
The Covariance between Air Pollution Annoyance and Noise Annoyance, and Its Relationship with Health-Related Quality of Life




Abstract
:1. Introduction
1.1. The Health Effect of Noise and Air Pollution
1.2. Combined Effects of Air and Noise Pollution on Health
1.3. Environmental Stressors and Health Effects
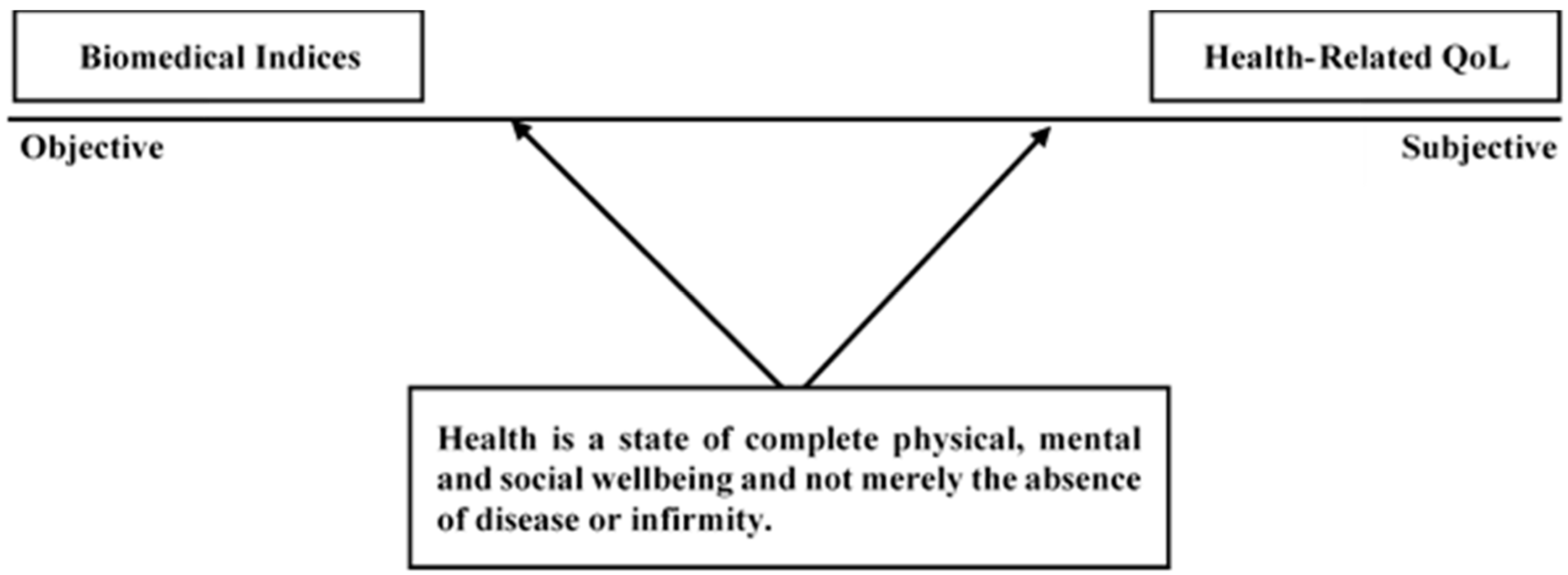
An individual's perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards and concerns. It is a broad-ranging concept, incorporating in a complex way the person's physical health, psychological state, level of independence, social relationships, and their relationship to salient features of their environment.(WHOQOL Group, [44])
1.4. Study Objectives
2. Materials and Methods
2.1. Participants
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
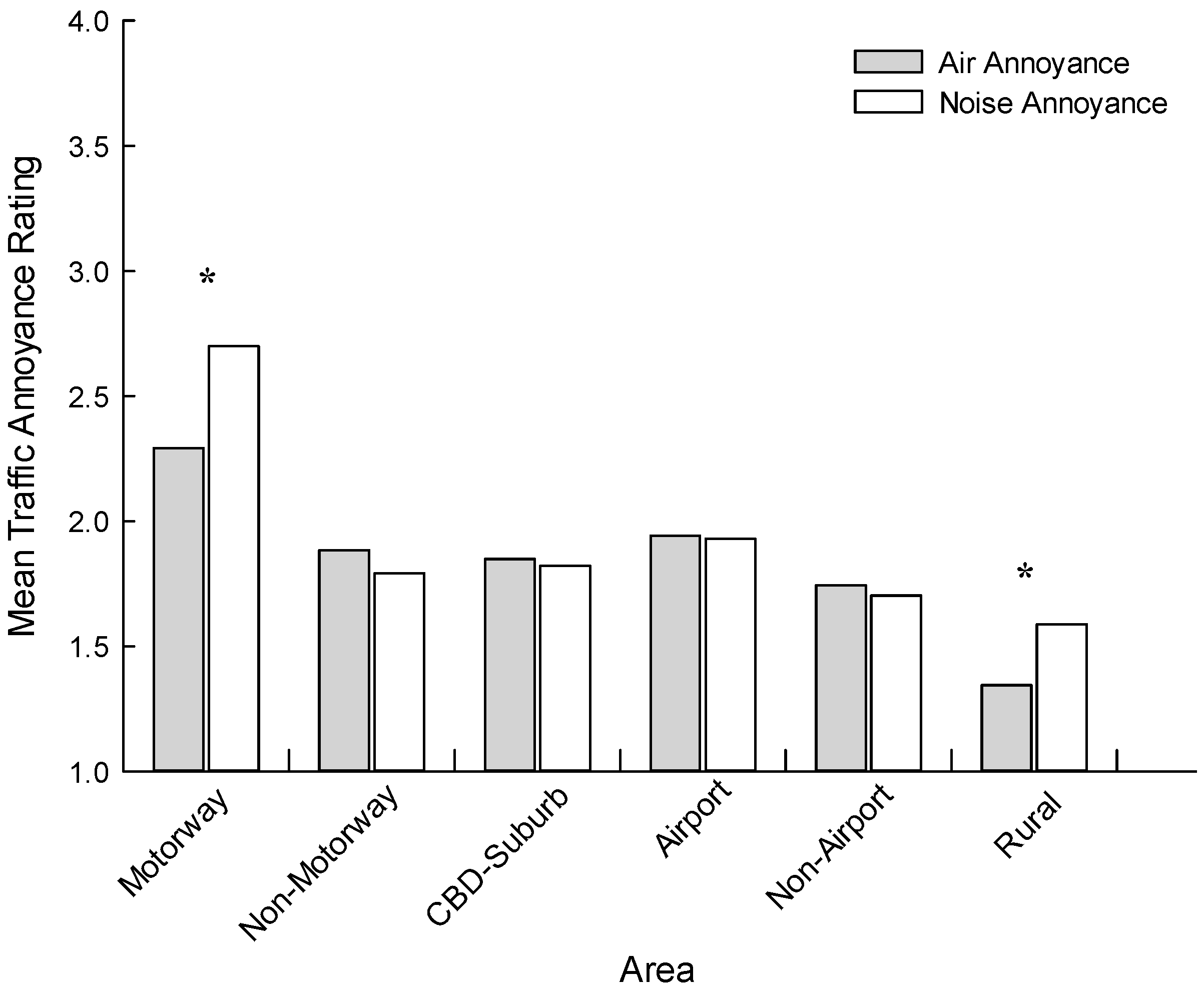
3.1. Summary Statistics for Annoyance Data
3.2. Correlational Analysis
3.3. Summary Statistics for Health Related Quality of Life
3.4. Multiple Linear Regression
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Wilson, K.; Elliott, S.; Law, M.; Eyles, J.; Jerrett, M.; Keller-Olaman, S. Linking perceptions of neighbourhood to health in Hamilton, Canada. J. Epidemiol. Community Health 2004, 58, 192–198. [Google Scholar] [PubMed]
- Tonne, C.; Halonen, J.I.; Beevers, S.D.; Dajnak, D.; Gulliver, J.; Kelly, F.J.; Wilkinson, P.; Anderson, H.R. Long-term traffic air and noise pollution in relation to mortality and hospital readmissions among myocardial infarction survivors. Int. J. Hyg. Environ. Health 2016, 219, 72–78. [Google Scholar] [PubMed]
- Franklin, B.A.; Brook, R.; Pope, C.A., III. Air pollution and cardiovascular disease. Curr. Probl. Cardiol. 2015, 40, 207–238. [Google Scholar] [CrossRef] [PubMed]
