Screening Value of Social Frailty and Its Association with Physical Frailty and Disability in Community-Dwelling Older Koreans: Aging Study of PyeongChang Rural Area

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Assessment of Social Frailty
2.3. Assessment of Physical Frailty
2.4. Assessment of Geriatric Conditions
2.5. Statistical Analysis
3. Results
3.1. Psychometrics of Social Frailty
3.1.1. Content Validity
3.1.2. Construct Validity
3.2. Prevalence of Social Frailty and Associated Characteristics
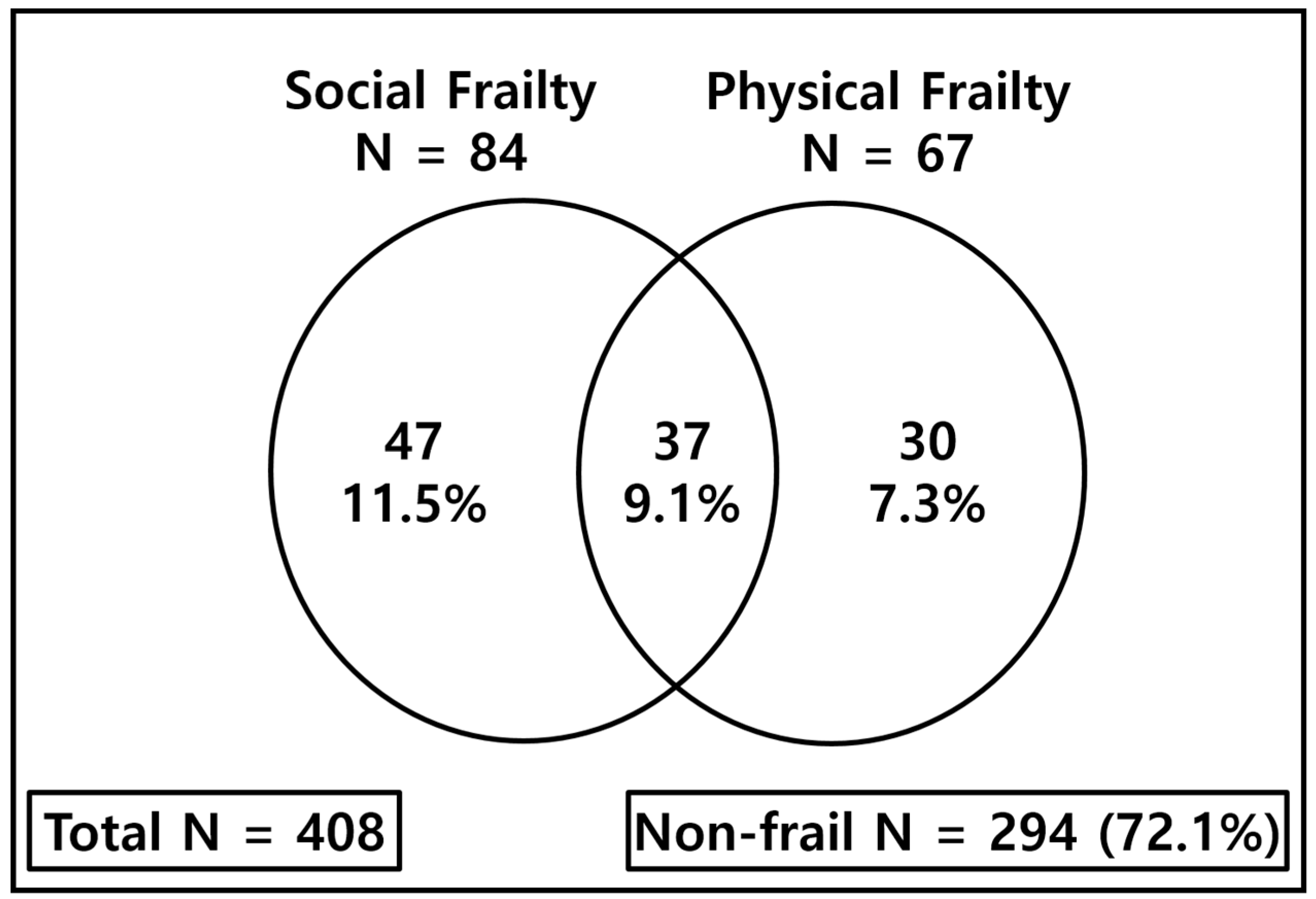
3.3. Social Frailty, Physical Frailty, and Geriatric Conditions
3.4. Association of Social Frailty and Physical Frailty in Geriatric Conditions
3.5. Social Frailty as a Screening Tool of ADL Disability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.-W.; Kim, S.-W.; Ahn, S.; Lim, J.-Y.; Han, J.-W.; Kim, T.-H.; Kim, C.H. Prevalence and outcomes of frailty in Korean elderly population: Comparisons of a multidimensional frailty index with two phenotype models. PLoS ONE 2014, 9, e87958. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Jang, I.Y.; Lee, Y.S.; Lee, C.K.; Cho, E.I.; Kang, W.Y.; Kim, D.H. Prevalence of Frailty and Aging-Related Health Conditions in Older Koreans in Rural Communities: A Cross-Sectional Analysis of the Aging Study of Pyeongchang Rural Area. J. Korean Med. Sci. 2016, 31, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K. What would make a definition of frailty successful? Age Ageing 2005, 34, 432–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Bunt, S.; Steverink, N.; Olthof, J.; van der Schans, C.P.; Hobbelen, J.S.M. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Makizako, H.; Hotta, R.; Nakakubo, S.; Makino, K.; Shimada, H. Association of Social Frailty With Both Cognitive and Physical Deficits Among Older People. J. Am. Med. Dir. Assoc. 2017, 18, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Tsutsumimoto, K.; Lee, S.; Doi, T.; Nakakubo, S.; Suzuki, T. Social Frailty in Community-Dwelling Older Adults as a Risk Factor for Disability. J. Am. Med. Dir. Assoc. 2015, 16, 1003. [Google Scholar] [CrossRef] [PubMed]
- Teo, N.; Gao, Q.; Nyunt, M.S.Z.; Wee, S.L.; Ng, T.P. Social Frailty and Functional Disability: Findings from the Singapore Longitudinal Ageing Studies. J. Am. Med. Dir. Assoc. 2017, 18, 637. [Google Scholar] [CrossRef]
- Yamada, M.; Arai, H. Social Frailty Predicts Incident Disability and Mortality Among Community-Dwelling Japanese Older Adults. J. Am. Med. Dir. Assoc. 2018, 19, 1099–1103. [Google Scholar] [CrossRef]
