Changes in Water Soluble Uremic Toxins and Urinary Acute Kidney Injury Biomarkers After 10- and 100-km Runs

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
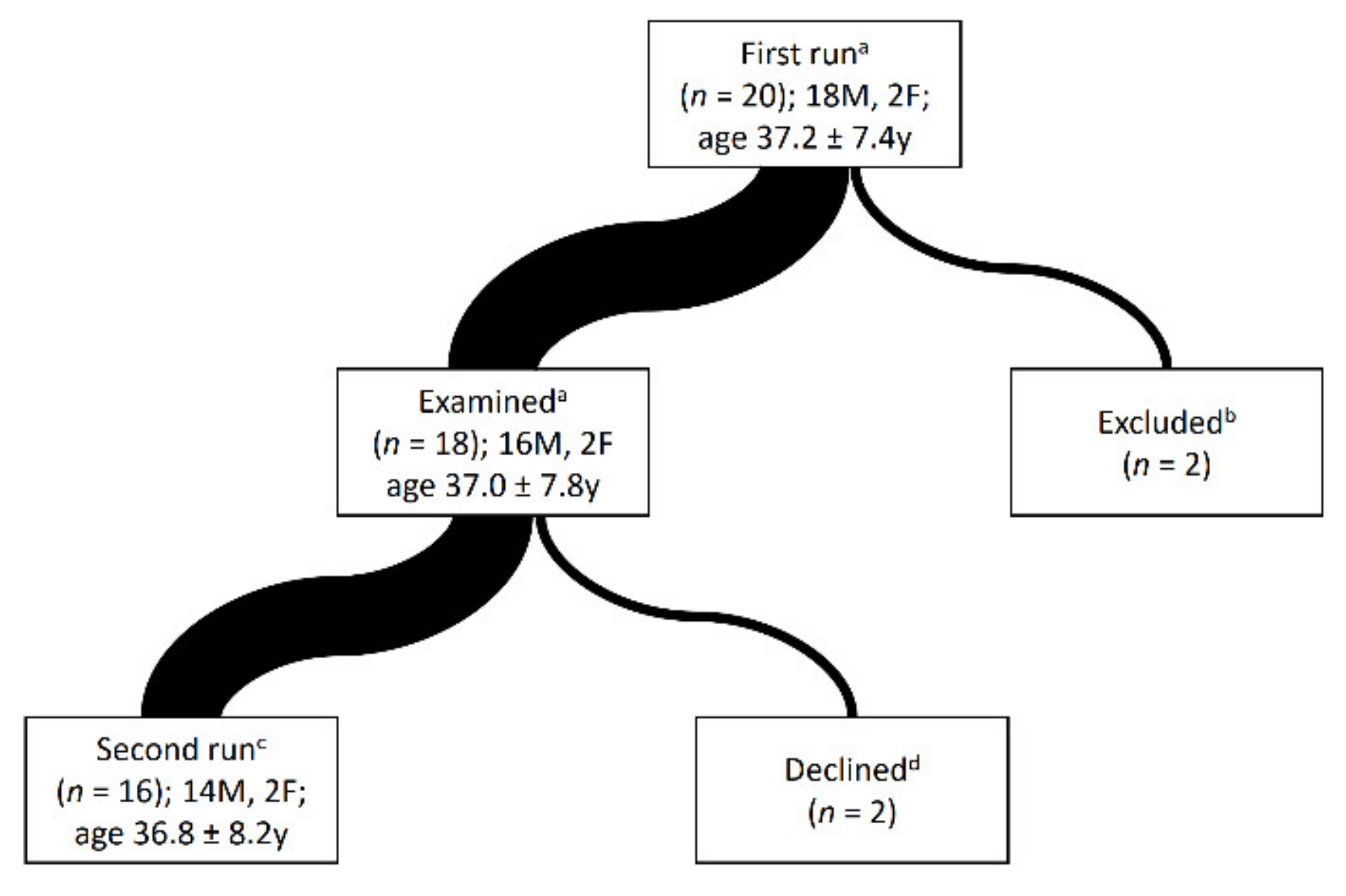
2.1. Subjects Selection
2.2. Races
2.3. Questionnaires and Anthropometric Data
2.4. Weather Conditions
2.5. Biochemical Analyses
2.5.1. Urinalysis
2.5.2. Measurement of Creatinine, Urea and Uric Acid
Creatinine, Urea and Uric Acid Were Measured in Serum and Spot Urine
100-km—Creatinine, Urea and Uric Acid Were Measured in Serum and Spot Urine
10-km—Creatinine, Urea and Uric Acid Were Measured in Serum and Spot Urine
2.5.3. Measurement of ADMA, SDMA, TMAO
2.5.4. Measurement of Albuminuria
Albuminuria—100 km
Albuminuria—10 km
