Signs, Fines and Compliance Officers: A Systematic Review of Strategies for Enforcing Smoke-Free Policy

 ,
,
Abstract
:1. Introduction
Aims
- the effectiveness of enforcement strategies at increasing compliance with and implementation of smoke-free policies;
- the circumstances associated with compliance with smoke-free policies (other than enforcement strategies).
2. Methods
2.1. Search Strategy
2.2. Definitions
2.3. Inclusion Criteria
2.4. Data Extraction
2.5. Methodological Quality Assessment
2.6. Data Synthesis
3. Results
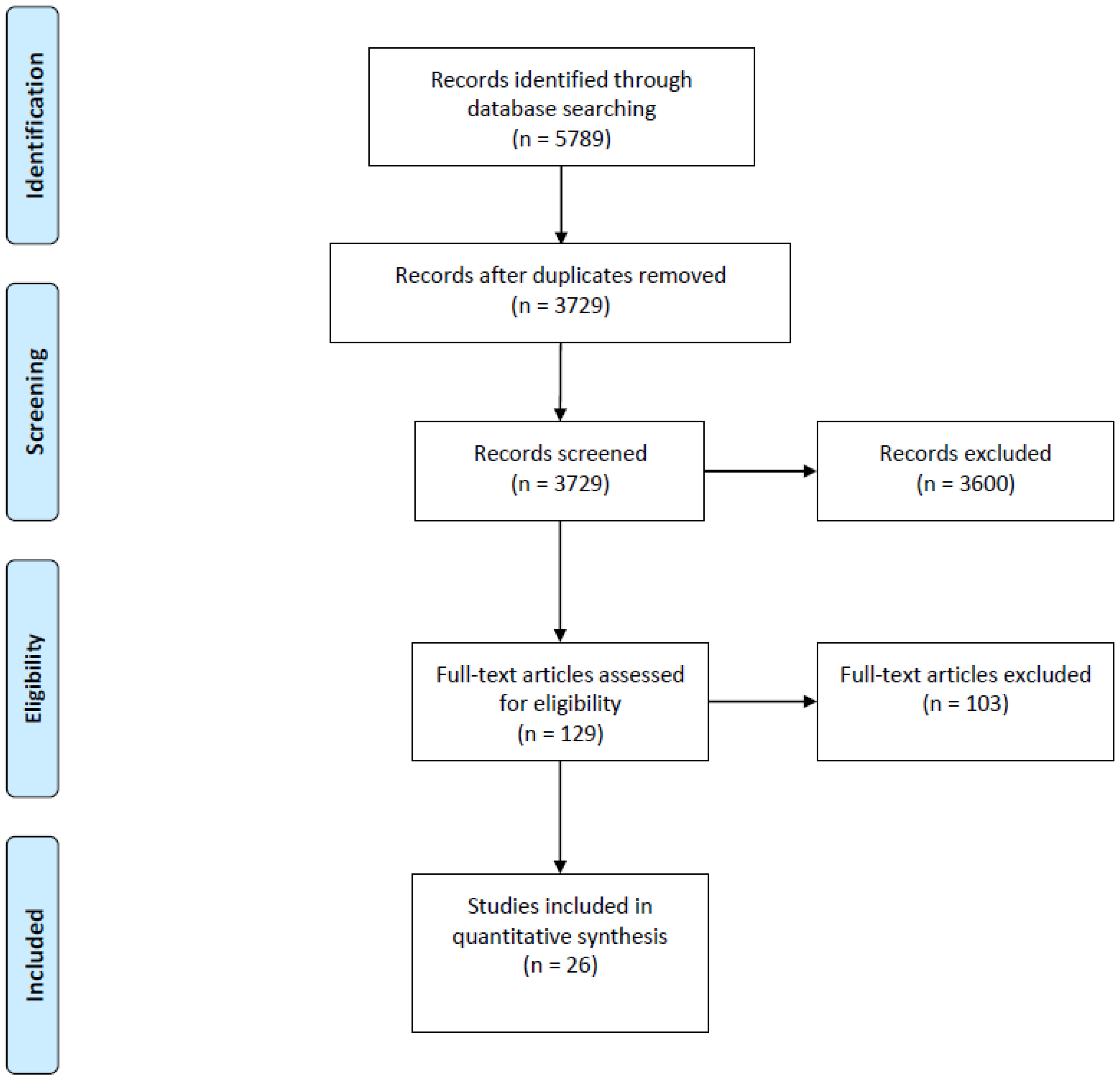
3.1. Search Results
3.2. Study Characteristics
3.2.1. Effectiveness of Enforcement Strategies at Increasing Compliance and Implementation of Smoke-Free Policies
3.2.2. Circumstances Other Than Enforcement Strategies That Are Associated with Compliance
3.2.3. Methodological Quality Assessment
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- World Health Organization. WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Hyland, A.; Barnoya, J.; Corral, J.E. Smoke-free air policies: Past, present and future. Tob. Control 2012, 21, 154–161. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tobacco Control Policies and Interventions: Protecting People from Tobacco Smoke; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Kelleher, C.C.; Frazer, K. An international smoking ban-how many lives will be saved? Curr. Atheroscler. Rep. 2014, 16, 418. [Google Scholar] [CrossRef] [PubMed]
- Frazer, K.; Callinan, J.E.; McHugh, J.; van Baarsel, S.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2016, 2, Cd005992. [Google Scholar] [CrossRef] [PubMed]
- Ragg, M.; Ahmed, T. Smoke and Mirrors: A Review of the Literature on Smoking and Mental Illness; Tackling Tobacco Program Research Series No. 1; Cancer Council NSW: Sydney, Australia, 2008. [Google Scholar]
- Mons, U.; Nagelhout, G.E.; Guignard, R.; McNeill, A.; van den Putte, B.; Willemsen, M.C.; Brenner, H.; Potschke-Langer, M.; Breitling, L.P. Comprehensive smoke-free policies attract more support from smokers in Europe than partial policies. Eur. J. Public Health 2012, 22, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC. Evaluating the Effectiveness of Smoke-Free Policies; IARC Handbooks of Cancer Prevention, Tobacco Control; International Agency for Research on Cancer: Lyon, France, 2009; Volume 13, p. 334. [Google Scholar]
- World Health Organization and Tobacco Free Initiative. Protection from Exposure to Second-Hand Tobacco Smoke: Policy Recommendations; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- McCrabb, S.; Baker, A.L.; Attia, J.; Balogh, Z.J.; Lott, N.; Palazzi, K.; Naylor, J.; Harris, I.A.; Doran, C.M.; George, J.; et al. Hospital Smoke-Free Policy: Compliance, Enforcement, and Practices. A Staff Survey in Two Large Public Hospitals in Australia. Int. J. Environ. Res. Public Health 2017, 14, E1358. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.; Thomson, G.; Wilson, N.; Waa, A.; Bullen, C.; O’Dea, D.; Gifford, H.; Glover, M.; Laugesen, M.; Woodward, A. After the smoke has cleared: Evaluation of the impact of a new national smoke-free law in New Zealand. Tob. Control 2008, 17, e2. [Google Scholar] [CrossRef] [PubMed]
