1. Introduction
Phthalates are diesters of phthalic acid with a wide variety of industrial applications. There is an interest in the safety evaluation of phthalate exposure because these compounds are ubiquitous environmental contaminants, resulting in widespread human exposure, with varied toxicological endpoints. Several phthalates have been cataloged as ubiquitous environmental endocrine-disrupting chemicals (EDCs) and that is why there is a strong demand for their reliable determination. Phthalates with endocrine-disrupting properties, such as di(2-ethylhexyl phthalate (DEHP), dibutyl phthalate (DBP) and butyl benzyl phthalate (BBP), are suspected to interfere with developmental androgen action, possibly leading to adverse effects on reproductive function [
1,
2]. Phthalates have been classified as “chemicals of concern” by the U.S. EPA [
3]. In addition, the European Chemicals Agency’s Committee for Risk Assessment (RAC) recommends that the trends in exposure to phthalates (in consumer products, body burden based on biomonitoring, content in and migration from articles, etc.) should be monitored [
4]. Certain phthalates, like DBP, BBP, DEHP, diethyl phthalate (DEP), and dimethyl phthalate (DMP) have numerous industrial applications and uses including food packaging, personal-care products, pharmaceuticals, medical devices, building materials, nutritional supplements, cleaning materials, solvents, adhesives, paints, lacquers, insecticides, children’s toys, and children’s school supplies which makes them omnipresent in the environment [
5,
6,
7]. In these products phthalates are not chemically bound to the polymer matrices and therefore might easily migrate to the food and surrounding environment which leads to exposure of humans by multiple routes including mainly ingestion, inhalation and dermal uptake throughout their lifetime beginning in fetal stages [
8,
9,
10].
Several animal studies reported that exposure to DBP, BBP, DEP, and DEHP has been associated with reproductive developmental damage, endocrine disruption and neurodevelopmental toxicity, and the European Food Safety Authority (EFSA) determined the critical effects of DEHP, BBP and DBP to relate to reproduction as derived from data from reproduction/developmental toxicity studies [
11,
12,
13,
14,
15,
16,
17]. In addition, epidemiological studies, in spite of their limitations, suggest that there are strong and rather consistent indications that phthalates may affect reproductive outcome and children’s health [
18]. Although phthalates have short biological half-lives, and are quickly excreted from the body as their respective metabolites (e.g., monoesters), particular consideration has been given to phthalates for years, especially due to their ubiquitous existence in the environment, the size of the population exposed and their endocrine-disrupting properties [
18,
19,
20,
21]. Phthalates can undergo metabolism in two stages in the human body namely phase I (hydrolysis, oxidation) catalyzed by esterases and lipases and phase II (conjugation) catalyzed by uridine 5′-diphosphoglucuronyl transferase enzyme. Lower molecular weight phthalates such as DEP, DMP and DBP will undergo phase I biotransformation to become hydrolytic monoester metabolites while higher molecular weight phthalates such as DEHP first will hydrolyze into a monoester and that can further be oxidized to secondary oxidized metabolites. Hydrolytic monoesters and secondary oxidized metabolites are further metabolized through phase II biotransformation to produce glucuronide conjugates. The metabolites are more soluble in water than the parent compounds and are excreted in urine [
22,
23,
24].
Young children, as a result of their proportionally higher rates of breathing, eating and drinking, are likely to be more exposed per unit of body weight than adults [
25]. A Canadian study reported children to display significantly higher urinary concentrations of metabolites of DEHP, DBP and BBP than adolescents and adults [
26]. Similar results were also observed in German school children and the U.S. National Health and Nutrition Examination Survey (NHANES) and Demonstration of a study to Co-ordinate and Perform Human Biomonitoring on a European Scale’ (DEMOCOPHES) study [
27,
28], which is also in concordance with the results of other studies [
29,
30,
31,
32].
