
Association between Obese Phenotype and Mildly Reduced eGFR among the General Population from Rural Northeast China

Abstract
:1. Introduction
2. Method
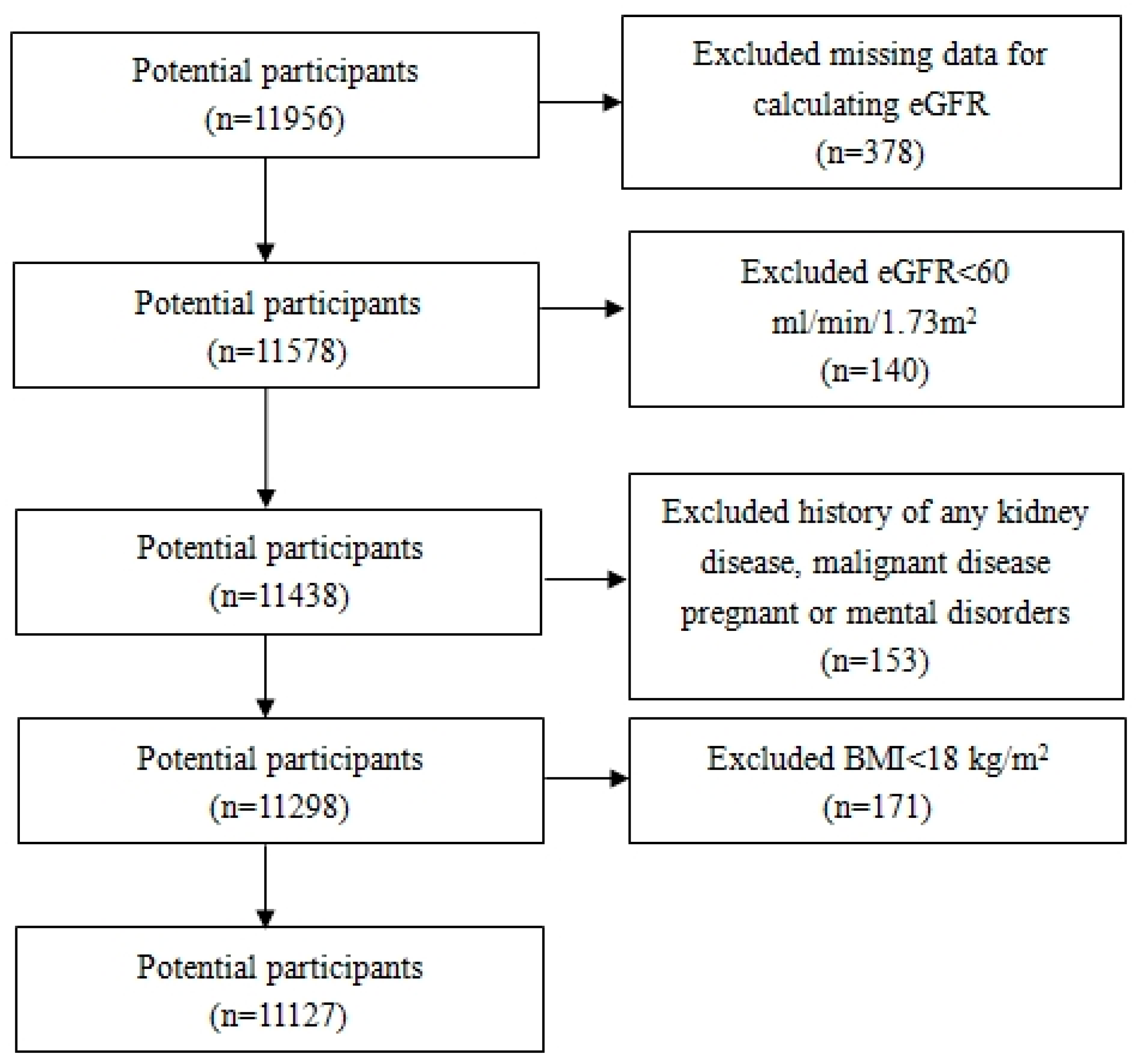
2.1. Study Population
2.2. Data Collection and Measurements
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Characteristics of MHNO, MHO, MANO and MAO Subjects
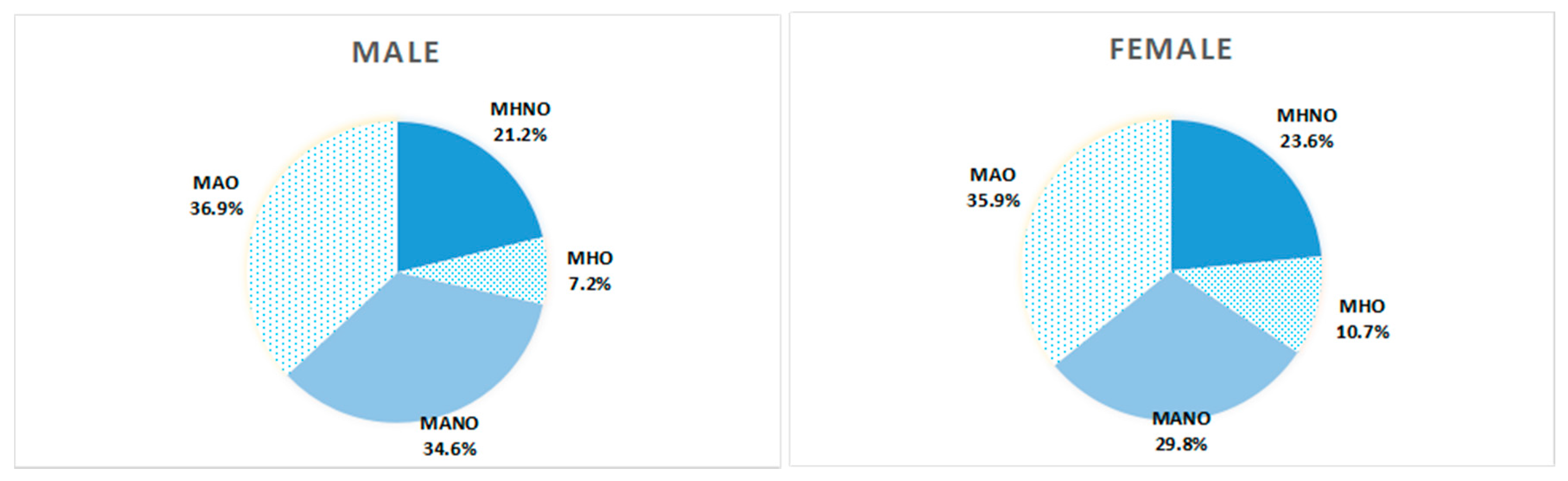
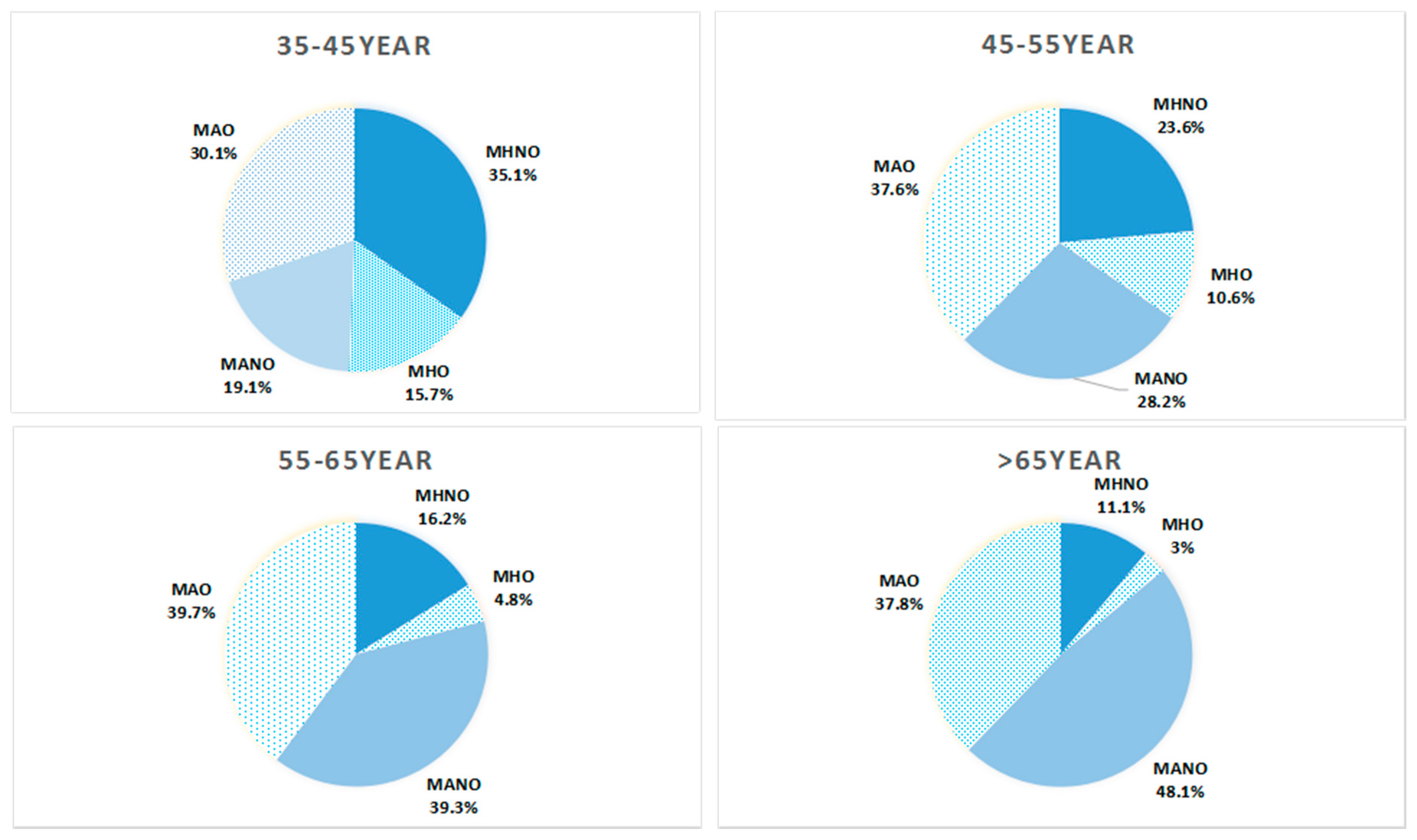
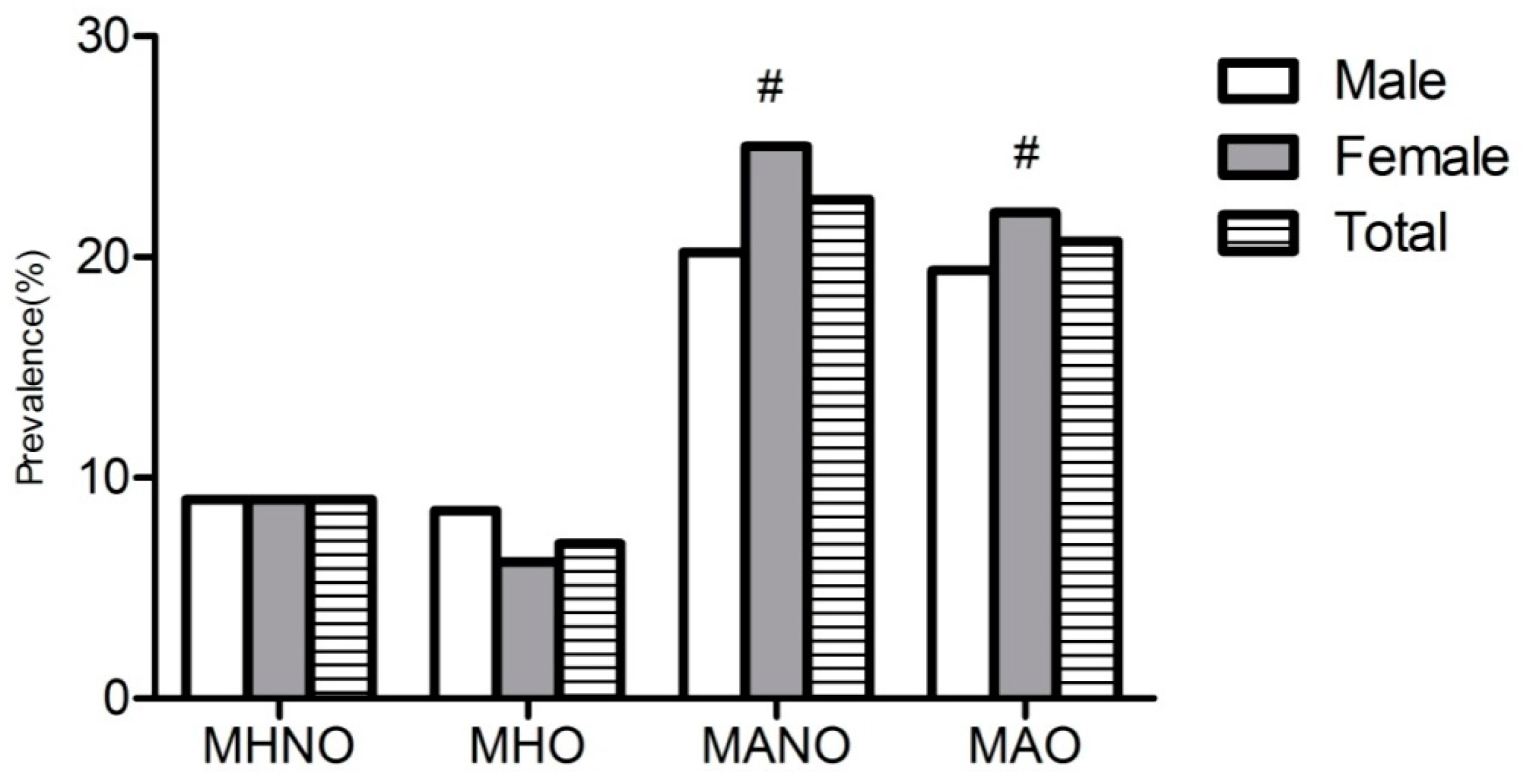
3.2. Characteristics of Obese Phenotype and Mildly Reduced eGFR According to Gender and Age
3.3. Logistic Regression Analysis of the Association between Different Obese Phenotypes and Mildly Reduced eGFR
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Satirapoj, B.; Supasyndh, O.; Mayteedol, N.; Punpanich, D.; Chaiprasert, A.; Nata, N.; Ruangkanchanasetr, P.; Kanjanakul, I.; Choovichian, P. Obesity and its relation to chronic kidney disease: A population-based, cross-sectional study of a Thai army population and relatives. Nephrology 2013, 18, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Malkina, A.; Katz, R.; Shlipak, M.G.; Ix, J.H.; de Boer, I.H.; Sarnak, M.J.; Allison, M.; Kramer, H.J.; Lin, J.; Siscovick, D.; et al. Association of Obesity and Kidney Function Decline among Non-Diabetic Adults with eGFR > 60 mL/min/1.73 m: Results from the Multi-Ethnic Study of Atherosclerosis (MESA). Open J. Endocr. Metab. Dis. 2013, 3, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, E.F.; Sarnak, M.J.; Tighiouart, H.; Griffith, J.L.; Kurth, T.; Salem, D.N.; Levey, A.S.; Weiner, D.E. Waist-to-hip ratio, body mass index, and subsequent kidney disease and death. Am. J. Kidney Dis. 2008, 52, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Sehgal, A.R.; Kashyap, S.R.; Srinivas, T.R.; Kirwan, J.P.; Navaneethan, S.D. Metabolic syndrome and kidney disease: A systematic review and meta-analysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 2364–2373. