Objectively Measured Sitting and Standing in Workers: Cross-Sectional Relationship with Autonomic Cardiac Modulation

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Data Collection
2.3. Assessment of Sitting and Standing
2.4. Assessment of Heart Rate Variability During Sleep
2.5. Assessment of Possible Confounders and Effect Modifiers
2.6. Statistical Analyses
3. Results
3.1. Sitting Time and Nocturnal Resting Heart Rate and Heart Rate Variability
3.2. Standing Time, Nocturnal Resting Heart Rate, and Heart Rate Variability
4. Discussion
4.1. Sitting Time and Nocturnal Autonomic Modulation
4.2. Standing Time and Nocturnal Autonomic Modulation
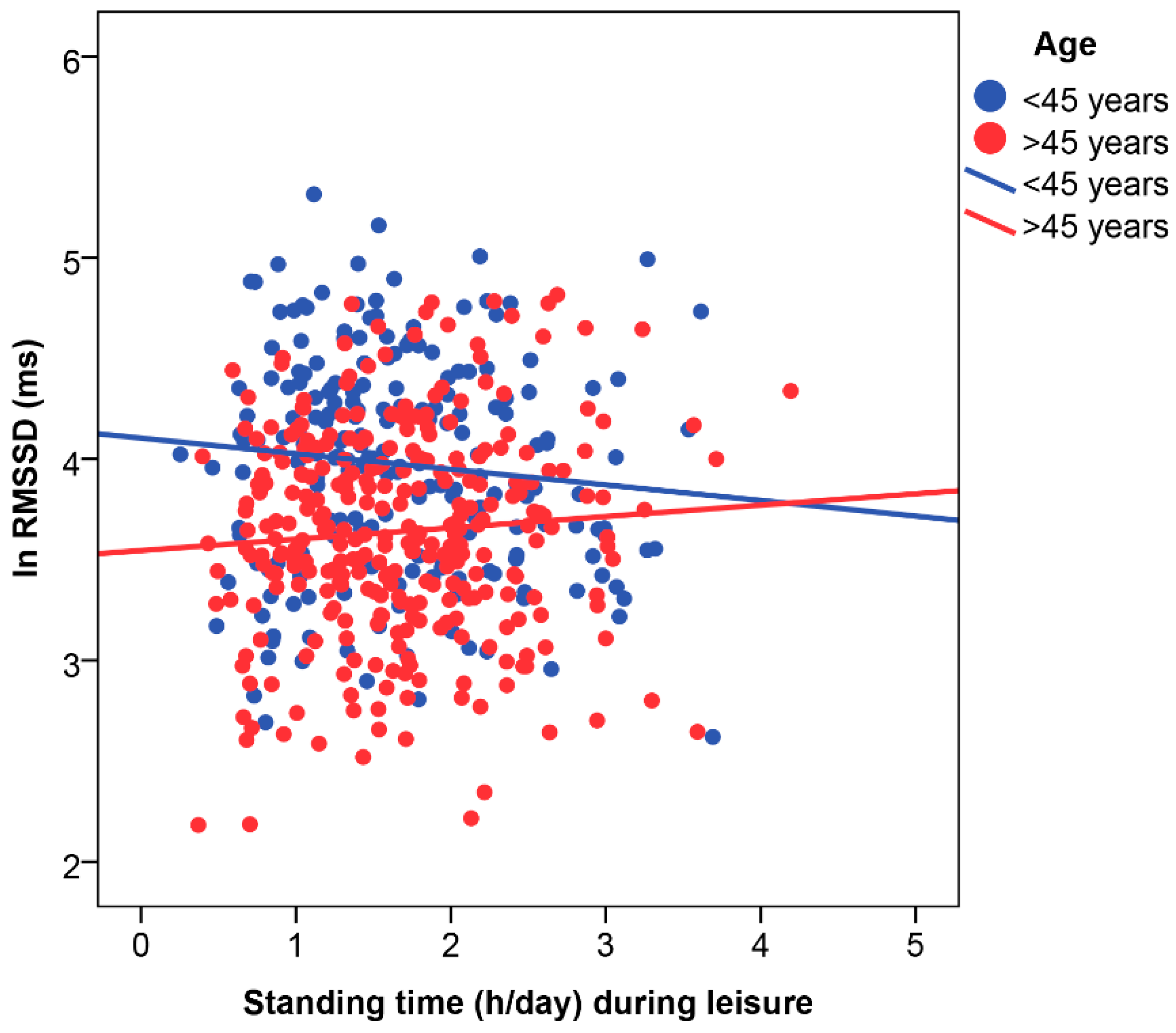
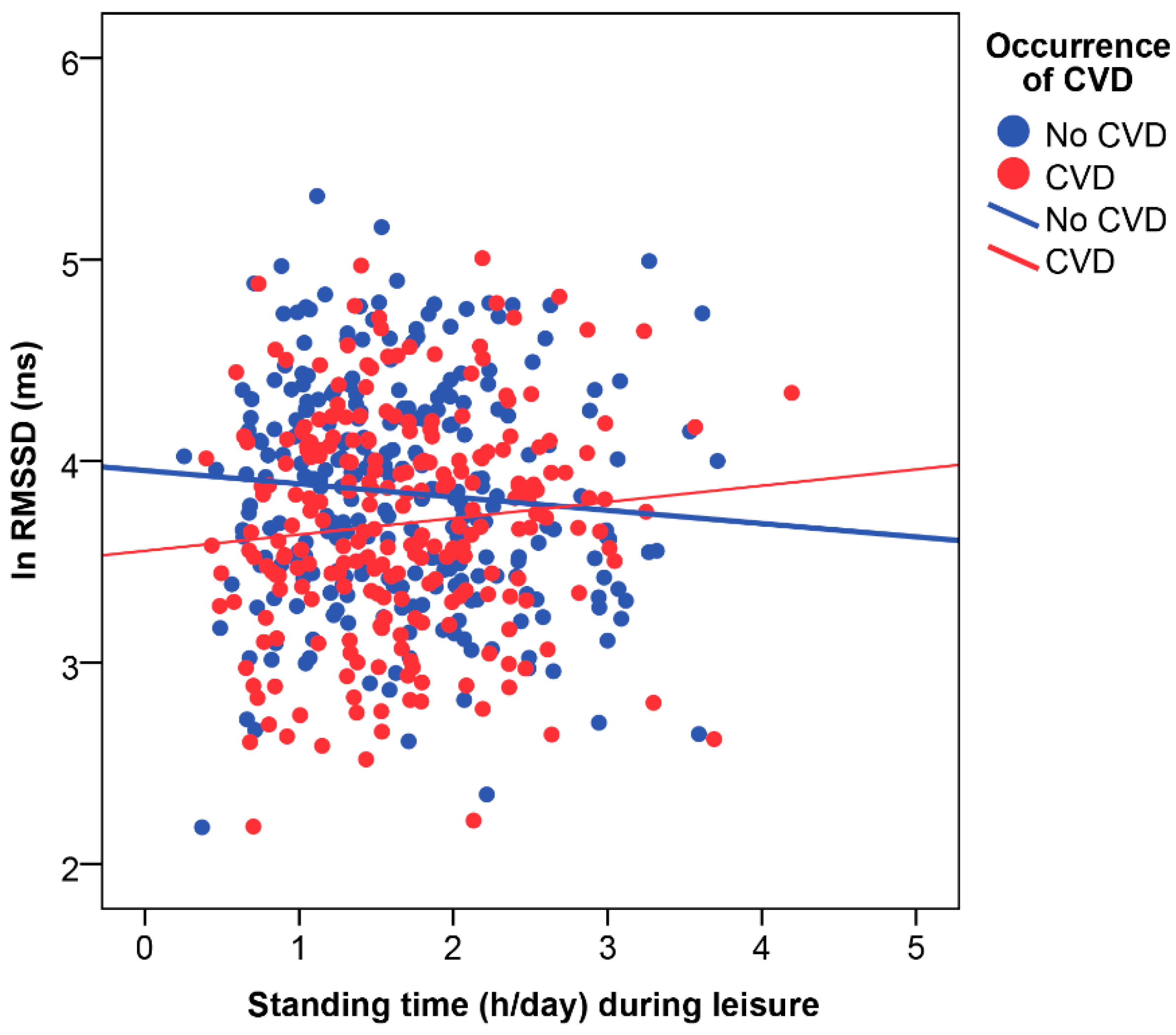
4.3. Effect Modification by Age, Cardiovascular Disease Status, and Physical Activity Domain
4.4. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Young, D.R.; Hivert, M.-F.; Alhassan, S.; Camhi, S.M.; Ferguson, J.F.; Katzmarzyk, P.T.; Lewis, C.E.; Owen, N.; Perry, C.K.; Siddique, J.; et al. Sedentary behavior and cardiovascular morbidity and mortality: A science advisory from the american heart association. Circulation 2016, 134, e262. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Salahuddin, U.; Garg, S.; Ayers, C.; Kulinski, J.; Anand, V.; Mayo, H.; Kumbhani, D.J.; de Lemos, J.; Berry, J.D. Continuous dose-response association between sedentary time and risk for cardiovascular disease: A meta-analysis. JAMA Cardiol. 2016, 1, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Bernstein, L.; Deka, A.; Feigelson, H.S.; Campbell, P.T.; Gapstur, S.M.; Colditz, G.A.; Thun, M.J. Leisure time spent sitting in relation to total mortality in a prospective cohort of us adults. Am. J. Epidemiol. 2010, 172, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.; Hartman, Y.; Holder, S.; Thijssen, D.H.; Hopkins, N.D. Sedentary behavior and cardiovascular disease risk: Mediating mechanisms. Exerc. Sport Sci. Rev. 2017, 45, 80–86. [Google Scholar] [CrossRef]
- Mueller, P.J. Physical (in)activity-dependent alterations at the rostral ventrolateral medulla: Influence on sympathetic nervous system regulation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R1468–R1474. [Google Scholar] [CrossRef]
- Hughson, R.L.; Shoemaker, J.K. Autonomic responses to exercise: Deconditioning/inactivity. Auton. Neurosci. 2015, 188, 32–35. [Google Scholar] [CrossRef]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. The role of vagal function in the risk for cardiovascular disease and mortality. Biol. Psychol. 2007, 74, 224–242. [Google Scholar] [CrossRef]
