Does Community-Level Social Capital Predict Decline in Instrumental Activities of Daily Living? A JAGES Prospective Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
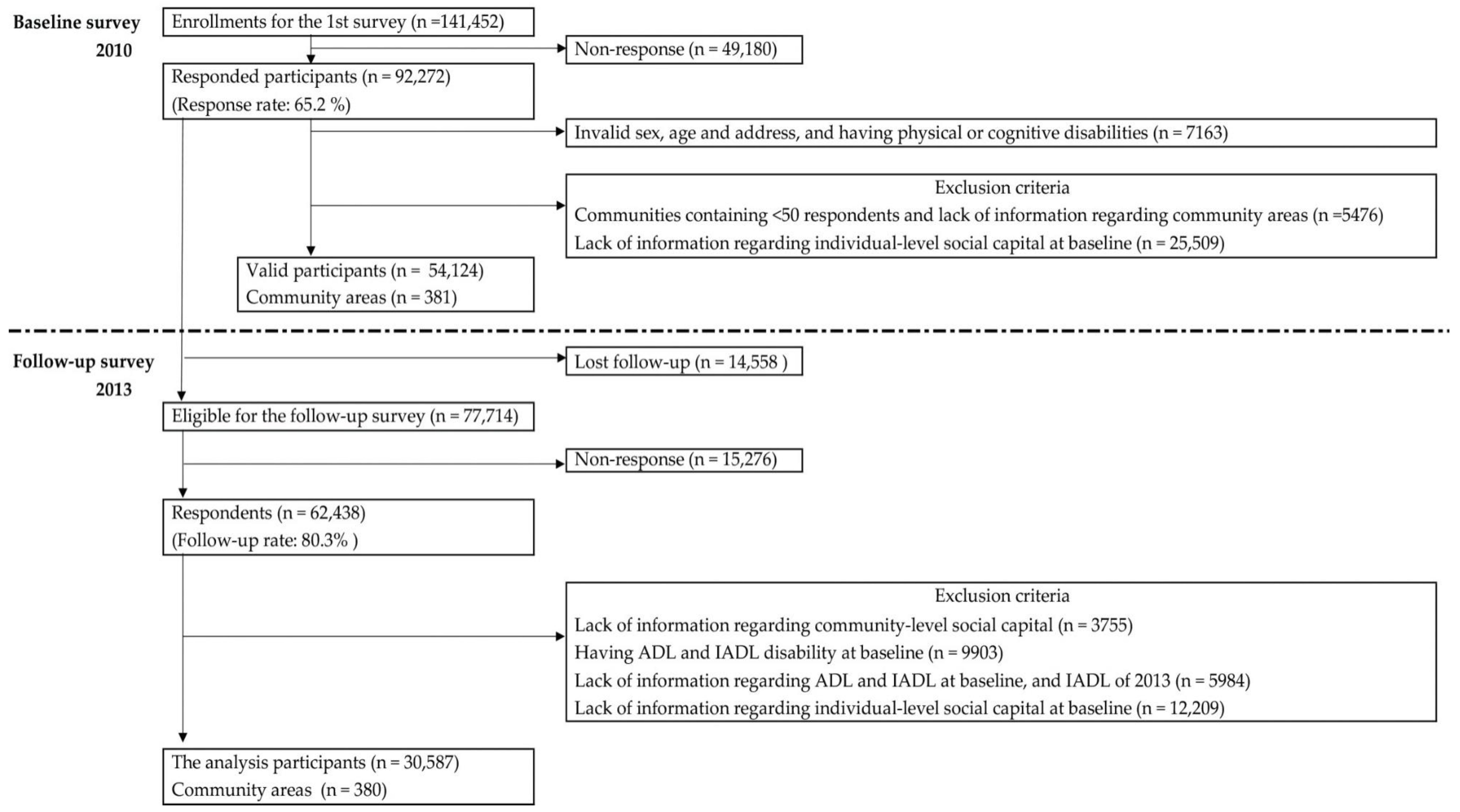
2.1. Data Sources and Participants
2.2. Dependent Variable: IADL
2.2.1. Main Predictor Variable: Community-Level Social Capital
2.2.2. Predictor Variable: Individual-Level Social Capital
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Spector, W.D.; Katz, S.; Murphy, J.B.; Fulton, J.P. The hierarchical relationship between activities of daily living and instrumental activities of daily living. J. Chronic Dis. 1987, 40, 481–489. [Google Scholar] [CrossRef]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG Index of Competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Millán-Calenti, J.C.; Tubío, J.; Pita-Fernández, S.; González-Abraldes, I.; Lorenzo, T.; Fernández-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, K.; Helmer, C.; Amieva, H.; Orgogozo, J.M.; Rouch, I.; Dartigues, J.F.; Barberger-Gateau, P. Natural history of decline in instrumental activities of daily living performance over the 10 years preceding the clinical diagnosis of dementia: A prospective population-based study. J. Am. Geriatr. Soc. 2008, 56, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Sorbye, L.W.; Hamran, T.; Henriksen, N.; Norberg, A. Home care patients in four Nordic capitals—Predictors of nursing home admission during one-year followup. J. Multidiscip. Healthc. 2010, 3, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Brettschneider, C.; Lange, C.; Posselt, T.; Wiese, B.; Steinmann, S.; Weyerer, S.; Werle, J.; Pentzek, M.; Fuchs, A.; et al. Longitudinal Predictors of Institutionalization in Old Age. PLoS ONE 2015, 10, e0144203. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Alecxih, L.; Branch, L.G.; Wiener, J.M. Medical and long-term care costs when older persons become more dependent. Am. J. Public Health 2002, 92, 1244–1245. [Google Scholar] [CrossRef] [PubMed]
- Fried, T.R.; Bradley, E.H.; Williams, C.S.; Tinetti, M.E. Functional disability and health care expenditures for older persons. Arch. Intern. Med. 2001, 161, 2602–2607. [Google Scholar] [CrossRef] [PubMed]
- Porell, F.W.; Miltiades, H.B. Regional differences in functional status among the aged. Soc. Sci. Med. 2002, 54, 1181–1198. [Google Scholar] [CrossRef]
- Kato, K.; Kondo, K.; Takeda, T.; Jeong, S. Are there inter-municipality differences in the ratio of individuals with limited activities of daily living?: The JAGES Project. J. Jpn. Assoc. Occup. Ther. 2015, 34, 541–554. (In Japanese) [Google Scholar]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, M.; Kawakami, N.; Kido, Y.; Sakurai, K. Social capital and suicide: An ecological study in Tokyo, Japan. Environ. Health Prev. Med. 2013, 1, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Skrabski, A.; Kopp, M.; Kawachi, I. Social