2.5.5. Measurement of Urine Human Lipocalin-2/NGAL, TIM-1/KIM-1/HAVCR and Cystatin C Concentrations
2.5.6. Calculations and Equations
Acute Kidney Injury Definition and Reference Values for Urinary AKI Biomarkers
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Runners and the Races
3.2. Urinalysis
3.3. Albuminuria and Urinary New Biomarkers of AKI
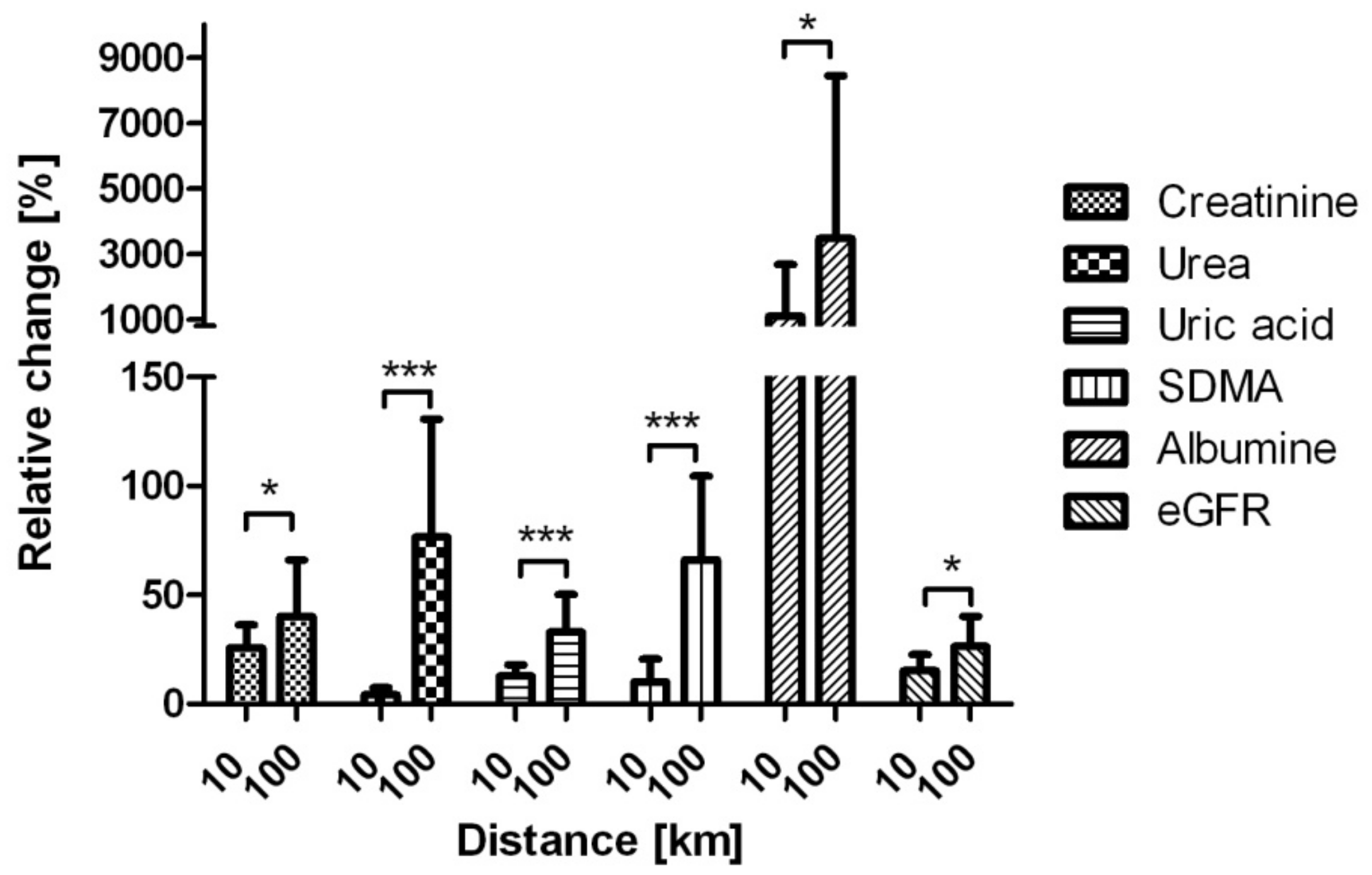
3.4. Urea, Uric Acid, Creatinine, eGFR CKD EPI
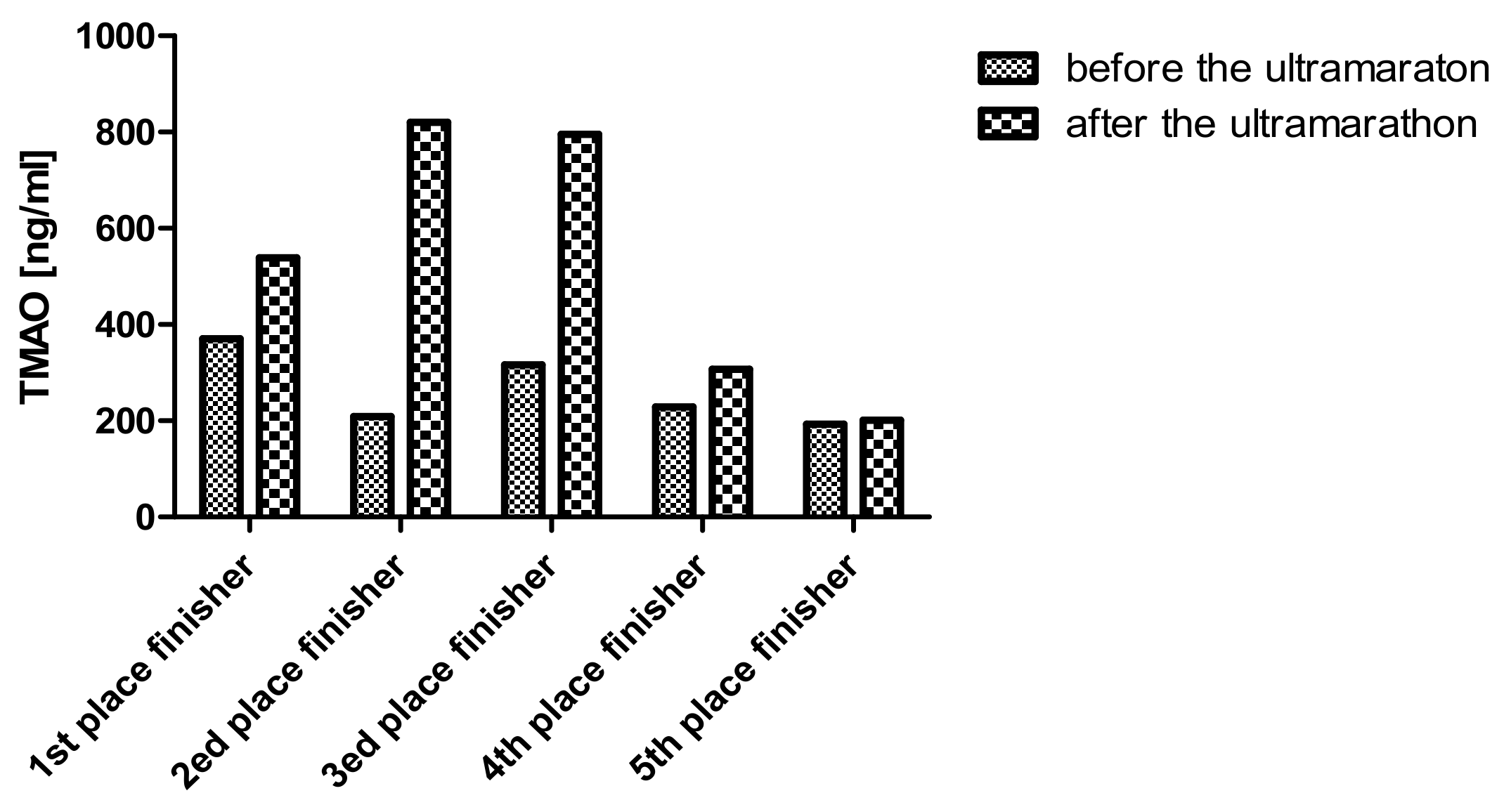
3.5. Novel Water Soluble Toxins
3.6. Relative Changes in Uremic Toxins After Both Races
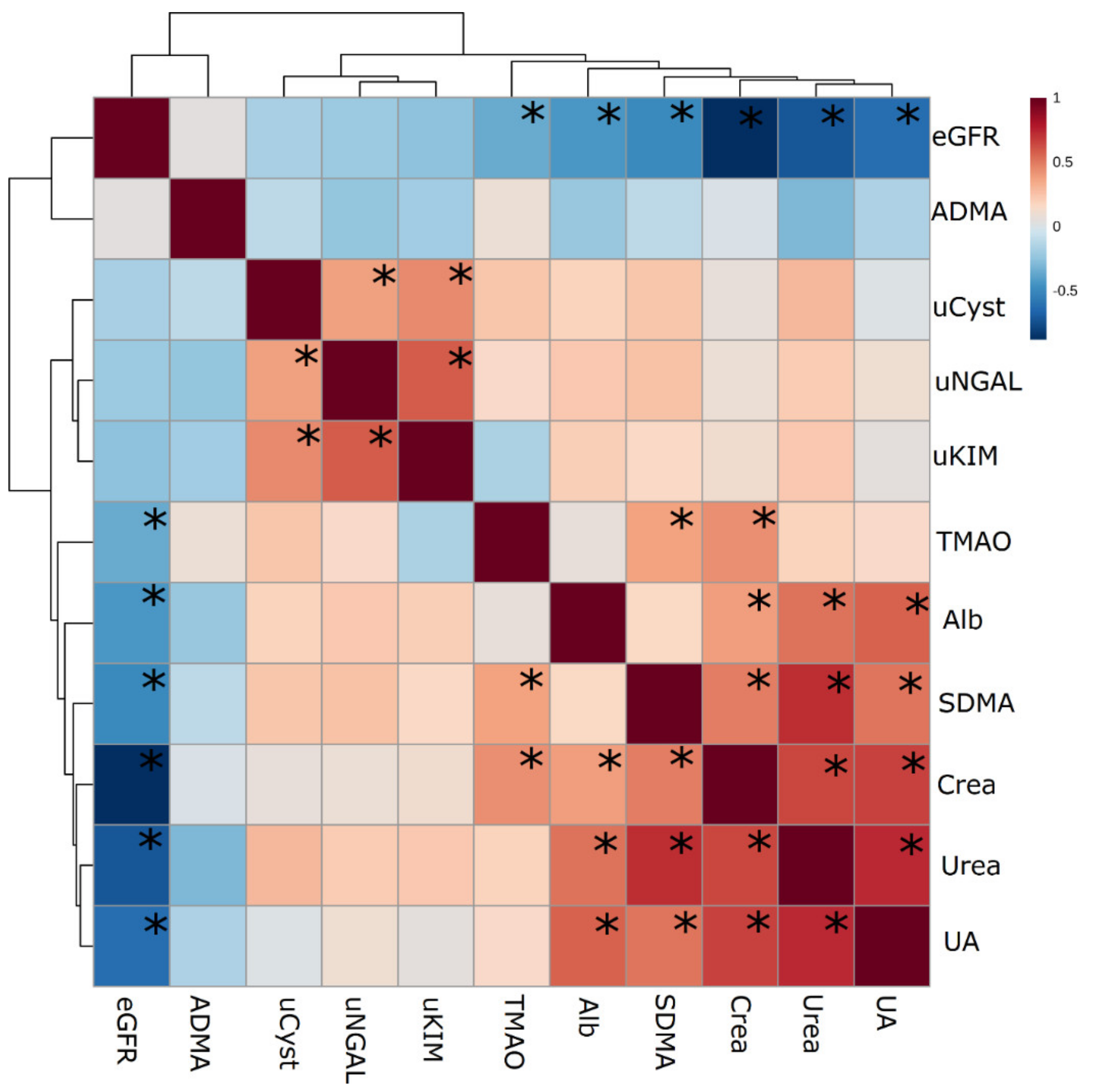
3.7. Correlations between Studied Markers of AKI
3.8. Diagnosis of AKI
4. Discussion
4.1. The Changes in Urinary Markers are Universal After Running
4.2. Changes in Serum Toxins and Their Fractional Excretion
4.3. Changes in New Water Soluble Toxins
4.4. Summary
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hodgson, L.E.; Walter, E.; Venn, R.M.; Galloway, R.; Pitsiladis, Y.; Sardat, F.; Forni, L.G. Acute kidney injury associated with endurance events-is it a cause for concern? A systematic review. Nephrology 2018, 23, 969–980. [Google Scholar] [CrossRef] [PubMed]
- Rangaswamy, D.; Sud, K. Acute kidney injury and disease: Long-term consequences and management. BMJ Open Sport Exerc. Med. 2017, 3, e000093. [Google Scholar] [CrossRef] [PubMed]
- 52 Marathons in Fifty Two Weeks Running Club. Available online: http://52in52.org/ (accessed on 6 September 2019).
