Technology-Based Motivation Support for Seniors’ Physical Activity—A Qualitative Study on Seniors’ and Health Care Professionals’ Views


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
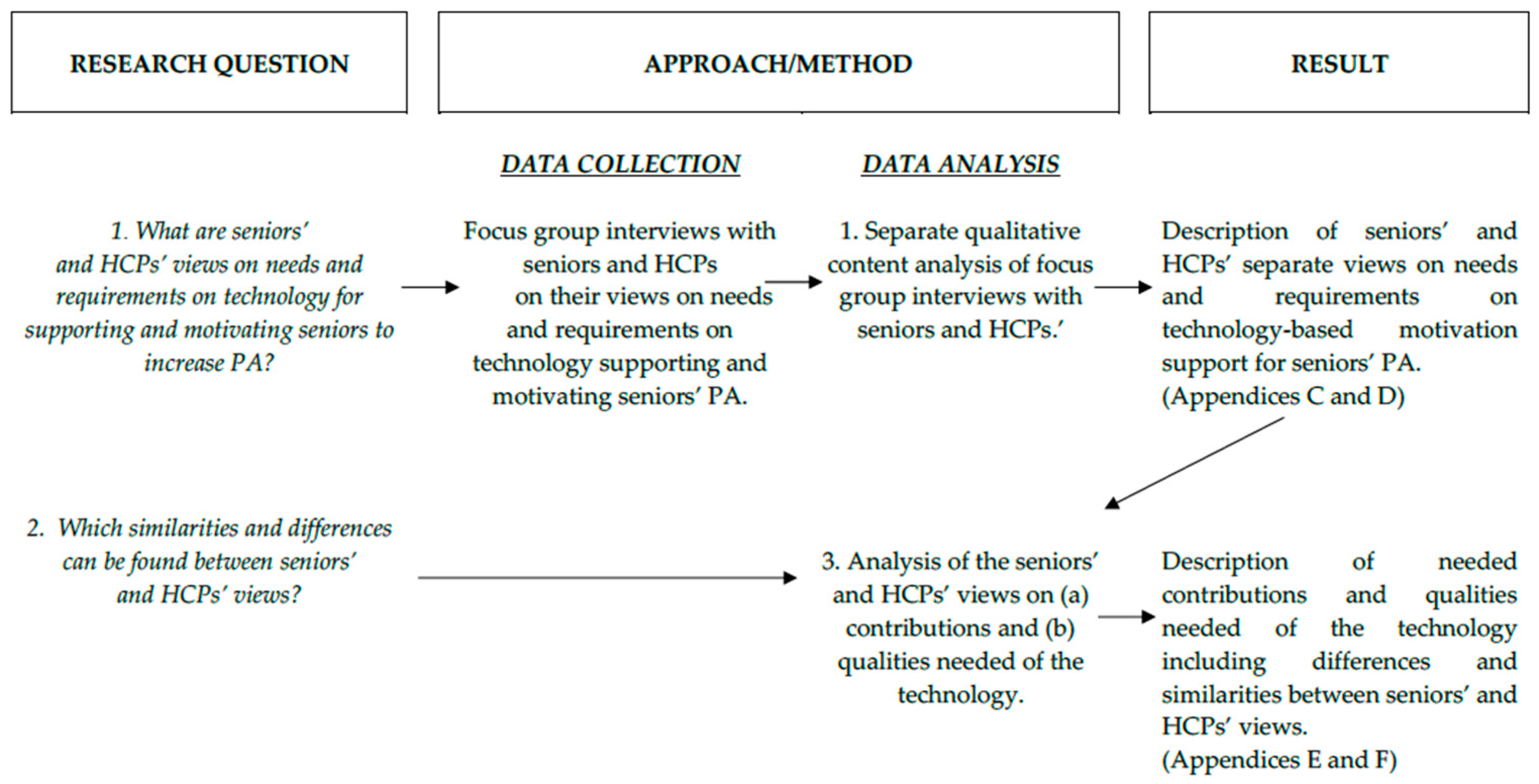
2.1. Study Design
2.2. Ethical Considerations
2.3. Recruitement and Participants
2.3.1. Seniors
2.3.2. Health Care Professionals
2.4. Data Collection
2.5. Data Analysis
2.5.1. Analysis of Seniors’ and HCPs’ Views Expressed in Focus Group Interviews
2.5.2. Analysis of Similarities and Differences in Views Expressed by Seniors and HCPs
3. Results
3.1. Focus Group Interviews
3.1.1. Seniors Views on Needs and Requirements on Technology-Based Motivation Support for PA
Surmountable
“That (a step counter) was not so fun. You needed to remember to put it on.”
