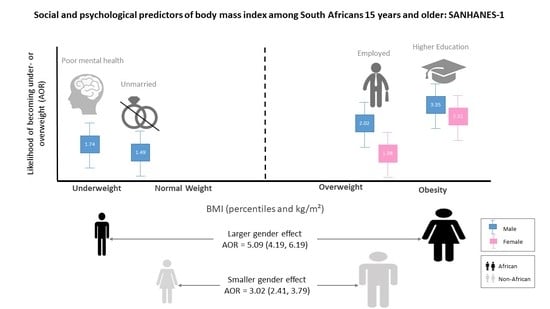
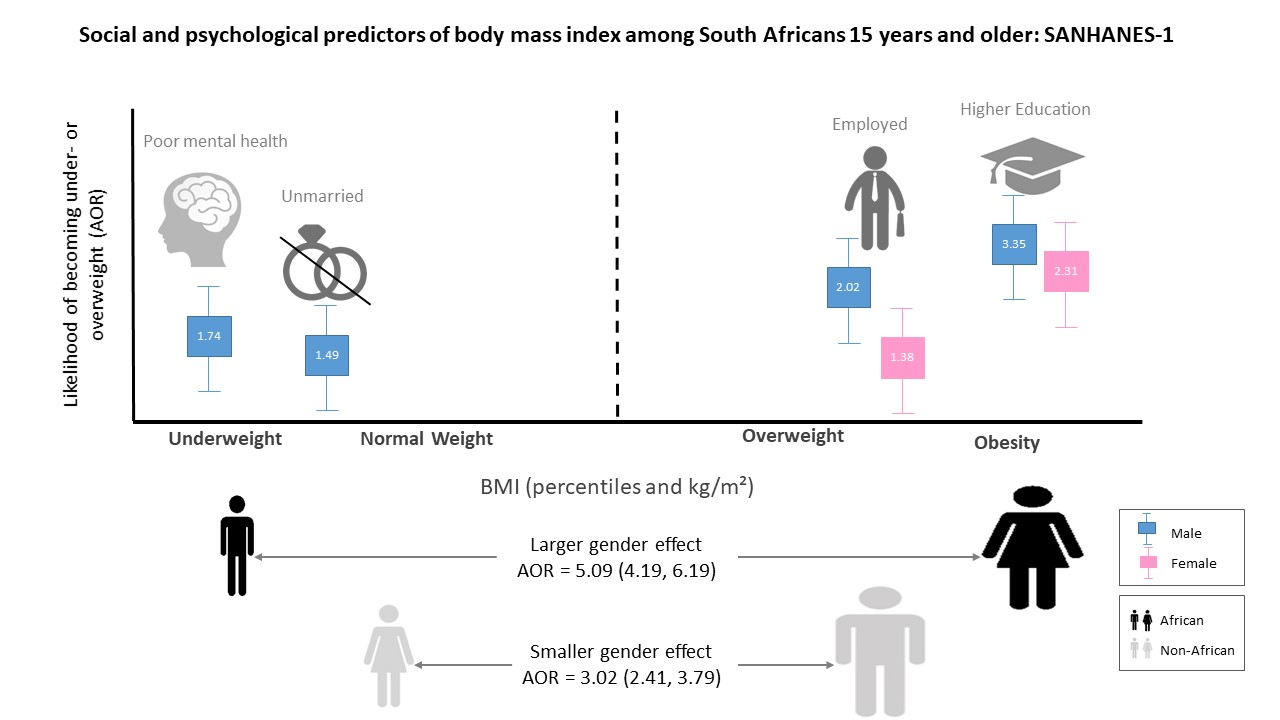
Social and Psychological Predictors of Body Mass Index among South Africans 15 Years and Older: SANHANES-1

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Measures
2.3. Statistical Analyses
3. Results
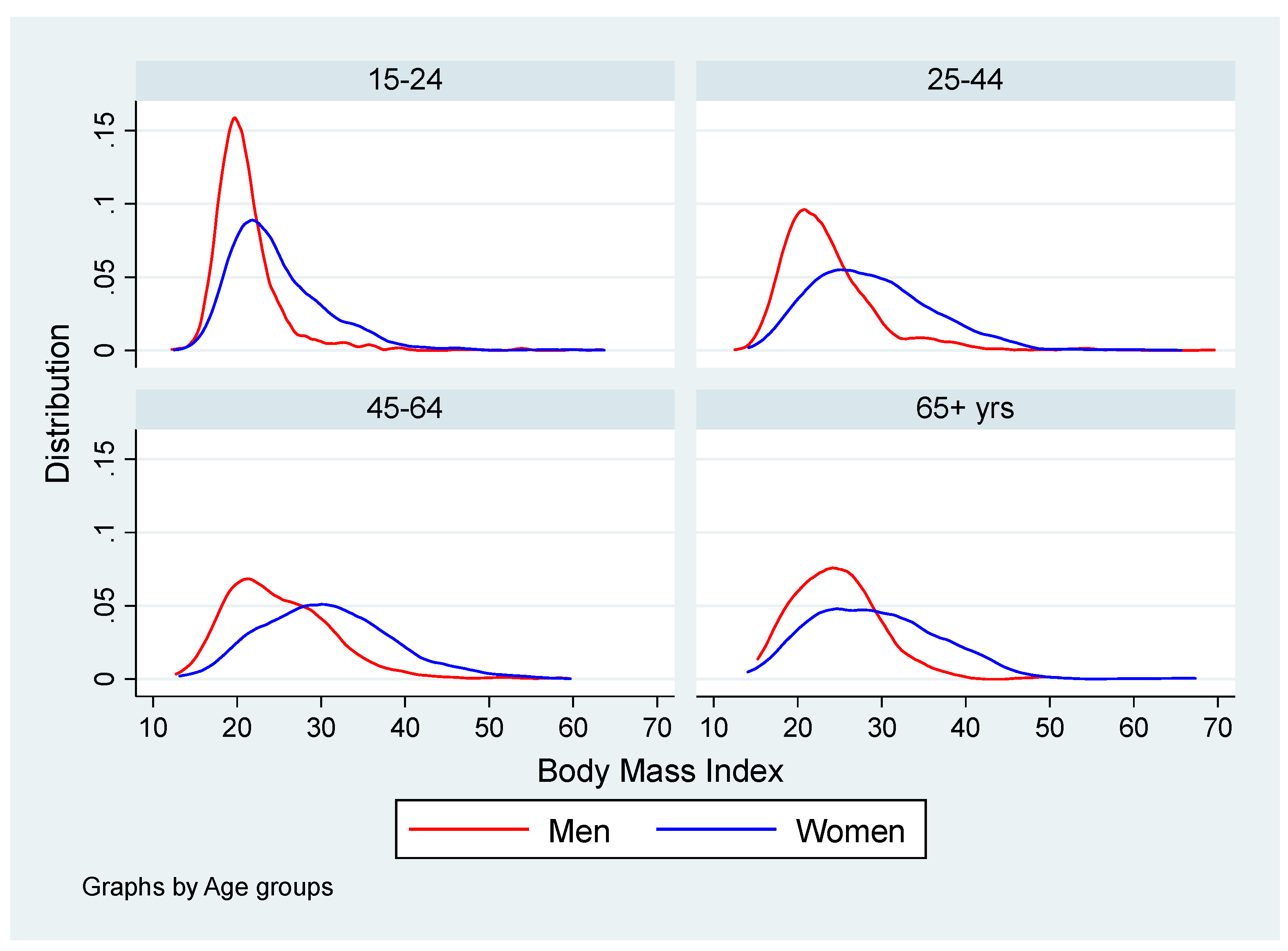
3.1. Body Mass Index of Participants by Age and Gender
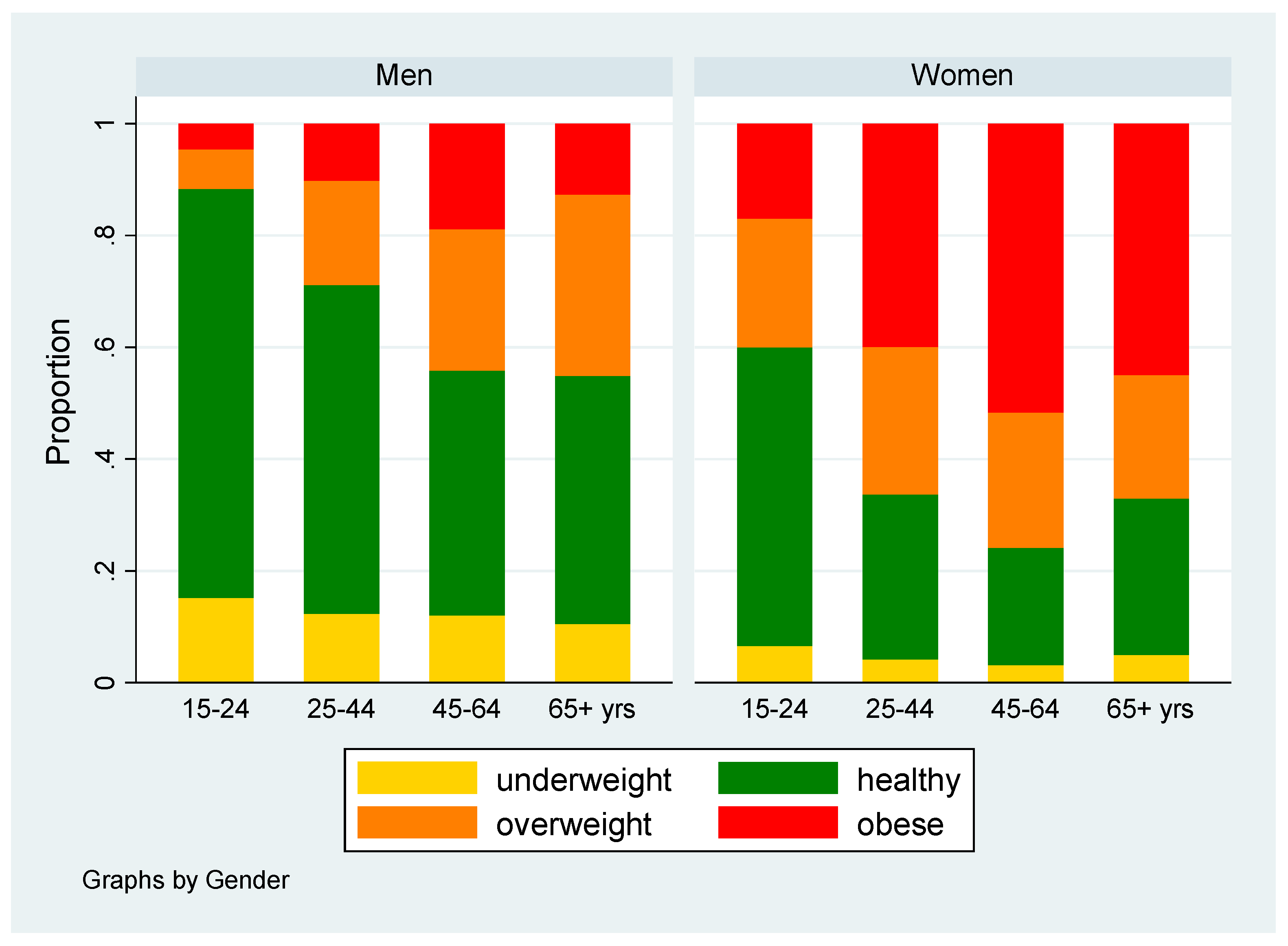
3.2. Proportion of Underweight, Healthy Weight, Overweight and Obesity Participants by Socio-demography
3.3. Multinomial Logistic Regression Analysis of BMI Categories Versus Exposures Using Healthy Weight as the Baseline
3.4. Restricted Analyses of Social Patterning of Underweight, Overweight and Obesity Versus Household Income
3.5. The Statistical Analyses Using Binary Logistic Regression Models Where BMI Was Entered as A Dichotomized Variable
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Department of Health, South Africa Demographic and Health Survey: Final Report. 1998. Available online: https://www.dhsprogram.com/pubs/pdf/FR131/FR131.pdf (accessed on 24 September 2019).
- Department of Health, Medical Research Council, OrcMacro South Africa Demographic and Health Survey 2003. Available online: https://dhsprogram.com/pubs/pdf/FR206/FR206.pdf (accessed on 24 September 2019).
- South Africa Demographic Health Survey SADHS 2016. Available online: https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf. (accessed on 24 September 2019).