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Wang, X.; Cai, Q.; Ding, W.; Huang, S.; Zhuo, L. Association of metabolic syndrome with decreased glomerular filtration rate among 75,468 Chinese adults: A cross-sectional study. PLoS ONE 2014, 9, e113450. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.M. Metabolically healthy obesity: Definitions, determinants and clinical implications. Rev. Endocr. Metab. Disord. 2013, 14, 219–227. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Petrie, J.; Littler, W.; de Swiet, M.; Padfield, P.L.; O’Malley, K.; Jamieson, M.; Altman, D.; Bland, M.; Atkins, N. The British Hypertension Society protocol for the evaluation of automated and semi-automated blood pressure measuring devices with special reference to ambulatory systems. J. Hypertens. 1990, 8, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.R.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.C.; Cha, S.C.; Sung, J.W.; So, M.S.; Byrne, C.D. Metabolically healthy obese subjects are at risk of fatty liver but not of pre-clinical atherosclerosis. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Pais, R.; Bellentani, S.; Day, C.P.; Ratziu, V.; Loria, P.; Lonardo, A. From NAFLD in clinical practice to answers from guidelines. J. Hepatol. 2013, 59, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liang, K.; Zhang, X.; Li, C.; Yang, W.; Ma, Z.; Sun, Y.; Song, J.; Lin, P.; Gong, L.; et al. Metabolic abnormalities, but not obesity, contribute to the mildly reduced eGFR in middle-aged and elderly Chinese. Int. Urol. Nephrol. 