Human biomonitoring (HBM) is an important tool in the investigation of phthalate exposure and risk assessment since it reflects the phthalate body burden by measuring specific metabolites especially in the urine [
33,
34]. Although phthalate metabolites can be detected in several body fluids such as amniotic fluid, breast milk, saliva and seminal plasma [
35,
36,
37,
38,
39], the presence of enzymes such as esterases in these matrices can cleave phthalates converting the phthalates samples from external sources into their monoesters [
40]. In general, in epidemiological studies urine has been considered the matrix of choice for non-persistent chemicals, such as phthalates because urinary concentrations of especially their metabolites are usually considerably adequate biomarkers of exposure [
21,
41,
42]. Therefore, the measurement of phthalate metabolites in urine as a valuable approach in environmental epidemiology studies, represents an integrated measure of exposure to phthalates from all possible known and unknown sources and routes, and incorporates individual variability in exposure profiles [
21,
43]. Forward and backward methods can be used for exposure assessment with the latter one being based on interpretation of HBM data [
40]. Forward analysis uses measured intake doses to predict body burden while backward (reverse) analysis uses urinary HBM data to reconstruct past exposure by calculating estimated daily intake (EDI) [
44]. One of the simplest methods to convert urinary HBM concentrations into exposure doses (e.g., EDIs) is based on the fractional urinary excretion (F
UE), defining the fraction of the dose that ends up as a defined biomarker in a relevant matrix. Thus, the F
UE can be used for reverse dosimetry and convert the urinary level of a biomarker into an oral dose level. In this approach a correction for urinary dilution can be made applying the urine volume-adjustment method or the creatinine adjustment approach [
40].
When considering the use of urinary biomarkers for estimation of phthalate exposure it is also of importance to consider combined exposure, since disregard of combination effects may lead to underestimation of risks [
45]. For instance with a mixture of two phthalates, DBP and DEHP, which act through a common mode of action by suppressing testosterone synthesis, the combined effects were shown to be additive [
46]. This illustrates the importance of cumulative risk assessment (CRA), considering the effects of combined exposure. In the case of phthalates, chronic co-exposure may constitute a risk of anti-androgenic effects during the stages of puberty due to hormonal changes and development of reproductive organs [
47]. Therefore, the U.S. National Research Council in recent recommendations has reported that phthalates meet the conditions necessary to warrant a mixture risk approach [
7].
The aim of the present study was to determine the extent of exposure to the phthalates BBP, DBP, DEHP, DEP and DMP, for the first time, among children and adolescents in Iran, and to estimate for this population the risk of exposure to the individual phthalates as well as to the combined exposure to the anti-androgenic phthalates BBP, DBP and DEHP.
4. Discussion
In this study, we used a human biomonitoring approach to determine EDI values for five different phthalates in Iranian children and adolescents, based on phthalate metabolite levels in urine spot samples, and performed an associated risk assessment. For this risk assessment the EDI values obtained were compared to two sets of health-based guidance values as acceptable levels of exposure, derived based on anti-androgenic effects as the critical endpoint, including TDI values established by EFSA [
63,
64,
65] and RfD-AA values determined by Kortenkamp and Faust [
62] using the HQ approach. The evaluation also included a combined risk assessment for exposure to phthalate mixtures using the HI approach.