- Van Kempen, E.; Fischer, P.; Janssen, N.; Houthuijs, D.; van Kamp, I.; Stansfeld, S.; Cassee, F. Neurobehavioral effects of exposure to traffic-related air pollution and transportation noise in primary school children. Environ. Res. 2012, 115, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, M.; Hjortebjerg, D.; Eriksen, K.T.; Ketzel, M.; Tjønneland, A.; Overvad, K.; Raaschou-Nielsen, O. Exposure to long-term air pollution and road traffic noise in relation to cholesterol: A cross-sectional study. Environ. Int. 2015, 85, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Persson, R.; Bjork, J.; Ardo, J.; Albin, M.; Jakobsson, K. Trait anxiety and modeled exposure as determinants of self-reported annoyance to sound, air pollution and other environmental factors in the home. Int. Arch. Occup. Environ. Health 2007, 81, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Ross, Z.; Kheirbek, I.; Clougherty, J.E.; Ito, K.; Matte, T.; Markowitz, S.; Eisl, H. Noise, air pollution and traffic: Continuous measurement and correlation at a high-traffic location in New York city. Environ. Res. 2011, 111, 1054–1063. [Google Scholar] [CrossRef] [PubMed]
- Dekoninck, L.; Botteldooren, D.; Panis, L.I. Using city-wide mobile noise assessments to estimate bicycle trip annual exposure to black carbon. Environ. Int. 2015, 83, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Lercher, P.; Schmitzberger, R.; Kofler, W. Perceived traffic air pollution, associated behaviour and health in an alpine area. Sci. Total Envrion. 1995, 169, 71–74. [Google Scholar] [CrossRef]
- Georgoulis, L.B.; Hanninen, O.; Samoli, E.; Katsouyanni, K.; Kunzli, N.; Polanska, L.; Bruinen de Bruin, Y.; Alm, S.; Jantunen, M. Personal carbon monoxide exposure in five European cities and its determinants. Atmos. Environ 2002, 36, 963–974. [Google Scholar] [CrossRef]