“I think many people are afraid of technology. These things with credit cards and phones and people calling pretending to be…That strikes back on all technology in a way.”
Customizable
“Imagine that I came home one evening and when I sat down in front of the TV, sitting down there is something most people do anyway, and the first thing happening is that the screen asks me How am I today? What do I need to do to feel better?”
Helpful Facilitator
“But it is all the short distances you walk, if you summarize them every day. But that really adds up to something. Then you are adding on to the sum. That sounded a bit exciting”.
Conscious-Raising
“It might come as a shock, to see the amount of sedentary behavior this time of the year”.
Making Physical Activity Enjoyable
“We used to say that, for example, when we go bowling, that half of the amusement is the bowling and the other half is to get out and socialize with others. That is almost more important. For most of us it is at least more important than getting a good result”.
“But then you become motivated to do better in the next training session. I want to get thumbs up again.”
Useful for Organizations Reaching Inactive Persons
“If we [in the associations] had anything enabling us to attract for example 10–12 persons on our group walks instead of the seven persons that usually come, then we would have made an impact for those who really need the walks.”
3.1.2. HCPs’ Views on Needs and Requirements on Technology-Based Motivation Support for PA
Increasing Seniors’ Direct Motivation for PA
“It is still very much about understanding the aim and meaning of PA. Many persons think that a short walk with their dog is enough. But trying to make them realize that they need to increase and be active at another intensity is a challenge.”
“For the seniors we meet at the geriatric clinic, the main benefit might be just to be active during the day. Because an enormous amount of time is spent on nothing, people are very passive.”
Helping Seniors Overcome Hinderances to PA
“Among persons with weak balance that might have fallen. There is often, a not very much expressed, but a certain doubt to be active. And maybe above all else doubts, to be active by oneself.”
Increasing Senior’s Motivation for PA through Decreased Inactivity
“I guess many seniors think that they are worth sitting down, because they have worked and labored all their lives. And this I hear very often from older persons.”
“It is a form of help to self-help too. Then it might depend a lot on how you approach the person, how it is communicated.”
Attractive for Seniors
“My experience is that seniors used to say that they want to feel that they own the data themselves. That they want to have control of the information.”
Supporting the HCPs’ Clinical Work
“If we talk about a target group that needs rehabilitation in order to be activated, then it can be a real failure if you have a really bad day and are not able to do anything. In that situation, to get digital feedback saying today you have accomplished nothing. When instead I could already, from the start, lower my goal. Because then I might feel cheered up despite the bad day with low energy. Because I did something. And I think that is important.”
“I think that there is also a downside to this, a risk I can see is if the technology is used in order to replace any form of human contact. Especially when it comes to the oldest seniors with cognitive failure, then it is important to get another form of support, otherwise the technology will only become an obstacle.”
Facilitating Dialogue and Cooperation between Senior and Professional
“Seen to the work process of a physiotherapist, if you work with a patient for a longer period of time, it is always good to see if there has been an actual change. And in that sense, it might be difficult for some individuals to actually describe themselves if they have done something significantly different or not.”
“It might facilitate, I also think, if you are going to evaluate something. If you for example give the person an exercise program or a process and then the person says, ‘I have done a lot of training every day’, and then you see no progress. ‘Well, you haven’t been physically active according to this’. Then you can sort of discuss—is the lack of progress due to the fact that the exercises given are irrelevant or due to the low activity. So, it might facilitate our evaluation.”
3.2. Analysis of Similarities and Differences between Seniors’ and HCPs’ Views
3.2.1. Views on Possible Contributions from the Digital Technology in Supporting and Motivating Seniors to Increase PA
3.2.2. Views on Qualities that the Digital Technology-Based Motivational Support Should Have
4. Discussion
5. Conclusions
Supplementary Materials
Supplementary File 1Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
Appendix C
Appendix D
Appendix E
Appendix F
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.H.; Cable, N.T.; Faulkner, G.; Hillsdon, M.; Narici, M.; Van Der Bij, A.K. Physical activity and older adults: A review of health benefits and the effectiveness of interventions. J. Sports Sci. 2004, 22, 703–725. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.ncbi.nlm.nih.gov/books/NBK305057/ (accessed on 5 July 2019).
