
Investigation of Acute Pulmonary Deficits Associated with Biomass Fuel Cookstove Emissions in Rural Bangladesh

Abstract
:1. Introduction
2. Materials and Methods
2.1. Spirometry
2.2. Air Quality Measurements
3. Results
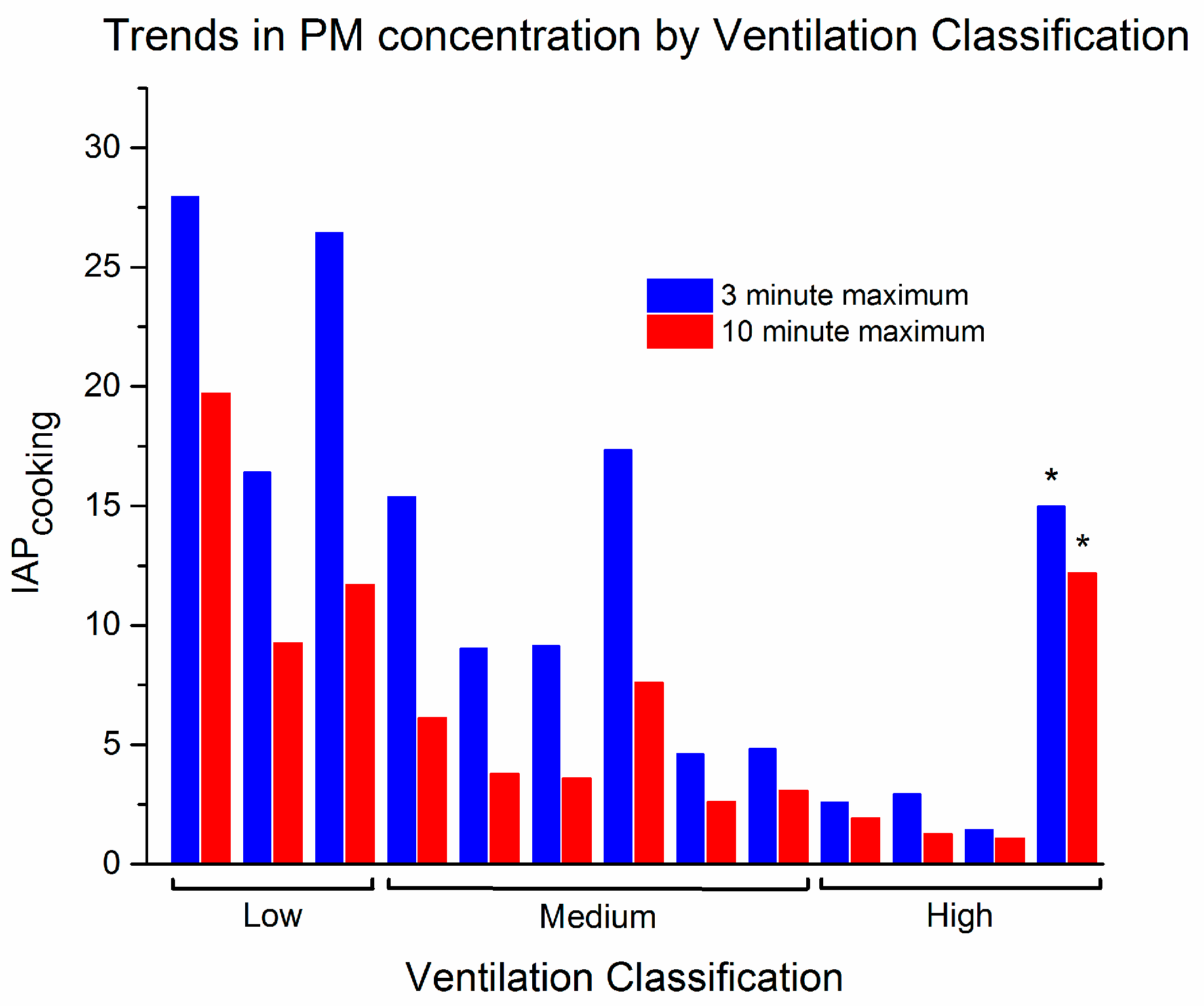
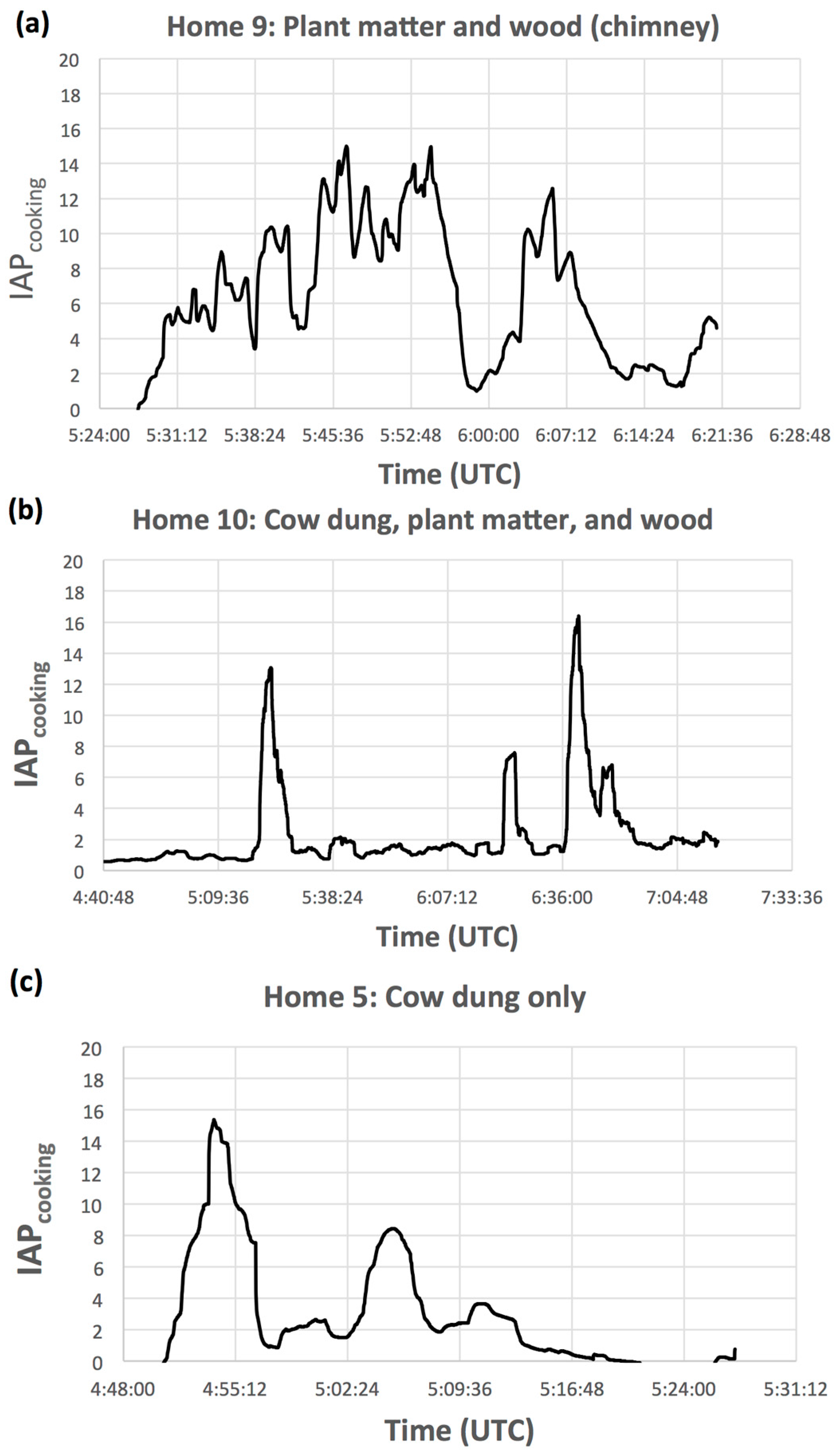
3.1. Air Quality Measurements
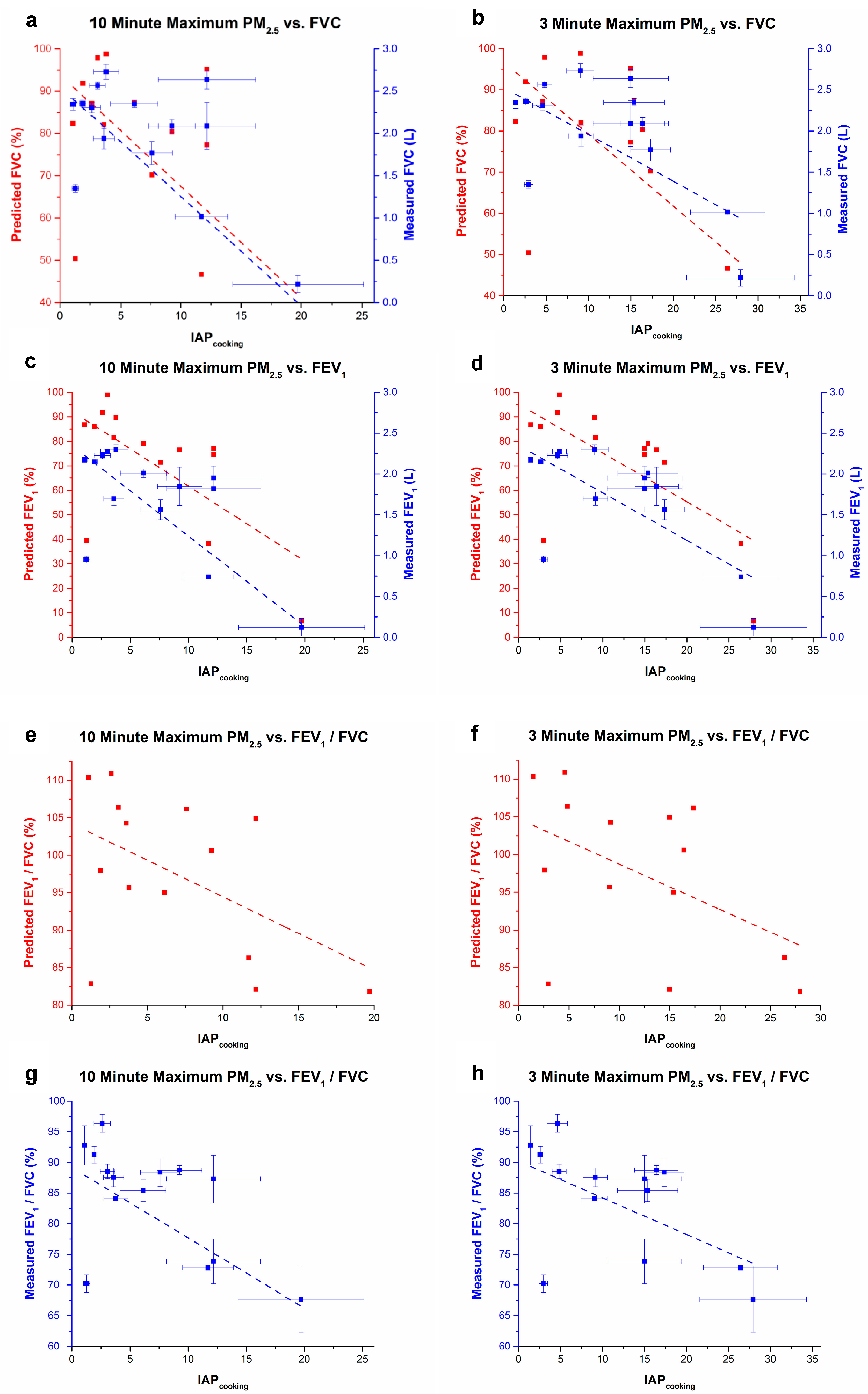
3.2. Pulmonary Health
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Naeher, L.P.; Brauer, M.; Lipsett, M.; Zelikoff, J.T.; Simpson, C.D.; Koenig, J.Q.; Smith, K.R. Woodsmoke health effects: A review. Inhal. Toxicol. 2007, 19, 67–106. [Google Scholar] [CrossRef] [PubMed]
- Sheesley, R.J.; Schauer, J.J.; Chowdhury, Z.; Cass, G.R.; Simoneit, B.R.T. Characterization of organic aerosols emitted from the combustion of biomass indigenous to south asia. J. Geophys. Res. 2003, 108, 4285. [Google Scholar] [CrossRef]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Clark, M.L.; Peel, J.L.; Burch, J.B.; Nelson, T.L.; Robinson, M.M.; Conway, S.; Bachand, A.M.; Reynolds, S.J. Impact of improved cookstoves on indoor air pollution and adverse health effects among Honduran women. Int. J. Environ. Health Res. 2009, 19, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, D.G.; Bruce, N.; Gordon, S.B. Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 843–851. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Household Air Pollution and Health; Fact Sheet no 292; WHO: Geneva, Switzerland, 2016; Available online: http://www.who.int/mediacentre/factsheets/fs292/en/ (accessed on 13 June 2017).