- Berglund, B.; Lindvall, T.; Schwela, D.H. Guidelines for Community Noise; World Health Organization (WHO): Geneva, Switzerland, 1999. [Google Scholar]
- World Health Organization (WHO). Burden of Disease from Ambient Air Pollution for 2012; World Health Organization (WHO): Geneva, Switzerland, 2014. [Google Scholar]
- De Hollander, A.E.M.; Melse, J.M.; Lebret, E.; Kramers, P.G.N. An aggregate public health indicator to represent the impact of multiple environmental exposures. Epidemiology 1999, 10, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Zijlema, W.L.; Wolf, K.; Emeny, R.; Ladwig, K.H.; Peters, A.; Kongsgård, H.; Hveem, K.; Kvaløy, K.; Yli-Tuomi, T.; Partonen, T.; et al. The association of air pollution and depressed mood in 70.928 individuals from four European cohorts. Int. J. Hyg. Environ. Health 2015, 219, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.J.; Kubzansky, L.D.; Coull, B.A.; Kloog, I.; Koutrakis, P.; Sparrow, D.; Spiro, A.; Volkonas, P.; Schwartz, J. Associations between air pollution and perceived stress: The Veterans Administration Normative Aging Study. Environ. Health 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Boogaard, H.; Janssen, N.A.H.; Fischer, P.H.; Kos, G.P.; Weijers, A.E.P.; Cassee, F.R.; van der Zee, S.C.; de Hartog, J.J.; Brunekreef, B.; Hoek, G. Contrasts in oxidative potential and other particulate matter characteristics collected near major streets and background locations. Environ. Health Perspect. 2012, 120, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Auckland Council. State of Air Quality Report Card. Available online: http://stateofauckland.aucklandcouncil.govt.nz/air-quality-report-card/auckland-reporting-area/ (accessed on 21 May 2013).