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, CD007146. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Simek, E.M.; McPhate, L.; Haines, T.P. Adherence to and efficacy of home exercise programs to prevent falls: A systematic review and meta-analysis of the impact of exercise program characteristics. Prev. Med. 2012, 55, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Pye, V.; Macniven, R.; van der Ploeg, H.; Milat, A.; Sherrington, C.; Lord, S.; Bauman, A. Prevalence and correlates of participation in fall prevention exercise/physical activity by older adults. Prev. Med. 2012, 55, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Chase, J.A. Physical activity interventions among older adults: A literature review. Res. Theory Nurs. Pract. 2013, 27, 53–80. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Beyer, N.; Hauer, K.; McKee, K.; Ballinger, C.; Todd, C. Recommendations for promoting the engagement of older people in activities to prevent falls. Qual. Saf. Health Care 2007, 16, 230–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sport Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Hamm, J.; Money, A.G.; Atwal, A.; Paraskevopoulos, I. Fall prevention intervention technologies: A conceptual framework and survey of the state of the art. J. Biomed. Inform. 2016, 59, 319–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, S.K.; Lewis, B.; Oakes, M.; Guan, W.; Wyman, J.F.; Rothman, A.J. Older Adults’ Experiences Using a Commercially Available Monitor to Self-Track Their Physical Activity. JMIR Mhealth Uhealth 2016, 4, e35. [Google Scholar] [CrossRef] [PubMed]
- Puri, A.; Kim, B.; Nguyen, O.; Stolee, P.; Tung, J.; Lee, J. User Acceptance of Wrist-Worn Activity Trackers Among Community-Dwelling Older Adults: Mixed Method Study. JMIR Mhealth Uhealth 2017, 5, e173. [Google Scholar] [CrossRef] [PubMed]
- Mercer, K.; Giangregorio, L.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of Commercially Available Wearable Activity Trackers Among Adults Aged Over 50 and With Chronic Illness: A Mixed-Methods Evaluation. JMIR Mhealth Uhealth 2016, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Ehn, M.; Eriksson, L.C.; Akerberg, N.; Johansson, A.C. Activity Monitors as Support for Older Persons’ Physical Activity in Daily Life: Qualitative Study of the Users’ Experiences. JMIR Mhealth Uhealth 2018, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Abras, C.; Maloney-Krichmar, D.; Preece, J. User-centered design. In Encyclopedia of Human-Computer Interaction; Bainbridge, W., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Rhodes, R.E.; McEwan, D.; Rebar, A.L. Theories of physical activity behaviour change: A history and synthesis of approaches. Psychol. Sport Exerc. 2018, 42, 100–109. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.N.; Markland, D.; Carraca, E.V.; Vieira, P.N.; Coutinho, S.R.; Minderico, C.S.; Matos, M.G.; Sardinha, L.B.; Teixeira, P.J. Exercise autonomous motivation predicts 3-yr weight loss in women. Med. Sci. Sports Exerc. 2011, 43, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Sebire, S.J.; Standage, M.; Vansteenkiste, M. Predicting objectively assessed physical activity from the content and regulation of exercise goals: Evidence for a mediational model. J. Sport Exerc. Psychol. 2011, 33, 175–197. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Intrinsic Motivation and Self-Determination in Human Behaviour; Plenum: New York, NY, USA, 1985. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraca, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- The Act Concerning the Ethical Review of Research Involving Humans (SFS 2003:460). Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-2003460-om-etikprovning-av-forskning-som_sfs-2003-460 (accessed on 5 July 2019).
- Ethical Review of Research. Available online: http://www.codex.vr.se/en/manniska5.shtml (accessed on 12 June 2019).