2014, 46, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Gelber, R.P.; Kurth, T.; Kausz, A.T.; Manson, J.E.; Buring, J.E.; Levey, A.S.; Gaziano, J.M. Association between body mass index and CKD in apparently healthy men. Am. J. Kidney Dis. 2005, 46, 871–880. [Google Scholar] [CrossRef] [PubMed]
- De Boer, I.H.; Katz, R.; Fried, L.F.; Ix, J.H.; Luchsinger, J.; Sarnak, M.J.; Shlipak, M.G.; Siscovick, D.S.; Kestenbaum, B. Obesity and change in estimated GFR among older adults. Am. J. Kidney Dis. 2009, 54, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Artunc, F.; Heyne, N.; Machann, J.; Schleicher, E.D.; Haring, H.U. Obesity and renal disease: Not all fat is created equal and not all obesity is harmful to the kidneys. Nephrol. Dial. Transp. 2014, 31, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Primeau, V.; Coderre, L.; Karelis, A.D.; Brochu, M.; Lavoie, M.E.; Messier, V.; Sladek, R.; Rabasa-Lhoret, R. Characterizing the profile of obese patients who are metabolically healthy. Int. J. Obes. 2011, 35, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Velho, S.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Marques-Vidal, P. Metabolically healthy obesity: Different prevalences using different criteria. Eur. J. Clin. Nutr. 2010, 64, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D. Metabolically healthy but obese individuals. Lancet 2008, 372, 1281–1283. [Google Scholar] [CrossRef]
- Jung, C.H.; Lee, M.J.; Kang, Y.M.; Hwang, J.Y.; Kim, E.H.; Park, J.Y.; Kim, H.K.; Lee, W.J. The risk of chronic kidney disease in a metabolically healthy obese population. Kidney Int. 2015, 88, 843–850. [Google Scholar] [CrossRef] [PubMed]