- Stansfeld, S.A. Noise effects on health in the context of air pollution exposure. Int. J. Environ. Res. Public Health 2015, 12, 12735–12760. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, X.; Braubach, M.; Krapavickaite, D.; Ormandy, D.; Zurlyte, I. Housing conditions and self-reported health status: A study in panel block buildings in three cities of Eastern Europe. J. Hous. Built Environ. 2003, 18, 329–352. [Google Scholar] [CrossRef]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Burden of Disease from Environmental Noise. Quantification of Healthy Life Years Lost in Europe; World Health Organization (WHO): Geneva, Switzerland, 2011. [Google Scholar]
- Kaltenbach, M.; Maschke, C.; Heb, F.; Niemann, H.; Führ, M. Health impairments, annoyance and learning disorders caused by aircraft noise. Int. J. Environ. Protect. 2016, 6, 15–46. [Google Scholar] [CrossRef]
- Shepherd, D.; Heinonen-Guzejevb, M.; Hautus, M.J.; Heikkiläb, K. Elucidating the relationship between noise sensitivity and personality. Noise Health 2015, 17, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Fidell, S.; Tabachnick, B.; Mestre, V.; Fidell, L. Aircraft noise-induced awakenings are more reasonably predicted from relative than from absolute sound exposure levels. J. Acoust. Soc. Am. 2013, 134, 3645–3653. [Google Scholar] [CrossRef] [PubMed]
- Miedema, H.M.; Vos, H. Noise sensitivity and reactions to noise and other environmental conditions. J. Acoust. Soc. Am. 2003, 113, 1492–1504. [Google Scholar] [CrossRef] [PubMed]
- Fidell, S. The Schultz curve 25 years later: A research perspective. J. Acoust. Soc. Am. 2003, 114, 3007–3015. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, E.; Fastl, H. Psychoacoustics: Facts and Models, 3rd ed.; Springer: Heidelberg, Germany, 1999. [Google Scholar]
- Dratva, J.; Zemp, E.; Felber, D.D.; Brideraux, P.O.; Rochat, T.; Schindler, C.; Gerbase, M.W. Impact of road traffic noise annoyance on health-related quality of life: Results from a population-based study. Qual. Life Res. 2010, 19, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Sunyer, J.; Forsberg, B.; Götschi, T.; Bayer-Oglesby, L.; Ackermann-Liebrich, U.; de Marco, R.; Heinrich, J.; Jarvis, D.; Torén, K.; et al. Annoyance due to air pollution in Europe. Int. J. Epidemiol. 2007, 36, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Klæboe, R.; Kolbenstvedt, M.; Clench-Aas, J.; Bartonova, A. Oslo traffic study—Part 1: An integrated approach to assess the combined effects of noise and air pollution on annoyance. Atmos. Environ. 2000, 34, 4727–4736. [Google Scholar] [CrossRef]
- Roberts, M.J.; Western, A.W.; Webber, M.J. A theory of patterns of pass by noise. J. Sound Vib. 2003, 262, 1047–1056. [Google Scholar] [CrossRef]
- De Coensel, B.; Botteldooren, D.; De Muer, T.; Berglund, B.; Nilsson, M.E.; Lercher, P. A model for the perception of environmental sound based on notice-events. J. Acoust. Soc. Am. 2009, 126, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Lercher, P.; Bockstael, A.; Dekoninck, L.; De Coensel, B.; Botteldooren, D. Can noise from a main road be more annoying than from a highway? An environmental health and soundscape approach. In Proceedings of the 42nd International Congress of Noise Control Engineering (INTER-NOISE 2013), Innsbruck, Austria, 15–18 September 2013.
