. Therefore, post-stratification weighting is needed to adjust the data and reduce errors [
17]. The weights were calculated in this study by first calculating the individual basis weights, then calculating the individual adjustment weights, and finally calculating the product of the individual basis weights and the adjustment weights to obtain the individual final weights [
18], according to the method described previously [
19]. The Weighted process is shown in
Figure 2.
2.3.1. The Calculation of Individual Base Weight
The sampling weight (Wi) of observing individual (i) is the inverse of the sampling probability Pi of that individual, i.e., Wi = 1/Pi. Therefore, for three-stage stratified cluster random sampling, the sampling weight of the sampling units in stage 1 is W1, the sampling weight of the sampling units in stage 2 is W2| 1, and the sampling weight of the sampling units in stage 3 is W 3| 2, 1. The individual base weight is the product of sampling weights of each stage, so the individual base weight observation units is: Wbase = W1 × W2| 1 × W 3| 2, 1.
2.3.2. The Calculation of Individual Adjusted Weight
The adjustment weight is calculated to make the distribution of individual sex and age in the sample consistent with the distribution of individual sex and age in the known population. First, the gender and age are stratified, that is, there were 2 layers of gender (i = 1, 2) and 8 layers of age (j = 1, 2, 3, 4, 5, 6, 8). The overlapping of these layers is the minimum layer, with a total of 16 layers (2 × 8 = 16). The population Nij of each individual layer after cross stratification of gender and age in the known population is then calculated.
The sum of the base weights of the respondents after cross-stratification of gender and age is:
Individual adjusted weights in each layer after cross-stratification of gender and age in the sample is calculated:
2.3.3. The Calculation of Individual Final Weight
Individual final weight is the product of the individual basis weight and the individual adjustment weight, and the calculation formula is:
2.4. Index Construction
2.4.1. Chronic Diseases
Various chronic diseases, including chronic infectious and non-communicable diseases, were clearly diagnosed by medical staff through inquiring surveyed people during the first half year of the survey; participants who were diagnosed with chronic diseases by doctors half a year before the survey, and had seizures and were taking treatment, including medication and physical therapy, was also taken into account.
2.4.2. Hospitalization within One Year
Surveyed people went to the hospital for hospitalization within one year from the date of survey.
2.4.3. Should be Hospitalized but Not Hospitalized
Within one year from the date of the survey, the respondent had a case in which the doctors recommended the person to be hospitalized but was not actually hospitalized.
2.4.4. Early Hospital Discharge
A case of early discharge from hospital in the previous year from the date of investigation.
2.4.5. Utilization of Inpatient Services
The hospitalization rate, early discharge rate, and rate of recommendation for hospitalization but not hospitalized in the past year. Hospitalization rate (%) = number of hospitalizations/number of surveyed ×100%; Early discharge rate (%) = number of patients discharged in advance/number of hospitalization ×100%; rate of supposed to be hospitalized but not hospitalized (%) = number of recommended but not hospitalized/number of recommended for hospitalization but not hospitalized + number of hospitalized inpatients×100%.
2.4.6. Income Level
The household income per capita was arranged in order of low to high, and then divided into five groups: low level income, low middle level income, middle level income, upper middle level income, and high-level income.
2.4.7. The New Rural Cooperative Medical Care (NRMC)
This is a new type of rural medical care and mutual aid system that is organized, guided, and supported by the government. The NRMC system collects funds through individual payment, collective support, and government subsidy with voluntary participation by farmers, and the overall goal is to better coordinate major diseases and reduce rural medical disasters [
13,
20,
21,
22,
23]. The NRMC started its pilot implementation in 2003 and the amount of funds raised in 2006 was 30 yuan in Jiangxi Province. The level of fundraising increased to 60 yuan in 2006, 300 yuan in 2012, and reached 390 yuan by 2014, respectively. At the same period, the hospitalization deduction line was designed to be 100 yuan for the designated township (town) level medical institutions with the hospitalization reimbursement ratio of 60%. The initial deduction line was removed in 2014 for the designated medical institutions and the proportion of hospitalization reimbursement increased to 90% (
Table 1).
2.5. Statistic Methods
Epidata 3.0 was employed to input data, and the database was imported into Excel and transferred to SPSS 24.0 statistical software (IBM Corporation, Chicago, IL, USA,) for analysis. The differences between variables were compared using the χ
2 statistic method after the complex sampling was weighted. The complex sampling logistics regression was used in multi-factor analysis with the test standard set as α = 0.05 and to analyze 3 index factors in the utilization of inpatient services. Crude odds ratio (cOR) refers to the result obtained by putting variables into the equation separately for analysis. Adjust odds ratio (aOR) refers to the result of putting the independent variables into thee equations together for analysis [
24,
25].