- Shisana, O.; Labadarios, D.; Rehle, T.; Simbayi, L.; Zuma, K.; Dhansay, A.; Reddy, P.; Parker, W.; Hoosain, E.; Naidoo, P.; et al. The South African National Health and Nutrition Examination Survey SANHANES-1 2013. Available online: http://www.hsrc.ac.za/uploads/pageNews/72/SANHANES-launch%20edition%20(online%20version).pdf (accessed on 24 September 2019).
- Rossouw, H.A.; Grant, C.C.; Viljoen, M. Overweight and obesity in children and adolescents: The South African problem. South Afr. J. Sci. 2012, 108, 31–37. [Google Scholar] [CrossRef]
- Cois, A.; Day, C. Obesity trends and risk factors in the South African adult population. BMC Obes. 2015, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.G.; Crowther, N.J.; Gómez-Olivé, F.X.; Kabudula, C.; Kahn, K.; Mhembere, M.; Myakayaka, Z.; Tollman, S.; Wade, A.N.; as members of AWI-Gen and the H3Africa Consortium. Sociodemographic, socioeconomic, clinical and behavioural predictors of body mass index vary by sex in rural South African adults-findings from the AWI-Gen study. Glob. Health Action 2018, 11, 1549436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartorius, B.; Veerman, L.J.; Manyema, M.; Chola, L.; Hofman, K. Determinants of obesity and associated population attributability, South Africa: Empirical evidence from a national panel survey, 2008–2012. PloS One 2015, 10, e0130218. [Google Scholar] [CrossRef] [PubMed]
- Nienaber-Rousseau, C.; Sotunde, O.F.; Ukegbu, P.O.; Myburgh, P.H.; Wright, H.H.; Havemann-Nel, L.; Moss, S.J.; Kruger, I.M.; Kruger, H.S. Socio-Demographic and Lifestyle Factors Predict 5-Year Changes in Adiposity among a Group of Black South African Adults. Int. J. Environ. Res. Public. Health 2017, 14, 1089. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Hoyo, C.; Østbye, T.; Hughes, G.; Schwartz, D.; Tsolekile, L.; Zulu, J.; Puoane, T. Determinants of obesity in an urban township of South Africa. South Afr. J. Clin. Nutr. 2008, 21, 315–320. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K.; Phaswana-Mafuya, N. Prevalence and correlates of physical activity among female and male adolescents and adults in South Africa. Gend. Behav. 2018, 16, 11193–11206. [Google Scholar]
- Micklesfield, L.K.; Lambert, E.V.; Hume, D.J.; Chantler, S.; Pienaar, P.R.; Dickie, K.; Goedecke, J.H.; Puoane, T. Socio-cultural, environmental and behavioural determinants of obesity in black South African women. Cardiovasc. J. Afr. 2013, 24, 369. [Google Scholar] [CrossRef]
- Yako, Y.Y.; Fanampe, B.L.; Hassan, M.S.; Erasmus, R.T.; Van der Merwe, L.; Van Rensburg, S.J.; Matsha, T.E. Association of cocaine-and amphetamine-related transcript, leptin and leptin receptor gene polymorphisms with anthropometric obesity phenotype indicators in South African learners. Lifestyle Genom. 2011, 4, 210–221. [Google Scholar] [CrossRef]
- Yako, Y.Y.; Echouffo-Tcheugui, J.B.; Balti, E.V.; Matsha, T.E.; Sobngwi, E.; Erasmus, R.T.; Kengne, A.P. Genetic association studies of obesity in A frica: A systematic review. Obes. Rev. 2015, 16, 259–272. [Google Scholar] [CrossRef]
- Pillay, V.; Crowther, N.J.; Ramsay, M.; Smith, G.D.; Norris, S.A.; Lombard, Z. Exploring genetic markers of adult obesity risk in black adolescent South Africans—the Birth to Twenty Cohort. Nutr. Diabetes 2015, 5, e157. [Google Scholar] [CrossRef] [PubMed]
- Dickie, K.; Micklesfield, L.K.; Chantler, S.; Lambert, E.V.; Goedecke, J.H. Meeting physical activity guidelines is associated with reduced risk for cardiovascular disease in black South African women; a 5.5-year follow-up study. BMC Public Health 2014, 14, 498. [Google Scholar] [CrossRef] [PubMed]
- Mlambo, V. An overview of rural-urban migration in South Africa: its causes and implications. Arch. Bus. Res. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Nnyepi, M.S.; Gwisai, N.; Lekgoa, M.; Seru, T. Evidence of nutrition transition in Southern Africa. Proc. Nutr. Soc. 2015, 74, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, A.; Kumar, K.; Singh, A. Association between obesity and selected morbidities: A study of BRICS countries. PloS One 2014, 9, e94433. [Google Scholar] [CrossRef]
- Maimela, E.; Alberts, M.; Modjadji, S.E.; Choma, S.S.; Dikotope, S.A.; Ntuli, T.S.; Van Geertruyden, J.-P. The prevalence and determinants of chronic non-communicable disease risk factors amongst adults in the Dikgale health demographic and surveillance system (HDSS) site, Limpopo Province of South Africa. PLoS One 2016, 11, e0147926. [Google Scholar] [CrossRef]
- Joubert, J.; Norman, R.; Bradshaw, D.; Goedecke, J.H.; Steyn, N.P.; Puoane, T. Estimating the burden of disease attributable to excess body weight in South Africa in 2000. S. Afr. Med. J. 2007, 97, 683–690. [Google Scholar]
- Patel, S.A.; Ali, M.K.; Alam, D.; Yan, L.L.; Levitt, N.S.; Bernabe-Ortiz, A.; Checkley, W.; Wu, Y.; Irazola, V.; Gutierrez, L. Obesity and its relation with diabetes and hypertension: A cross-sectional study across 4 geographical regions. Glob. Heart 2016, 11, 71–79. [Google Scholar] [CrossRef]
- Marmot, M. The status syndrome: How social status affects our health and longevity. BMJ 2004, 329, 408. [Google Scholar]
