Increased Inequalities in Health Resource and Access to Health Care in Rural China

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Data Analysis
3. Results
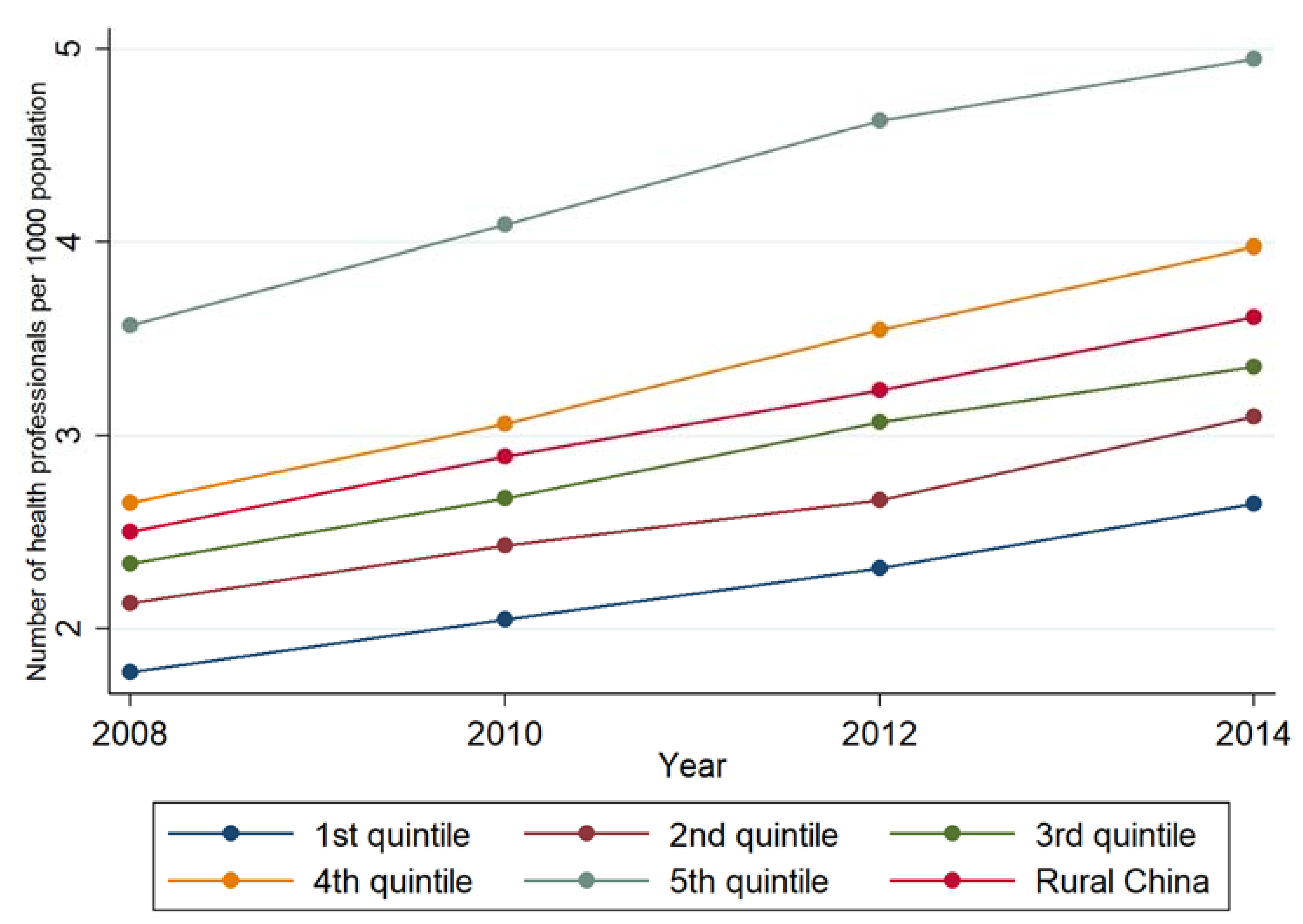
3.1. Description of the Inequality in Health Professionals per 1000 Population
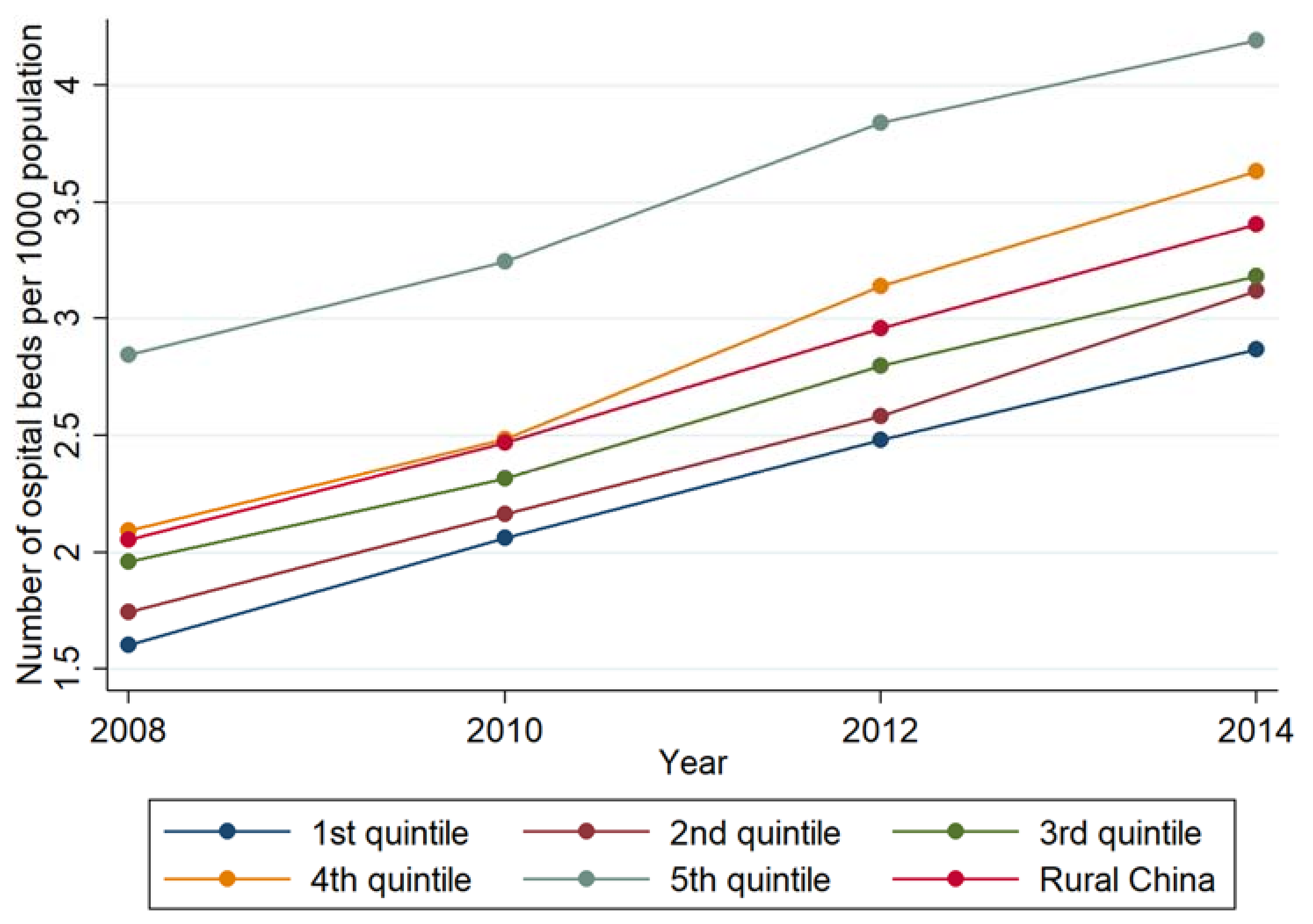
3.2. Description of the Inequality in Hospital Beds per 1000 Population
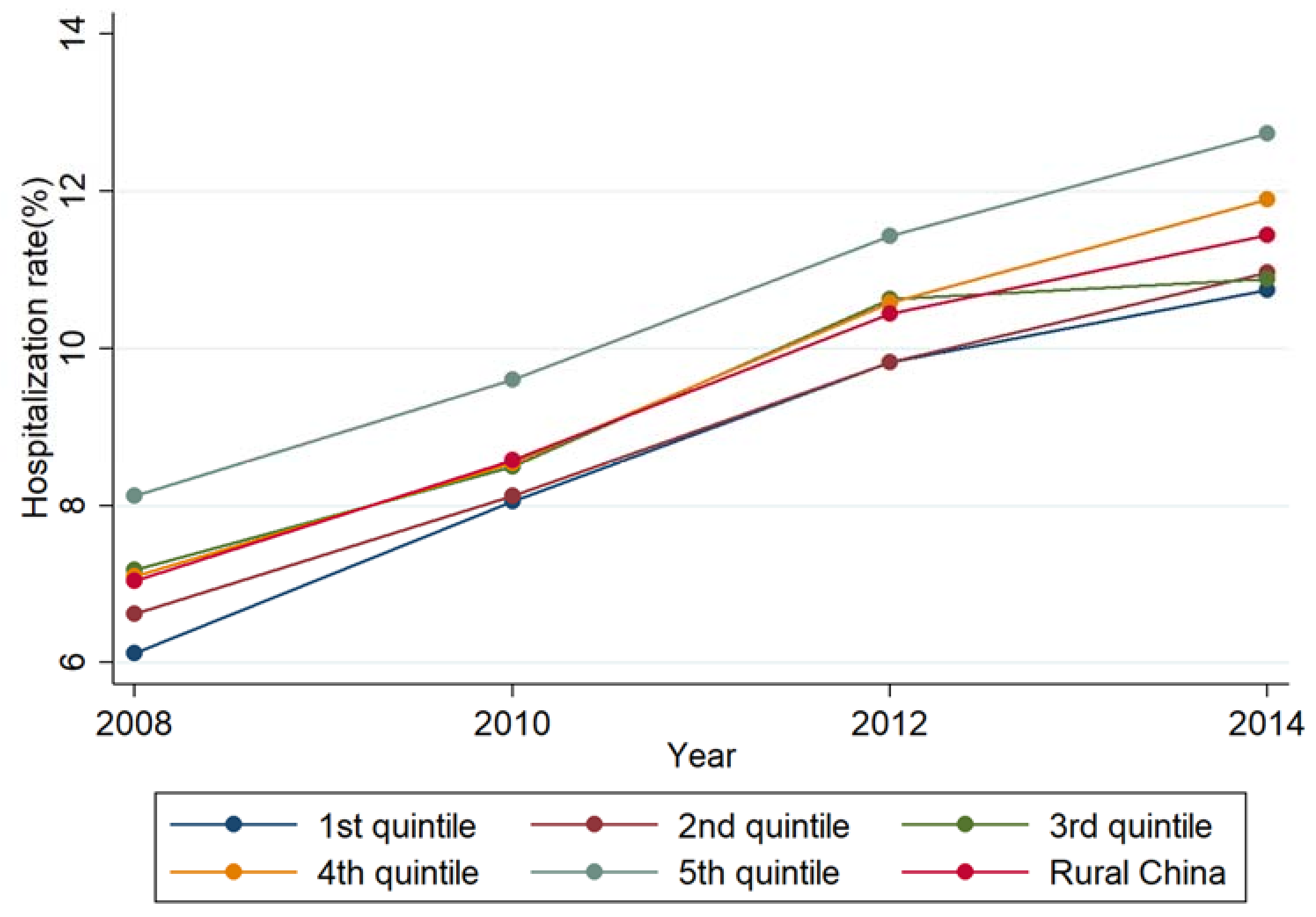
3.3. Description of the Inequality in the Hospitalization Rate
3.4. Changes in the Inequality in Health Resource and Access to Health Care
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- State Council. Opinion on Deepening the Health Care System Reform. 2009. Available online: http://www.nhfpc.gov.cn/tigs/s7846/200904/902e526039424a2ca87e8d78f307e9f5.shtml (accessed on 16 November 2018).
- Chen, R.; Zhao, Y.; Du, J.; Wu, T.; Huang, Y.; Guo, A. Health workforce equity in urban community health service of China. PLoS ONE 2014, 9, e115988. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Finance of People’s Republic of China. Tax Rebates and Transfer Payments in General Public Budget from Central Government to Local Governments by Region. Available online: http://yss.mof.gov.cn/2015js/201607/t20160713_2354956.html (accessed on 16 November 2018).