- Duflo, E.; Greenstone, M.; Hanna, R. Cooking stoves, indoor air pollution and respiratory health in rural Orissa. Econ. Political Wkly. 2008, 43, 71–76. [Google Scholar]
- Smith, K.R. Fuel combustion, air pollution exposure, and health: The situation in developing countries. Annu. Rev. Energy Environ. 1993, 18, 529–566. [Google Scholar] [CrossRef]
- Romieu, I.; Riojas-Rodríguez, H.; Marrón-Mares, A.T.; Schilmann, A.; Perez-Padilla, R.; Masera, O. Improved biomass stove intervention in rural Mexico: Impact on the respiratory health of women. Am. J. Respir. Crit. Care Med. 2009, 180, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.T.; Nakai, S. Prevalence of acute respiratory infections in women and children in Western Sierra Leone due to smoke from wood and charcoal stoves. Int. J. Environ. Res. Public Health 2012, 9, 2252–2265. [Google Scholar] [CrossRef] [PubMed]
- Bihari, V.; Iqbal, S.M.; Srivastava, L.P.; Kesavachandran, C.; Siddique, M.J. Lung function impairment in women exposed to biomass fuels during cooking compared to cleaner fuels in Uttar Pradesh, India. J. Environ. Biol. 2013, 34, 971–974. [Google Scholar] [PubMed]
- Köksal, H.; Saygı, A.; Sarıman, N.; Alıcı, E.; Yurtlu, Ş.; Yılmaz, H.; Düzgün, Y. Evaluation of clinical and functional parameters in female subjects with biomass smoke exposure. Respir. Care 2013, 58, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. Pocket Guide to COPD Diagnosis, Management, and Prevention: A Guide for Health Care Professionals, 2017 Report; GOLD, Inc. Available online: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/ (accessed on 13 June 2017).
- Regalado, J.; Pérez-Padilla, R.; Sansores, R.; Páramo Ramirez, J.I.; Brauer, M.; Paré, P.; Vedal, S. The effect of biomass burning on respiratory symptoms and lung function in rural mexican women. Am. J. Respir. Crit. Care Med. 2006, 174, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R. Health, energy, and greenhouse-gas impacts of biomass combustion in household stoves. Energy Sustain. Dev. 1994, 1, 23–29. [Google Scholar] [CrossRef]
- Duwell International. Available online: http://www.duwell.org/ (accessed on 13 June 2017).
- COSMED. Advanced Desktop Spirometer with Spirometry, Airway Resistance and Respiratory Mechanics; Pony FX Desktop Spirometer; COSMED: Rome, Italy, 2016. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Eaton, T.; Withy, S.; Garrett, J.E.; Mercer, J.; Whitlock, R.M.; Rea, H.H. Spirometry in primary care practice: The importance of quality assurance and the impact of spirometry workshops. Chest 1999, 116, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Chang, D.P.; Kleeman, M.J.; Perry, K.D.; Cahill, T.A.; Dutcher, D.; McDougall, E.M.; Stroud, K. Comparison of real-time instruments used to monitor airborne particulate matter. J. Air Waste Manag. Assoc. 2001, 51, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Jetter, J.; Zhao, Y.; Smith, K.R.; Khan, B.; Yelverton, T.; Decarlo, P.; Hays, M.D. Pollutant emissions and energy efficiency under controlled conditions for household biomass cookstoves and implications for metrics useful in setting international test standards. Environ. Sci. Technol. 2012, 46, 10827–10834. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.; Lam, N.; Brant, S.; Gray, C.; Pennise, D. Modeling indoor air pollution from cookstove emissions in developing countries using a monte carlo single-box model. Atmos. Environ. 2011, 45, 3237–3243. [Google Scholar] [CrossRef]
- Gauderman, W.J.; McConnell, R.; Gilliland, F.; London, S.; Thomas, D.; Avol, E.; Vora, H.; Berhane, K.; Rappaport, E.B.; Lurmann, F.; et al. Association between air pollution and lung function growth in Southern California children. Am. J. Respir. Crit. Care Med. 2000, 162, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Halbert, R.J.; Natoli, J.L.; Gano, A.; Badamgarav, E.; Buist, A.S.; Mannino, D.M. Global burden of COPD: Systematic review and meta-analysis. Eur. Respir. J. 2006, 28, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Eur. Respir. J. 1993, 6 (Suppl. 16), 5–40. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, and UNAIDS. Air Quality Guidelines: Global update 2005. World Health Organization: Geneva, Switzerland, 2006. Available online: whqlibdoc.who.int/hq/2006/WHO_SDE_PHE_OEH_06.02_eng.pdf (accessed on 13 June 2017).