- Klæboe, R.; Amundsen, A.H.; Fyhri, A. Annoyance from vehicular air pollution: A comparison of European exposure response relationships. Atmos. Environ. 2008, 42, 7689–7694. [Google Scholar] [CrossRef]
- Von Lindern, E.; Hartig, T.; Lercher, P. Traffic-related exposures, constrained restoration, and health in the residential context. Health Place 2016, 39, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Claeson, A.S.; Lidén, E.; Nordin, M.; Nordin, S. The role of perceived pollution and health risk perception in annoyance and health symptoms: A population-based study of odorous air pollution. Int. Arch. Occup. Environ. Health 2013, 86, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, D.; Welch, D.; Dirks, K.N.; Mathews, R. Exploring the relationship between noise sensitivity, annoyance and health-related quality of life in a sample of adults exposed to environmental noise. Int. J. Environ. Res. Public Health 2010, 7, 3579–3594. [Google Scholar] [CrossRef] [PubMed]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, R.P. What is an adverse health effect? Environ. Health Perspect. 1983, 52, 177–182. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Night Noise Guidelines for Europe; World Health Organization (WHO): Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization (WHO). Health and the Environment in the Who European Region: Creating Resilient Communities and Supportive Environments; World Health Organization (WHO): Geneva, Switzerland, 2013. [Google Scholar]
- Salomon, J.A.; Mathers, C.D.; Chatterji, S.; Sadana, R.; Ustun, T.B.; Murray, C.J.L. Quantifying individual levels of health: Definitions, concepts, and measurement issues. In Health Systems Performance Assessment: Debates, Methods and Empiricism; Murray, C.J.L., Evans, D.B., Eds.; World Health Organization (WHO): Geneva, Switzerland, 2003; pp. 301–318. [Google Scholar]
- World Health Organization (WHO). Basic Documents 1948; World Health Organization (WHO): Geneva, Switzerland, 1948. [Google Scholar]
- Kuyken, K.; (on Behalf of WHOQOL Group). The World Health Organization Quality of Life Assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar]
- Vienneau, D.; Perez, L.; Schindler, C.; Lieb, C.; Sommer, H.; Probst-Hensch, N.; Künzlia, N.; Röösli, M. Years of life lost and morbidity cases attributable to transportation noise and air pollution: A comparative health risk assessment for Switzerland in 2010. Int. J. Hyg. Environ. Health 2015, 218, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Tzivian, L.; Winkler, A.; Dlugaj, M.; Schikowski, T.; Vossoughi, M.; Fuks, K.; Weinmayr, G.; Hoffmann, B. Effect of long-term outdoor air pollution and noise on cognitive and psychological functions in adults. Int. J. Hyg. Environ. Health 2015, 218, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Welch, D.; Shepherd, D.; Dirks, K.N.; McBride, D.I.; Marsh, S. Road traffic noise and health-related quality of life: A cross-sectional study. Noise Health 2013, 15, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Wellington Airport. Available online: www.wellingtonairport.co.nz (accessed on 5 February 2016).