- Makizako, H.; Tsutsumimoto, K.; Shimada, H.; Arai, H. Social Frailty Among Community-Dwelling Older Adults: Recommended Assessments and Implications. Ann. Geriatr. Med. Res. 2018, 22, 3–8. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Makino, K.; Lee, S. Social Frailty Leads to the Development of Physical Frailty among Physically Non-Frail Adults: A Four-Year Follow-Up Longitudinal Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 490. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Kubozono, T.; Kiyama, R.; Takenaka, T.; Kuwahata, S.; Tabira, T.; Ohishi, M. Associations of social frailty with loss of muscle mass and muscle weakness among community-dwelling older adults. Geriatr. Gerontol. Int. 2019, 19, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Andrew, M.K.; Mitnitski, A.B.; Rockwood, K. Social vulnerability, frailty and mortality in elderly people. PLoS ONE 2008, 3, e2232. [Google Scholar] [CrossRef] [PubMed]
- Avlund, K.; Lund, R.; Holstein, B.E.; Due, P. Social relations as determinant of onset of disability in aging. Arch. Gerontol. Geriatr. 2004, 38, 85–99. [Google Scholar] [CrossRef]
- Lund, R.; Nilsson, C.J.; Avlund, K. Can the higher risk of disability onset among older people who live alone be alleviated by strong social relations? A longitudinal study of non-disabled men and women. Age Ageing 2010, 39, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Garre-Olmo, J.; Calvó-Perxas, L.; López-Pousa, S.; de Gracia Blanco, M.; Vilalta-Franch, J. Prevalence of frailty phenotypes and risk of mortality in a community-dwelling elderly cohort. Age Ageing 2012, 42, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Jang, I.-Y.; Jung, H.-W.; Lee, C.K.; Lee, Y.S.; Lee, E.; Kim, D.H. Comparison Between Korean Version of Physical Activity Scale for the Elderly and International Physical Activity Questionnaire-Short form in Evaluation of Frailty Phenotype. Ann. Geriatr. Med. Res. 2017, 21, 101. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; McBurnie, M.A. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Chun, M.Y. Validity and reliability of korean version of international physical activity questionnaire short form in the elderly. Korean J. Fam. Med. 2012, 33, 144–151. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the korean mini-mental state examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Hong, Y.J.; Yang, D.W.; Yoon, B.; Shim, Y.S.; Cho, A.H.; Han, I.W.; Moon, M.S. One-Year Follow-up Pilot Study for Dementia Diagnosis in Elderly with Recall Score of 0 in Korean-version of Mini-Mental State Examination. J. Korean Geriatr. Soc. 2014, 18, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.J.; Hong, Y.H.; Park, H.J.; Lee, J.E.; Yun, J.M.; Shin, D.W.; Kim, S.H. Depressive Mood and the Risk of Future Functional Decline in an Elderly Population. Ann. Geriatr. Med. Res. 2017, 21, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Lee, J.S. