Changes in Lumbopelvic Movement and Muscle Recruitment Associated with Prolonged Deep Squatting: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
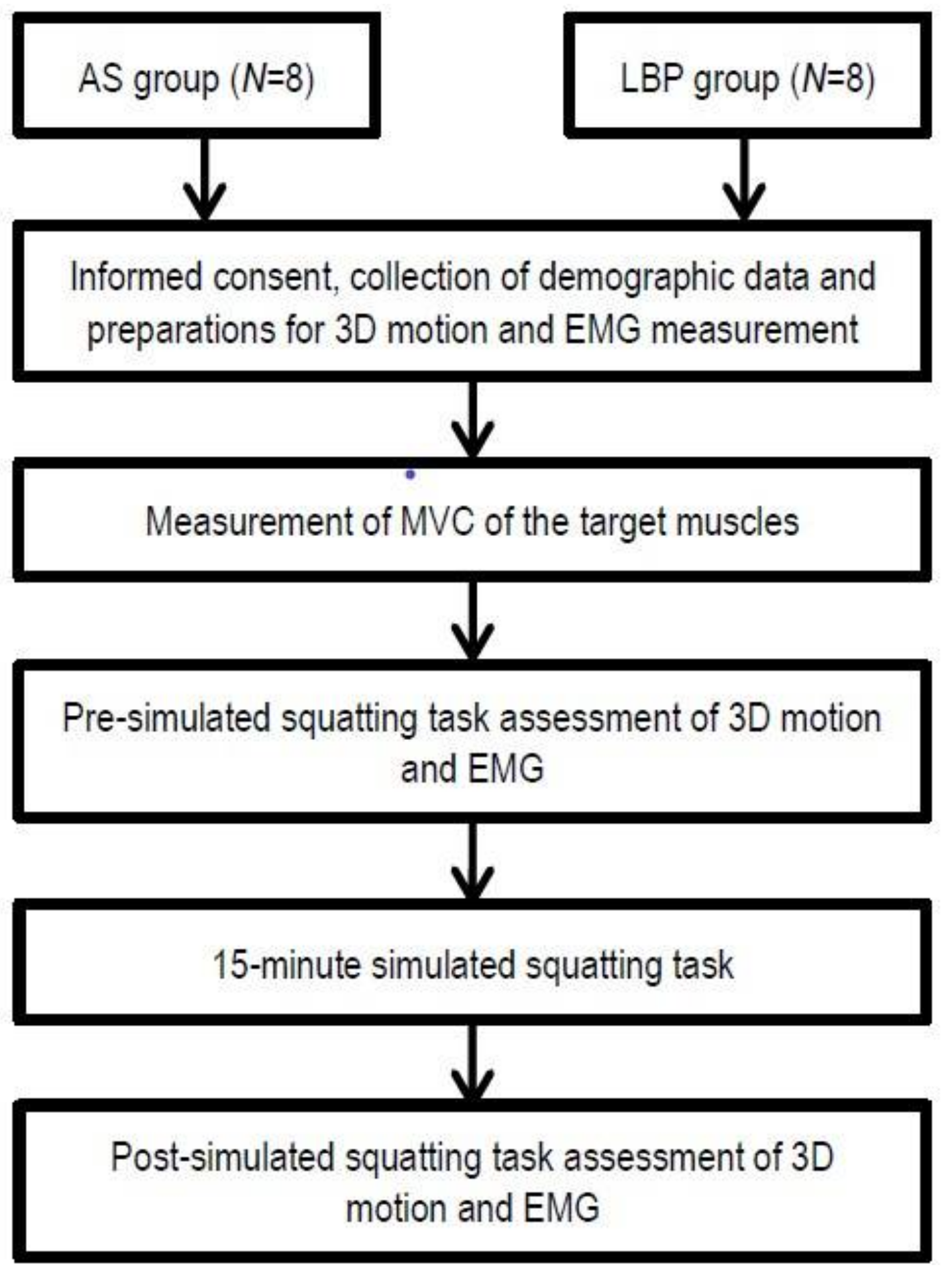
2.1. Study Design
2.2. Subjects
2.3. Measurements
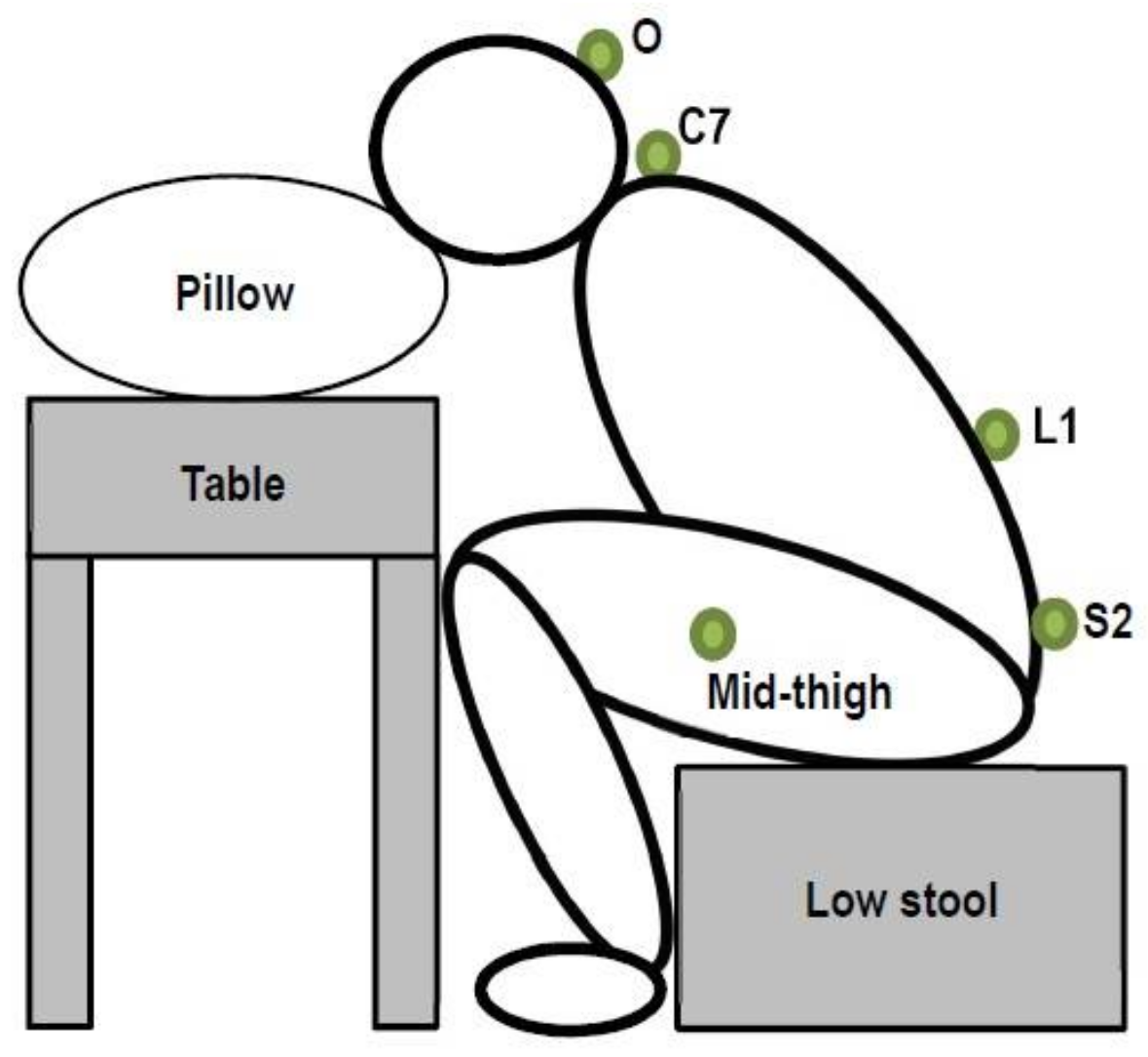
2.3.1. Measurement of Joint Kinematics
2.3.2. Measurement of Muscle Recruitment
2.3.3. Measurement of Maximal Voluntary Contraction (MVC)
2.3.4. Simulated Deep Squatting Position and Assessments of Squat-to-Stand and Stand-to-Squat Tasks
2.3.5. Data Processing and Statistical Analysis
3. Results
3.1. Standardization and Verification of Simulated Deep Squatting Position
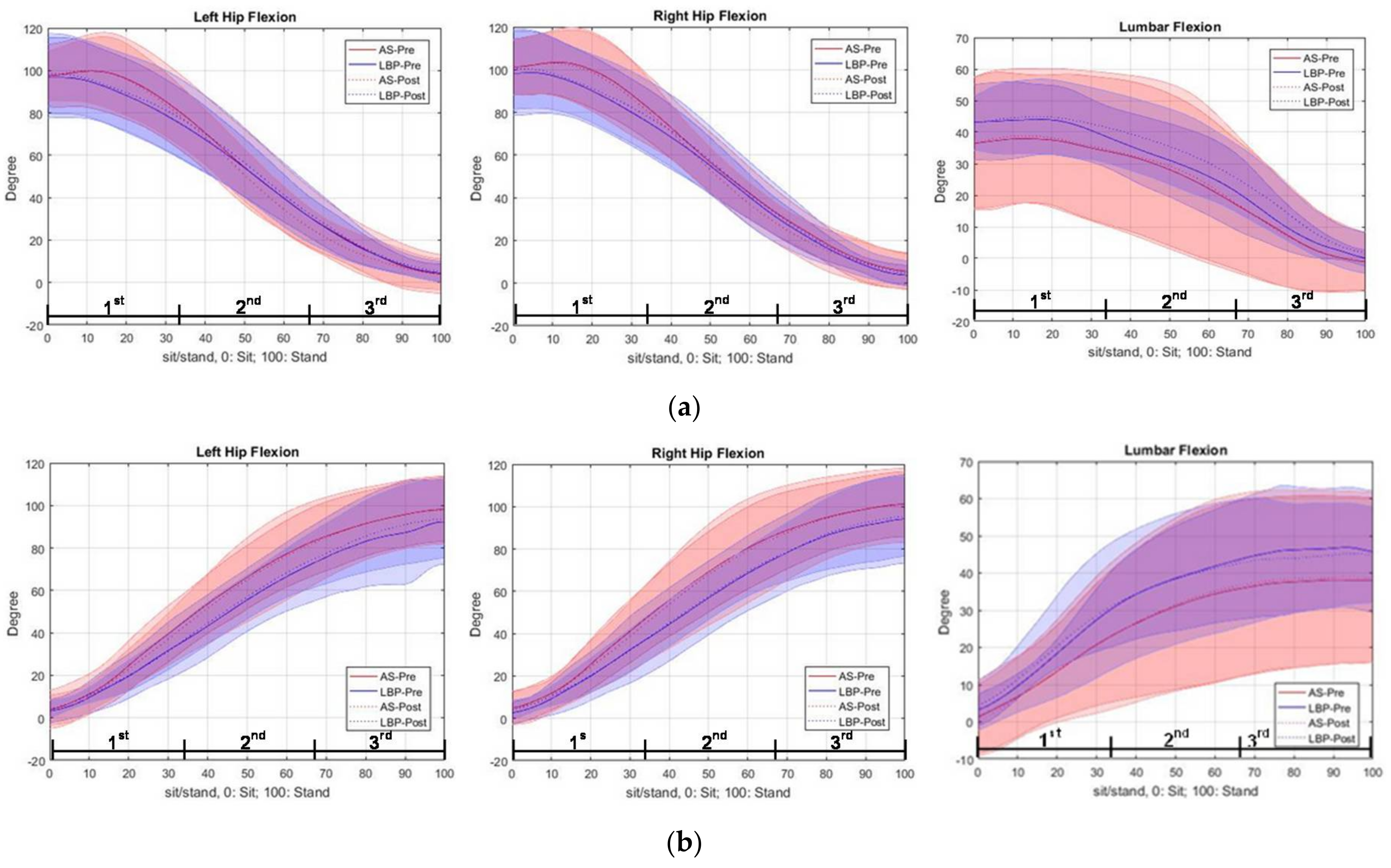
3.2. Trajectory of Regional Joint Angles of the Lumbopelvic Region during Squat-to-Stand and Stand-to-Squat Tasks
3.2.1. During Squat-to-Stand Phase (Before and Immediately after Deep Squatting)
3.2.2. During Stand-to-Squat Phase (Before and Immediately after Deep Squatting)
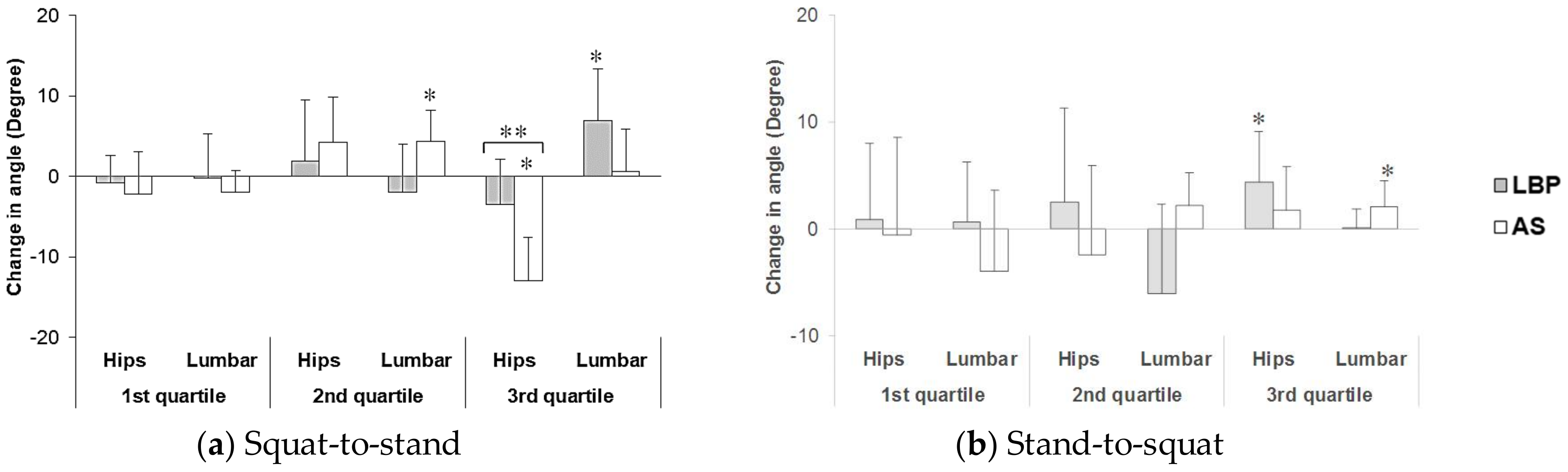
3.2.3. Changes in Lumbar Spine and Hip Joint Flexion Angles
- During Squat-to-Stand Phase
- During Stand-to-Squat Phase
3.3. Muscle Recruitment Pattern (Expressed in %MVC of EMG Activity)
3.3.1. During Squat-to-Stand Phase
3.3.2. During Stand-to-Squat Phase
4. Discussion
4.1. Verification of Deep Squatting Position
4.2. Changes in Movement Kinematics and Muscle Recruitment after Adoption of Prolonged Deep Squatting Posture
4.3. Limitations and Recommendations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Sterud, T.; Tynes, T. Work-related psychosocial and mechanical risk factors for low back pain: A 3-year follow-up study of the general working population in Norway. Occup. Environ. Med. 2013, 70, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Solomonow, M.; Zhou, B.H.; Baratta, R.V.; Burger, E. Biomechanics and electromyography of a cumulative lumbar disorder: Response to static flexion. Clin. Biomech. 2003, 18, 890–898. [Google Scholar] [CrossRef]