- Hallman, D.M.; Sato, T.; Kristiansen, J.; Gupta, N.; Skotte, J.; Holtermann, A. Prolonged sitting is associated with attenuated heart rate variability during sleep in blue-collar workers. Int. J. Environ. Res. Public Health 2015, 12, 14811–14827. [Google Scholar] [CrossRef]
- Rennie, K.L.; Hemingway, H.; Kumari, M.; Brunner, E.; Malik, M.; Marmot, M. Effects of moderate and vigorous physical activity on heart rate variability in a british study of civil servants. Am. J. Epidemiol. 2003, 158, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Melanson, E.L. Resting heart rate variability in men varying in habitual physical activity. Med. Sci. Sports Exerc. 2000, 32, 1894–1901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallman, D.M.; Birk Jørgensen, M.; Holtermann, A. On the health paradox of occupational and leisure-time physical activity using objective measurements: Effects on autonomic imbalance. PLoS ONE 2017, 12, e0177042. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.; Bromley, P.D.; Brodie, D.A. Effects of exercise on heart rate variability: Inferences from meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Iso, H.; Cui, R.; Tamakoshi, A. Occupational physical activity in relation to risk of cardiovascular mortality: The japan collaborative cohort study for evaluation for cancer risk (jacc study). Prev. Med. 2016, 89, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Waters, T.R.; Dick, R.B. Evidence of health risks associated with prolonged standing at work and intervention effectiveness. Rehabil. Nurs. 2015, 40, 148–165. [Google Scholar] [CrossRef] [PubMed]
- Krause, N.; Lynch, J.W.; Kaplan, G.A.; Cohen, R.D.; Salonen, R.; Salonen, J.T. Standing at work and progression of carotid atherosclerosis. Scand. J. Work. Environ. Health 2000, 26, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.; Ma, H.; Glazier, R.H.; Gilbert-Ouimet, M.; Mustard, C. The relationship between occupational standing and sitting and incident heart disease over a 12-year period in ontario, canada. Am. J. Epidemiol. 2018, 187, 27–33. [Google Scholar] [CrossRef]
- Hall, C.; Heck, J.E.; Sandler, D.P.; Ritz, B.; Chen, H.; Krause, N. Occupational and leisure-time physical activity differentially predict 6-year incidence of stroke and transient ischemic attack in women. Scand. J. Work. Environ. Health 2018. [Google Scholar] [CrossRef]
- Hallman, D.M.; Hed Ekman, A.; Lyskov, E. Changes in physical activity and heart rate variability in chronic neck-shoulder pain—Monitoring during work and leisure time. Int. Arch. Occup. Environ. Health 2014, 87, 735–744. [Google Scholar] [CrossRef]