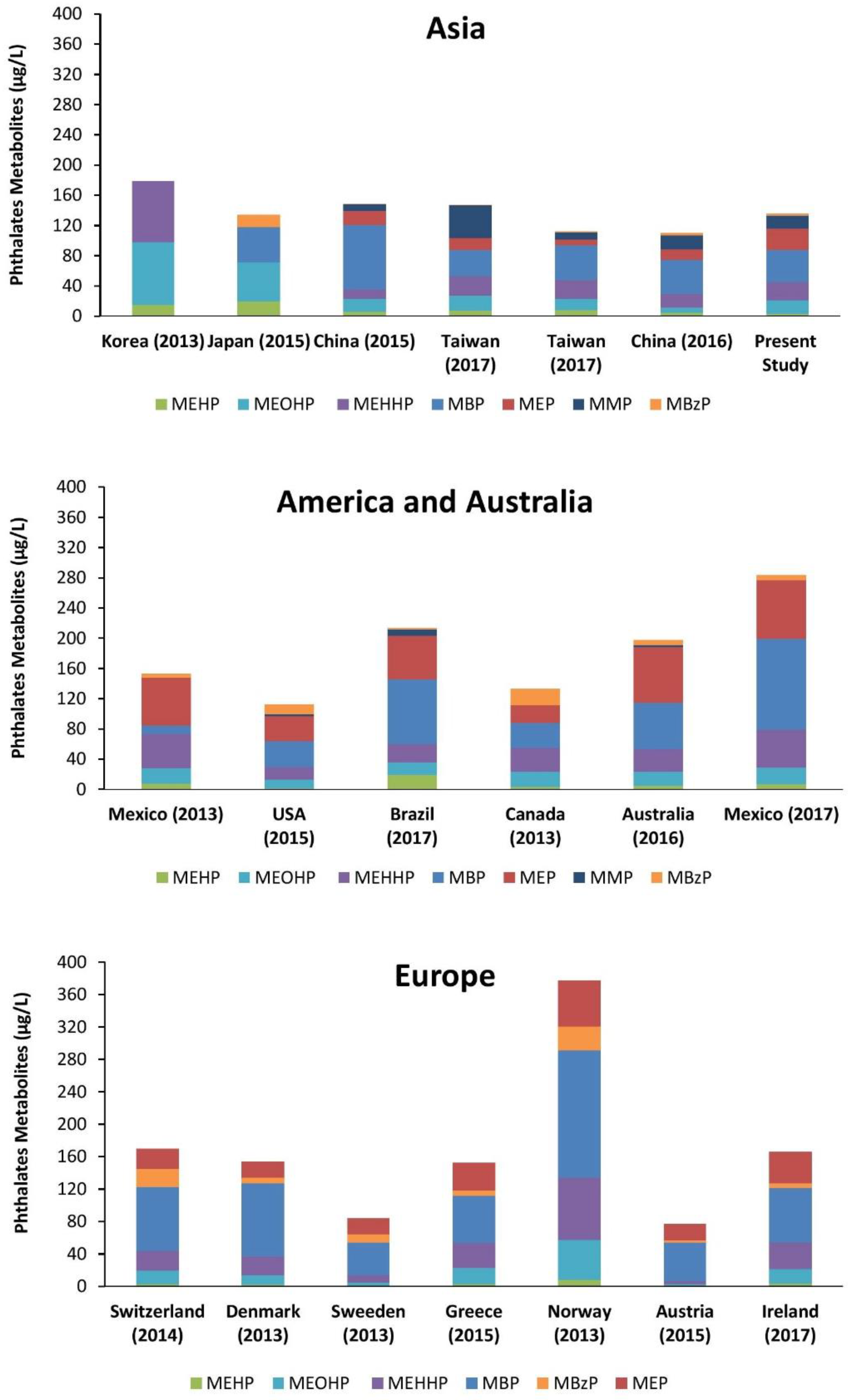
The results of this study show that Iranian children and adolescents are ubiquitously exposed to certain phthalates included in the study, namely DEHP, DBP, DEP and DMP. Our findings showed that the levels of the urinary biomarkers for phthalate exposure varied in the order MBP > MEP > DEHP metabolites > MMP > MBzP. For comparison the results from other studies on exposure of children and adolescents to phthalates as reported in the literature on a worldwide scale are presented in
Figure 3. The urinary metabolite patterns obtained in our study are especially similar to the urinary phthalate metabolite patterns reported for children and adolescents from other countries such as Taiwan, China, Brazil and Greece [
76,
77,
78]. All the reviewed studies were population-based cross-sectional studies conducted among minors (<18 years old) after 2010. Consistent with our results, among all studies the lowest urinary concentrations were observed for MBzP. This reveals that children and adolescents have relatively lower exposure to BBP compared to other phthalates, and that this is the case in several countries over the world, probably reflecting that the application and sources of exposure to BBP are comparable [
4]. The urinary metabolite patterns in our study revealed also differences to urinary metabolite patterns reported in several of the other countries for which data were available (
Figure 3). Such differences may reflect differences in patterns of exposure in different countries due to country specific use patterns for phthalates in relevant products, differences in food consumption habits, and/or differences in socio-economic strata [
79]. These differences may also reflect changes in the phthalate content of specific products over time, and further may be the result of public pressure and political regulations [
21]. For example in 2004, the European Union (EU) has banned the use of certain phthalates including DEHP, DBP and BBP from cosmetics and food packaging (Directive 2004/93/EC) and in 2005 from all toys and childcare products (Directive 2005/84/EC) [
80]. Furthermore, comparison of data from two studies in Denmark with sampling in the period 2006 to 2008 or more recent in 2011 revealed a decreasing trend in phthalate exposure [
32,
81]. Reported urinary concentrations for BBP, DBP and DEHP in the studies conducted by [
32,