- Van Vuuren, B.J.; Becker, P.J.; van Heerden, H.J.; Zinzen, E.; Meeusen, R. Lower back problems and occupational risk factors in a South African steel industry. Am. J. Ind. Med. 2005, 47, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Pal, A.; De, S.; Sengupta, P.; Maity, P.; Dhara, P.C. Evaluation of work related musculoskeletal disorder and postural stress among female potato cultivators in West Bengal, India. Ergon. SA 2015, 27, 46–64. [Google Scholar] [CrossRef]
- Jia, N.; Li, T.; Hu, S.; Zhu, X.; Sun, K.; Yi, L.; Zhang, Q.; Luo, G.; Li, Y.; Zhang, X.; et al. Prevalence and its risk factors for low back pain among operation and maintenance personnel in wind farms. BMC Musculoskelet. Disord. 2016, 17, 314. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-A.; Shoemaker, C.A. Observing body position of older adults while gardening for health benefits and risks. Act. Adapt. Aging 2009, 33, 31–38. [Google Scholar] [CrossRef]
- Panjabi, M.M. The Stabilizing System of the Spine. Part I. Function, Dysfunction, Adaptation, and Enhancement. Clin. Spine Surg. 1992, 5, 383–389. [Google Scholar] [CrossRef]
- Mueller, M.J.; Maluf, K.S. Tissue Adaptation to Physical Stress: A Proposed ‘Physical Stress Theory’ to Guide Physical Therapist Practice, Education, and Research. Phys. Ther. 2002, 82, 383–403. [Google Scholar] [PubMed]
- Bergmark, A. Stability ofthe lumbar spine. A study in mechanical engineering. Acta Orthop. Scand. Suppl. 1989, 230, 1–54. [Google Scholar] [CrossRef] [PubMed]
- Cholewicki, J.; McGill, S.M. Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clin. Biomech. 1996, 11, 1–15. [Google Scholar] [CrossRef]