- Coenen, P.; Parry, S.; Willenberg, L.; Shi, J.W.; Romero, L.; Blackwood, D.M.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. Associations of prolonged standing with musculoskeletal symptoms—A systematic review of laboratory studies. Gait Posture 2017, 58, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.A.; Perez-Bravo, F.; Ibañez, L.; Salas, C.; Bailey, M.E.S.; Gill, J.M.R. Objective vs. Self-reported physical activity and sedentary time: Effects of measurement method on relationships with risk biomarkers. PLoS ONE 2012, 7, e36345. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Christiansen, C.S.; Hanisch, C.; Bay, H.; Burr, H.; Holtermann, A. Is questionnaire-based sitting time inaccurate and can it be improved? A cross-sectional investigation using accelerometer-based sitting time. BMJ Open 2017, 7, e013251. [Google Scholar] [CrossRef] [PubMed]
- Lagersted-Olsen, J.; Korshöj, M.; Skotte, J.; Carneiro, I.G.; Søgaard, K.; Holtermann, A. Comparison of objectively measured and self-reported time spent sitting. Int. J. Sports Med. 2014, 35, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.; Faude, O.; Schwager, S.; Zahner, L.; Donath, L. Deviation between self-reported and measured occupational physical activity levels in office employees: Effects of age and body composition. Int. Arch. Occup. Environ. Health 2016, 89, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Messing, K.; Stock, S.; Cote, J.; Tissot, F. Is sitting worse than static standing? How a gender analysis can move us toward understanding determinants and effects of occupational standing and walking. J. Occup. Environ. Hyg. 2015, 12, D11–D17. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Loerbroks, A.; Angerer, P. Physical activity and risk of cardiovascular disease: What does the new epidemiological evidence show? Curr. Opin. Cardiol. 2013, 28, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Krause, N.; van der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (opa) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Krause, N. Physical activity and cardiovascular mortality—Disentangling the roles of work, fitness, and leisure. Scand. J. Work. Environ. Health 2010, 36, 349–355. [Google Scholar] [CrossRef]
- Rempel, D.; Krause, N. Do sit–stand workstations improve cardiovascular health? J. Occup. Environ. Med. 2018, 60, e319–e320. [Google Scholar]
- Böhm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Heart rate as a risk factor in chronic heart failure (shift): The association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef]