- Jackson, N.; Waters, E. Criteria for the systematic review of health promotion and public health interventions. Health Promot. Int. 2005, 20, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.J.; Stearns, J.N.; Kovach, R.G.; Harrar, S.W. Enforcing an outdoor smoking ban on a college campus: Effects of a multicomponent approach. J. Am. Coll. Health 2009, 58, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Ballbe, M.; Nieva, G.; Mondon, S.; Pinet, C.; Bruguera, E.; Saltó, E.; Fernández, E.; Gual, A. Smoke-free policies in psychiatric services: Identification of unmet needs. Tob. Control 2012, 21, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Nieva, G.; Mondon, S.; Pinet, C.; Bruguera, E.; Saltó, E.; Fernández, E.; Gual, A. Implementing and complying with the Smoke-free Hospitals Project in Catalonia, Spain. Eur. J. Cancer Prev. 2006, 15, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, N.A.; Bourne, D.; Rosen, A.; Locke, J.A.; Schelling, T.C. Workplace compliance with a no-smoking law: A randomized community intervention trial. Am. J. Public Health 1992, 82, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, N.A.; Stoto, M.A.; Schelling, T.C. Do businesses comply with a no-smoking law? Assessing the self-enforcement approach. Prev. Med. 1994, 23, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Boris, N.W.; Johnson, C.C.; Huang, S.; Myers, L.; Andrew, K.; Webber, L.S. Targeting school tobacco policy: Lessons from the Acadiana Coalition of Teens against Tobacco (ACTT). Health Promot. Pract. 2009, 10, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Record, R.A.; Helme, D.; Savage, M.W.; Harrington, N.G. Let’s Clear the Air: A campaign that effectively increased compliance with a university’s tobacco-free policy. J. Appl. Commun. Res. 2017, 45, 79–95. [Google Scholar] [CrossRef]
- Fallin, A.; Johnson, A.O.; Rikerm, C.; Cohen, E.; Rayens, M.K.; Hahn, E.J. An intervention to increase compliance with a tobacco-free university policy. Am. J. Health Promot. 2013, 27, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Russette, H.C.; Harris, K.J.; Schuldberg, D.; Green, L. Policy compliance of smokers on a tobacco-free university campus. J. Am. Coll. Health 2014, 62, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Nimpitakpong, P.; Dhippayom, T.; Chaiyakunapruk, N.; Aromdee, J.; Chotbunyong, S.; Charnnarong, S. Compliance of drugstores with a national smoke-free law: A pilot survey. Public Health 2010, 124, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Ravara, S.B.; Castelo-Branco, M.; Aguiar, P.; Calheiros, J.M. Compliance and enforcement of a partial smoking ban in Lisbon taxis: An exploratory cross-sectional study. BMC Public Health 2013, 13, 134. [Google Scholar] [CrossRef] [PubMed]
- Hyland, A.; Cummings, K.M.; Wilson, M.P. Compliance with the New York City Smoke-Free Air Act. J. Public Health Manag. Pract. 1999, 5, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lawn, S.; Campion, J. Factors associated with success of smoke-free initiatives in Australian psychiatric inpatient units. Psychiatr. Serv. 2010, 61, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Peterson, E.; Knight, S.; Hiller, M.; Pelletier, A. Survey of restaurants regarding smoking policies. J. Public Health Manag. Pract. 2004, 10, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Wang, C.; Chen, H.; Hajek, P. Making hospitals in China smoke-free: A prospective study of implementing the new standard. Nicotine Tob. Res. 2013, 15, 2076–2080. [Google Scholar] [CrossRef] [PubMed]