- Lima, R.S.A.; Junior, G.B.D.S.; Liborio, A.B.; Daher, E.D.F. Acute kidney injury due to rhabdomyolysis. Saudi J. Kidney Dis. Transplant. 2008, 19, 721–729. [Google Scholar]
- Lipman, G.S.; Shea, K.; Christensen, M.; Phillips, C.; Burns, P.; Higbee, R.; Koskenoja, V.; Eifling, K.; Krabak, B.J. Ibuprofen versus placebo effect on acute kidney injury in ultramarathons: A randomised controlled trial. Emerg. Med. J. 2017, 34, 637–642. [Google Scholar] [CrossRef]
- Chapman, C.L.; Johnson, B.D.; Sackett, J.R.; Parker, M.D.; Schlader, Z.J. Soft drink consumption during and following exercise in the heat elevates biomarkers of acute kidney injury. Am. J. Physiol. Integr. Comp. Physiol. 2019, 316, R189–R198. [Google Scholar] [CrossRef]
- Ad-Hoc Working Group of ERBP; Fliser, D.; Laville, M.; Covic, A.; Fouque, D.; Vanholder, E.; Juillard, L.; Van Biesen, W. A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: Part 1: Definitions, conservative management and contrast-induced nephropathy. Nephrol. Dial. Transplant. 2012, 27, 4263–4272. [Google Scholar]
- Shoaib, M.; Mahmud, S.N.; Safdar, M. Early Diagnosis Of Acute Kidney Injury By Urinary Neutrophil Gelatinase Associated Lipocalin In Adult Critically Ill Patients. J. Ayub Med. Coll. Abbottabad: JAMC 2019, 31, 12–15. [Google Scholar]
- Skowron, B.; Baranowska, A.; Dobrek, L.; Ciesielczyk, K.; Kaszuba-Zwoinska, J.; Wiecek, G.; Malska-Wozniak, A.; Strus, M.; Gil, K. Urinary neutrophil gelatinase-associated lipocalin, kidney injury molecule-1, uromodulin, and cystatin C concentrations in an experimental rat model of ascending acute kidney injury induced by pyelonephritis. J. Physiol. Pharmacol. 2018, 69, 625–637. [Google Scholar]
- Brinley, A.; Chakravarthy, B.; Kiester, D.; Hoonpongsimanont, W.; McCoy, C.E.; Lotfipour, S. Compartment Syndrome with Rhabdomyolysis in a Marathon Runner. Clin. Pr. Cases Emerg. Med. 2018, 2, 197–199. [Google Scholar] [CrossRef]
- Little, C.E.; Lipman, G.S.; Migliaccio, D.; Young, D.S.; Krabak, B.J. Accuracy of Estimated Creatinine in Multistage Ultramarathon Runners. Wilderness Environ. Med. 2019, 30, 129–133. [Google Scholar] [CrossRef]
- Wołyniec, W.; Ratkowski, W.; Kasprowicz, K.; Małgorzewicz, S.; Aleksandrowicz, E.; Witek, K.; Grzywacz, T.; Żmijewski, P.; Renke, M. Changes in electrolytes and uric acid excretion during and after a 100 km run. J. Biol. Regul. Homeost. Agents. 2018, 32, 1205–1210. [Google Scholar] [PubMed]
- Liu, X.; Xu, X.; Shang, R.; Chen, Y. Asymmetric dimethylarginine (ADMA) as an important risk factor for the increased cardiovascular diseases and heart failure in chronic kidney disease. Nitric Oxide 2018, 78, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Noel, S.; Pluznick, J.L.; Hamad, A.R.A.; Rabb, H. Gut Microbiota-Kidney Cross-Talk in Acute Kidney Injury. Semin. Nephrol. 2019, 39, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ufnal, M.; Zadlo, A.; Ostaszewski, R.; Zadlo-Dobrowolska, A. TMAO: A small molecule of great expectations. Nutrition 2015, 31, 1317–1323. [Google Scholar] [CrossRef]
- Erickson, M.L.; Malin, S.K.; Wang, Z.; Brown, J.M.; Hazen, S.L.; Kirwan, J.P. Effects of Lifestyle Intervention on Plasma Trimethylamine N-Oxide in Obese Adults. Nutrition 2019, 11, 179. [Google Scholar] [CrossRef]
- Riccioni, G.; Scotti, L.; Guagnano, M.T.; Bosco, G.; Bucciarelli, V.; Di Ilio, E.; Speranza, L.; Martini, F.; Bucciarelli, T. Physical exercise reduces synthesis of ADMA, SDMA, and L-Arg. Front. Biosci. 2015, 7, 417–422. [Google Scholar] [CrossRef]
- Shirley, D.G.; Unwin, R.J. Renal Physiology. In Comprehensive Clinical Nephrology, 4th ed.; Floege, J., Johnson, R.J., Feehally, J., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2010; pp. 15–28. ISBN 978-0-323-05876-6. [Google Scholar]
- Jay, V. Richard Bright—Physician Extraordinaire. Arch. Pathol. Lab. Med. 2000, 124, 1262–1263. [Google Scholar]
- Shephard, R.J. Exercise proteinuria and hematuria: Current knowledge and future directions. J. Sports Med. Phys. Fitness 2016, 56, 1060–1076. [Google Scholar]
- Skálová, S. The diagnostic role of urinary N-acetyl-beta-D-glucosaminidase (NAG) activity in the detection of renal tubular impairment. Acta Med. 2005, 48, 75–80. [Google Scholar]
- Vaidyanathan, K. Urinary proteomics and metabolomics in the diagnosis of pediatric disorders. Proteom. Clin. Appl. 2015, 9, 482–489. [Google Scholar] [CrossRef]