- Zhang, D.; Shen, X.; Qi, X. Resting heart rate and all-cause and cardiovascular mortality in the general population: A meta-analysis. CMAJ 2016, 188, E53–E63. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.T.; Suadicani, P.; Hein, H.O.; Gyntelberg, F. Elevated resting heart rate, physical fitness and all-cause mortality: A 16-year follow-up in the copenhagen male study. Heart 2013, 99, 882. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Rosei, E.A.; Casiglia, E.; Chalmers, J.; Ferrari, R.; Grassi, G.; Inoue, T.; Jelakovic, B.; Jensen, M.T.; Julius, S.; et al. Management of the hypertensive patient with elevated heart rate: Statement of the second consensus conference endorsed by the european society of hypertension. J. Hypertens. 2016, 34, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Johansen, C.D.; Olsen, R.H.; Pedersen, L.R.; Kumarathurai, P.; Mouridsen, M.R.; Binici, Z.; Intzilakis, T.; Køber, L.; Sajadieh, A. Resting, night-time, and 24 h heart rate as markers of cardiovascular risk in middle-aged and elderly men and women with no apparent heart disease. Eur. Heart J. 2013, 34, 1732–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Task force of the european society of cardiology and the north american society of pacing and electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Nolan, J.; Batin, P.D.; Andrews, R.; Lindsay, S.J.; Brooksby, P.; Mullen, M.; Baig, W.; Flapan, A.D.; Cowley, A.; Prescott, R.J.; et al. Prospective study of heart rate variability and mortality in chronic heart failure: Results of the united kingdom heart failure evaluation and assessment of risk trial (uk-heart). Circulation 1998, 98, 1510–1516. [Google Scholar] [CrossRef]
- Hillebrand, S.; Gast, K.B.; de Mutsert, R.; Swenne, C.A.; Jukema, J.W.; Middeldorp, S.; Rosendaal, F.R.; Dekkers, O.M. Heart rate variability and first cardiovascular event in populations without known cardiovascular disease: Meta-analysis and dose–response meta-regression. EP Eur. 2013, 15, 742–749. [Google Scholar] [CrossRef]
- Binici, Z.; Mouridsen, M.R.; Køber, L.; Sajadieh, A. Decreased nighttime heart rate variability is associated with increased stroke risk. Stroke 2011, 42, 3196. [Google Scholar] [CrossRef]
- Jørgensen, M.; Korshøj, M.; Lagersted-Olsen, J.; Villumsen, M.; Mortensen, O.; Skotte, J.; Søgaard, K.; Madeleine, P.; Thomsen, B.; Holtermann, A. Physical activities at work and risk of musculoskeletal pain and its consequences: Protocol for a study with objective field measures among blue-collar workers. BMC Musculoskelet. Disord. 