- Callaghan, J.P.; Dunk, N.M. Examination of the flexion relaxation phenomenon in erector spinae muscles during short duration slumped sitting. Clin. Biomech. 2002, 17, 353–360. [Google Scholar] [CrossRef]
- Shirado, O.; Ito, T.; Kaneda, K.; Strax, T.E. Flexion-relaxation phenomenon in the back muscles. A comparative study between healthy subjects and patients with chronic low back pain. Am. J. Phys. Med. Rehabilit. 1995, 74, 139–144. [Google Scholar]
- Solomonow, M. Neuromuscular manifestations of viscoelastic tissue degradation following high and low risk repetitive lumbar flexion. J. Electromyogr. Kinesiol. 2012, 22, 155–175. [Google Scholar] [CrossRef] [PubMed]
- Shin, G.; D’Souza, C.; Liu, Y.-H. Creep and Fatigue Development in the Low Back in Static Flexion. Spine 2009, 34, 1873–1878. [Google Scholar] [CrossRef] [PubMed]
- Abboud, J.; Nougarou, F.; Descarreaux, M. Muscle Activity Adaptations to Spinal Tissue Creep in the Presence of Muscle Fatigue. PLoS ONE 2016, 11, e0149076. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Zuriaga, D.; Adams, M.A.; Dolan, P. Is Activation of the Back Muscles Impaired by Creep or Muscle Fatigue? Spine 2010, 35, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.S. A compensation of angular displacements of the hip joints and lumbosacral spine between subjects with and without idiopathic low back pain during squatting. J. Electromyogr. Kinesiol. 2013, 23, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Eungpinichpong, W.; Buttagat, V.; Areeudomwong, P.; Pramodhyakul, N.; Swangnetr, M.; Kaber, D.; Puntumetakul, R. Effects of restrictive clothing on lumbar range of motion and trunk muscle activity in young adult worker manual material handling. Appl. Ergon. 