- De Jong, P.E.; Verhave, J.C.; Pinto-Sietsma, S.J.; Hillege, H.L. Obesity and target organ damage: The kidney. Int. J. Obes. Relat. Metab. Disord. 2002, 26 (Suppl. S4), S21–S24. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Liu, Z.; Xiang, Z.; Zeng, C.; Chen, Z.; Ma, X.; Li, L. Obesity-related glomerulopathy: Insights from gene expression profiles of the glomeruli derived from renal biopsy samples. Endocrinology 2006, 147, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Darouich, S.; Goucha, R.; Jaafoura, M.H.; Zekri, S.; Ben, M.H.; Kheder, A. Clinicopathological characteristics of obesity-associated focal segmental glomerulosclerosis. Ultrastruct. Pathol. 2011, 35, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Salinas, C.A.; Garcia, E.G.; Robles, L.; Riano, D.; Ruiz-Gomez, D.G.; Garcia-Ulloa, A.C.; Melgarejo, M.A.; Zamora, M.; Guillen-Pineda, L.E.; Mehta, R.; et al. High adiponectin concentrations are associated with the metabolically healthy obese phenotype. J. Clin. Endocrinol. Metab. 2008, 93, 4075–4079. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D.; Brochu, M.; Rabasa-Lhoret, R. Can we identify metabolically healthy but obese individuals (MHO)? Diabetes Metab. 2004, 30, 569–572. [Google Scholar] [CrossRef]
- Lynch, L.A.; O’Connell, J.M.; Kwasnik, A.K.; Cawood, T.J.; O’Farrelly, C.; O’Shea, D.B. Are natural killer cells protecting the metabolically healthy obese patient? Obesity 2009, 17, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function—Measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 354, 2473–2483. [Google Scholar] [CrossRef] [PubMed]