81] (sampling time between 2006–2008 on 517 boys aged 6 to 19 years) are 1.5, 6.8 and 2 times higher than the results of the study in 2011 on 143 participants aged group of 6 to 11. Likewise, in another study with the same sampling year conducted by Frederiksen et al. on 725 Danish girls (ranged from 5.6 to 19.1 years) the level of phthalates are higher than the latest study carried out by Frederiksen et al. in 2013 [
32]. This decreasing trend in phthalate exposure also becomes apparent when comparing two studies in the USA one with 2005–2006 and one with 2009–2010 as sampling periods [
82]. In this comparison, the study populations were comparable with regard to age group, sex, sample size and country. This reduction in phthalate exposure is likely attributable to prohibition of usage of specific phthalates. In addition, dietary habits and life styles play an important role in exposure to phthalates [
83]. One remarkable difference in the urinary phthalate metabolite pattern between the Iranian children and adolescents and data from several other countries was the fact that the Iranian samples revealed the presence of MMP, the metabolite of DMP. This metabolite was also observed to a significant extent in 6 to 18 year old children in China and Taiwan [
77,
84]. The possible sources of this DMP exposure are not clearly known. A study conducted in China suggested that the concentrations of DMP in milk products, instant noodle, cakes, cookies and salt eggs were higher than those in other foods [
85]. DMP was detected in some food samples such as yogurt, fish, and spice from Europe and North America as well [
86].
According to the results of the current study and in line with results from related studies, the concentrations of the oxidative metabolites of DEHP (MEHHP and MEOHP) appeared to be excreted in several-fold higher concentrations than MEHP the metabolite resulting from hydroxylation of DEHP (
Figure 3). Although metabolic abilities may differentiate between age groups, previous studies already showed that these oxidative metabolites could be more sensitive biomarkers for monitoring exposure to DEHP than MEHP [
95]. In addition, previous studies reported that children had a particularly faster relative metabolic rate (RMR) than adults, specifically for the first step of DEHP metabolism (RMR1: ratio MEHP/MEHHP) [
61]. The results from the present study also corroborate that RMR1 is higher than RMR2, because the transformation of MEHP to MEHHP (as expressed by RMR1) appears to be positively related with age implying a reduced ability of DEHP metabolism at lower ages [
94,
95].