2.6. Quality Control
In order to ensure the comparability of the data, both the follow-up survey and the baseline survey were sampled in the same towns and villages. Study team members included postgraduates of the public health school of Nanchang University and they all had experience in survey study and received special training before the investigation including unified standard language. During the survey, village cadres of the study sites were available to assist investigators in any translation and completion of the survey together. At the end of the survey day, all investigators gathered together to input data. If any errors or omissions were found, the local village cadres were contacted to reach the respondents by telephone or other approaches to complete the questionnaire. Data input was carried out through double entry with logical correction and timely error correction.
The Maye index is an indicator for judging the quality of survey data by evaluating the logic within the survey data [
26]. A Maye coefficient greater than 60 indicates that there is a serious age preference or accumulation in the survey population data. The Maye index is less than 60, which can be judged as good data quality [
27]. The Maye index of the six surveys in this study was 7.78, 9.81, 12.02, 8.52, 3.54, and 7.07, respectively, indicating that there was no serious age preference in the sample population data, and the survey data quality was good.
The goodness-of-fit test is a statistical method developed by K Pearson, a British statistician, and it is used to ensure the consistency between actual observations and theoretical numbers, calculated according to some hypothesis or model [
28]. This study used the data of the population age (gender) of the Jiangxi Statistical Yearbook as a reference and the census data of each year in Jiangxi Province as the theoretical frequency, which were assumed to be in a normal distribution. Each survey data was used as sample data to observe the degree to which the distribution of sample data fits the theoretical frequency distribution. If there was no significant difference in the test results, it indicated that the survey data are of good quality and the sample data are representative. The chi-square values of the population age composition of Jiangxi Province for the six-time surveys were 3.17, 4.99, 7.48, 5.63, 6.44, and 3.49, respectively. The chi-square values of the gender composition fitness test were 0.001445, 0.000196, 0.000484, 0.110294, 0.002118, and 0.006895, respectively. All the P values are greater than 0.05, which indicates that the distribution of age and gender of the sample data is not significantly different from the overall population distribution in Jiangxi Province, and thus the survey data is representative.
2.7. Ethical Approval
The study was approved by the Nanchang University Institutional Review Board. We have ethical approval on file. Oral consents of farmers who participated in the survey were obtained.
4. Discussion
Jiangxi Province, as one of the economically underdeveloped regions, has a large number of labor force output. However, middle-aged and elderly females who do not have many labor skills have to stay in the countryside to undertake agricultural production and heavy and trivial housework. Therefore, they become the vulnerable group whom needs to get special attention. In the past 20 years, China has carried out a series of medical and health security system reforms in order to promote health equity and eliminate the gap between groups; medical coverage has almost reached the entire population [
29]. However, there are few studies investigating the utilization of inpatient services in vulnerable groups. This study found that more than half of MAEF staying in rural areas were over 55 years old, the majority (75%) had primary education or below, 94.6% were farmers, and 25.7% suffered from chronic diseases. Due to the low health and high ratio of chronic diseases among MAEF, the utilization of inpatient services is worthy of attention.
The hospitalization rate of middle-aged and elderly rural females in underdeveloped regions has an overall upward trend from 2006 to 2014. In 2006, the proportion of inpatients for those who should be hospitalized but not hospitalized exhibited an overall downward trend. A similar trend is also detected for the early discharge rate. According to the study by the China Health and Retirement Longitudinal Study (CHARLS), about 9% of middle-aged and elderly people have been hospitalized in the past year, which means at least 40.4 million middle-aged and elderly people are hospitalized in China every year [
4]. According to the fourth national health service survey of China, the hospitalization rate of the whole rural population was 9.0% in 2013, varying between 7.6% and 10.0% in different regions [
30], which was lower than the survey results of this study. This can be explained that the use of inpatient services for middle-aged and elderly females in rural areas in less developed areas in China such as Jiangxi has been gradually enhanced since 2006.
The medical security system is known to have an impact on the use of inpatient services [
23,
31,
32]. Some studies have shown that patients enrolled in NRCM are more likely to seek health care services [
2,
33,
34,
35]. The NRCM got started in Jiangxi Province in 2003, and Wuyuan, Xiushui, and Luxi counties were randomly selected for this study to examine the impact of this new system in 2005. The rate of hospitalization of middle-aged and elderly females in 2014 was higher than that in 2006 (aOR = 2.384), while the early discharge rate from hospital (aOR = 0.177) and rate of females who should be hospitalized but not hospitalized (aOR = 0.347) were lower than those reported in 2006. These findings indicate that the utilization of inpatient services for middle-aged and elderly females in rural underdeveloped areas was further promoted with time. The positive change may be related to the improvement of the NRCM system [
36]. In addition, with the increase of finding levels from 2006 to 2014, its reimbursement compensation program is also constantly being adjusted and improved [
31]. In 2014, the township (town)-level fixed-point medical institutions did not set up deductible lines, and the proportion of hospitalization compensation increased to 90%. The proportion of hospitalization compensation for designated medical institutions at county (city, district)-level reached 80%. These results reveal that the improvement of compensation programs has improved residents’ utilization of primary inpatient medical services. Also the implementation of the NRCM system has effectively provided health protection for middle-aged and elderly women, and promoted the utilization of inpatient health services for rural middle-aged and elderly women in underdeveloped areas [
3].