- Teo, S.H.; Endre, Z.H. Biomarkers in acute kidney injury (AKI). Best Pr. Res. Clin. Anaesthesiol. 2017, 31, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Nan-Ya, K.; Kajihara, M.; Kojima, N.; Degawa, M. Usefulness of urinary kidney injury molecule-1 (Kim-1) as a biomarker for cisplatin-induced sub-chronic kidney injury. J. Appl. Toxicol. 2015, 35, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Junglee, N.A.; Di Felice, U.; Dolci, A.; Fortes, M.B.; Jibani, M.M.; Lemmey, A.B.; Walsh, N.P.; Macdonald, J.H. Exercising in a hot environment with muscle damage: Effects on acute kidney injury biomarkers and kidney function. Am. J. Physiol. Renal Physiol. 2013, 305, F813–F820. [Google Scholar] [CrossRef]
- Andreazzoli, A.; Fossati, C.; Spaccamiglio, A.; Salvo, R.; Quaranta, F.; Minganti, C.; Di Luigi, L.; Borrione, P. Assessment of pN-GAL as a marker of renal function in elite cyclists during professional competitions. J. Biol. Regul. Homeost. Agents 2017, 31, 829–835. [Google Scholar] [PubMed]
- Mansour, S.G.; Verma, G.; Pata, R.W.; Martin, T.G.; Perazella, M.A.; Parikh, C.R. Kidney Injury and Repair Biomarkers in Marathon Runners. Am. J. Kidney Dis. 2017, 70, 252–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlesinger, S.; Sonntag, S.R.; Lieb, W.; Maas, R. Asymmetric and Symmetric Dimethylarginine as Risk Markers for Total Mortality and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Studies. PLoS ONE 2016, 11, 0165811. [Google Scholar] [CrossRef]
- Poniewierka 14.09.2019—Biegi ultra na Kaszubach! Available online: http://www.kaszubskaponiewierka.pl/ (accessed on 6 September 2019).
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute kidney injury network. Acute kidney injury network: Report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Pennemans, V.; Rigo, J.-M.; Faes, C.; Reynders, C.; Penders, J.; Swennen, Q. Establishment of reference values for novel urinary biomarkers for renal damage in the healthy population: Are age and gender an issue? Clin. Chem. Lab. Med. 2013, 51, 1795–1802. [Google Scholar] [CrossRef]
- Bramble, D.M.; Lieberman, D.E. Endurance running and the evolution of Homo. Nature 2004, 432, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Schulte, K.; Kunter, U.; Moeller, M.J. The evolution of blood pressure and the rise of mankind. Nephrol. Dial. Transplant. 2015, 30, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Knechtle, B.; Nikolaidis, P.T. Physiology and Pathophysiology in Ultra-Marathon Running. Front. Physiol. 2018, 9, 634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, K.D. “Athletic Pseudonephritis”-Alteration of Urine Sediment by Athletic Competition. J. Am. Med. Assoc. 1956, 161, 1613. [Google Scholar] [CrossRef]
- Wołyniec, W.; Ratkowski, W.; Urbański, R.; Bartoszewicz, M.; Siluk, D.; Wołyniec, Z.; Kasprowicz, K.; Zorena, K.; Renke, M. Urinary Kidney Injury Molecule-1 but Not Urinary Neutrophil Gelatinase Associated Lipocalin Is Increased after Short Maximal Exercise. Nephron 2018, 138, 29–34. [Google Scholar] [CrossRef]
- Wasung, M.E.; Chawla, L.S.; Madero, M. Biomarkers of renal function, which and when? Clin. Chim. Acta 2015, 438, 350–357. [Google Scholar] [CrossRef]
- Jensen, D.; Kierulf-Lassen, C.; Kristensen, M.L.V.; Nørregaard, R.; Weyer, K.; Nielsen, R.; Christensen, E.I.; Birn, H. Megalin dependent urinary cystatin C excretion in ischemic kidney injury in rats. PLoS ONE 2017, 12, e0178796. [Google Scholar] [CrossRef]
- Dubin, R.F.; Judd, S.E.; Scherzer, R.; Shlipak, M.; Warnock, D.G.; Cushman, M.; Sarnak, M.; Parikh, C.; Bennett, M.; Powe, N.; et al. Urinary Tubular Injury Biomarkers Are Associated with ESRD and Death in the REGARDS Study. Kidney Int. Rep. 2018, 3, 1183–1192. [Google Scholar] [CrossRef]
- Machado, J.C.Q.; Volpe, C.M.; Vasconcellos, L.S.; Nogueira-Machado, J.A. Quantification of NGAL in Urine of Endurance Cycling Athletes. J. Phys. Act. Heal. 2018, 15, 679–682. [Google Scholar] [CrossRef]
- Bongers, C.C.W.G.; Alsady, M.; Nijenhuis, T.; Tulp, A.D.M.; Eijsvogels, T.M.H.; Deen, P.M.T.; Hopman, M.T.E. Impact of acute versus prolonged exercise and dehydration on kidney function and injury. Physiol. Rep. 2018, 6, e13734. [Google Scholar] [CrossRef]