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Studenski, S.; Ferrucci, L. A diagnosis of dismobility—Giving mobility clinical visibility: A Mobility Working Group recommendation. JAMA 2014, 311, 2061–2062. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millan-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Jang, I.-Y.; Jung, H.-W.; Park, H.; Lee, C.K.; Yu, S.S.; Lee, Y.S.; Kim, D.H. A multicomponent frailty intervention for socioeconomically vulnerable older adults: A designed-delay study. Clin. Interv. Aging 2018, 13, 1799. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Belli, L.; Giudice, T.L.; Lorenzo, F.D.; Sancesario, G.M.; Sorge, R.; Martorana, A. Frailty among Alzheimer’s disease patients. CNS Neurol. Disord. Drug Targets 2013, 12, 507–511. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Social Frailty | |||
|---|---|---|---|
| Variables (n, %) | Robust | Prefrail | Frail |
| N = 203 | N = 121 | N = 84 | |
| Age (mean ± SD) | 72.7 ± 5.1 | 75.4 ± 5.6 | 79.3 ± 6.2 |
| 65–74 | 123 (60.6) | 52 (43.0) | 20 (23.8) |
| 75–84 | 76 (37.4) | 61 (50.4) | 51 (60.7) |
| 85– | 4 (2.0) | 8 (6.6) | 13 (15.5) |
| Female, n | 97 (47.8) | 80 (66.1) | 59 (70.2) |
| Multimorbidity, n | 93 (45.8) | 74 (61.2) | 64 (76.2) |
| Cognitive impairment, n [21,22] | 35 (17.2) | 31 (25.6) | 40 (47.6) |
| Depressed mood, n [3,23] | 9 (4.4) | 6 (5.0) | 17 (20.2) |
| Sarcopenia, n [24] | 30 (14.8) | 30 (24.8) | 34 (40.5) |
| Dysmobility, n [25] | 49 (24.1) | 56 (46.3) | 59 (70.2) |
| Fall, n | 38 (18.7) | 27 (22.3) | 28 (33.3) |
| Polypharmacy, n | 51 (25.1) | 40 (33.1) | 36 (42.9) |
| Malnutrition, n [26] | 41 (20.2) | 34 (28.1) | 33 (39.3) |
| Living alone, n | 2 (1.0) | 47 (38.8) | 46 (54.8) |
| Low income, n | 0 (0) | 3 (2.5) | 5 (6.0) |
| The CHS scale, n [19] | |||
| Robust | 96 (47.3) | 37 (30.6) | 11 (13.1) |
| Prefrail | 98 (48.3) | 64 (52.9) | 36 (42.9) |
| Frail | 9 (4.4) | 20 (16.5) | 37 (44.0) |
| Geriatric Conditions | Model 1 | Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Neither | SF Alone | PF Alone | Both | Neither | SF Alone | PF Alone | Both | |
| Cognitive impairment | ||||||||
| Prevalence, number [n (%)] | 53 (18.0%) | 14 (29.8%) | 13 (43.3%) | 26 (70.3%) | 53 (18.0%) | 14 (29.8%) | 13 (43.3%) | 26 (70.3%) |
| OR (95% CI) | Reference | 1.93 (0.97–3.86) | 3.48 (1.59–7.59) | 10.75 (5.00–23.10) | Reference | 1.28 (0.60–2.73) | 1.69 (0.71–4.01) | 4.94 (2.07–11.79) |
| p-value | 0.063 | 0.002 | <0.001 | 0.53 | 0.236 | <0.001 | ||
| Depressed mood | ||||||||
| Prevalence, number [n (%)] | 9 (3.1%) | 6 (12.8%) | 6 (20.0%) | 11 (29.7%) | 9 (3.1%) | 6 (12.8%) | 6 (20.0%) | 11 (29.7%) |
| OR (95% CI) | Reference | 4.63 (1.57–13.70) | 7.92 (2.60–24.11) | 13.40 (5.09–35.28) | Reference | 4.26 (1.38–13.19) | 6.29 (1.91–20.73) | 10.66 (3.45–32.93) |