capital in a changing society: Cross sectional associations with middle aged female and male mortality rates. J. Epidemiol. Community Health 2003, 57, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Kawachi, I. Social Capital, Social Cohesion, and Health. In Social Epidemiology, 2nd ed.; Berkman, L.F., Kawachi, I., Glymour, M.M., Eds.; Oxford University Press: New York, NY, USA, 2014; pp. 290–319. [Google Scholar]
- Aida, J.; Kondo, K.; Kawachi, I.; Subramanian, S.V.; Ichida, Y.; Hirai, H.; Kondo, N.; Osaka, K.; Sheiham, A.; Tsakos, G.; et al. Does social capital affect the incidence of functional disability in older Japanese? A prospective population-based cohort study. J. Epidemiol. Community Health 2013, 67, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Koyama, S.; Aida, J.; Saito, M.; Kondo, N.; Sato, Y.; Matsuyama, Y.; Tani, Y.; Sasaki, Y.; Kondo, K.; Ojima, T.; et al. Community social capital and tooth loss in Japanese older people: A longitudinal cohort study. BMJ Open 2016, 6, e010768. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, T.; Miyaguni, Y.; Kanamori, S.; Hanazato, M.; Kondo, K. Community-level Sports Group Participation and Older Individuals’ Depressive Symptoms. Med. Sci. Sports Exerc. 2018, 50, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Mohan, J.; Twigg, L.; Barnard, S.; Jones, K. Social capital, geography and health: A small-area analysis for England. Soc. Sci. Med. 2005, 60, 1267–1283. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Johansson, S.E.; Yang, M.; Sundquist, K. Low linking social capital as a predictor of coronary heart disease in Sweden: A cohort study of 2.8 million people. Soc. Sci. Med. 2006, 62, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Subramanian, S.V.; Kawachi, I. Social capital and physical health: A systematic review of the literature. In Social Capital and Health; Kawachi, I., Subramanian, S.V., Kim, D., Eds.; Springer: New York, NY, USA, 2008; pp. 139–190. [Google Scholar]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social capital and health: A review of prospective multilevel studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Saito, M.; Kondo, N.; Aid, J.; Kawachi, I.; Koyama, S.; Ojima, T.; Kondo, K. Development of an instrument for community-level health related social capital among Japanese older people: The JAGES Project. J. Epidemiol. 2017, 27, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Aida, J.; Yamamoto, T.; Otsuka, R.; Nakade, M.; Suzuki, K.; Kondo, K.; Osaka, K. Individual- and community-level social gradients of edentulousness. BMC Oral Health 2015, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.; Cagney, K.A.; Christakis, N.A. Effect of specific aspects of community social environment on the mortality of individuals diagnosed with serious illness. Soc. Sci. Med. 2005, 61, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K. Progress in aging epidemiology in Japan: The JAGES project. J. Epidemiol. 