Functional Validity of a Judgment Skills Measure within the Concept of Health Literacy for Sleeping Disorder Patients


Abstract
:1. Introduction


{kind=link}
{kind=link}
| Medication use and adherence | |
|---|---|
| 1 | Your doctor prescribed you a medicine for sleeping disorders. Even though you are sticking to the medical regimen, you can’t fall asleep. How would you react? |
| 2 | You are in bed for more than half an hour and can’t fall asleep. The next day you have an important meeting with your boss/an important family event. What would you do? |
| 3 | A friend tells you about the positive effect of a certain medication, but your doctor doesn’t want to give you a prescription. What would you do? |
| 4 | Your doctor has prescribed you a strong medication for sleeping disorders. You should use this medication only when your usual medication isn’t helping, and you’ve had more than three nights with complaints. You couldn’t sleep last night, and tomorrow you have an important meeting. What would you do? |
| 5 | A friend or family member of yours has been having problems falling asleep for several nights and has been staying awake during the day. Your friend is desperate and asks you for prescription medication to get some sleep, and finally feel better. What would you do? |
| 6 | At the moment you have difficulties falling asleep. A friend or family member currently takes a medication for sleeping disorders that works well. Since you have sleeping problems yourself these days, what would you do? |
| Self-management and knowledge | |
| 7 | Some friends tell you about a new medication for sleeping disorders and their positive experience with it. How would you react? |
| 8 | In the media you heard of a new alternative medication and some home remedies for sleeping disorders. What would you do? |
| 9 | You’ve been having sleeping problems, so you went to your doctor. The doctor asked you about your personal situation, your workplace setting, and your general medical condition. The doctor talks to you about managing sleeping disorders without a medication and doesn’t give you a prescription. How would you react? |
| 10 | For a while you have been taking a medication for sleeping disorders that contains benzodiazepine. These days this medication isn’t working very well for you. The doctor told you to stick to your medical regimen, but you know that slightly overdosing on benzodiazepines isn’t dangerous. What would you do? |
| Social recognition | |
| 11 | You realize that your sleeping disorders disturb your bed partner’s sleep. What would you do? |
| 12 | You stop by a pharmacy for some headache medicine. You realize that you also need a refill of your prescribed medication for sleeping disorders, but you left your prescription at home. The pharmacist says that you can’t get the medication without your prescription in hand. How would you react? |