- Gaião, S.M.; de Carvalho Paiva, J.A.O. Biomarkers of renal recovery after acute kidney injury. Rev. Bras. Ter. Intensiv. 2017, 29, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Da Ponte, A.; Giovanelli, N.; Antonutto, G.; Nigris, D.; Curcio, F.; Cortese, P.; Lazzer, S. Changes in cardiac and muscle biomarkers following an uphill-only marathon. Res. Sports Med. 2018, 26, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Sutton, J.R.; Toews, C.J.; Ward, G.R.; Fox, I.H. Purine metabolism during strenuous muscular exercise in man. Metabolism 1980, 29, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Kaya, M.; Moriwaki, Y.; Ka, T.; Inokuchi, T.; Yamamoto, A.; Takahashi, S.; Tsutsumi, Z.; Tsuzita, J.; Oku, Y.; Yamamoto, T. Plasma concentrations and urinary excretion of purine bases (uric acid, hypoxanthine, and xanthine) and oxypurinol after rigorous exercise. Metabolism 2006, 55, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Wołyniec, W.; Ratkowski, W.; Kasprowicz, K.; Puch-Walczak, A.; Wierucki, Ł.; Aleksandrowicz-Wrona, E.; Małgorzewicz, S.; Zdrojewski, T.; Renke, M. Changes in fractional uric excretion after marathon and ultramarathon. 55th ERA-EDTA Congress, Copenhagen, Denmark, May 24th–27th 2018. Nephrol. Dial. Transplant. 2018, 33 (Suppl. 1), i51–i52. [Google Scholar] [CrossRef]
- Hyndman, D.; Liu, S.; Miner, J.N. Urate Handling in the Human Body. Curr. Rheumatol. Rep. 2016, 18, 34. [Google Scholar] [CrossRef]
- De Oliveira, E.P.; Burini, R.C. High plasma uric acid concentration: Causes and consequences. Diabetol. Metab. Syndr. 2012, 4, 12. [Google Scholar] [CrossRef]
- Ortlund, E.; Murphy, M. Evolutionary history and metabolic insights of ancient mammalian uricases. Evol. Hist. Metab. Insights Anc. Mamm. Uricases 2014, 111, 3763–3768. [Google Scholar] [Green Version]
- Tanahashi, K.; Akazawa, N.; Miyaki, A.; Choi, Y.; Ra, S.-G.; Matsubara, T.; Kumagai, H.; Oikawa, S.; Miyauchi, T.; Maeda, S. Plasma ADMA concentrations associate with aerobic fitness in postmenopausal women. Life Sci. 2014, 108, 30–33. [Google Scholar] [CrossRef]
- Fiodorenko-Dumas, Z.; Dumas, I.; Mastej, K.; Adamiec, R. Physical activity–related changes in ADMA and vWF levels in patients with type 2 diabetes—A preliminary study. Adv. Clin. Exp. Med. 2017, 26, 601–608. [Google Scholar] [CrossRef]
- Teplan, V.; Mahrova, A.; Racek, J.; Gürlich, R.; Valkovsky, I.; Štollova, M.; Pitha, J.; Telphan, V., Jr. Early Exercise Training After Renal Transplantation and Asymmetric Dimethylarginine: The Effect of Obesity. Kidney Blood Press. Res. 2014, 39, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Mittermayer, F.; Pleiner, J.; Krzyzanowska, K.; Wiesinger, G.F.; Francesconi, M.; Wolzt, M. Regular physical exercise normalizes elevated asymmetrical dimethylarginine concentrations in patients with type 1 diabetes mellitus. Wien. Klin. Wochenschr. 2005, 117, 816–820. [Google Scholar] [CrossRef] [PubMed]
- Tanahashi, K.; Akazawa, N.; Miyaki, A.; Choi, Y.; Ra, S.G.; Matsubara, T.; Kumagai, H.; Oikawa, S.; Maeda, S. Aerobic exercise training decreases plasma asymmetric dimethylarginine concentrations with increase in arterial compliance in postmenopausal women. Am. J. Hypertens. 2014, 27, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Baldassarri, F.; Schwedhelm, E.; Atzler, D.; Böger, R.H.; Cordts, K.; Haller, B.; Pressler, A.; Müller, S.; Suchy, C.; Wachter, R.; et al. Relationship between Exercise Intervention and NO pathway in Patients with Heart Failure with Preserved Ejection Fraction. Biomarkers 2018, 23, 1–37. [Google Scholar] [CrossRef]
- Ilic, M.D.; Pavlovic, R.; Lazarevic, G.; Živanović, S.; Cvetkovic, T.; Kocic, G.; Ilić, S.; Ambrosio, G. Detrimental effects of a bout of physical exercise on circulating endogenous inhibitors of endothelial function in patients with coronary artery disease. J. Cardiovasc. Med. 2017, 18, 610–616. [Google Scholar] [CrossRef]
- Zoccali, C.; Kielstein, J.T. Asymmetric dimethylarginine: A new player in the pathogenesis of renal disease? Curr. Opin. Nephrol. Hypertens. 2006, 15, 314–320. [Google Scholar] [CrossRef]
- Achan, V.; Broadhead, M.; Malaki, M.; Whitley, G.; Leiper, J.; MacAllister, R.; Vallance, P. Asymmetric Dimethylarginine Causes Hypertension and Cardiac Dysfunction in Humans and Is Actively Metabolized by Dimethylarginine Dimethylaminohydrolase. Arter. Thromb. Vasc. Boil. 2003, 23, 1455–1459. [Google Scholar] [CrossRef] [Green Version]