2016, 26, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P. Assessing the competence of older people. In Research Planning and Action for the Elderly: The Power and Potential of Social Science; Kent, D.P., Kastenbaum, R., Sherwood, S., Eds.; Behavioral Publications: New York, NY, USA, 1972; pp. 122–143. [Google Scholar]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Sugiura, Y.; Tsuda, Y.; Kimura, M.; Hayashida, I.; Kusabiraki, T.; Kono, K. Association between sarcopenia and higher-level functional capacity in daily living in community-dwelling elderly subjects in Japan. Arch. Gerontol. Geriatr. 2012, 55, e9–e13. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, A.S.; Hayakawa, H.; Morimoto, T.; Kakuma, T. Screening for late life depression: Cut-off scores for the Geriatric Depression Scale and the Cornell Scale for Depression in Dementia among Japanese subjects. Int. J. Geriatr. Psychiatry 2003, 18, 498–505. [Google Scholar] [CrossRef] [PubMed]
- James, B.D.; Boyle, P.A.; Buchman, A.S.; Bennett, D.A. Relation of late-life social activity with incident disability among community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Association Between Social Participation and 3-Year Change in Instrumental Activities of Daily Living in Community-Dwelling Elderly Adults. J. Am. Geriatr. Soc. 2017, 65, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Portes, A. Social Capital: Its Origins and Applications in Modern Sociology. Annu. Rev. Sociol. 1998, 24, 1–24. [Google Scholar] [CrossRef]
- Villalonga-Olives, E.; Kawachi, I. The dark side of social capital: A systematic review of the negative health effects of social capital. Soc. Sci. Med. 2017, 194, 105–127. [Google Scholar] [CrossRef] [PubMed]
- Takagi, D.; Kondo, K.; Kondo, N.; Cable, N.; Ikeda, K.; Kawachi, I. Social disorganization/social fragmentation and risk of depression among older people in Japan: Multilevel investigation of indices of social distance. Soc. Sci. Med. 2013, 83, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Hirai, H. Change in individual-level social capital indicators among elderly salon program participants. J. Rural Plan. Assoc. 2010, 28, 201–206. (In Japanese) [Google Scholar] [CrossRef]
- Rostad, B.; Deeg, D.J.H.; Schei, B. Socioeconomic inequalities in health in older women. Eur. J. Ageing 2009, 6, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Darin-Mattsson, A.; Fors, S.; Kareholt, I. Different indicators of socioeconomic status and their relative importance as determinants of health in old age. Int. J. Equity Health 2017, 16, 173. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Hoeymans, N.; Feskens, E.J.; Van Den Bos, G.A.; Kromhout, D. Non-response bias in a study of cardiovascular diseases, functional status and self-rated health among elderly men. Age Ageing 1998, 27, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hikichi, H.; Kondo, N.; Kondo, K.; Aida, J.; Takeda, T.; Kawachi, I. Effect of a community intervention programme promoting social interactions on functional disability prevention for older adults: Propensity score matching and instrumental variable analyses, JAGES Taketoyo study. J. Epidemiol. Community Health 2015, 69, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Hikichi, H.; Kondo, K.; Takeda, T.; Kawachi, I. Social interaction and cognitive decline: Results of a 7-year community intervention. Alzheimers Dement (N. Y.) 2017, 3, 23–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Newly Decline of IADL | Total | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| Individual-Level Variable | Number | % | Number | % | Number |
| Sex | |||||
| Men | 12,034 | 86.5 | 1885 | 13.5 | 13,919 |
| Women | 15,667 | 94.0 | 1001 | 6.0 | 16,668 |
| Age (years) | |||||
| 65–69 | 11,628 | 93.1 | 858 | 6.9 | 12,486 |
| 70–74 | 8885 | 91.7 | 809 | 8.4 | 9694 |
| 75–79 | 5029 | 88.7 | 643 | 11.3 | 5672 |
| 80–84 | 1781 | 81.1 | 416 | 18.9 | 2197 |
| ≥85 | 378 | 70.3 | 160 | 29.7 | 538 |
| Marital status | |||||
| Married | 20,529 | 90.1 | 2264 | 9.9 | 22,793 |
| Windowed | 5039 | 91.2 | 485 | 8.8 | 5524 |
| Divorced | 960 | 96.4 | 36 | 3.6 | 996 |
| Never married | 602 | 95.3 | 30 | 4.8 | 632 |
| Educational attainment (years) | |||||
| <10 | 10,169 | 87.9 | 1400 | 12.1 | 11,569 |
| 10–12 | 10,969 | 92.5 | 895 | 7.5 | 11,864 |
| ≥13 | 6002 | 92.3 | 501 | 7.7 | 6503 |
| Annual household income (yen) | |||||
| <2,000,000 | 10,724 | 90.1 | 1182 | 9.9 | 11,906 |
| 2,000,000–3,999,999 | 10,861 | 91.3 | 1038 | 8.7 | 11,899 |
| ≥4,000,000 | 3093 | 91.6 | 282 | 8.4 | 3375 |
| Individual-level social capital | |||||
| Civic participation | |||||
| Yes | 14,257 | 93.2 | 1037 | 6.8 | 15,294 |
| No | 13,444 | 87.9 | 1849 | 12.1 | 15,293 |
| Social cohesion | |||||
| Yes | 24,820 | 90.59 | 2578 | 9.4 | 27,398 |
| No | 2881 | 90.34 | 308 | 9.7 | 3189 |
| Reciprocity | |||||
| Yes | 27,382 | 90.6 | 2852 | 9.4 | 30,234 |
| No | 319 | 90.4 | 34 | 9.6 | 353 |
| Presence of illnesses | |||||
| Yes | 18,914 | 90.1 | 2085 | 9.9 | 20,999 |
| No | 7114 | 92.0 | 621 | 8.0 | 7735 |
| Depression symptoms (GDS-15) | |||||
| Depression symptom (>5) | 4676 | 87.8 | 649 | 12.2 | 5325 |
| No depression | 22,862 | 91.1 | 2223 | 8.9 | 25,085 |
| Body mass index (kg/m2) | |||||
| <18.5 | 1538 | 89.99 | 171 | 10.01 | 1709 |
| 18.5–24.9 | 19,593 | 91.11 | 1912 | 8.89 | 21,505 |
| ≥25.0 | 5884 | 89.61 | 682 | 10.39 | 6566 |
| Smoking habit | |||||
| Yes | 2560 | 86.8 | 390 | 13.2 | 2950 |
| No | 24,308 | 91.0 | 2399 | 9.0 | 26,707 |
| Alcohol consumption | |||||
| Yes | 10,553 | 89.8 | 1199 | 10.2 | 11,752 |
| No | 16,928 | 91.1 | 1665 | 9.0 | 18,593 |
| Daily walking time (min/day) | |||||
| <30 | 7229 | 87.9 | 1000 | 12.2 | 21,898 |