- De Hauteclocque, A.; Ragot, S.; Slaoui, Y.; Gand, E.; Miot, A.; Sosner, P.; Halimi, J.M.; Zaoui, P.; Rigalleau, V.; Roussel, R.; et al. The influence of sex on renal function decline in people with type 2 diabetes. Diabet. Med. 2014, 31, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Gackler, D.; Jakel, S.; Fricke, L.; Reinsch, B.; Fischer, F. Diabetes and kidneys. Dtsch. Med. Wochenschr. 2013, 138, 949–955. [Google Scholar] [PubMed]
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.; Levy, D. Predictors of new-onset kidney disease in a community-based population. JAMA 2004, 291, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The atherosclerosis risk in communities study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Hung, C.C.; Kuo, M.C.; Lee, J.J.; Chiu, Y.W.; Chang, J.M.; Hwang, S.J.; Chen, H.C. Association of dyslipidemia with renal outcomes in chronic kidney disease. PLoS ONE 2013, 8, e55643. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.W.; Wan, J.; Liu, Z.S.; Wang, P.; Cheng, G.Y.; Shi, X.Z. Association between dyslipidemia and chronic kidney disease: A cross-sectional study in the middle-aged and elderly Chinese population. Chin. Med. J. 2013, 126, 1207–1212. [Google Scholar] [PubMed]
- Abrass, C.K. Cellular lipid metabolism and the role of lipids in progressive renal disease. Am. J. Nephrol. 2004, 24, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Cases, A.; Coll, E. Dyslipidemia and the progression of renal disease in chronic renal failure patients. Kidney Int. Suppl. 2005, 68, S87–S93. [Google Scholar] [CrossRef] [PubMed]
- Jessani, S.; Levey, A.S.; Bux, R.; Inker, L.A.; Islam, M.; Chaturvedi, N.; Mariat, C.; Schmid, C.H.; Jafar, T.H. Estimation of GFR in South Asians: A study from the general population in Pakistan. Am. J. Kidney Dis. 2014, 63, 49–58. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Scr (μmol/L) | eGFR (mL/min/1.73 m2) |