2013, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hallman, D.M.; Mathiassen, S.E.; Gupta, N.; Korshoj, M.; Holtermann, A. Differences between work and leisure in temporal patterns of objectively measured physical activity among blue-collar workers. BMC Public Health 2015, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hallman, D.M.; Mathiassen, S.E.; Heiden, M.; Gupta, N.; Jørgensen, M.B.; Holtermann, A. Temporal patterns of sitting at work are associated with neck–shoulder pain in blue-collar workers: A cross-sectional analysis of accelerometer data in the dphacto study. Int. Arch. Occup. Environ. Health 2016, 89, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Skotte, J.; Korshøj, M.; Kristiansen, J.; Hanisch, C.; Holtermann, A. Detection of physical activity types using triaxial accelerometers. J. Phys. Act. Health 2014, 11, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Stemland, I.; Ingebrigtsen, J.; Christiansen, C.S.; Jensen, B.R.; Hanisch, C.; Skotte, J.; Holtermann, A. Validity of the acti4 method for detection of physical activity types in free-living settings: Comparison with video analysis. Ergonomics 2015, 58, 953–965. [Google Scholar] [CrossRef] [PubMed]
- Ingebrigtsen, J.; Stemland, I.; Christiansen, C.S.; Skotte, J.; Christiana, H.; Krustrup, P.; Holtermann, A. Validation of a commercial and custom made accelerometer-based software for step count and frequency during walking and running. J. Ergon. 2013, 3, 1–6. [Google Scholar] [CrossRef]
- Peeters, G.; van Gellecum, Y.; Ryde, G.; Farías, N.A.; Brown, W.J. Is the pain of activity log-books worth the gain in precision when distinguishing wear and non-wear time for tri-axial accelerometers? J. Sci. Med. Sport 2013, 16, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Stordal Christiansen, C.; Hallman, D.M.; Korshøj, M.; Gomes Carneiro, I.; Holtermann, A. Is objectively measured sitting time associated with low back pain? A cross-sectional investigation in the nomad study. PLoS ONE 2015, 10, e0121159. [Google Scholar] [CrossRef]
- Skotte, J.; Kristiansen, J. Heart rate variability analysis using robust period detection. Biomed. Eng. Online 2014, 13, 138. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 esh/esc guidelines for the management of arterial hypertension. Blood Press. 2013, 22, 193–278. [Google Scholar] [CrossRef]
- Palatini, P. Elevated heart rate: A “new” cardiovascular risk factor? Prog. Cardiovasc. Dis. 2009, 52, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Reyes del Paso, G.A.; Langewitz, W.; Mulder, L.J.M.; van Roon, A.; Duschek, S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: A review with emphasis on a reanalysis of previous studies. Psychophysiology 2013, 50, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Arah, O.A.; Kauhanen, J.; Krause, N. Effects of leisure-time