- Pawlak-Chaouch, M.; Boissière, J.; Munyaneza, D.; Tagougui, S.; Gamelin, F.X.; Cuvelier, G.; Heyman, E.; Goossens, J.F.; Descat, A.; Berthoin, S.; et al. Plasma asymmetric dimethylarginine concentrations are not related to differences in maximal oxygen uptake in endurance trained and untrained men. Exp. Physiol. 2019, 104, 254–263. [Google Scholar] [CrossRef]
- Niebauer, J.; Clark, A.L.; Webb-Peploe, K.M.; Boger, R.; Coats, A.S. Home-based exercise training modulates pro-oxidant substrates in patients with chronic heart failure. Eur. J. Hear. Fail. 2005, 7, 183–188. [Google Scholar] [CrossRef]
- Penka, M.; Grdić, M.; Steiner, S.; Strasser, B.; Ziegler, S.; Zorn, G.; Maurer, G.; Simeon-Rudolf, V.; Wojta, J.; Huber, K.; et al. Endurance training reduces circulating asymmetric dimethylarginine and myeloperoxidase levels in persons at risk of coronary events. Thromb. Haemost. 2005, 94, 1306–1311. [Google Scholar] [CrossRef]
- Maeda, S.; Miyaki, A.; Kumagai, H.; Eto, M.; So, R.; Tanaka, K.; Ajisaka, R. Lifestyle modification decreases arterial stiffness and plasma asymmetric dimethylarginine level in overweight and obese men. Coron. Artery Dis. 2013, 24, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Ballard, K.D.; Duguid, R.M.; Berry, C.W.; Dey, P.; Bruno, R.S.; Ward, R.M.; Timmerman, K.L. Effects of prior aerobic exercise on sitting-induced vascular dysfunction in healthy men. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 117, 2509–2518. [Google Scholar] [CrossRef] [PubMed]
- Kielstein, J.T.; Salpeter, S.R.; Bode-Boeger, S.M.; Cooke, J.P.; Fliser, D. Symmetric dimethylarginine (SDMA) as endogenous marker of renal function—A meta-analysis. Nephrol. Dial. Transplant. 2006, 21, 2446–2451. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Pletinck, A.; Schepers, E.; Glorieux, G. Biochemical and Clinical Impact of Organic Uremic Retention Solutes: A Comprehensive Update. Toxins 2018, 10, 33. [Google Scholar] [CrossRef]
- Velasquez, M.T.; Ramezani, A.; Manal, A.; Raj, D.S. Trimethylamine N-Oxide: The Good, the Bad and the Unknown. Toxins 2016, 8, 326. [Google Scholar] [CrossRef]
- Stubbs, J.R.; House, J.A.; Ocque, A.J.; Zhang, S.; Johnson, C.; Kimber, C.; Schmidt, K.; Gupta, A.; Wetmore, J.B.; Nolin, T.D.; et al. Serum Trimethylamine-N-Oxide is Elevated in CKD and Correlates with Coronary Atherosclerosis Burden. J. Am. Soc. Nephrol. 2016, 27, 305–513. [Google Scholar] [CrossRef]
- Gruppen, E.G.; Garcia, E.; Connelly, M.A.; Jeyarajah, E.J.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F. TMAO is Associated with Mortality: Impact of Modestly Impaired Renal Function. Sci. Rep. 2017, 7, 13781. [Google Scholar] [CrossRef]
- Koppe, L.; Fouque, D.; Soulage, C.O. Metabolic Abnormalities in Diabetes and Kidney Disease: Role of Uremic Toxins. Curr. Diabetes Rep. 2018, 18, 97. [Google Scholar] [CrossRef]
- Castillo-Rodriguez, E.; Fernandez-Prado, R.; Esteras, R.; Perez-Gomez, M.V.; Gracia-Iguacel, C.; Fernandez-Fernandez, B.; Kanbay, M.; Tejedor, A.; Lazaro, A.; Ruiz-Ortega, M.; et al. Impact of Altered Intestinal Microbiota on Chronic Kidney Disease Progression. Toxins 2018, 10, 300. [Google Scholar] [CrossRef]
- Griffin, L.E.; Djuric, Z.; Angiletta, C.J.; Mitchell, C.M.; Baugh, M.E.; Davy, K.P.; Neilson, A.P.; Grifin, L.E.; Angiletta, C.J. A Mediterranean diet does not alter plasma trimethylamine N-oxide concentrations in healthy adults at risk for colon cancer. Food Funct. 2019, 10, 2138–2147. [Google Scholar] [CrossRef]
- Jouffroy, R.; Lebreton, X.; Mansencal, N.; Anglicheau, D. Acute kidney injury during an ultra-distance race. PLoS ONE 2019, 14, e0222544. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Marker | Reference Values for Healthy Population | |||
|---|---|---|---|---|
| 21–30 Years | 31–40 Years | 41–50 Years | 51–60 Years | |
| uNGAL (ng/mL) | M: < 73.88 F: < 149.26 | M: < 87.54 F: < 153.60 | M: < 103.95 F: < 158.37 | M: < 123.70 F: < 163.62 |
| uNGAL/uCr (μg/g) | M < 125.5 F < 243.2 | M < 122.1 F < 236.5 | M < 127.6 F < 247.0 | M < 142.9 F 276.6 |
| uKIM-1 (ng/mL) | M: < 1.86 F: <1.56 | M: < 2.06 F: < 1.74 | M: < 2.28 F: < 1.94 | M: < 2.52 F: < 2.15 |
| uKIM/uCr (μg/g) both sexes | < 2.28 | < 2.14 | < 2.24 | < 2.61 |
| uCyst-C (ng/mL) | M: < 208.2 F: < 180.4 | |||
| uCyst/uCr (μg/g) both sexes | < 220 | < 191 | < 183 | < 193 |
| Variable | Result |
|---|---|
| Age (years) | 36.8 ± 8.2 |
| Weight (kg) | 74 ± 13 |