|---|---|---|
| Female | ≤62 | 144 × (Scr/62)−0.329 × (0.993) age |
| >62 | 144 × (Scr/62)−1.209 × (0.993) age | |
| Males | ≤80 | 144 × (Scr/62)−0.411 × (0.993) age |
| >80 | 144 × (Scr/62)−1.209 × (0.993) age |
| Characteristics | MHNO (n = 2500, 22.5%) | MHO (n = 1009, 9.1%) | MANO (n = 3567, 32.1%) | MAO (n = 4051, 36.4%) | p Value a |
|---|---|---|---|---|---|
| Female (%) | 1392 (55.7) | 632 (62.6) | 1759 (49.3) | 2123 (52.4) | <0.001 |
| Age (years) | 49.60 ± 9.54 | 48.11 ± 8.75 b | 56.79 ± 10.34 b,c | 54.26 ± 9.90 b,c,d | <0.001 |
| BMI (kg/m2) | 22.05 ± 1.74 | 27.45 ± 2.65 b | 22.57 ± 1.68 b,c | 28.10 ± 2.64 b,c,d | <0.001 |
| WC (cm) | 75.07 ± 6.39 | 86.41 ± 7.59 b | 78.23 ± 6.87 b,c | 90.15 ± 7.89 b,c,d | <0.001 |
| Current smoking (%) | 920 (36.8) | 258 (25.6) | 1466 (41.1) | 1271 (31.4) | <0.001 |
| Current drining (%) | 523 (20.9) | 183 (18.1) | 919 (25.8) | 934 (23.1) | <0.001 |
| Systolic BP (mmHg) | 122.58 ± 10.04 | 125.18 ± 9.22 b | 148.29 ± 22.69 b,c | 151.80 ± 22.78 b,c,d | <0.001 |
| Diastolic BP (mmHg) | 73.72 ± 7.36 | 75.89 ± 6.96 b | 84.23 ± 11.47 b,c | 87.06 ± 11.54 b,c,d | <0.001 |
| FBG (mmol/L) | 5.27 ± 0.42 | 5.34 ± 0.42 | 6.06 ± 1.77 b,c | 6.28 ± 1.96 b,c,d | <0.001 |
| TC (mmol/L) | 4.87 ± 0.91 | 4.98 ± 0.93 b | 5.30 ± 1.10 b,c | 5.45 ± 1.11 b,c,d | <0.001 |
| TG (mmol/L) | 0.95 ± 0.32 | 1.06 ± 0.32 b | 1.66 ± 1.57 b,c | 2.17 ± 1.77 b,c,d | <0.001 |
| LDL-C (mmol/L) | 2.62 ± 0.68 | 2.82 ± 0.71 b | 2.92 ± 0.82 b,c | 3.15 ± 0.86 b,c,d | <0.001 |
| HDL-C (mmol/L) | 1.50 ± 0.35 | 1.40 ± 0.31 b | 1.46 ± 0.42 b,c | 1.30 ± 0.34 b,c,d | <0.001 |
| Creatinine (μmol/L) | 69.98 ± 11.85 | 68.90 ± 12.47 | 71.77 ± 14.00 b,c | 72.55 ± 15.09 b,c,d | <0.001 |