and occupational physical activities on 20-year incidence of acute myocardial infarction: Mediation and interaction. Scand. J. Work. Environ. Health 2016, 42, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Glagov, S.; Zarins, C.; Giddens, D.P.; Ku, D.N. Hemodynamics and atherosclerosis—Insights and perspectives gained from studies of human arteries. Arch. Pathol. Lab. Med. 1988, 112, 1018–1031. [Google Scholar] [PubMed]
- Czernichow, S.; Zanchetti, A.; Turnbull, F.; Barzi, F.; Ninomiya, T.; Kengne, A.-P.; Lambers Heerspink, H.J.; Perkovic, V.; Huxley, R.; Arima, H.; et al. The effects of blood pressure reduction and of different blood pressure-lowering regimens on major cardiovascular events according to baseline blood pressure: Meta-analysis of randomized trials. J. Hypertens. 2011, 29, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S. Compendium of physical activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.H.; Jones, G.R.; Rice, C.L. Aging and physical activity data on which to base recommendations for exercise in older adults. Appl. Physiol. Nutr. Metab. 2007, 32, S75–S171. [Google Scholar] [CrossRef] [PubMed]
- Holme, I.; Helgeland, A.; Hjermann, I.; Leren, P.; Lund-Larsen, P.G. Physical activity at work and at leisure in relation to coronary risk factors and social class. Acta Med. Scand. 1981, 209, 277–283. [Google Scholar] [CrossRef]
- Krause, N.; Arah, O.A.; Kauhanen, J. Physical activity and 22-year all-cause and coronary heart disease mortality. Am. J. Ind. Med. 2017, 60, 976–990. [Google Scholar] [CrossRef]
- Coenen, P.; Huysmans, M.; Holtermann, A.; Krause, N.; van Mechelen, W.; Straker, L.; van der Beek, J. Do highly physically active workers die early? A systematic review with meta-analysis of data from 154,459 participants. Br. J. Sports Med. 2018, 52, 1320–1326. [Google Scholar] [CrossRef]
- Hall, M.; Vasko, R.; Buysse, D.; Ombao, H.; Chen, Q.; Cashmere, J.D.; Kupfer, D.; Thayer, J.F. Acute stress affects heart rate variability during sleep. Psychosom. Med. 2004, 66, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | N | n | % | Mean (SD) | Range |
|---|---|---|---|---|---|
| Age (years) | 490 | 45 (10) | 18–68 | ||
| Gender (female) | 490 | 215 | 43.9 | ||
| BMI (kg/m2) | 490 | 27.4 (4.7) | 18.1–43.8 | ||
| Smoking (yes) | 490 | 121 | 24.7 | ||
| Sector | 490 | ||||
| Cleaning | 99 | 20.2 | |||
| Manufacturing | 349 | 71.2 | |||
| Transportation | 42 | 8.6 | |||
| Seniority (years) | 479 | 13.8 (10.3) | 0–45 | ||
| MVPA leisure (h/day) | 0.7 (0.4) | 0.1–2.0 | |||
| Medication | 489 | ||||
| CVD medication a | 85 | 17.4 | |||
| Antidepressants b | 15 | 3.1 | |||