- Institute of Medicine (US) Committee on Assessing Interactions Among Social, Behavioral, and Genetic Factors in Health. Genes, Behavior, and the Social Environment: Moving Beyond the Nature/Nurture Debate; Hernandez, L.M., Blazer, D.G., Eds.; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Ajayi, I.O.; Adebamowo, C.; Adami, H.-O.; Dalal, S.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Njelekela, M.; Nankya-Mutyoba, J.; Chiwanga, F.S. Urban–rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: A multi-country cross-sectional study. BMC Public Health 2016, 16, 1126. [Google Scholar] [CrossRef]
- Munthali, R.J.; Manyema, M.; Said-Mohamed, R.; Kagura, J.; Tollman, S.; Kahn, K.; Gómez-Olivé, F.X.; Micklesfield, L.K.; Dunger, D.; Norris, S.A. Body composition and physical activity as mediators in the relationship between socioeconomic status and blood pressure in young South African women: A structural equation model analysis. BMJ Open 2018, 8, e023404. [Google Scholar] [CrossRef] [PubMed]
- Fokeena, W.B.; Jeewon, R. Is there an association between socioeconomic status and body mass index among adolescents in mauritius? Sci. World J. 2012, 2012, 750659. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Sharma, S.V.; Park, S.K. Association between socioeconomic status and obesity in adults: Evidence from the 2001 to 2009 Korea national health and nutrition examination survey. J. Prev. Med. Pub. Health 2014, 47, 94. [Google Scholar] [CrossRef] [PubMed]
- Lipowicz, A.; Gronkiewicz, S.; Malina, R.M. Body mass index, overweight and obesity in married and never married men and women in Poland. Am. J. Hum. Biol. Off. J. Hum. Biol. Assoc. 2002, 14, 468–475. [Google Scholar] [CrossRef]
- Tzotzas, T.; Vlahavas, G.; Papadopoulou, S.K.; Kapantais, E.; Kaklamanou, D.; Hassapidou, M. Marital status and educational level associated to obesity in Greek adults: data from the National Epidemiological Survey. BMC Public Health 2010, 10, 732. [Google Scholar] [CrossRef]
- Klos, L.A.; Sobal, J. Marital status and body weight, weight perception, and weight management among US adults. Eat Behav. 2013, 14, 500–507. [Google Scholar] [CrossRef]
- Janghorbani, M.; Amini, M.; Rezvanian, H.; Gouya, M.M.; Delavari, A.R.; Alikhani, S.; Mahdavi, A. Association of body mass index and abdominal obesity with marital status in adults. Arch. Iran. Med. 2008, 11, 274–281. [Google Scholar]
- Averett, S.L.; Sikora, A.; Argys, L.M. For better or worse: relationship status and body mass index. Econ. Hum. Biol. 2008, 6, 330–349. [Google Scholar] [CrossRef]
- Statistics South Africa. Subjective Poverty in South Africa: Findings from the Living Conditions Surveys 2008/2009; Statistics South Africa: Pretoria, ZA, South Africa, 2012. [Google Scholar]
- The Experience of Poverty in South Africa: A summary of Afrobarometer Indicators, 2000–2011. Available online: http://africabusiness.com/wp-content/uploads/2013/02/SAF_R5.Poverty.Indicators_22jan13_final.pdf (accessed on 24 September 2019).
- Statistics South Africa. National Poverty Lines 2018; Statistics South Africa: Pretoria, ZA, South Africa, 2018; pp. 1–10. [Google Scholar]
- World Health Organization. Nutrition for Health and Development. A global agenda for combating malnutrition. Nutrition for Health and Development (NHD): Sustainable Development and Healthy Environments (SDE); World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- FAO, IFAD, UNICEF, WFP and WHO. The State of Food Security in the Wold 2017; FAO, IFAD, UNICEF, WFP and WHO: Rome, Italy, 2017. [Google Scholar]
- Mchiza, Z.J.; Parker, W.; Makoae, M.; Sewpaul, R.; Kupamupindi, T.; Labadarios, D. Body image and weight control in South Africans 15 years or older: SANHANES-1. BMC Public Health 2015, 15, 992. [Google Scholar] [CrossRef]
- Brandheim, S.; Rantakeisu, U.; Starrin, B. BMI and psychological distress in 68, 000 Swedish adults: A weak association when controlling for an age-gender combination. BMC Public Health 2013, 13, 68. [Google Scholar] [CrossRef]
- Kelly, S.J.; Daniel, M.; Dal Grande, E.; Taylor, A. Mental ill-health across the continuum of body mass index. BMC Public Health 2011, 11, 765. [Google Scholar] [CrossRef] [PubMed]
- Martínez, E.; Gutiérrez-Bedmar, M.; García-Rodríguez, A.; Mariscal, A.; Muñoz-Bravo, C.; Navajas, J. Weight status and psychological distress in a Mediterranean Spanish population: A symmetric U-shaped relationship. Nutr. 2014, 6, 1662–1677. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; Koehn, S.; Happell, B.; Dwyer, T.; Moxham, L. Implications of excess weight on mental wellbeing. Aust. Health Rev. 2010, 34, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kim, J.J.; Kim, M.Y.; Kim, S.K.; Roh, S.; Seo, J.S. A U-shaped association between body mass index and psychological distress on the multiphasic personality inventory: retrospective cross-sectional analysis of 19-year-old men in Korea. J. Korean Med. Sci. 2015, 30, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Division of Nutrition, Physical Activity, Overweight and Obesity. Available online: https://www.cdc.gov/nccdphp/dnpao/index.html (accessed on 21 August 2019).
- Census 2011: Statistical release-P0301.4/Statistics South Africa. Pretoria. 2012. Available online: http://www.statssa.gov.za/publications/P03014/P030142011.pdf (accessed on 24 September 2019).