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Kolt, G.S.; Caperchione, C.M.; Savage, T.N.; Rosenkranz, R.R.; Maeder, A.J.; Van Itallie, A.; Tague, R.; Oldmeadow, C.; Mummery, W.K.; et al. Effectiveness of a Web 2.0 Intervention to Increase Physical Activity in Real-World Settings: Randomized Ecological Trial. J. Med. Internet Res. 2017, 19, e390. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175–1184. [Google Scholar] [CrossRef]
- Eckerstorfer, L.V.; Tanzer, N.K.; Vogrincic-Haselbacher, C.; Kedia, G.; Brohmer, H.; Dinslaken, I.; Corcoran, K. Key Elements of mHealth Interventions to Successfully Increase Physical Activity: Meta-Regression. JMIR Mhealth Uhealth 2018, 6, e10076. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior change techniques implemented in electronic lifestyle activity monitors: A systematic content analysis. J. Med. Internet Res. 2014, 16, e192. [Google Scholar] [CrossRef] [PubMed]
- Mercer, K.; Li, M.; Giangregorio, L.; Burns, C.; Grindrod, K. Behavior Change Techniques Present in Wearable Activity Trackers: A Critical Analysis. JMIR Mhealth Uhealth 2016, 4, e40. [Google Scholar] [CrossRef] [PubMed]
- Lockenhoff, C.E.; Carstensen, L.L. Socioemotional selectivity theory, aging, and health: The increasingly delicate balance between regulating emotions and making tough choices. J. Personal. 2004, 72, 1395–1424. [Google Scholar] [CrossRef] [PubMed]
- French, D.P.; Olander, E.K.; Chisholm, A.; Mc Sharry, J. Which behaviour change techniques are most effective at increasing older adults’ self-efficacy and physical activity behaviour? A systematic review. Ann. Behav. Med. 2014, 48, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Consolvo, S.; Everitt, K.; Smith, I.; Landa, J.A. Design requirements for technologies that encourage physical activity. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ‘06), Montreal, QC, Canada, 22–27 April 2006; ACM: New York, NY, USA; pp. 457–466. [Google Scholar] [CrossRef]
- Revenas, A.; Opava, C.H.; Asenlof, P. Lead users’ ideas on core features to support physical activity in rheumatoid arthritis: A first step in the development of an internet service using participatory design. BMC Med. Inform. Decis. Mak. 2014, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.M.; Moran, K.; Cornelissen, V.; Buys, R.; Cornelis, N.; Woods, C. Electronic Health Physical Activity Behavior Change Intervention to Self-Manage Cardiovascular Disease: Qualitative Exploration of Patient and Health Professional Requirements. J. Med. Internet Res. 2018, 20, e163. [Google Scholar] [CrossRef] [PubMed]
- Mehra, S.; Visser, B.; Dadema, T.; van den Helder, J.; Engelbert, R.H.H.; Weijs, P.J.M.; Krose, B.J.A. Translating Behavior Change Principles Into a Blended Exercise Intervention for Older Adults: Design Study. JMIR Res. Protoc. 2018, 7, e117. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, S.; Talley, K.M.; Wyman, J.F. Older people’s perspectives on fall risk and fall prevention programs: A literature review. Int. J. Older People Nurs. 2011, 6, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Middelweerd, A.; Mollee, J.S.; van der Wal, C.N.; Brug, J.; Te Velde, S.J. Apps to promote physical activity among adults: A review and content analysis. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 97. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D. Interpreting Qualitative Data: Methods for Analysing Talk, Text and Interaction, 2nd ed.; SAGE Publications: London, UK, 2001. [Google Scholar]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ehn, M.; Johansson, A.-C.; Revenäs, Å. Technology-Based Motivation Support for Seniors’ Physical Activity—A Qualitative Study on Seniors’ and Health Care Professionals’ Views. Int. J. Environ. Res. Public Health 2019, 16, 2418. https://doi.org/10.3390/ijerph16132418
Ehn M, Johansson A-C, Revenäs Å. Technology-Based Motivation Support for Seniors’ Physical Activity—A Qualitative Study on Seniors’ and Health Care Professionals’ Views. International Journal of Environmental Research and Public Health. 2019; 16(13):2418. https://doi.org/10.3390/ijerph16132418
Chicago/Turabian StyleEhn, Maria, Ann-Christin Johansson, and Åsa Revenäs. 2019. "Technology-Based Motivation Support for Seniors’ Physical Activity—A Qualitative Study on Seniors’ and Health Care Professionals’ Views" International Journal of Environmental Research and Public Health 16, no. 13: 2418. https://doi.org/10.3390/ijerph16132418