| ≥30 | 20,066 | 91.6 | 1832 | 8.4 | 8229 |
| Frequency of going outside | |||||
| 1 time or more per week | 26,719 | 90.9 | 2673 | 9.1 | 29,392 |
| Less than 1 time per week | 826 | 81.3 | 190 | 18.7 | 1016 |
| Variables | Exploratory Factor Analysis * | ||
|---|---|---|---|
| Social Cohesion | Civic Participation | Reciprocity | |
| Community trust | 0.820 | 0.101 | 0.076 |
| Norms of reciprocity | 0.851 | −0.029 | −0.076 |
| Community attachment | 0.765 | −0.025 | −0.021 |
| Sports group | −0.026 | 0.781 | −0.020 |
| Volunteer group | 0.060 | 0.398 | 0.047 |
| Hobby activity | −0.001 | 0.887 | −0.006 |
| Received emotional support | −0.027 | −0.082 | 0.883 |
| Provided emotional support | −0.069 | 0.145 | 0.716 |
| Receiver instrumental support | 0.283 | −0.050 | 0.425 |
| Correlation coefficient | |||
| Social cohesion & Civic participation | 0.069 (p = 0.178) | ||
| Social cohesion & Reciprocity | 0.483 (p < 0.001) | ||
| Civic participation & Reciprocity | 0.278 (p < 0.001) | ||
| Variables | N | Mean | (SD) | (Min–Max) |
|---|---|---|---|---|
| Community-level social capital | ||||
| Social cohesion (factor score) | 380 | −0.0021 | (0.93) | (−2.67–2.61) |
| Civic participation (factor score) | 380 | −0.0027 | (0.92) | (−2.97–3.87) |
| Reciprocity (factor score) | 380 | −0.0014 | (0.91) | (−3.79–2.05) |
| Average annual household income (1,000,000 yen) | 380 | 2.55 | (0.41) | (1.46–4.27) |
| Population density (persons per km2 of inhabitable area) | ||||
| <2040 | 96 | |||
| 2040–6852 | 95 | |||
| 6853–10,122 | 95 | |||
| ≥10,123 | 94 | |||
| Area (km2) | ||||
| <1.256 | 96 | |||
| 1.256–2.2563 | 94 | |||
| 2.2564–5.134 | 95 | |||
| ≥5.135 | 95 |
| Variables | Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | |||||
| Community-level independent variable | ||||||||||
| Social cohesion | 1.15 | (1.07–1.24) | 1.02 | (0.94–1.10) | 1.01 | (0.93–1.09) | ||||
| Civic participation | 0.81 | (0.76–0.85) | 0.89 | (0.83–0.95) | 0.90 | (0.84–0.96) | ||||
| Reciprocity | 1.10 | (1.00–1.19) | 1.07 | (0.98–1.16) | 1.07 | (0.98–1.16) | ||||
| Community-level covariates | ||||||||||
| Average annual household income (1000 yen) | 1.16 | (0.99–1.35) | 1.19 | (1.02–1.39) | ||||||
| Population density (people/km2 of inhabitable area) (ref. ≥10,123) | ||||||||||
| <2040 | 1.82 | (1.43–2.33) | 1.77 | (1.39–2.25) | ||||||
| 2040–6852 | 1.54 | (1.25–1.90) | 1.50 | (1.21–1.84) | ||||||
| 6853–10,122 | 1.04 | (0.83–1.29) | 1.03 | (0.82–1.28) | ||||||
| Area (km2) (ref. ≥5.135) | ||||||||||
| <1.256 | 1.05 | (0.83–1.34) | 1.04 | (0.82–1.32) | ||||||
| 1.256–2.2563 | 1.00 | (0.82–1.22) | 1.00 | (0.82–1.21) | ||||||
| 2.2564–5.134 | 1.09 | (0.97–1.23) | 1.10 | (0.97–1.24) | ||||||
| Individual-level independent variable (ref. no) | ||||||||||
| Social cohesion | 0.87 | (0.76–0.99) | 0.95 | (0.83–1.08) | ||||||
| Civic participation | 0.64 | (0.58–0.69) | 0.68 | (0.63–0.74) | ||||||