- Shepherd, D.; Welch, D.; Dirks, K.N.; McBride, D. Do quiet areas afford greater health-related quality of life than noisy areas? Int. J. Environ. Res. Public Health 2013, 10, 1284–1303. [Google Scholar] [CrossRef] [PubMed]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial—A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Lercher, P. Which health outcomes should be measured in health related environmental quality of life studies? Landsc. Urban Plan 2003, 65, 63–72. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research—Conceptual, strategic, and statistical considerations. J. Personal Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Gan, W.Q.; McLean, K.; Brauer, M.; Chiarello, S.A.; Davies, H.W. Modeling population exposure to community noise and air pollution in a large metropolitan area. Environ. Res. 2012, 116, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E. City dweller responses to multiple stressors intruding into their homes: Noise, light, odour, and vibration. Int. J. Environ. Res. Public Health 2015, 12, 3246–3263. [Google Scholar] [CrossRef] [PubMed]
- De Kluizenaar, Y.; Gansevoort, R.T.; Miedema, H.M.E.; de Jong, P.E. Hypertension and road traffic noise exposure. J. Occup. Environ. Med. 2007, 49, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Honold, J.; Beyer, R.; Lakes, T.; van der Meer, E. Multiple environmental burdens and neighborhood-related health of city residents. J. Environ. Psychol. 2012, 32, 305–317. [Google Scholar] [CrossRef]
- Lercher, P. Combined noise exposure at home. Encycl. Environ. Health 2011, 764–777. [Google Scholar]
- Birk, M.; Ivina, O.; von Klot, S.; Babisch, W.; Heinrich, J. Road traffic noise: Self-reported noise annoyance versus GIS modelled road traffic noise exposure. J. Environ. Monit. 2011, 13, 3237–3245. [Google Scholar] [CrossRef] [PubMed]
- Botteldooren, D.; Lercher, P. Soft computing—Base analyses of the relationship between annoyance and coping with noise and odor. J. Acoust. Soc. Am. 2004, 115, 2974–2985. [Google Scholar] [CrossRef] [PubMed]
- Oiamo, T.H.; Baxter, J.; Grgicak-Mannion, A.; Xu, X.; Luginaah, I.N. Place effects on noise annoyance: Cumulative exposures, odour annoyance and noise sensitivity as mediators of environmental context. Atmos. Environ. 2015, 116, 183–193. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Samples | Auckland Samples | Wellington Samples | ||||
|---|---|---|---|---|---|---|
| Motorway | Non-Motorway | CBD-Suburb | Airport | Non-Airport | Rural | |
| Sex | ||||||
| Male | 93 (34.6) | 105 (43) | 65 (37.6) | 28 (32.6) | 31 (33.3) | 69 (40.4) |
| Female | 171 (63.6) | 140 (57) | 107 (61.8) | 58 (67.4) | 61 (65.6) | 98(57.3) |
| Chi-Square | (χ2 (2) = 3.29, p = 0.078) | (χ2 (1) = 0.05, p = 0.824) | ||||
| Age Group (Years) | ||||||
| 18–20 | 7 (2.6) | 4 (1.6) | 3 (1.7) | 3 (3.4) | 2 (2.2) | 2 (1.2) |
| 21–30 | 36 (13.4) | 14 (5.5) | 15 (8.7) | 7 (8) | 8 (8.6) | 2 (1.2) |
| 31–40 | 47 (17.5) | 68 (26.9) | 22 (12.7) | 16 (18.4) | 18 (19.4) | 22 (12.9) |
| 41–50 | 55 (20.4) | 56 (22.1) | 25 (14.5) | 16 (18.4) | 20 (21.5) | 57 (33.3) |
| 51–60 | 47 (17.5) | 40 (15.8) | 39 (22.7) | 14 (16.1) | 20 (21.5) | 46 (26.9) |
| 61–70 | 35 (13) | 43 (17.0) | 39 (22.7) | 16 (18.4) | 16 (17.2) | 32 (18.7) |
| 70+ | 37 (13.8) | 23 (9.1) | 29(16.9) | 14 (16.1) | 8 (8.6) | 10 (5.8) |
| Chi-Square | (χ2 (7) = 18.51, p = 0.005) | (χ2 (7) = 4.527, p = 0.75) | ||||
| Noise Sensitivity | ||||||
| Low | 98 (38) | 91 (34.9) | 67 (38.7) | 40 (46) | 39 (41.9) | 66 (38.6) |
| Moderate | 125 (50) | 139 (53.3) | 81(46.8) | 33 (37.9) | 41 (44.1) | 79 (46.2) |
| High | 26 (10.4) | 31 (11.9) | 23 (13.3) | 14 (16.1) | 13 (14) | 23 (13.5) |
| Chi-Square | (χ2 (2) = 1.159, p = 0.56) | (χ2 (2) =7.15, p = 0.699) | ||||
| Sample | Auckland Samples | Wellington Samples | ||||
|---|---|---|---|---|---|---|
| Motorway | Non-Motorway | CBD-Suburb | Airport | Non-Airport | Rural | |
| r | 0.566 | 0.317 | 0.537 | 0.630 | 0.461 | 0.377 |
| Partial | 0.532 | 0.292 | 0.456 | 0.633 | 0.492 | 0.355 |