- Andrews, G.; Slade, T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Aust. N. Z. J. Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.D. Biochemical Assessment of Nutritional Status; Lee, R.D., Nieman, D.C., Eds.; Nutritional Assessment: Ney York, NY, USA, 2013. [Google Scholar]
- Dinour, L.; Leung, M.M.; Tripicchio, G.; Khan, S.; Yeh, M.-C. The Association between Marital Transitions, Body Mass Index, and Weight: A Review of the Literature. J. Obes. 2012, 2012, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puoane, T.; Matwa, P.; Bradley, H.; Hughes, G. Socio-cultural factors influencing food consumption patterns in the black African population in an urban township in South Africa. Hum. Ecol. 2006, 14, 89–93. [Google Scholar]
- Puoane, T.; Fourie, J.M.; Shapiro, M.; Rosling, L.; Tshaka, N.C.; Oelefse, A. ‘Big is beautiful’—An exploration with urban black community health workers in a South African township. SAJCN 2005, 18, 6–15. [Google Scholar] [CrossRef]
- Sobal, J.; Rauschenbach, B.; Frongillo, E.A. Marital status changes and body weight changes: A US longitudinal analysis. Soc. Sci. Med. 2003, 56, 1543–1555. [Google Scholar] [CrossRef]
- Eng, P.M.; Kawachi, I.; Fitzmaurice, G.; Rimm, E.B. Effects of marital transitions on changes in dietary and other health behaviors in US male health professionals. J. Epidemiol. Community Health 2005, 59, 56–62. [Google Scholar] [CrossRef]
- Lee, S.; Cho, E.; Grodstein, F.; Kawachi, I.; Hu, F.B.; Colditz, G.A. Effects of marital transitions on changes in dietary and other health behaviors in US women. Int. J. Epidemiol 2004, 34, 69–78. [Google Scholar] [CrossRef]
- OECD Organisation for Economic Co-operation and Development Economic Surveys: South Africa 2017. Available online: https://www.oecd.org/eco/surveys/2017-OECD-Economic-Survey-South-Africa-overview-2017.pdf (accessed on 24 September 2019).
- Wilcox, S.; Evenson, K.R.; Aragaki, A.; Wassertheil-Smoller, S.; Mouton, C.P.; Loevinger, B.L. The effects of widowhood on physical and mental health, health behaviors, and health outcomes: The Women’s Health Initiative. Health Psychol. 2003, 22, 513. [Google Scholar] [CrossRef]
- Shahar, D.R.; Schultz, R.; Shahar, A.; Wing, R.R. The effect of widowhood on weight change, dietary intake, and eating behavior in the elderly population. J. Aging Health 2001, 13, 186–199. [Google Scholar] [CrossRef]
- Statistics South Africa. Quarterly Labour Force Survey; Statistics South Africa: Pretoria, ZA, South Africa, 2019. [Google Scholar]
- NCES The Condition of Education – Glossary. Available online: https://nces.ed.gov/programs/coe/glossary.asp (accessed on 21 August 2019).
- Lawlor, D.A.; Smith, G.D.; O’Callaghan, M.; Alati, R.; Mamun, A.A.; Williams, G.M.; Najman, J.M. Epidemiologic Evidence for the Fetal Overnutrition Hypothesis: Findings from the Mater-University Study of Pregnancy and Its Outcomes. Am. J. Epidemiol. 2007, 165, 418–424. [Google Scholar] [CrossRef]
- Barrera, C.; Valenzuela, R.; Chamorro, R.; Bascuñán, K.; Sandoval, J.; Sabag, N.; Valenzuela, F.; Valencia, M.P.; Puigrredon, C.; Valenzuela, A. The Impact of Maternal Diet during Pregnancy and Lactation on the Fatty Acid Composition of Erythrocytes and Breast Milk of Chilean Women. Nutr. 2018, 10, 839. [Google Scholar] [CrossRef]
- Kruger, H.S.; Puoane, T.; Senekal, M.; van der Merwe, M.T. Obesity in South Africa: Challenges for government and health professionals. Public Health Nutrition 2005, 8, 491–500. [Google Scholar] [CrossRef]
- Groenewald, P.; Vos, T.; Norman, R.; Laubscher, R.; van Walbeek, C.; Saloojee, Y.; Sitas, F.; Bradshaw, D.; South African Comparative Risk Assessment Collaborating Group. Estimating the burden of disease attributable to smoking in South Africa in 2000. S Afr Med J. 2007, 97, 674–681. [Google Scholar]
- Sturm, R.; An, R.; Maroba, J.; Patel, D. The effects of obesity, smoking, and excessive alcohol intake on healthcare expenditure in a comprehensive medical scheme. S. Afr. Med. J. 2013, 103, 840–844. [Google Scholar] [CrossRef]
- Hernandez-Rodas, M.; Valenzuela, R.; Videla, L. Relevant Aspects of Nutritional and Dietary Interventions in Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [Green Version]
- Mchiza, Z.; Temple, N.J.; Steyn, N.P.; Abrahams, Z.; Clayford, M. Content analysis of television food advertisements aimed at adults and children in South Africa. Public Health Nutr. 2013, 16, 2213–2220. [Google Scholar] [CrossRef] [Green Version]