| Analgesics b | 93 | 19.0 | |||
| Other medication b | 114 | 23.3 | |||
| Hypertension c | 188 | 38.4 | |||
| Accelerometer wear-time | 490 | ||||
| Number of measured days | 2.7 (1.0) | 1–5 | |||
| Work hours (h/day) | 7.6 (1.2) | 4–14 | |||
| Leisure time (h/day) | 8.8 (1.5) | 4–13 | |||
| Exposure at work | 490 | ||||
| Sitting (h/day) | 2.4 (1.7) | 0.2–9.2 | |||
| Standing (h/day) | 2.5 (1.1) | 0.2–6.7 | |||
| Exposure during leisure | 490 | ||||
| Sitting (h/day) | 4.8 (1.3) | 1.8–10.2 | |||
| Standing (h/day) | 1.7 (0.7) | 0.3–4.2 |
| Variable | Age < 45 years (N = 196) | Age ≥ 45 years (N = 294) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % | Mean (SD) | Range | N | n | % | Mean (SD) | Range | |
| Age (years) | 196 | 36 (7) | 18–44 | 294 | 52 (5) | 45–68 | ||||
| Gender (female) | 196 | 76 | 38.8 | 294 | 139 | 47.3 | ||||
| BMI (kg/m2) | 196 | 26.8 (4.8) | 18.4–43.8 | 294 | 27.8 (4.7) | 18.1–43.5 | ||||
| Smoking (yes) | 196 | 46 | 23.5 | 294 | 75 | 25.5 | ||||
| Sector | 196 | 294 | ||||||||
| Cleaning | 35 | 17.9 | 64 | 21.8 | ||||||
| Manufacturing | 145 | 74.0 | 204 | 69.4 | ||||||
| Transportation | 16 | 8.2 | 26 | 8.8 | ||||||
| Seniority (years) | 192 | 9.6 (6.9) | 0.1–29.2 | 287 | 16.5 (11.3) | 0.2–45.0 | ||||
| MVPA leisure (h/day) | 196 | 0.7 (0.3) | 0.1–1.9 | 294 | 0.7 (0.4) | 0.1–2.0 | ||||
| Medication | 195 | 294 | ||||||||
| CVD medication a | 13 | 6.7 | 72 | 24.5 | ||||||
| Antidepressants b | 10 | 5.1 | 5 | 1.7 | ||||||
| Analgesics b | 34 | 17.4 | 59 | 20.1 | ||||||
| Other medication b | 32 | 16.4 | 82 | 27.9 | ||||||
| Hypertension c | 196 | 52 | 26.5 | 294 | 136 | 46.3 | ||||
| Accelerometer wear-time | ||||||||||
| Number of measured days | 196 | 2.6 (1.0) | 1–5 | 294 | 2.8 (0.9) | 1–5 | ||||
| Work hours (h/day) | 196 | 7.6 (1.3) | 4.5–12.0 | 294 | 7.6 (1.2) | 3.8–13.7 | ||||
| Leisure time (h/day) | 196 | 8.6 (1.5) | 4.2–13.1 | 294 | 9.0 (1.5) | 4.5–13.4 | ||||
| Exposure at work | ||||||||||
| Sitting (h/day) | 196 | 2.5 (1.6) | 0.4–9.2 | 294 | 2.3 (1.7) | 0.2–8.0 | ||||
| Standing (h/day) | 196 | 2.5 (1.2) | 0.2–6.3 | 294 | 2.5 (1.1) | 0.2–6.7 | ||||
| Exposure during leisure | ||||||||||
| Sitting (h/day) | 196 | 4.5 (1.2) | 1.8–8.0 | 294 | 5.0 (1.4) | 1.9–10.2 | ||||
| Standing (h/day) | 196 | 1.7 (0.7) | 0.3–0.7 | 294 | 1.7 (0.7) | 0.4–4.2 | ||||
| Sitting at Work | Sitting During Leisure | |||||
|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |
| Unadjusted model (n = 490) | ||||||
| Heart rate (bpm) | −0.19 | −0.59 to 0.21 | 0.35 | 0.83 | 0.33 to 1.34 | <0.001 |
| SDNN (ms) | −0.33 | −1.53 to 0.88 | 0.60 | −2.26 | −3.78 to −0.75 | <0.001 |