| eGFR (mL/min/1.73 m2) | 103.09 ± 29.11 | 103.41 ± 10.02 | 98.24 ± 43.18 b,c | 98.59 ± 23.51 b,c | <0.001 |
| Mildly reduced eGFR (%) | 225 (9.0) | 71 (7.0) | 805 (22.6) | 840 (20.7) | <0.001 |
| Characteristics | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | OR (95%CI) | |||||||
| General | Female | Male | General | Female | Male | General | Female | Male | |
| Female | 1.528 (1.303, 1.975) | - | - | 1.544 (1.319, 1.808) | - | - | 1.475 (1.258, 1.729) | - | - |
| MHNO | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| MHO | 1.097 (0.763, 1.575) | 0.957 (0.591, 1.549) | 1.297 (0.747, 2.251) | 1.039 (0.695, 1.554) | 1.033 (0.604, 1.768) | 1.020 (0.553, 1.883) | 1.107 (0.738, 1.660) | 1.068 (0.622, 1.835) | 1.106 (0.598, 2.047) |
| MANO | 1.042 (0.844, 1.287) | 0.925 (0.693, 1.235) | 1.162 (0.852, 1.585) | 1.026 (0.829, 1.269) | 0.924 (0.690, 1.237) | 1.130 (0.826, 1.547) | 0.800 (0.601, 1.066) | 0.865 (0.589, 1.269) | 0.652 (0.418, 1.018) |
| MAO | 1.604 (1.303, 1.975) | 1.204 (0.909, 1.596) | 2.217 (1.624, 3.026) | 1.496 (1.127, 1.985) | 1.283 (0.873, 1.886) | 1.725 (1.133, 2.627) | 1.119 (0.738, 1.660) | 1.150 (0.725, 1.824) | 0.935 (0.546, 1.600) |
| Age (years) | 1.280 (1.266, 1.294) | 1.304 (1.283, 1.326) | 1.258 (1.239, 1.278) | 1.279 (1.265, 1.294) | 1.303 (1.281, 1.325) | 1.260 (1.241, 1.280) | 1.283 (1.268, 1.298) | 1.308 (1.286, 1.331) | 1.264 (1.244, 1.284) |
| Current smoking | 0.970 (0.832, 1.130) | 0.949 (0.754, 1.196) | 0.951 (0.775, 1.168) | 0.972 (0.833, 1.133) | 0.933 (0.739, 1.178) | 0.968 (0.788, 1.190) | 0.962 (0.824, 1.123) | 0.912 (0.720, 1.155) | 0.965 (0.784, 1.187) |