Present studies have shown that household income is beneficial to the use of inpatients in the rich, which is the dominant determinant of inequality in the utilization of inpatient services since more wealthy individuals are able to pay for and utilize more inpatient services [
37,
38,
39]. But some studies have shown that the differences of health service utilization between income groups were not significant [
40]. In this study, the average annual household income was divided into five levels and the differences in the inpatient service utilization among middle-aged and elderly females at different levels were not statistically significant. Some studies have shown that residents’ household economic income level should play a role in their utilization of hospitalization services, but this study did not find that household economic income has a significant impact on the utilization of hospitalization services for middle-aged and elderly females. From 2006 to 2014, China’s economy developed rapidly, and the per capita annual income of residents also greatly improved. Our study also reveals that the gradual increase in the utilization of inpatient service among MAEF is not affected by economic income, but mainly due to the continuous improvement of the new rural cooperative medical insurance system. The new rural cooperative medical care system is a basic medical insurance system established by China in the world’s largest population group. The establishment of the system greatly facilitated the demand and utilization of medical services by rural residents, improved the fairness and access to medical service in rural areas, and offered special benefit to vulnerable groups [
41] such as middle-aged and elderly women. At present, this system has been merged with the basic medical care system for urban residents and is constantly being improved [
31]. Findings from this study suggest to speed up the improvement of this medical security system, further improve its financing level and compensation scheme, so as to provide better medical protection for urban and rural residents [
12,
42].
Many studies have shown that the utilization of inpatient service is influenced by demographic or socioeconomic factors, such as age, gender, marital status, education, medical insurance, standard of living, and urban residence [
4,
29,
43,
44]. Based on the multivariate complex sampling logistic regression analysis, this study shows that the utilization of inpatient services of middle-aged and elderly females in underdeveloped areas was mainly related to marital status, whether they were in the labor force, and whether they suffered from chronic diseases. This study also reveals that, compared to married MAEF, divorced or widowed ones inadequately utilized hospitalization services, with a lower likelihood of hospitalization (aOR = 0.569), but higher rate for the recommended hospitalization but hot hospitalized (aOR = 3.237). It may be due to divorced and widowed females who need to bear the pressure of life alone and have a heavier living burden. In situations where a doctor recommends hospitalization, divorced or widowed ones may choose to self-medicate or postpone hospitalization. The lack of family care during hospitalization may also affect the utilization of hospitalization services for middle-aged and elderly females who are divorced or widowed.
In this study, it was found that the hospitalization rate of middle-aged and elderly females not in the labor force was 1.976 times than that of elderly females in the labor force (
p < 0.05). It is possible that non-labor MAEF in rural areas are older with poorer health [
45].
This study shows that the middle-aged and elderly females with chronic diseases had a higher rate for hospitalization (aOR = 3.682), higher rate for recommended hospitalization but not hospitalized (aOR = 7.689), and higher rate for early discharge (aOR = 3.258) than those without chronic diseases. This may reflect the situation in that MAEF with chronic non-communicable diseases have the needs for health care on one hand, however, they have heavier medical economic burden because of long-time illness and the lack of the sense of paying attention to diseases. In addition, as the NRCM can only recapture some of the cost for medicine which may aggravate more cases of early hospital discharge and also the recommended hospitalization but not hospitalized [
46,
47]. These findings indicate an urgent need to strength the prevention and treatment of chronic diseases among MAEF and improve the health status of these females [
48]. Also, there is a need to design appropriate corresponding compensation scheme for patients with chronic diseases, so that they can make full use of inpatient services.
5. Limitation
Data in this paper is collected according to the sampling plan using multi-stage stratified cluster sampling with the assistance of the local government department staff and village cadres through interviews with householders. Although every household answered the questionnaire to avoid bias caused by not replying, the use of the local government department staff and village cadres may cause selection bias. Thus, more attention was paid to limit and reduce the involvement of local government staff and village cadres.
The annual per capita income included in this study may have recall bias, which is a common limitation of the survey research. Our research group conducted a special explanation for the survey method of annual per capita income. All investigators followed the same standard for the recording of household per capita income thereby reducing error. In this study, the utilization of inpatient services was answered only by the respondents, and some villagers would even present their hospitalization documents to ensure the accuracy of information.
One of the limitations of this study was that household heads were responsible for answering all the questions for their household members. In the absence of the household head, an adult member of the household with information about the household members responded for the household members. It may be problematic for the household head or the representative to provide accurate responses for all household members. However, considering that the household sizes are generally small (often less than five), and being a rural area where information is often shared among household members, we do not expect so much variation in the responses from individuals from the same household. And the utilization of inpatient services of household members in rural regions is significant, which may get accurate responses.

 ,
, 


{kind=link}
{kind=link}