- Abrahams, Z.; Temple, N.; Mchiza, Z.; Steyn, N.P. A Study of Food Advertising in Magazines in South Africa. J. Hunger Environ. Nutr. 2016, 12, 429–441. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Age Group (Years) | Underweight % (n) | Healthy BMI % (n) | Overweight % (n) | Obesity % (n) | Total N |
|---|---|---|---|---|---|
| 15–24 | 9.9 (174) | 61.1 (1069) | 16.9 (295) | 12.2 (213) | 1 751 |
| 25–44 | 6.8 (141) | 38.9 (806) | 23.9 (494) | 30.4 (629) | 2 070 |
| 45–64 | 6.3 (119) | 29.2 (549) | 24.6 (462) | 39.9 (751) | 1 881 |
| 65+ | 6.8 (49) | 33.4 (241) | 25.5 (184) | 34.4 (248) | 722 |
| Total | 7.5 (483) | 41.5 (2665) | 22.3 (1435) | 28.7 (1841) | 6 424 |
| Socio-Demographic Factors | Men | Underweight Proportion (95% CI) | Healthy Weight Proportion (95% CI) | Overweight Proportion (95% CI) | Obese Proportion (95% CI) |
|---|---|---|---|---|---|
| N | |||||
| Ethnicity: | |||||
| African | 1109 | 11.9 (10.1, 13.9) | 57.7 (54.9, 60.5) | 18.7 (16.6, 21.1) | 11.6 (9.8, 13.6) |
| Non-African | 546 | 13.1 (10.4, 16.2) | 50.9 (46.7, 55.0) | 23.1 (19.8, 26.8) | 12.9 (10.4, 15.9) |
| Education: | |||||
| No education | 155 | 26.9 (18.4, 37.5) | 38.1 (29.2, 48.0) | 27.1 (20.6, 34.7) | 7.8 (4.9, 12.2) |
| Grade 1–7 | 420 | 16.4 (13.0, 20.6) | 57.9 (52.8, 62.9) | 16.5 (13.5, 20.1) | 9.1 (6.4, 12.7) |
| Grade 8–11 | 664 | 12.0 (9.7, 14.8) | 57.0 (53.2, 60.8) | 20.3 (17.2, 23.7) | 10.6 (8.4, 13.4) |
| Grade 12 | 305 | 7.0 (4.0, 12.0) | 52.5 (44.9, 60.0) | 20.7 (15.1, 27.7) | 19.7 (14.1, 26.9) |
| Higher | 111 | 1.9 (0.5, 7.1) | 39.4 (30.9, 48.5) | 36.5 (28.2, 45.8) | 22.2 (15.7, 30.5) |
| Employment: | |||||
| Not employed | 1087 | 15.8 (13.7, 18.2) | 56.5 (53.5, 59.5) | 18.4 (16.2, 20.9) | 9.3 (7.6, 11.2) |
| Employed | 568 | 4.6 (3.3, 6.4) | 58.4 (53.8, 62.9) | 19.7 (16.3, 23.6) | 17.3 (13.7, 21.5) |
| Marital status: | |||||
| Married/cohabiting | 763 | 10.4 (6.7, 15.9) | 49.5 (43.2, 55.8) | 24.5 (20.1, 29.5) | 15.6 (11.7, 20.6) |
| Never married | 797 | 17.2 (13.7, 21.4) | 60.7 (55.8, 65.4) | 14.4 (11.1, 18.5) | 7.6 (5.3, 10.9) |
| Divorced/separated/widowed | 95 | 16.6 (8.0, 31.3) | 56.7 (44.5, 68.1) | 18.6 (10.9, 30.0) | 8.1 (3.1, 19.3) |
| Poor mental health: | |||||
| No | 1388 | 11.1 (9.6, 12.9) | 56.1 (53.6, 58.7) | 20.6 (18.6, 22.8) | 12.1 (10.5, 13.9) |
| Yes | 267 | 18.3 (13.9, 23.8) | 55.0 (49.0, 60.8) | 16.0 (12.4, 20.5) | 10.6 (7.7, 14.5) |
| Household Income *: | |||||
| No income | 363 | 14.7 (10.8, 20.0) | 56.4 (49.8, 62.7) | 14.0 (10.5, 18.5) | 14.8 (10.2, 21.0) |
| Low income | 589 | 13.2 (10.5, 16.4) | 58.0 (53.8, 62.0) | 19.3 (16.4, 22.6) | 9.5 (7.3, 12.2) |
| Medium/high income | 188 | 2.7 (1.1, 6.6) | 46.1 (38.0, 54.3) | 27.6 (20.7, 35.8) | 23.6 (17.4, 31.1) |
| Socio-Demographic Factors | Women | Underweight Proportion (95% CI) | Healthy Weight Proportion (95% CI) | Overweight Proportion (95% CI) | Obese Proportion (95% CI) |
|---|---|---|---|---|---|
| N | |||||
| Ethnicity: | |||||
| African | 2120 | 4.2 (3.5, 5.2) | 31.3 (29.4, 33.2) | 23.3 (21.5, 25.1) | 41.1 (39.2, 43.2) |
| Non-African | 984 | 4.8 (3.6, 6.3) | 34.2 (31.4, 37.2) | 26.6 (23.9, 29.5) | 34.3 (31.4, 37.2) |
| Education: | |||||
| No education | 350 | 8.3 (4.6, 14.6) | 36.7 (29.3, 44.9) | 21.4 (16.4, 27.4) | 33.5 (26.6, 41.2) |
| Grade 1–7 | 760 | 6.7 (4.8, 9.2) | 33.3 (29.5, 37.3) | 23.7 (20.5, 27.3) | 36.2 (32.6, 40.0) |
| Grade 8–11 | 1185 | 2.8 (2.0, 3.9) | 27.4 (25.0, 30.0) | 25.9 (23.3, 28.7) | 43.9 (41.0, 46.8) |
| Grade 12 | 631 | 3.2 (2.1, 4.8) | 36.1 (31.3, 41.2) | 22.8 (19.0, 27.1) | 37.9 (32.9, 43.1) |
| Higher | 178 | 2.3 (0.8, 6.2) | 24.2 (18.5, 30.9) | 22.7 (17.0, 29.6) | 50.9 (43.8, 57.8) |
| Employment: | |||||
| Not employed | 2406 | 4.6 (3.8, 5.5) | 33.6 (31.8, 35.5) | 23.4 (21.7, 25.2) | 38.3 (36.4, 40.2) |
| Employed | 698 | 4.4 (2.0, 9.3) | 22.1 (18.2, 26.5) | 29.2 (23.5, 35.8) | 44.2 (39.3, 49.2) |
| Marital status: | |||||
| Married/cohabiting | 1244 | 3.8 (2.6, 5.5) | 32.6 (30.0, 35.7) | 24.4 (21.9, 27.2) | 39.1 (36.4, 41.9) |
| Never married | 1407 | 5.1 (3.9, 6.6) | 35.5 (32.7, 38.4) | 22.5 (20.0, 25.1) | 36.9 (34.0, 40.0) |
| Divorced/separated/widowed | 453 | 2.3 (0.9, 5.6) | 39.0 (28.6, 50.5) | 22.3 (13.5, 34.6) | 36.4 (31.3, 41.7) |
| Poor mental health: | |||||
| No | 2425 | 4.0 (3.3, 4.8) | 32.9 (31.1, 34.7) | 24.3 (22.7, 26.1) | 38.7 (36.9, 40.6) |
| Yes | 679 | 6.1 (4.4, 8.3) | 30.0 (26.6, 33.6) | 24.8 (21.6, 28.4) | 39.1 (35.6, 42.6) |