- Chen, Y.; Yin, Z.; Xie, Q. Suggestions to ameliorate the inequity in urban/rural allocation of healthcare resources in China. Int. J. Equity Health 2014, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Increasing Access to Health Workers in Remote and Rural Areas through Improved Retention: Global Policy Recommendations; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Hou, J.; Ke, Y. Addressing the shortage of health professionals in rural China: Issues and progress Comment on “Have health human resources become more equal between rural and urban areas after the new reform?”. Int. J. Health Policy Manag. 2015, 4, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Zhang, X.; Ding, Y.; Wang, D.; Lu, Z.; Yu, M. Inequality trends of health workforce in different stages of medical system reform (1985–2011) in China. Hum. Resour. Health 2015, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Wu, Q.; Zhang, Z.; Gao, L.; Ning, N.; Jiao, M.; Zakus, D. The impact of different benefit packages of Medical Financial Assistance Scheme on health service utilization of poor population in rural China. BMC Health Serv. Res. 2010, 10, 170. [Google Scholar] [CrossRef] [PubMed]
- Suhrcke, M.; McKee, M.; Rocco, L. Health investment benefits economic development. Lancet 2007, 370, 1467–1468. [Google Scholar] [CrossRef]
- World Bank. Financing Health Care: Issues and Options for China; World Bank: Washington, DC, USA, 1997. [Google Scholar]
- World Bank. World Development Report 2000: Attacking Poverty; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Ministry of Health. China Health Statistical Yearbook; Ministry of Health: Singapore, 2009.
- National Health and Family Planning Commission. China Health Statistical Yearbook; National Health and Family Planning Commission: Beijing, China, 2015.
- Anand, S.; Fan, V.Y.; Zhang, J.; Zhang, L.; Ke, Y.; Dong, Z.; Chen, L.C. China’s human resources for health: Quantity, quality, and distribution. Lancet 2008, 372, 1774–1781. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, W.; Zhou, H.; Xu, H.; Qu, Z.; Guo, M.; Wang, F.; Zhong, Y.; Gu, L.; Liang, X.; et al. How China’s new health reform influences village doctors’ income structure: Evidence from a qualitative study in six counties in China. Hum. Resour. Health 2015, 13, 26. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.N.; Tulloch, J. Incentives for retaining and motivating health workers in Pacific and Asian countries. Hum. Resour. Health 2008, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, P.; Han, S.; Zhao, L.; Fang, Z.; Zhang, Y.; Zou, X. What limits the utilization of health services among the rural population in the Dabie Mountains-evidence from Hubei province, China? BMC Health Serv. Res. 2014, 14, 379. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Evans, T.; Anand, S.; Boufford, J.I.; Brown, H.; Chowdhury, M.; Cueto, M.; Dare, L.; Dussault, G.; Elzinga, G.; et al. Human resources for health: Overcoming the crisis. Lancet 2004, 364, 1984–1990. [Google Scholar] [CrossRef]
- Guilbert, J.J. The World Health Report 2006: Working together for health. Educ. Health 2006, 19, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Wu, W. Study on Income Disparities in China. 2016. Available online: http://www.stats.gov.cn/tjzs/tjsj/tjcb/dysj/201608/t20160808_1385893.html (accessed on 9 October 2017). (In Chinese)
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 940–941. [Google Scholar]