| Height (cm) | 175.9 ± 8.7 |
| BMI (kg/m2) | 23.8 ± 3.1 |
| WHR | 0.8 ± 0.05 |
| The body fat percentage (%) | 13.4 ± 4.9 |
| The mean heart rate (bpm) | 56 ± 11 |
| Duration of regular running (years) | 7.6 ± 6.1 |
| Mean training (days/week) | 5.5 ± 1.7 |
| Average training (km/month) | 146 (112–265) |
| Results of ultra-marathon | |
| 15 runners finished 100 km 2 runners finished 51 km | 13 h 33 min ± 01 h 55 min 7 h 55 min and 7 h 56 min |
| Results of 10-km race | 45 min 27 sec ± 4 min 16 sec |
| Marker | 10 km | 100 km | ||||
|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | |
| Specific gravity | 1014 ± 6 | 1015 ±6 | ns | 1015 ± 8 | 1023±7 | <0.005 |
| pH | 6.2 ±1.1 | 6.2 ±1.1 | ns | 5.84 ± 0.85 | 5.5±1.0 | ns |
| Hematuria a (n) | 0/16 | 1/16 | ns | 0/16 | 8/16 | <0.005 |
| Overt proteinuria b (n) | 0/16 | 9/16 | <0.001 | 0/16 | 8/16 | <0.005 |
| Protein in urine c (g/l) | na | 0.37 (0.25–0.43) | - | na | 0.72 (0.54–0.97) | - |
| Marker | 10 km | 100 km | ||||
|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | |
| uAlb (mg/L) | 5.7(5.0–7.6) | 41(16–126) | <0.001 | 3.0(3.0–9.5) | 57(27–306) | <0.0005 |
| ACR (mg/g) | 9(5.2–14.20) | 31(11–81) | <0.005 | 7.0(3.2–15) | 30(14–94) | <0.005 |
| uNGAL (ng/mL) | 4.9(0.8–8.3) | 19(9.0–30) | <0.005 | 4.4(0.3–11) | 30(19–63) | <0.0005 |
| uNGAL/uCr (μg/g) | 4.09(1.92–6.35) | 11.89(9.28–18.15) | <0.005 | 4.56(2.97–6.98) | 13.42(9.92–26.49) | <0.005 |
| uKIM-1 (ng/mL) | 0.44 (0.15–1.1) | 1.3(0.19–2.5) | <0.01 | 0.21(0.09–0.78) | 1.6(0.58–2.5) | <0.001 |
| uKIM/uCr (μg/g) | 0.49(0.34–0.81) | 0.72(0.34–1.45) | ns | 0.37(0.07–0.99) | 0.68(0.35-1.05) | ns |
| uCyst-C (ng/mL) | 46 (5.7–90) | 118(72–144) | <0.005 | 28(2.4–88) | 139(116–156) | <0.0005 |
| uCyst/uCr (μg/g) | 49.56 (11.49–72.03) | 68.88 (52.96–96.77) | <0.05 | 34.54 (6.15–73.38) | 67.31 (48.36–75.78) | ns (p = 0.08) |
| Markers | 10 km | 100 km | ||||
|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | |
| Creatinine a (mg/dL) | 0.79 ± 0.14 | 0.99 ± 0.18 | <0.001 | 0.85 ± 0.13 | 1.19 ± 0.26 | <0.001 |
| eGFR CKD-EPI (mL/min/1.73m2) | 112 ± 13 | 95 ± 15 | <0.001 | 107 ± 13 | 78 ± 15 | <0.001 |
| Urea a(mg/dL) | 32(31–39) | 33 (32–42) | <0.005 | 34(30–37) | 66 (49–70) | <0.001 |
| FeUrea (%) | 44 ± 12 | 3314 | <0.01 | 49 ± 12 | 29 ± 11 | <0.001 |
| Uric acid a(mg/dL) | 5.03 ± 0.99 | 5.65 ± 0.06 | <0.001 | 4.22 ± 0.76 | 5.6 ± 1.2 | <0.001 |
| FeUA (%) | 6.0 ± 1.6 | 5.46 ± 1.95 | ns | 5.59 ± 1.6 | 6.1 ± 2.3 | ns |
| Markers | 10 km | 100 km | ||||
|---|---|---|---|---|---|---|
| Before | After | p | Before | After | p | |
| ADMA (ng/mL) | 133 ± 25 | 137 ± 17 | ns | 136 ± 16 | 123 ± 24 | ns |
| SDMA (ng/mL) | 287 ± 51 | 312 ± 38 | <0.01 | 227 ± 41 | 369 ± 79 | <0.001 |
| TMAO (ng/mL) | 329 (212–502) | 429(243–520) | ns (p = 0.07) | 306 (225–447) | 513 (262–751) | ns |
| Subjects | AKI Stage 1 a | AKI stage 2 a | uNGAL above ref. value b | uKIM-1 above ref. value b | uCyst-C above ref. value b | uNGAL/uCr above ref. value b | uKIM/uCr above ref. value b | uCyst/uCr above ref. value b |
|---|---|---|---|---|---|---|---|---|
| 10-km run | 3 | 0 | 1 | 6 | 1 | 0 | 1 | 1 |
| 100-km run | 7 | 1 | 1 | 6 | 0 | 0 | 0 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wołyniec, W.; Kasprowicz, K.; Giebułtowicz, J.; Korytowska, N.; Zorena, K.; Bartoszewicz, M.; Rita-Tkachenko, P.; Renke, M.; Ratkowski, W. Changes in Water Soluble Uremic Toxins and Urinary Acute Kidney Injury Biomarkers After 10- and 100-km Runs. Int. J. Environ. Res. Public Health 2019, 16, 4153. https://doi.org/10.3390/ijerph16214153
Wołyniec W, Kasprowicz K, Giebułtowicz J, Korytowska N, Zorena K, Bartoszewicz M, Rita-Tkachenko P, Renke M, Ratkowski W. Changes in Water Soluble Uremic Toxins and Urinary Acute Kidney Injury Biomarkers After 10- and 100-km Runs. International Journal of Environmental Research and Public Health. 2019; 16(21):4153. https://doi.org/10.3390/ijerph16214153
Chicago/Turabian StyleWołyniec, Wojciech, Katarzyna Kasprowicz, Joanna Giebułtowicz, Natalia Korytowska, Katarzyna Zorena, Maria Bartoszewicz, Patrycja Rita-Tkachenko, Marcin Renke, and Wojciech Ratkowski. 2019. "Changes in Water Soluble Uremic Toxins and Urinary Acute Kidney Injury Biomarkers After 10- and 100-km Runs" International Journal of Environmental Research and Public Health 16, no. 21: 4153. https://doi.org/10.3390/ijerph16214153