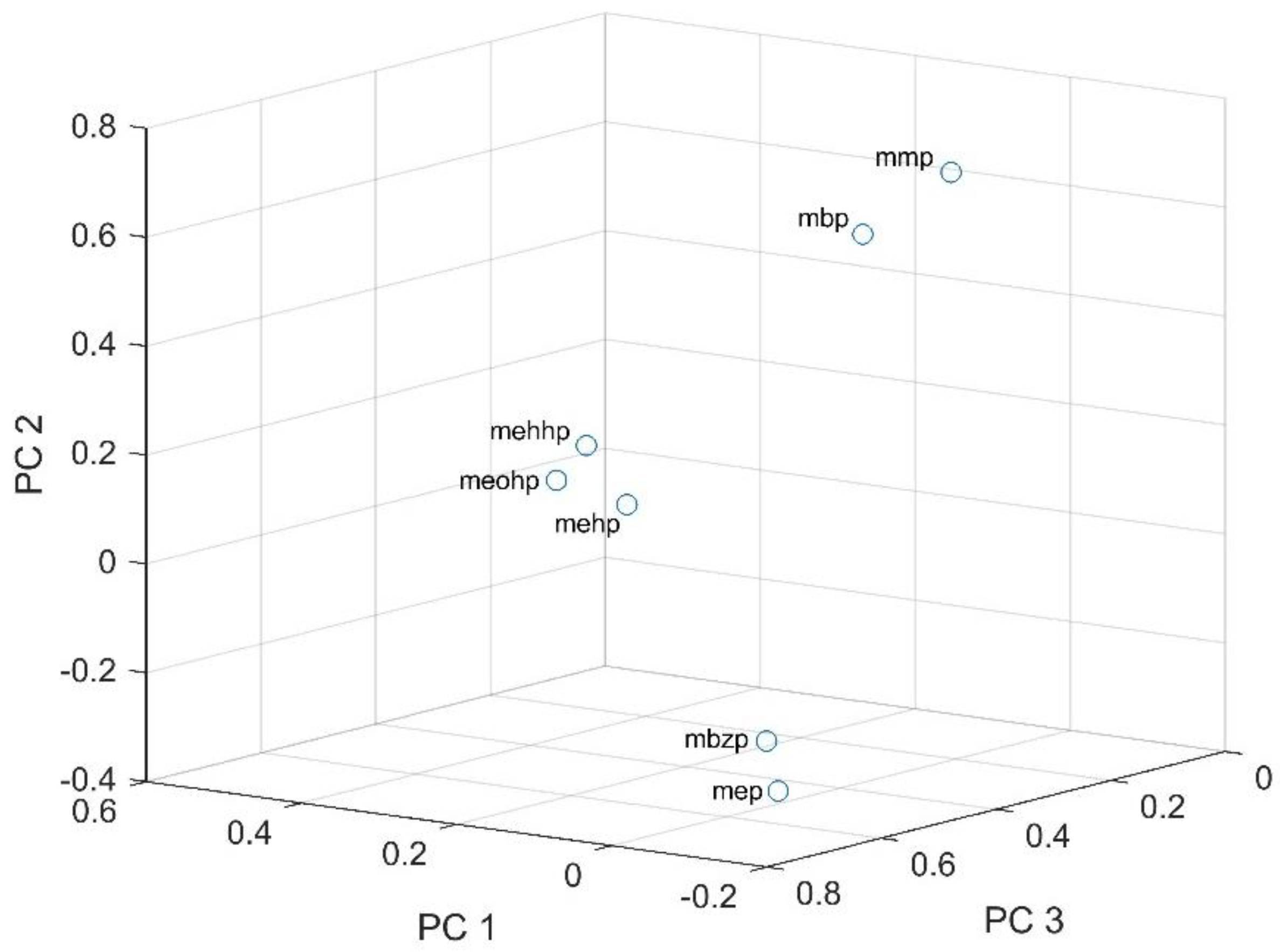
Furthermore, the urinary biomarker patterns confirmed the observation that Iranian children and adolescents, like children and adolescents in other countries, are simultaneously exposed to mixtures of phthalates. The PCA analysis indicated grouping of some phthalates (DEHP, DBP, DMP) and thus pointed at combined exposure from similar sources, like food packaging material and several consumer products, leading to combined exposure to DBP, DMP, and DEHP, and or/similar ADME [
86]. In contrast, MEP and MBzP were positively correlated with PC3, which could be an indication of the same origin of exposure via for example personal care-hygienic products and cosmetics [
96] which may explain why the concentrations of these two phthalates were higher in girls with statistically significant differences compared to values for boys. Generally, multiple phthalates correlate with one another if they are used in the same applications and thus share similar sources of exposure, and again there may be some other existing unknown sources of exposure [
96].