| Household Income *: | |||||
| No income | 817 | 4.3 (3.1, 5.8) | 30.3 (26.5, 34.3) | 21.9 (18.8, 25.4) | 43.5 (39.3, 47.8) |
| Low income | 1235 | 4.4 (3.4, 5.9) | 29.0 (26.4, 31.7) | 23.9 (21.5, 26.5) | 42.6 (39.9, 45.4) |
| Medium/high income | 166 | 2.6 (0.8, 7.9) | 23.2 (15.4, 33.5) | 28.9 (20.6, 38.9) | 45.2 (38.4, 52.2) |
| Socio-Demographic Factors | Men | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: | Model 2: | |||||||
| Underweight | Healthy Weight | Overweight | Obesity | Underweight | Healthy Weight | Overweight | Obesity | |
| Age-adjusted OR (95% CI) | Reference (p-value) | Age-adjusted OR (95% CI) | Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | Reference (p-value) | Fully Adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | |
| Ethnicity: | ||||||||
| African | 1 | 1 (0.066) | 1 | 1 | 1 | 1 (0.027) | 1 | 1 |
| Non-African | 1.25 (0.90, 1.73) | 1.40 (1.07, 1.84) | 1.28 (0.92, 1.77) | 1.66 (1.17, 2.34) | 1.26 (0.95, 1.68) | 1.11 (0.78, 1.57) | ||
| Education: | ||||||||
| No-education | 1 | 1 (< 0.001) | 1 | 1 | 1 | 1 (< 0.001) | 1 | 1 |
| Grade 1–7 | 0.73 (0.43, 1.23) | 1.08 (0.66, 1.77) | 0.75 (0.41, 1.39) | 0.74 (0.43, 1.26) | 1.07 (0.65, 1.77) | 0.77 (0.41, 1.43) | ||
| Grade 8–11 | 0.47 (0.27, 0.81) | 1.32 (0.80, 2.16) | 1.06 (0.58, 1.92) | 0.45 (0.26, 0.78) | 1.20 (0.72, 1.99) | 0.98 (0.53, 1.81) | ||
| Grade 12 | 0.24 (0.12, 0.48) | 1.57 (0.89, 2.76) | 2.13 (1.11, 4.09) | 0.24 (0.12, 0.49) | 1.44 (0.81, 2.58) | 1.92 (0.98, 3.76) | ||
| Higher | 0.12 (0.03, 0.53) | 3.54 (1.88, 6.68) | 3.35 (1.61, 6.96) | 0.14 (0.03, 0.62) | 3.13 (1.64, 5.98) | 2.73 (1.29, 5.79) | ||
| Employment: | ||||||||
| Not employed | 1 | 1 (< 0.001) | 1 | 1 | 1 | 1 (< 0.001) | 1 | 1 |
| Employed | 0.39 (0.25, 0.59) | 1.35 (1.00, 1.81) | 2.02 (1.43, 2.84) | 0.44 (0.29, 0.68) | 1.10 (0.81, 1.50) | 1.63 (1.14, 2.35) | ||
| Marital status: | ||||||||
| Married/cohabiting | 1 | 1 (< 0.001) | 1 | 1 | 1 | 1 (< 0.001) | 1 | 1 |
| Never married | 1.49 (0.98, 2.24) | 0.46 (0.32, 0.65) | 0.37 (0.24, 0.57) | 1.27 (0.83, 1.95) | 0.49 (0.34, 0.70) | 0.42 (0.27, 0.66) | ||
| Divorce/separated/widowed | 1.40 (0.72, 2.72) | 0.66 (0.38, 1.13) | 0.46 (0.22, 0.98) | 1.34 (0.68, 2.64) | 0.67 (0.39, 1.16) | 0.52 (0.24, 1.12) | ||
| Poor mental health: | ||||||||
| No | 1 | 1 (0.014) | 1 | 1 | 1 | 1 (0.089) | 1 | 1 |
| Yes | 1.74 (1.19, 2.55) | 0.85 (0.59, 1.21) | 0.98 (0.64, 1.50) | 1.63 (1.09, 2.42) | 0.96 (0.66, 1.40) | 1.21 (0.78, 1.90) | ||
| Socio-Demographic Factors | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: | Model 2: | |||||||
| Underweight | Healthy Weight | Overweight | Obesity | Underweight | Healthy Weight | Overweight | Obesity | |
| Age-adjusted OR (95% CI) | Reference (p-value) | Age-adjusted OR (95% CI) | Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | Reference (p-value) | Fully Adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | |
| Ethnicity: | ||||||||
| African | 1 | 1 (0.002) | 1 | 1 | 1 | 1 (< 0.001) | 1 | 1 |
| Non-African | 1.02 (0.70, 1.50) | 1.03 (0.84, 1.26) | 0.74 (0.61, 0.89) | 1.26 (0.85, 1.87) | 0.93 (0.76, 1.15) | 0.64 (0.52, 0.78) | ||
| Education: | ||||||||
| No-education | 1 | 1 (< 0.001) | 1 | 1 | 1 | 1 (< 0.001) | 1 | 1 |
| Grade 1–7 | 0.73 (0.41, 1.32) | 1.28 (0.88, 1.86) | 1.26 (0.91, 1.74) | 0.69 (0.38, 1.27) | 1.28 (0.88, 1.87) | 1.35 (0.97, 1.88) | ||
| Grade 8–11 | 0.34 (0.18, 0.66) | 1.82 (1.24, 2.67) | 2.15 (1.54, 3.00) | 0.32 (0.16, 0.62) | 1.82 (1.24, 2.69) | 2.43 (1.72, 3.42) | ||
| Grade 12 | 0.36 (0.18, 0.72) | 1.27 (0.84, 1.91) | 1.36 (0.95, 1.96) | 0.33 (0.16, 0.68) | 1.24 (0.82, 1.88) | 1.51 (1.04, 2.19) | ||
| Higher | 0.34 (0.11, 1.08) | 1.55 (0.90, 2.67) | 2.31 (1.44, 3.71) | 0.33 (0.10, 1.05) | 1.42 (0.82, 2.48) | 2.45 (1.51, 3.97) | ||
| Employment: | ||||||||
| Not employed | 1 | 1 (0.005) | 1 | 1 | 1 | 1 (0.005) | 1 | 1 |
| Employed | 1.02 (0.61, 1.70) | 1.50 (1.17, 1.92) | 1.38 (1.10, 1.73) | 1.12 (0.66, 1.88) | 1.54 (1.20, 1.98) | 1.38 (1.10, 1.75) | ||
| Marital status: | ||||||||
| Married/cohabiting | 1 | 1 (0.083) | 1 | 1 | 1 | 1 (0.068) | 1 | 1 |
| Never married | 1.17 (0.74, 1.85) | 0.75 (0.59, 0.95) | 0.78 (0.63, 0.97) | 1.18 (0.75, 1.85) | 0.77 (0.60, 0.97) | 0.76 (0.61, 0.95) | ||
| Divorce/separated/widowed | 0.68 (0.34, 1.38) | 0.86 (0.62, 1.20) | 0.93 (0.70, 1.24) | 0.64 (0.31, 1.30) | 0.84 (0.60, 1.17) | 0.89 (0.67, 1.20) | ||
| Poor mental health: | ||||||||