- El Arifeen, S.; Christou, A.; Reichenbach, L.; Osman, F.A.; Azad, K.; Islam, K.S.; Ahmed, F.; Perry, H.B.; Peters, D.H. Community-based approaches and partnerships: Innovations in health-service delivery in Bangladesh. Lancet 2013, 382, 2012–2026. [Google Scholar] [CrossRef]
- Bell, M.L.; O’Neill, M.S.; Cifuentes, L.A.; Braga, A.L.F.; Collin, G.; Nweke, A.; Rogat, J.; Sibold, K. Challenges and recommendations for the study of socioeconomic factors and air pollution health effects. Environ. Sci. Policy 2005, 8, 525–533. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Measured Non-Cooking *** IAP Variability | Measured Cooking IAP Level | Lung Function Decrements | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| While Cooking | ||||||||||||
| Subj/Home | Age | Years Cooking | Fuels Utilized | Ventilation Class | **** % FEV1/FVC † | FEV1 | FEV1% Change | |||||
| Baseline Differences between Homes | 3′ Max | 10′ Max | Non-Cooking | Cooking | Non-Cooking | Cooking | * 100 | |||||
| Average (Standard Deviation), n = 3 | ||||||||||||
| 1 | 18 | 2–3 days | W | high | −0.02 | 2.6 | 1.9 | NA | NA | NA | NA | NA |
| 2 | 60 | 30 | CD, PM, W | low | 0.09 | 27.9 | 19.7 | 91.50 (0.42) | 67.7 (5.37) | 1.39 (0.03) | 0.12 (0.11) | −91.11 |
| 4 | 21 | 4–5 months | CD, PM, W | low | 0.09 | NA | NA | 85.33 (4.16) | 83.97 (2.33) | 2.02 (0.21) | 2.24 (0.10) | 11.06 |
| 5 | 25 | 14 | CD, PM, W | medium | 0.08 | 15.4 | 6.1 | 88.03 (0.96) | 85.43 (1.82) | 2.12 (0.11) | 2.01 (0.05) | −5.04 |
| 6 | 30 | 15 | CD, W | medium | −0.05 | 9 | 3.8 | 84.87 (3.07) | 84.10 (0.30) | 2.44 (0.06) | 2.30 (0.06) | −6.00 |
| 8 | 40 | 30 | W ** | high | 0.01 | 2.9 | 1.3 | 70.00 (1.20) | 70.23 (1.43) | 0.95 (0.02) | 0.95 (0.04) | 0.35 |
| 9A | 25 | 2–3 months | CD, PM, W | high | 0.01 | 15 | 12.2 | 86.00 (10.06) | 73.87 (3.65) | 2.20 (0.32) | 1.95 (0.15) | −11.36 |
| 9B | 50 | 30 | CD, PM, W | high | 0.01 | 15 | 12.2 | NA | NA | NA | NA | NA |
| 10 | 30 | 16 | CD, PM, W | low | −0.25 | 16.4 | 9.3 | 88.83 (1.40) | 88.77 (0.75) | 1.98 (0.03) | 1.85 (0.24) | −6.41 |
| 11 | 50 | 38 | CD, PM, W | medium | −0.11 | 9.1 | 3.6 | 88.70 (1.47) | 87.57 (1.54) | 1.57 (0.07) | 1.70 (0.08) | 8.07 |
| 12 | 45 | 25 | CD, PM, W | high | −0.04 | 1.4 | 1.1 | 91.07 (2.44) | 92.83 (3.20) | 2.11 (0.02) | 2.17 (0.03) | 3.16 |
| 14 | 50 | 34 | CD, W * | low | 0.04 | 26.4 | 11.7 | 71.13 (1.33) | 72.80 (0.44) | 0.76 (0.03) | 0.74 (0.01) | −2.20 |
| 15 | 55 | 43 | CD, PM, W | medium | 0.08 | 17.3 | 7.6 | NA | NA | NA | NA | NA |
| 16 | 35 | 12 | CD, PM | medium | 0.06 | 4.6 | 2.6 | 99.23 (0.49) | 96.40 (1.48) | 2.21 (0.03) | 2.23 (0.04) | 0.75 |