2013, 44, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Schelldorfer, S.; Ernst, M.J.; Rast, F.M.; Bauer, C.M.; Meichtry, A.; Kool, J. Low back pain and postural control, effects of task difficulty on centre of pressure and spinal kinematics. Gait Posture 2015, 41, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Bauer, C.M.; Rast, F.M.; Ernst, M.J.; Oetiker, S.; Meichtry, A.; Kool, J.; Rissanen, S.M.; Suni, J.H.; Kankaanpää, M. Pain intensity attenuates movement control of the lumbar spine in low back pain. J. Electromyogr. Kinesiol. 2015, 25, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Bauer, C.M.; Rast, F.M.; Ernst, M.J.; Kool, J.; Oetiker, S.; Rissanen, S.M.; Suni, J.H.; Kankaanpää, M. Concurrent validity and reliability of a novel wireless inertial measurement system to assess trunk movement. J. Electromyogr. Kinesiol. 2015, 25, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar]
- Hermens, H.J.; Merletti, R.; Freriks, B. SENIAM European Recommendations for Surface Electromyography; Roessingh Research and Development: Enschede, The Netherlands, 1999. [Google Scholar]
- Arokoski, J.P.; Valta, T.; Kankaanpää, M.; Airaksinen, O. Activation of lumbar paraspinal and abdominal muscles during therapeutic exercises in chronic low back pain patients. Arch. Phys. Med. Rehabilit. 2004, 85, 823. [Google Scholar] [CrossRef]
- De Ridder, E.M.; Van Oosterwijck, J.O.; Vleeming, A.; Vanderstraeten, G.G.; Danneels, L.A. Posterior muscle chain activity during various extension exercises: An observational study. BMC Musculoskelet. Disord. 2013, 14, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffiuletti, N.A.; Lepers, R. Quadriceps Femoris Torque and EMG Activity in Seated versus Supine Position. Med. Sci. Sports Exerc. 2003, 35, 1511–1516. [Google Scholar] [CrossRef] [PubMed]