- Shi, L.; Song, K.; Rane, S.; Sun, X.; Li, H.; Meng, Q. Factors associated with job satisfaction by Chinese primary care providers. Prim. Health Care Res. Dev. 2014, 15, 46–57. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Handbook on Health Inequality Monitoring: With a Special Focus on Low- and Middle-Income Countries; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Meng, Q.; Xu, K. Progress and challenges of the rural cooperative medical scheme in China. Bull. World Health Organ. 2014, 92, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Gao, J.; Fox, A.; Rao, K.; Xu, K.; Xu, L.; Zhang, Y. Measuring the equity of inpatient utilization in Chinese rural areas. BMC Health Serv. Res. 2011, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Henderson, G.E.; Akin, J.S.; Hutchinson, P.M.; Jin, S.G.; Wang, J.M.; Dietrich, J.; Mao, L.M. Trends in health services utilization in eight provinces in China, 1989–1993. Soc. Sci. Med. 1998, 47, 1957–1971. [Google Scholar] [CrossRef]
- Song, S.; Ma, X.; Zhang, L.; Yuan, B.; Meng, Q. Precision targeting for more equitable distribution of health professionals in rural China. Health Policy Plan. 2018, 33, 821–827. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| GDP per Capita Quintile | 2008 | 2010 | 2012 | 2014 | ||||
|---|---|---|---|---|---|---|---|---|
| Number of Counties | Number of the Population (10,000) | Number of Counties | Number of the Population (10,000) | Number of Counties | Number of the Population (10,000) | Number of Counties | Number of the Population (10,000) | |
| 1st quintile (The poorest) | 375 | 15,816 | 362 | 14,109 | 378 | 18,045 | 396 | 17,950 |
| 2nd quintile | 375 | 19,026 | 362 | 18,173 | 378 | 19,868 | 395 | 19,572 |
| 3rd quintile | 376 | 18,918 | 361 | 17,814 | 377 | 19,057 | 396 | 20,015 |
| 4th quintile | 375 | 17,935 | 362 | 17,615 | 378 | 18,176 | 395 | 18,827 |
| 5th quintile (The richest) | 375 | 17,676 | 362 | 17,707 | 378 | 18,018 | 396 | 19,375 |
| Total | 1876 | 89,371 | 1809 | 85,418 | 1889 | 93,164 | 1978 | 95,739 |
| Dependent Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| The Density of Health Professionals | The Density of Hospital Beds | The Hospitalization Rate | |
| GDP per capita quintile | |||
| 2nd | 0.028 | 0.161 *** | 0.849 *** |
| 3rd | 0.152 * | 0.271 *** | 1.202 *** |
| 4th | 0.043 | 0.175 * | 1.015 *** |
| 5th | −0.130 | 0.162 | 0.767 ** |
| Year | |||
| 2010 | 0.308 *** | 0.468 *** | 2.269 *** |
| 2012 | 0.498 *** | 0.892 *** | 3.756 *** |
| 2014 | 0.865 *** | 1.328 *** | 4.782 *** |
| GDP per capita quintile * year | |||
| 2nd *year of 2010 | 0.033 | −0.050 | −0.755 *** |
| 2nd *year of 2012 | 0.078 | −0.088 * | −0.700 *** |
| 2nd *year of 2014 | 0.155 ** | −0.014 | −0.649 ** |
| 3rd *year of 2010 | −0.003 | −0.131 *** | −0.986 *** |
| 3rd *year of 2012 | 0.165 *** | −0.115 ** | −0.631 ** |
| 3rd *year of 2014 | 0.151 ** | −0.126 * | −1.073 *** |
| 4th *year of 2010 | 0.068 | 0.136 *** | −1.085 *** |
| 4th *year of 2012 | 0.385 *** | 0.092 | −0.401 |
| 4th *year of 2014 | 0.532 *** | 0.193 * | −0.122 |
| 5th *year of 2010 | 0.249 *** | −0.020 | −0.659 *** |
| 5th *year of 2012 | 0.667 *** | 0.204 *** | −0.127 |
| 5th *year of 2014 | 0.754 *** | 0.169 ** | −0.152 |
| Intercept | 2.797 *** | 2.163 *** | 6.270 *** |
| sigma_u | 1.634 | 1.397 | 4.256 |
| sigma_e | 0.707 | 0.695 | 2.272 |
| rho | 0.842 | 0.802 | 0.778 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, S.; Yuan, B.; Zhang, L.; Cheng, G.; Zhu, W.; Hou, Z.; He, L.; Ma, X.; Meng, Q. Increased Inequalities in Health Resource and Access to Health Care in Rural China. Int. J. Environ. Res. Public Health 2019, 16, 49. https://doi.org/10.3390/ijerph16010049
Song S, Yuan B, Zhang L, Cheng G, Zhu W, Hou Z, He L, Ma X, Meng Q. Increased Inequalities in Health Resource and Access to Health Care in Rural China. International Journal of Environmental Research and Public Health. 2019; 16(1):49. https://doi.org/10.3390/ijerph16010049
Chicago/Turabian StyleSong, Suhang, Beibei Yuan, Luyu Zhang, Gang Cheng, Weiming Zhu, Zhiyuan Hou, Li He, Xiaochen Ma, and Qingyue Meng. 2019. "Increased Inequalities in Health Resource and Access to Health Care in Rural China" International Journal of Environmental Research and Public Health 16, no. 1: 49. https://doi.org/10.3390/ijerph16010049