In a review conducted by Smith et al., aiming to prioritize hazardous chemicals in children’s products based on the U.S. Children’s Safe Product Act (CSPA) database, the relationships between phthalate exposure and adverse health effects was investigated [
96]. Four endpoints including endocrine disruption, reproductive and developmental toxicity, carcinogenicity and neurotoxicity were selected as relevant health endpoints in their framework. The analysis confirmed that toxicity drives a substantial part of the differences in health effects caused by the chemicals. Phthalates, including DEHP, BBP, and DBP were found to raise a concern because of reproductive and developmental toxicity, which would be in line with their activity as anti-androgens [
96].
Across the whole study population of the present study, the highest median phthalates intakes were for DEHP within the range of 0.58 to 17.85 µg/kg body weight/day and DBP within the range of 0.2 to 3.1 µg/kg body weight/day. Median BBP daily intakes were lowest, ranging from 0.01 to 0.23 µg/kg body weight/day.
The phthalate exposure profile was consistent with previous studies. These studies also revealed that levels of most urinary phthalate metabolites detected for children were found to decrease with increasing age [
97,
98,
99]. However, no significant differences were found between the two age groups in our study.
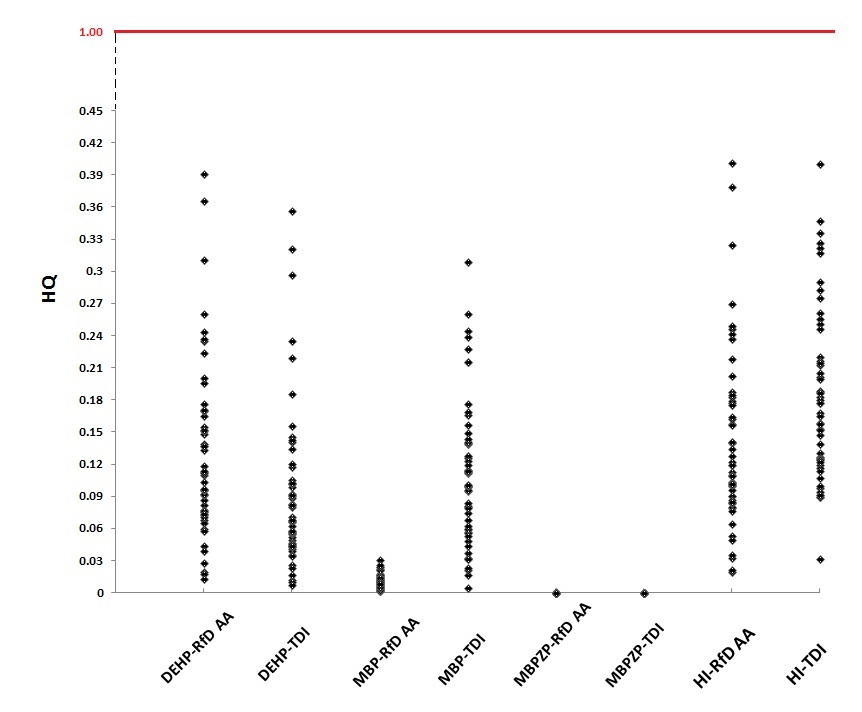
According to the results of our study, DEHP is the compound with the highest median HQ of 0.14 when based on the RfD-AA for anti-androgenic effects, whereas based on the TDI approach DBP with a median of 0.11 is the compound with the highest HQ value. However, since all HQ values, and also the HI values for combined exposure were markedly below 1.0 it can be concluded that for none of the surveyed participants the HQ and HI values raised a concern. It is also of interest to note that for the risk assessment performed, HQs and HIs were not calculated based on U.S. EPA RfDs, since these health based-guidance values are not based on endpoints that share an underlying mode of action. However, even when using U.S. EPA RfD values, EDI values for investigated phthalates in the present study would remain far below these health-based guidance values and thus corroborate that the exposure does not raise a concern. This result is in contrast to those from a study by Wittassek et al. (2007) conducted among German children (
n = 239, 2–14 years old), in which some individuals showed DEHP exposure estimates based on HBM data that exceeded the U.S. EPA RfD for DEHP (20 μg/kg body weight/day) [
100]. More so, Kim et al. (2014) in Seoul, using the U.S. EPA RfD value, approximately 3–8% of elementary school children (
n = 39, aged 9–12 years) showed a HQ greater than 1.0 for DEHP exposure, using HBM data for exposure estimation [
101]. The HI approach used in the present study for combined risk assessment has been previously used for combined risk assessments on phthalates in the literature. In a study conducted by Søeborg et al. (2012) [
102] 129 Danish children and adolescents, 19 children exceeded the HI value of 1.0 determined based on EFSA TDI values for the anti-androgenic phthalates (DBP, BBP and DEHP), while one child exceeded the HI value of 1.0 based on the RfD-AA values [