| RMSSD (ln) | −0.02 | −0.05 to 0.01 | 0.14 | −0.04 | −0.08 to −0.01 | 0.02 |
| HF (ln) | −0.05 | −0.11 to 0.01 | 0.12 | −0.08 | −0.15 to 0.00 | 0.06 |
| LF (ln) | 0.02 | −0.03 to 0.07 | 0.37 | −0.10 | −0.16 to −0.04 | <0.001 |
| Adjusted model a (n = 490) | ||||||
| Heart rate (bpm) | 0.02 | −0.38 to 0.42 | 0.91 | 0.58 | 0.08 to 1.08 | 0.02 |
| SDNN (ms) | −0.39 | −1.58 to 0.79 | 0.52 | −1.12 | −2.62 to 0.39 | 0.15 |
| RMSSD (ln) | −0.01 | −0.04 to 0.01 | 0.34 | −0.01 | −0.05 to 0.02 | 0.44 |
| HF (ln) | −0.03 | −0.09 to 0.03 | 0.37 | −0.01 | −0.09 to 0.06 | 0.71 |
| LF (ln) | 0.01 | −0.04 to 0.06 | 0.61 | −0.06 | −0.12 to 0.01 | 0.07 |
| Standing at Work | Standing During Leisure | ||||||
|---|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | ||
| Unadjusted model (n = 490) | |||||||
| Heart rate (bpm) | −0.65 | −1.24 to −0.05 | 0.03 | 0.73 | −0.23 to 1.70 | 0.14 | |
| SDNN (ms) | 1.50 | −0.29 to 3.29 | 0.10 | 1.70 | −1.20 to 4.60 | 0.25 | |
| RMSSD (ln) | 0.05 | 0.00 to 0.09 | 0.04 | 0.02 | −0.05 to 0.09 | 0.59 | |
| HF (ln) | 0.09 | 0.00 to 0.19 | 0.05 | 0.05 | −0.09 to 0.20 | 0.47 | |
| LF (ln) | 0.05 | −0.03 to 0.12 | 0.21 | 0.06 | −0.06 to 0.18 | 0.33 | |
| Adjusted model a (n = 490) | |||||||
| Heart rate (bpm) | −0.70 | −1.27 to −0.13 | 0.02 | 0.49 | −0.53 to 1.52 | 0.34 | |
| SDNN (ms) | 1.21 | −0.50 to 2.91 | 0.17 | 2.16 | −0.90 to 5.22 | 0.17 | |
| RMSSD (ln) | 0.04 | 0.00 to 0.08 | 0.05 | −0.01 | −0.09 to 0.06 | 0.77 | |
| HF (ln) | 0.08 | −0.01 to 0.16 | 0.07 | −0.02 | −0.17 to 0.14 | 0.84 | |
| LF (ln) | 0.04 | −0.03 to 0.11 | 0.27 | 0.11 | −0.01 to 0.22 | 0.08 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hallman, D.M.; Krause, N.; Jensen, M.T.; Gupta, N.; Birk Jørgensen, M.; Holtermann, A. Objectively Measured Sitting and Standing in Workers: Cross-Sectional Relationship with Autonomic Cardiac Modulation. Int. J. Environ. Res. Public Health 2019, 16, 650. https://doi.org/10.3390/ijerph16040650
Hallman DM, Krause N, Jensen MT, Gupta N, Birk Jørgensen M, Holtermann A. Objectively Measured Sitting and Standing in Workers: Cross-Sectional Relationship with Autonomic Cardiac Modulation. International Journal of Environmental Research and Public Health. 2019; 16(4):650. https://doi.org/10.3390/ijerph16040650
Chicago/Turabian StyleHallman, David M., Niklas Krause, Magnus Thorsten Jensen, Nidhi Gupta, Marie Birk Jørgensen, and Andreas Holtermann. 2019. "Objectively Measured Sitting and Standing in Workers: Cross-Sectional Relationship with Autonomic Cardiac Modulation" International Journal of Environmental Research and Public Health 16, no. 4: 650. https://doi.org/10.3390/ijerph16040650