| No | 1 | 1 (0.091) | 1 | 1 | 1 | 1 (0.079) | 1 | 1 |
| Yes | 1.71 (1.13, 2.58) | 1.12 (0.88, 1.42) | 1.14 (0.91, 1.41) | 1.74 (1.14, 2.64) | 1.16 (0.91, 1.48) | 1.13 (0.91, 1.42) | ||
| Socio-Economic Factors | Men | |||||||
| Model 1: | Model 2: | |||||||
| Underweight | Healthy Weight | Overweight | Obesity | Underweight | Healthy Weight | Overweight | Obesity | |
| Age-adjusted OR (95% CI) | Reference (p-value) | Age-adjusted OR (95% CI) | Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | Reference (p-value) | Fully Adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | |
| Household Income: | ||||||||
| No income | 1.18 (0.77, 1.81) | 1 (< 0.001) | 0.85 (0.56, 1.29) | 1.50 (0.92, 2.44) | 0.99 (0.59, 1.67) | 1 (0.004) | 0.76 (0.47, 1.24) | 1.77 (1.00, 3.13) |
| Low income | 1 | 1 | 1 | 1 | 1 | 1 | ||
| Medium/high income | 0.25 (0.10, 0.65) | 2.04 (1.33, 3.13) | 3.71 (2.28, 6.02) | 0.43 (0.16, 1.16) | 1.48 (0.90, 2.42) | 2.14 (1.22, 3.75) | ||
| Socio-Economic Factors | Women | |||||||
| Model 1: | Model 2: | |||||||
| Underweight | Healthy Weight | Overweight | Obesity | Underweight | Healthy Weight | Overweight | Obesity | |
| Age-adjusted OR (95% CI) | Reference (p-value) | Age-adjusted OR (95% CI) | Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | Reference (p-value) | Fully Adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | |
| Household Income: | ||||||||
| No income | 1.04 (0.65, 1.68) | 1 (0.136) | 0.91 (0.70, 1.18) | 0.95 (0.75, 1.20) | 1.18 (0.69, 2.02) | 1 (0.649) | 1.08 (0.80, 1.45) | 1.07 (0.82, 1.39) |
| Low income | 1 | 1 | 1 | 1 | 1 | 1 | ||
| Medium/high income | 0.87 (0.29, 2.62) | 1.56 (0.94, 2.59) | 1.78 (1.13, 2.80) | 1.10 (0.32, 3.71) | 1.51 (0.85, 2.68) | 1.63 (0.97, 2.74) | ||
| Socio-Demographic Characteristics | Men | Women | ||
|---|---|---|---|---|
| N = 1655 | N = 3104 | |||
| Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | Age-adjusted OR (95% CI) | Fully Adjusted OR (95% CI) | |
| Ethnicity: | ||||
| African | 1 | 1 | 1 | 1 |
| Non-African | 1.30 (1.04, 1.62) | 1.11 (0.87, 1.41) | 0.85 (0.72, 1.00) | 0.73 (0.62, 0.87) |
| p-value | 0.024 | 0.402 | 0.053 | < 0.001 |
| Education: | ||||
| No education | 1 | 1 | 1 | 1 |
| Grade 1–7 | 1.03 (0.69, 1.55) | 1.03 (0.68, 1.56) | 1.33 (1.00, 1.77) | 1.40 (1.05, 1.86) |
| Grade 8–11 | 1.44 (0.96, 2.16) | 1.31 (0.86, 1.99) | 2.32 (1.73, 3.11) | 2.50 (1.85, 3.38) |
| Grade 12 | 2.32 (1.46, 3.68) | 2.07 (1.28, 3.33) | 1.53 (1.11, 2.10) | 1.61 (1.17, 2.23) |
| Higher | 4.70 (2.73, 8.08) | 3.88 (2.22, 6.77) | 2.29 (1.50, 3.50) | 2.28 (1.48, 3.51) |
| p-value heterogeneity | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| Employment: | ||||
| Not employed | 1 | 1 | 1 | 1 |
| Employed | 1.85 (1.45, 2.35) | 1.44 (1.12, 1.87) | 1.43 (1.17, 1.74) | 1.43 (1.17, 1.76) |
| p-value | < 0.001 | 0.005 | < 0.001 | < 0.001 |
| Marital status: | ||||
| Married/cohabiting | 1 | 1 | 1 | 1 |
| Never married | 0.39 (0.30, 0.53) | 0.44 (0.33, 0.60) | 0.76 (0.63, 0.91) | 0.75 (0.62, 0.91) |
| Divorced/separated/widowed | 0.55 (0.35, 0.87) | 0.58 (0.36, 0.93) | 0.95 (0.73, 1.23) | 0.92 (0.71, 1.20) |
| p-value heterogeneity | < 0.001 | < 0.001 | 0.013 | 0.013 |
| Poor mental health: | ||||
| No | 1 | 1 | 1 | 1 |
| Yes | 0.79 (0.59, 1.06) | 0.95 (0.69, 1.29) | 1.05 (0.87, 1.27) | 1.06 (0.88, 1.29) |
| p-value | 0.121 | 0.729 | 0.618 | 0.536 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mchiza, Z.J.-R.; Parker, W.-A.; Hossin, M.Z.; Heshmati, A.; Labadarios, D.; Falkstedt, D.; Koupil, I. Social and Psychological Predictors of Body Mass Index among South Africans 15 Years and Older: SANHANES-1. Int. J. Environ. Res. Public Health 2019, 16, 3919. https://doi.org/10.3390/ijerph16203919
Mchiza ZJ-R, Parker W-A, Hossin MZ, Heshmati A, Labadarios D, Falkstedt D, Koupil I. Social and Psychological Predictors of Body Mass Index among South Africans 15 Years and Older: SANHANES-1. International Journal of Environmental Research and Public Health. 2019; 16(20):3919. https://doi.org/10.3390/ijerph16203919
Chicago/Turabian StyleMchiza, Zandile June-Rose, Whadi-Ah Parker, Muhammad Zakir Hossin, Amy Heshmati, Demetre Labadarios, Daniel Falkstedt, and Ilona Koupil. 2019. "Social and Psychological Predictors of Body Mass Index among South Africans 15 Years and Older: SANHANES-1" International Journal of Environmental Research and Public Health 16, no. 20: 3919. https://doi.org/10.3390/ijerph16203919