| Reciprocity | 1.07 | (0.73–1.56) | 1.17 | (0.80–1.71) | ||||||
| Individual-level covariates | ||||||||||
| Sex (ref. women) | ||||||||||
| Men | 2.45 | (2.25–2.68) | 2.55 | (2.31–2.82) | ||||||
| Age (ref. 65–69) | ||||||||||
| 70–74 | 1.24 | (1.12–1.38) | 1.22 | (1.10–1.35) | ||||||
| 75–79 | 1.71 | (1.53–1.91) | 1.64 | (1.46–1.83) | ||||||
| 80–84 | 3.00 | (2.62–3.43) | 2.83 | (2.47–3.25) | ||||||
| ≥85 | 5.52 | (4.47–6.82) | 5.22 | (4.21–6.48) | ||||||
| Marital status (ref. divorced) | ||||||||||
| Married | 2.61 | (1.85–3.67) | 2.74 | (1.94–3.87) | ||||||
| Widowed | 2.32 | (1.63–3.31) | 2.37 | (1.66–3.38) | ||||||
| Never married | 1.36 | (0.82–2.24) | 1.36 | (0.82–2.25) | ||||||
| Educational attainment (ref. 10–12 years) | ||||||||||
| <10 | 1.41 | (1.29–1.55) | 1.39 | (1.27–1.53) | ||||||
| ≥13 | 0.92 | (0.82–1.03) | 0.92 | (0.82–1.04) | ||||||
| Annual household income (yen) (ref. ≥4,000,000) | ||||||||||
| <2,000,000 | 1.09 | (0.94–1.26) | 1.04 | (0.90–1.20) | ||||||
| 2,000,000–3,999,999 | 1.01 | (0.87–1.16) | 1.00 | (0.87–1.15) | ||||||
| Presence of illnesses (ref. no) | ||||||||||
| Yes | 1.13 | (1.02–1.24) | ||||||||
| Depression symptoms (ref. no depression) (GDS-5) | ||||||||||
| Depression symptom (GDS >5) | 1.25 | (1.13–1.38) | ||||||||
| Body mass index (ref. 18.5–24.9) | ||||||||||
| <18.5 | 1.12 | (0.94–1.33) | ||||||||
| ≥25.0 | 1.15 | (1.04–1.26) | ||||||||
| Smoking habit (ref. no) | ||||||||||
| Yes | 1.19 | (1.06–1.35) | ||||||||
| Alcohol consumption (ref. no) | ||||||||||
| Yes | 0.91 | (0.84–1.00) | ||||||||
| Daily walking time (ref. ≥30 min/day) | ||||||||||
| <30 | 1.34 | (1.23–1.46) | ||||||||
| Frequency of going outside (ref. 1 time or more per week) | ||||||||||
| Less than 1 time per week | 1.61 | (1.35–1.92) | ||||||||
| Random-effects parameters | ||||||||||
| Community-level variance (standard error) | 0.150 | 0.035 | 0.084 | 0.048 | 0.073 | 0.056 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujihara, S.; Tsuji, T.; Miyaguni, Y.; Aida, J.; Saito, M.; Koyama, S.; Kondo, K. Does Community-Level Social Capital Predict Decline in Instrumental Activities of Daily Living? A JAGES Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 828. https://doi.org/10.3390/ijerph16050828
Fujihara S, Tsuji T, Miyaguni Y, Aida J, Saito M, Koyama S, Kondo K. Does Community-Level Social Capital Predict Decline in Instrumental Activities of Daily Living? A JAGES Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(5):828. https://doi.org/10.3390/ijerph16050828
Chicago/Turabian StyleFujihara, Satoko, Taishi Tsuji, Yasuhiro Miyaguni, Jun Aida, Masashige Saito, Shihoko Koyama, and Katsunori Kondo. 2019. "Does Community-Level Social Capital Predict Decline in Instrumental Activities of Daily Living? A JAGES Prospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 5: 828. https://doi.org/10.3390/ijerph16050828