| p-value | 0.006 | <0.001 | <0.001 | 0.012 | 0.003 | <0.001 | ||
| Sarcopenia | ||||||||
| Prevalence, number [n (%)] | 42 (14.3%) | 12 (25.5%) | 18 (60.0%) | 22 (59.5%) | 42 (14.3%) | 12 (25.5%) | 18 (60.0%) | 22 (59.5%) |
| OR (95% CI) | Reference | 2.06 (0.99–4.28) | 9.00 (4.04–20.03) | 8.80 (4.23–18.32) | Reference | 0.88 (0.37–2.08) | 4.71 (1.96–11.31) | 3.13 (1.34–7.32) |
| p-value | 0.054 | <0.001 | <0.001 | 0.763 | 0.001 | 0.008 | ||
| ADL disability | ||||||||
| Prevalence, number [n (%)] | 49 (16.7%) | 14 (29.8%) | 14 (46.7%) | 24 (64.9%) | 49 (16.7%) | 14 (29.8%) | 14 (46.7%) | 24 (64.9%) |
| OR (95% CI) | Reference | 3.10 (1.59–6.02) | 4.37 (2.00–9.55) | 9.23 (4.40–19.38) | Reference | 2.54 (1.26–5.13) | 3.10 (1.35–7.13) | 5.82 (2.56–13.25) |
| p-value | 0.001 | <0.001 | <0.001 | 0.009 | 0.008 | < 0.001 | ||
| Fall | ||||||||
| Prevalence, number [n (%)] | 57 (19.4%) | 11 (23.4%) | 8 (26.7%) | 17 (45.9%) | 57 (19.4%) | 11 (23.4%) | 8 (26.7%) | 17 (45.9%) |
| OR (95% CI) | Reference | 1.27 (0.61–2.65) | 1.51 (0.64–3.57) | 3.53 (1.74–7.18) | Reference | 1.14 (0.53–2.45) | 1.31 (0.53–3.25) | 2.85 (1.28–6.36) |
| p-value | 0.523 | 0.346 | <0.001 | 0.745 | 0.556 | 0.01 | ||
| Malnutrition | ||||||||
| Prevalence, number [n (%)] | 61 (20.7%) | 13 (27.7%) | 14 (46.7%) | 20 (54.1%) | 61 (20.7%) | 13 (27.7%) | 14 (46.7%) | 20 (54.1%) |
| OR (95% CI) | Reference | 1.46 (0.73–2.94) | 3.34 (1.55–7.22) | 4.49 (2.22–9.10) | Reference | 1.31 (0.63–2.72) | 2.92 (1.29–6.59) | 3.68 (1.67–8.11) |
| p-value | 0.288 | 0.002 | <0.001 | 0.47 | 0.010 | 0.001 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Jang, I.-Y.; Lee, H.y.; Jung, H.-W.; Lee, E.; Kim, D.H. Screening Value of Social Frailty and Its Association with Physical Frailty and Disability in Community-Dwelling Older Koreans: Aging Study of PyeongChang Rural Area. Int. J. Environ. Res. Public Health 2019, 16, 2809. https://doi.org/10.3390/ijerph16162809
Park H, Jang I-Y, Lee Hy, Jung H-W, Lee E, Kim DH. Screening Value of Social Frailty and Its Association with Physical Frailty and Disability in Community-Dwelling Older Koreans: Aging Study of PyeongChang Rural Area. International Journal of Environmental Research and Public Health. 2019; 16(16):2809. https://doi.org/10.3390/ijerph16162809
Chicago/Turabian StylePark, Hyungchul, Il-Young Jang, Hea yon Lee, Hee-Won Jung, Eunju Lee, and Dae Hyun Kim. 2019. "Screening Value of Social Frailty and Its Association with Physical Frailty and Disability in Community-Dwelling Older Koreans: Aging Study of PyeongChang Rural Area" International Journal of Environmental Research and Public Health 16, no. 16: 2809. https://doi.org/10.3390/ijerph16162809