- Olson, M.W.; Li, L.; Solomonow, M. Flexion-relaxation response to cyclic lumbar flexion. Clin. Biomech. 2004, 19, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Naserkhaki, S.; Jaremko, J.L.; El-Rich, M. Effects of inter-individual lumbar spine geometry variation on load-sharing: Geometrically personalized Finite Element study. J. Biomech. 2016, 49, 2909–2917. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Ning, X.; Mirka, G.A. An algorithm for defining the onset and cessation of the flexion-relaxation phenomenon in the low back musculature. J. Electromyogr. Kinesiol. 2012, 22, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Solomonow, M.; Baratta, R.V.; Zhou, B.H.; Burger, E.; Zieske, A.; Gedalia, A. Muscular dysfunction elicited by creep of lumbar viscoelastic tissue. J. Electromyogr. Kinesiol. 2003, 13, 381–396. [Google Scholar] [CrossRef]
- Marras, W.S.; Lavender, S.A.; Leurgans, S.E.; Fathallah, F.A.; Ferguson, S.A.; Gary Allread, W.; Rajulu, S.L. Biomechanical risk factors for occupationally related low back disorders. Ergonomics 1995, 38, 377–410. [Google Scholar] [CrossRef] [PubMed]
- Marras, W.S.; Parakkat, J.; Chany, A.M.; Yang, G.; Burr, D.; Lavender, S.A. Spine loading as a function of lift frequency, exposure duration, and work experience. Clin. Biomech. 2006, 21, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Rogers, E.; Moorhouse, K. Effects of static flexion-relaxation on paraspinal reflex behavior. Clin. Biomech. 2005, 20, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Slota, G.P.; Wilson, S.E. Influence of Fatigue in Neuromuscular Control of Spinal Stability. Hum. Factor. 2004, 46, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.M.; Fritz, J.M.; Kerrigan, D.C.; Saliba, E.N.; Gansneder, B.M.; Ingersoll, C.D. Quadriceps Inhibition After Repetitive Lumbar Extension Exercise in Persons with a History of Low Back Pain. J. Athl. Train. 2006, 41, 264–269. [Google Scholar] [PubMed]