| 17 | 50 | 25 | W | medium | 0.00 | 4.8 | 3.1 | 89.43 (0.46) | 88.53 (1.19) | 2.22 (0.04) | 2.27 (0.02) | 2.25 |
| General Symptoms Encountered While Cooking | Cardiorespiratory Symptoms | ||
|---|---|---|---|
| Symptom | Prevalence (%) | Symptom | Prevalence (%) |
| difficulty breathing | 29 | ever chest pain | 53 |
| coughing | 18 | chest pain walking uphill | 53 |
| wheezing | 12 | chest pain walking level | 29 |
| headache | 12 | severe chest pain >30′ | 29 |
| phlegm | 6 | shortness of breath | 41 |
| watery eyes | 6 | ||
| N = 17 | |||
| Model | Measurement | Pearson’s R | Adj. R Square | F Value | Prob>F | EE * |
|---|---|---|---|---|---|---|
| Measured | (a) 10 min max PM2.5 v FVC | −0.866 | 0.729 | 36.00 | 0.00006 | −0.13 |
| % Predicted | (a) 10 min max PM2.5 v FVC | −0.605 | 0.313 | 6.92 | 0.01 | −2.64 |
| Measured | (b) 3 min max PM2.5 v FVC | −0.886 | 0.767 | 43.90 | 0.00002 | −0.06 |
| % Predicted | (b) 3 min max PM2.5 v FVC | −0.620 | 0.333 | 7.49 | 0.02 | −1.75 |
| Measured | (c) 10 min max PM2.5 v FEV1 | −0.813 | 0.632 | 23.34 | 0.0004 | −0.11 |
| % Predicted | (c) 10 min max PM2.5 v FEV1 | −0.663 | 0.393 | 9.17 | 0.01 | −3.06 |
| Measured | (d) 3 min max PM2.5 v FEV1 | −0.936 | 0.865 | 84.48 | <0.00001 | −0.05 |
| % Predicted | (d) 3 min max PM2.5 v FEV1 | −0.663 | 0.393 | 9.41 | 0.01 | −1.99 |
| Measured | (e) 10 min max PM2.5 v FEV1/FVC | −0.667 | 0.399 | 9.63 | 0.009 | −1.15 |
| % Predicted | (g) 10 min max PM2.5 v FEV1/FVC | −0.510 | 0.198 | 4.22 | 0.06 | −0.98 |
| Measured | (f) 3 min max PM2.5 v FEV1/FVC | −0.749 | 0.525 | 15.36 | 0.002 | −0.60 |
| % Predicted | (h) 3 min max PM2.5 v FEV1/FVC | −0.487 | 0.173 | 3.72 | 0.08 | −0.60 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medgyesi, D.N.; Holmes, H.A.; Angermann, J.E. Investigation of Acute Pulmonary Deficits Associated with Biomass Fuel Cookstove Emissions in Rural Bangladesh. Int. J. Environ. Res. Public Health 2017, 14, 641. https://doi.org/10.3390/ijerph14060641
Medgyesi DN, Holmes HA, Angermann JE. Investigation of Acute Pulmonary Deficits Associated with Biomass Fuel Cookstove Emissions in Rural Bangladesh. International Journal of Environmental Research and Public Health. 2017; 14(6):641. https://doi.org/10.3390/ijerph14060641
Chicago/Turabian StyleMedgyesi, Danielle N., Heather A. Holmes, and Jeff E. Angermann. 2017. "Investigation of Acute Pulmonary Deficits Associated with Biomass Fuel Cookstove Emissions in Rural Bangladesh" International Journal of Environmental Research and Public Health 14, no. 6: 641. https://doi.org/10.3390/ijerph14060641