| PHYSICAL HRQOL | |||||
| Predictors | R | R2 | ∆R2 | B (SE) | B |
| Step 1 | 0.446 | 0.199 | 0.199 ** | ||
| Age | 0.035 (0.093) | 0.012 | |||
| Education | 0.683 (0.160) | 0.125 ** | |||
| Gender | 0.385 (0.280) | 0.040 | |||
| Illness | 3.937 (0.300) | 0.397 ** | |||
| Noise Sensitivity | −0.693 (0.206) | −0.099 ** | |||
| Step 2 | 0.482 | 0.132 | 0.033 ** | ||
| Air pollution Annoyance | −0.579 (0.124) | −0.131 ** | |||
| Noise Annoyance | −0.507 (0.121) | −0.117 ** | |||
| Step 3 | 0.484 | 0.134 | 0.002 | ||
| Air × Noise Annoyance | −0.103 (0.087) | −0.096 | |||
| PSYCHOLOGICAL HRQOL | |||||
| Predictors | R | R2 | ∆R2 | B (SE) | B |
| Step 1 | 0.305 | 0.093 | 0.093 ** | ||
| Age | 0.365 (0.077) | 0.155 ** | |||
| Education | 0.658 (0.133) | 0.154 ** | |||
| Gender | 0.170 (0.232) | 0.023 | |||
| Illness | 1.668 (0.249) | 0.215 ** | |||
| Noise Sensitivity | −0.728 (0.170) | −0.133 ** | |||
| Step 2 | 0.339 | 0.115 | 0.022 ** | ||
| Air pollution Annoyance | −0.321 (0.120) | −0.096 * | |||
| Noise Annoyance | −0.260 (0.117) | −0.180 * | |||
| Step 3 | 0.341 | 0.116 | 0.001 | ||
| Air × Noise Annoyance | −0.091 (0.081) | −0.117 | |||
| SOCIAL HRQOL | |||||
| Predictors | R | R2 | ∆R2 | B (SE) | B |
| Step 1 | 0.188 | 0.035 | 0.035 ** | ||
| Age | 0.162 (0.055) | 0.096 | |||
| Education | 0.367 (0.095) | 0.125 ** | |||
| Gender | 0.338 (0.166) | 0.066 | |||
| Illness | 0.609 (0.178) | 0.114 ** | |||
| Noise Sensitivity | −0.176 (0.122) | −0.046 | |||
| Step 2 | 0.237 | 0.056 | 0.021 ** | ||
| Air pollution Annoyance | −0.186 (0.087) | −0.080 * | |||
| Noise Annoyance | −0.207 (0.084) | −0.092 * | |||
| Step 3 | 0.239 | 0.057 | 0.001 | ||
| Air × Noise Annoyance | 0.049 (0.057) | 0.091 | |||
| ENVIRONMENTAL QOL | |||||
| Predictors | R | R2 | ∆R2 | B (SE) | B |
| Step 1 | 0.297 | 0.088 | 0.088 ** | ||
| Age | 0.606 (0.099) | 0.201 ** | |||
| Education | 1.016 (0.171) | 0.187 * | |||
| Gender | 0.699 (0.300) | 0.073 * | |||
| Illness | 1.790 (0.322) | 0.180 ** | |||
| Noise Sensitivity | −0.603 (0.221) | −0.086 * | |||
| Step 2 | 0.410 | 0.168 | 0.080 ** | ||
| Air pollution Annoyance | −0.509 (0.152) | −0.118 ** | |||
| Noise Annoyance | −0.891 (0.146) | −0.213 ** | |||
| Step 3 | 0.413 | 0.171 | 0.002 | ||
| Air × Noise Annoyance | −0.167 (0.102) | −0.167 | |||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shepherd, D.; Dirks, K.; Welch, D.; McBride, D.; Landon, J. The Covariance between Air Pollution Annoyance and Noise Annoyance, and Its Relationship with Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2016, 13, 792. https://doi.org/10.3390/ijerph13080792
Shepherd D, Dirks K, Welch D, McBride D, Landon J. The Covariance between Air Pollution Annoyance and Noise Annoyance, and Its Relationship with Health-Related Quality of Life. International Journal of Environmental Research and Public Health. 2016; 13(8):792. https://doi.org/10.3390/ijerph13080792
Chicago/Turabian StyleShepherd, Daniel, Kim Dirks, David Welch, David McBride, and Jason Landon. 2016. "The Covariance between Air Pollution Annoyance and Noise Annoyance, and Its Relationship with Health-Related Quality of Life" International Journal of Environmental Research and Public Health 13, no. 8: 792. https://doi.org/10.3390/ijerph13080792
APA StyleShepherd, D., Dirks, K., Welch, D., McBride, D., & Landon, J. (2016). The Covariance between Air Pollution Annoyance and Noise Annoyance, and Its Relationship with Health-Related Quality of Life. International Journal of Environmental Research and Public Health, 13(8), 792. https://doi.org/10.3390/ijerph13080792