- Wilson, J.; Ferris, E.; Heckler, A.; Maitland, L.; Taylor, C. A structured review of the role of gluteus maximus in rehabilitation. J. Physiother. 2005, 33, 95–100. [Google Scholar]
- Leinonen, V.; Kankaanpää, M.; Airaksinen, O.; Hãnninen, O. Back and hip extensor activities during trunk flexion/extension: Effects of low back pain and rehabilitation. Arch. Phys. Med. Rehabilit. 2000, 81, 32–37. [Google Scholar] [CrossRef]
- Vogt, L.; Pfeifer, K.; Banzer, W. Neuromuscular control of walking with chronic low-back pain. Man. Ther. 2003, 8, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Pries, E.; Dreischarf, M.; Bashkuev, M.; Putzier, M.; Schmidt, H. The effects of age and gender on the lumbopelvic rhythm in the sagittal plane in 309 subjects. J. Biomech. 2015, 48, 3080–3087. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Schmid, I.; Sander, S.; Högel, J.; Eisele, R.; Kinzl, L.; Hartwig, E. Guidelines for the intramuscular positioning of EMG electrodes in the semispinalis capitis and cervicis muscles. J. Electromyogr. Kinesiol. 2003, 13, 289–295. [Google Scholar] [CrossRef]
- Delitto, R.S.; Rose, S.J. An Electromyographic Analysis of Two Techniques for Squat Lifting and Lowering. Phys. Ther. 1992, 72, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Katsuhira, J.; Matsudaira, K.; Maruyama, H. Effect of pelvic forward tilt on low back compressive and shear forces during a manual lifting task. J. Phys. Ther. Sci. 2016, 28, 802–806. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | LBP Group (n = 8) | AS Group (n = 8) | p-Value 1 |
|---|---|---|---|
| Age | 24.50 ± 2.62 | 25.38 ± 2.88 | 0.535 |
| Height (m) | 1.72 ± 0.05 | 1.70 ± 0.08 | 0.626 |
| Weight (kg) | 69.94 ± 7.68 | 66.85 ± 15.48 | 0.621 |