| Current drinking | 0.528 (0.432, 0.645) | 0.691 (0.399, 1.196) | 0.511 (0.414, 0.631) | 0.528 (0.432, 0.645) | 0.691 (0.399, 1.196) | 0.509 (0.412, 0.629) | 0.535 (0.438, 0.653) | 0.705 (0.407, 1.223) | 0.869 (0.508, 1.486) |
| BMI (kg/m2) | - | - | - | 0.996 (0.959, 1.035) | 0.969 (0.920, 1.02) | 1.050 (0.992, 1.111) | 0.994 (0.957, 1.033) | 0.967 (0.918, 1.018) | 1.050 (0.598, 2.047) |
| WC (cm) | - | - | - | 1.006 (0.995, 1.017) | 1.010 (0.995, 1.025) | 0.998 (0.981, 1.015) | 1.002 (0.991, 1.014) | 1.008 (0.993, 1.023) | 0.992 (0.975, 1.009) |
| Hypertension | - | - | - | - | - | - | 1.028 (0.840, 1.258) | 0.770 (0.593, 1.001) | 1.550 (1.114, 2.158) |
| Hyperglycemia | - | - | - | - | - | - | 1.247 (1.068, 1.455) | 1.265 (1.025, 1.561) | 1.260 (1.001, 1.587) |
| Dyslipidemia | - | - | - | - | - | 1.544 (1.315, 1.814) | 1.509 (1.216, 1.873) | 1.576 (1.232, 2.016) | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, S.; Yang, H.; Guo, X.; Zheng, L.; Sun, Y. Association between Obese Phenotype and Mildly Reduced eGFR among the General Population from Rural Northeast China. Int. J. Environ. Res. Public Health 2016, 13, 540. https://doi.org/10.3390/ijerph13060540
Yu S, Yang H, Guo X, Zheng L, Sun Y. Association between Obese Phenotype and Mildly Reduced eGFR among the General Population from Rural Northeast China. International Journal of Environmental Research and Public Health. 2016; 13(6):540. https://doi.org/10.3390/ijerph13060540
Chicago/Turabian StyleYu, Shasha, Hongmei Yang, Xiaofan Guo, Liqiang Zheng, and Yingxian Sun. 2016. "Association between Obese Phenotype and Mildly Reduced eGFR among the General Population from Rural Northeast China" International Journal of Environmental Research and Public Health 13, no. 6: 540. https://doi.org/10.3390/ijerph13060540