- Jancey, J.; Bowser, N.; Burns, S.; Crawford, G.; Portsmouth, L.; Smith, J. No smoking here: Examining reasons for noncompliance with a smoke-free policy in a large university. Nicotine Tob. Res. 2014, 16, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Paek, H.J.; Hove, T.; Oh, H.J. Multilevel analysis of the impact of school-level tobacco policies on adolescent smoking: The case of Michigan. J. Sch. Health 2013, 83, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Glasgow, R.E.; Corbett, K.; Topor, M. Compliance with worksite nonsmoking policies: Baseline results from the COMMIT study of worksites. Am. J. Health Promot. 1992, 7, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Thomas, D.R.; Govindasamy, E.; Murhekar, M.V. Monitoring smoke-free laws in restaurants and educational institutions in chennai, India. Natl. Med. J. India 2014, 27, 76–78. [Google Scholar] [PubMed]
- Reis, M.F.; Namorado, S.; Aguiar, P.; Precioso, J.; Nunes, B.; Veloso, L.; Santos, S.; Miguel, J.P. Patterns of adherence to and compliance with the Portuguese smoke-free law in the leisure-hospitality sector. PLoS ONE 2014, 9, e102421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardavas, C.I.; Agaku, I.; Patelarou, E.; Anagnostopoulos, N.; Nakou, C.; Dramba, V.; Giourgouli, G.; Argyropoulou, P.; Antoniadis, A.; Gourgoulianis, K.; et al. Ashtrays and Signage as Determinants of a Smoke-Free Legislation’s Success. PLoS ONE 2013, 8, e72945. [Google Scholar] [CrossRef] [PubMed]
- Eby, L.T.D.T.; Laschober, T.C. Perceived implementation of the Office of Alcoholism and Substance Abuse Services (OASAS) tobacco-free regulation in NY State and clinical practice behaviors to support tobacco cessation: A repeated cross-sectional study. J. Subst. Abus. Treat. 2013, 45, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stillman, F.A.; Kaufman, M.R.; Zhen, A.; Yang, J.; Wang, J.; Zhao, N. Smoke-free or not: A pilot evaluation in selected Beijing Hospitals. BMC Public Health 2013, 13, 964. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.D.; Elton-Marshall, T.; Mutti, S.; Dubray, J.; Fong, G.T. Understanding the impact of the Smoke-Free Ontario Act on hospitality establishments' outdoor environments: A survey of restaurants and bars. Tob. Control 2010, 19, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, M.C. Exposure to environmental tobacco smoke (ETS) and determinants of support for complete smoking bans in psychiatric settings. Tob. Control 2004, 13, 180–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauri, D.D.; Lieb, C.M.; Rajkumar, S.; Kooijman, C.; Sommer, H.L.; Roosli, M. Direct health costs of environmental tobacco smoke exposure and indirect health benefits due to smoking ban introduction. Eur. J. Public Health 2011, 21, 316–322. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report on Smoke-Free Policies in Australia; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Hahn, E.J.; Fallin, A.; Darville, A.; Kercsmar, S.E.; McCann, M.; Record, R.A. The Three Ts of Adopting Tobacco-free Policies on College Campuses. Nurs. Clin. N. Am. 2012, 47, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rozema, A.D.; Mathijssen, J.J.P.; Jansen, M.W.J.; van Oers, J.A.M. Schools as smoke-free zones? Barriers and facilitators to the adoption of outdoor school ground smoking bans at secondary schools. Tob. Induc. Dis. 2016, 14, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbison, P.A.; Whitman, M.V. Barriers associated with implementing a campus-wide smoke-free policy. Health Educ. 2008, 108, 321–331. [Google Scholar] [CrossRef]
- Atieno, O. An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl. Educ. 21st Century 2009, 13, 13–18. [Google Scholar]


{kind=link}
| Study | Selection Bias | Study Design | Confounders | Blinding | Data Collection | Withdrawals |
|---|---|---|---|---|---|---|
| Balbe et al., 2012 [16] | M | W | * | * | S | N/A |
| Boris et al., 2009 [20] | M | M | S | M | S | N/A |
| Eby et al., 2013 [36] | W | W | * | * | S | N/A |
| Edwards et al., 2008 [12] | W | W | * | * | M | N/A |
| Fallin et al., 2013 [22] | W | M | * | M | S | N/A |
| Garcia et al., 2006 [17] | M | W | * | * | S | N/A |
| Harris et al., 2009 [15] | M | W | * | * | M | N/A |
| Hyland et al., 1999 [26] | M | W | * | * | S | N/A |
| Jancey et al., 2014 [30] | M | W | * | * | S | N/A |
| Kaur et al., 2014 [33] | M | W | * | M | S | N/A |
| Kennedy et al., 2009 [38] | M | W | * | * | S | N/A |
| Lawn et al., 2010 [27] | M | W | * | * | S | N/A |
| Nimpitakpong et al., 2010 [24] | W | W | * | * | W | N/A |
| Paek et al., 2013 [31] | M | W | * | * | S | N/A |
| Record et al., 2017 [21] | W | M | * | W | M | M |
| Ravara et al., 2013 [25] | M | W | * | * | W | N/A |
| Reis et al., 2014 [34] | M | W | * | * | W | N/A |
| Rigotti et al., 1992 [18] | S | S | S | M | S | N/A |
| Rigotti et al., 1994 [19] | M | M | S | W | W | N/A |
| Russette et al., 2014 [23] | M | W | * | * | S | N/A |
| Sorensen et al., 1992 [32] | M | W | * | * | M | N/A |
| Stillman et al., 2013 [37] | M | M | W | W | S | N/A |
| Vardavas et al., 2013 [35] | M | M | S | M | S | M |
| Willemsen et al., 2004 [39] | W | W | * | * | S | N/A |
| Williams et al., 2004 [28] | W | W | * | * | M | N/A |
| Xiao et al., 2013 [29] | M | M | W | W | W | N/A |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wynne, O.; Guillaumier, A.; Twyman, L.; McCrabb, S.; Denham, A.M.J.; Paul, C.; Baker, A.L.; Bonevski, B. Signs, Fines and Compliance Officers: A Systematic Review of Strategies for Enforcing Smoke-Free Policy. Int. J. Environ. Res. Public Health 2018, 15, 1386. https://doi.org/10.3390/ijerph15071386
Wynne O, Guillaumier A, Twyman L, McCrabb S, Denham AMJ, Paul C, Baker AL, Bonevski B. Signs, Fines and Compliance Officers: A Systematic Review of Strategies for Enforcing Smoke-Free Policy. International Journal of Environmental Research and Public Health. 2018; 15(7):1386. https://doi.org/10.3390/ijerph15071386
Chicago/Turabian StyleWynne, Olivia, Ashleigh Guillaumier, Laura Twyman, Sam McCrabb, Alexandra M. J. Denham, Christine Paul, Amanda L. Baker, and Billie Bonevski. 2018. "Signs, Fines and Compliance Officers: A Systematic Review of Strategies for Enforcing Smoke-Free Policy" International Journal of Environmental Research and Public Health 15, no. 7: 1386. https://doi.org/10.3390/ijerph15071386