| BMI (m/kg2) | 23.65 ± 2.71 | 23.11 ±5.43 | 0.807 |
| History of chronic LBP (month) | 23.75 ± 19.26 | N/A 2 | N/A |
| VAS before experiment (0–10) | 0–0.5 | 0 | N/A |
| Joint Angle | LBP Group | AS Group | p-Value 1 |
|---|---|---|---|
| Lumbar (°) | 42 ± 5 | 33 ± 16 | 0.158 |
| (R) hip (°) | 104 ± 15 | 102 ± 11 | 0.835 |
| (L) hip (°) | 101 ± 15 | 100 ± 13 | 0.918 |
| Mean of hip flexion angles 2 (°) | 102 ± 15 | 101 ± 12 | 0.535 |
| Total flexion angle (°) | 144 ± 13 | 134 ± 14 | 0.146 |
| LBP Subject | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| (R) ES | 1.79% | 1.97% | 2.21% | 2.92% | 3.95% | 3.99% | 4.01% | 9.70% |
| (L) ES | 1.64% | 1.80% | 2.56% | 2.87% | 3.49% | 3.71% | 4.64% | 11.25% |
| AS Subject | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| (R) ES | 0.90% | 1.40% | 1.75% | 2.93% | 3.20% | 3.92% | 7.97% | 12.48% |
| (L) ES | 1.02% | 1.18% | 2.62% | 4.26% | 4.57% | 6.63% | 7.89% | 8.22% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lui, T.K.S.; Tsang, S.M.H.; Kwok, A.W.L. Changes in Lumbopelvic Movement and Muscle Recruitment Associated with Prolonged Deep Squatting: A Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 1001. https://doi.org/10.3390/ijerph15051001
Lui TKS, Tsang SMH, Kwok AWL. Changes in Lumbopelvic Movement and Muscle Recruitment Associated with Prolonged Deep Squatting: A Pilot Study. International Journal of Environmental Research and Public Health. 2018; 15(5):1001. https://doi.org/10.3390/ijerph15051001
Chicago/Turabian StyleLui, Tim K. S., Sharon M. H. Tsang, and Anthony W. L. Kwok. 2018. "Changes in Lumbopelvic Movement and Muscle Recruitment Associated with Prolonged Deep Squatting: A Pilot Study" International Journal of Environmental Research and Public Health 15, no. 5: 1001. https://doi.org/10.3390/ijerph15051001