102]. Dewalque et al. (2014) also reported HI values based on TDIs exceeding the value of 1.0 in 25% of the children in a study on phthalate exposure of 52 male and female children (1–12 years) in Belgium [
103]. A study conducted among Austrian children aged 7–15 years on cumulative risk assessment for combined phthalate exposure demonstrated that in 4.2% of children the HI values calculated based on TDIs were more than 1.0 [
47]. In the present study, the HQ values for DBP based on EFSA-TDI values were higher compared to the estimated HQs based on RfD-AA values. This discrepancy is due to the fact that the underlying RfD-AA value used for DBP by [
62] is 10 times higher than the relevant EFSA-TDI value (
Table 2). However, DEHP was associated with the highest HQ value (~0.6) for Iranian children in RfD-AA approache. Thus, obviously, the HQ and HI values and resulting conclusions may to some extend depend on health-based guidance values used to calculate these values.
Regarding the MCR approach, the cumulative exposures of concern mainly originated from one of the three anti-androgenic phthalates including DBP and DEHP. The MCR approach has been applied to biomonitoring data on mixtures of dioxin-like chemicals [
73], exposures to mixtures of chemicals in water [
74,
104,
105], and mixtures in residential indoor air [
106]. A recent study conducted by [
75] was the first publication that used the MCR approach in a biomonitoring study on phthalates collecting data on six phthalates. The results of that study showed that HI values in the surveyed participants averaged 0.15 (HI < 1.0). Only 21 (0.8%) of the participants had HI values >1.0 [
75]. Reyes and Price, reported that for about 43% of these participants with HI >1.0, a potential risk would have been overlooked if only single chemical based risk assessment (HQ) rather than a combined exposure approach (HI) was performed. In addition, the MCR calculated among the participants ranged from 1.1 to 3.6, which indicated that a single or a subgroup of phthalates like DEHP and DBP had a dominant influence on the participant’s value of HI [
75]. Also in the present study, the HI values were dominated by specific phthalates, being DBP when determining HI values based on TDI values, and DEHP when determining HI values based on RfD-AA values.
Altogether, it can be concluded that, in line with other studies, our subjects were not exposed to single phthalates, but rather to a mixture of phthalates. In a previous study prioritizing chemicals and products, DBP, BBP and DEHP were identified as the highest priority chemicals based on both exposure and toxicity scores [
96]. Metabolites of these priority phthalates were also detected in the urinary samples of the present study and were shown to contribute to the combined HI values. This corroborates that biomonitoring data indicate that the overall combined exposure to phthalates of Iranian children does not raise a concern, while reduction of exposure is best focused on DEHP and DBP that showed the highest HQ.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}