| 13 | During the day it’s difficult for you to stay awake. You suffer from daytime fatigue and sleepiness. But as you have an appointment in the evening, you want to look refreshed. What would you do? |
| 14 | You are planning a weekend trip with friends. As there are a limited number of rooms in the hotel, you have to share the room with someone else. What would you do in order to avoid your roommate being disturbed by your sleeping problems? |
| Consumption of sleep-active substances | |
| 15 | For several nights you can’t sleep properly. What would you do? |
| 16 | Your medication works best when you reduce the consumption of caffeine, tobacco, and alcohol. You are at a party where everyone is drinking alcohol, and you are offered an alcoholic drink. What would you do? |
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Judgment Skills
2.2.2. Experience of Scenario
2.2.3. Functional Health Literacy
2.2.4. Epworth Sleepiness Scale
2.2.5. Coping with the Condition
2.2.6. Additional Variables
2.3. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics
| Variable | N | % |
|---|---|---|
| All participants | 87 | 100 |
| Gender | ||
| Male | 31 | 35.6 |
| Female | 54 | 62.1 |
| Missing | 2 | 2.3 |
| Age group | ||
| 25–39 | 16 | 18.4 |
| 40–49 | 22 | 25.3 |
| 50–59 | 31 | 35.6 |
| 60–73 | 15 | 17.2 |
| Missing | 3 | 3.4 |
| Mean 50.61 years; SD 10.82 | ||
| Education | ||
| No obligatory school | 1 | 1.1 |
| Obligatory school | 6 | 6.9 |
| Apprenticeship | 33 | 37.9 |
| High school | 16 | 18.4 |
| Professional school | 13 | 14.9 |
| University | 16 | 18.4 |
| Missing | 2 | 2.3 |
| Suffering from sleeping disorders | ||
| Mean 10.95 years; SD 7.83 | ||
| Epworth Sleepiness Scale | ||
| Dangerous situation | 50 | 57.5 |
| Problematic situation | 13 | 14.9 |
| Normal situation | 24 | 27.6 |
| Functional health literacy | ||
| Inadequate | 1 | 1.1 |
| Marginal | 54 | 62.1 |
| Adequate | 32 | 36.8 |
| Judgment Skills | ||
| Low | 46 | 52.9 |
| High | 41 | 47.1 |
3.2. Reliability and Construct Validity
3.3. Differences in Coping
| Item of the Coping Measure | Judgment Skills | Chi2 | df | p | ||
|---|---|---|---|---|---|---|
| High(n = 41) | Low(n = 46) | |||||
| % | % | |||||
| 1 | I wouldn’t share my medication with others | 80.5 | 47.8 | 9.95 | 1 | 0.001 |
| 2 | I wouldn’t take more than my prescribed medication | 70.7 | 56.6 | 1.87 | 1 | 0.13 |
| 3 | I wouldn’t drink alcohol while the time I’m on medication | 68.4 | 50.0 | 2.52 | 1 | 0.09 |
| 4 | It is no problem for me to follow my doctor’s advice | 65.9 | 47.8 | 2.85 | 1 | 0.18 |
| 5 | I feel well treated by my doctor | 65.9 | 41.3 | 5.23 | 1 | 0.02 |
| 6 | It is no problem for me to follow my prescribed medication | 51.5 | 36.6 | 1.66 | 1 | 0.15 |
| 7 | I feel better when I follow my medical treatment | 41.5 | 32.6 | 0.72 | 1 | 0.25 |
| 8 | My disease doesn’t cause big daytime impairments for me | 24.4 | 23.9 | 0.003 | 1 | 0.58 |
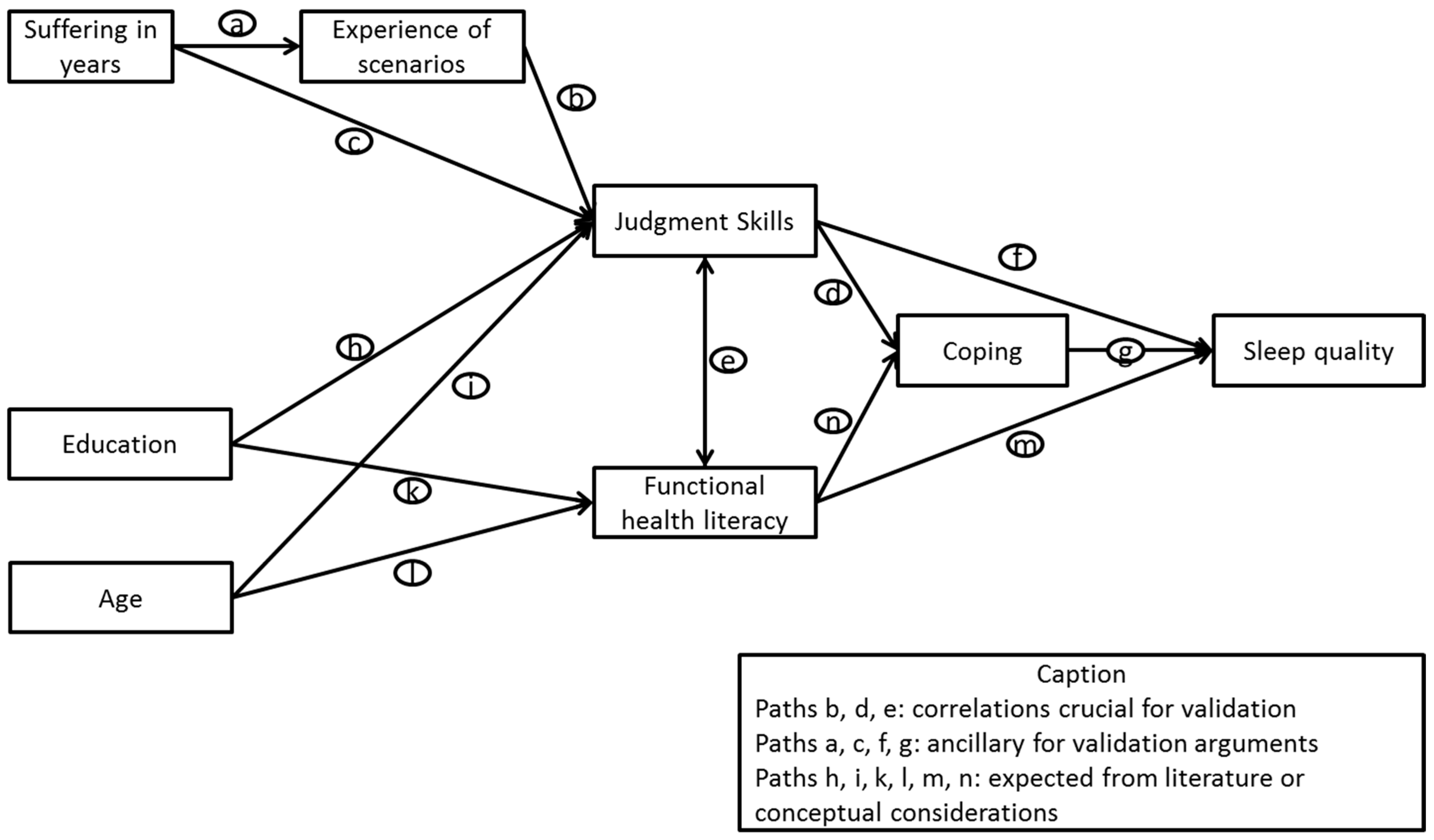
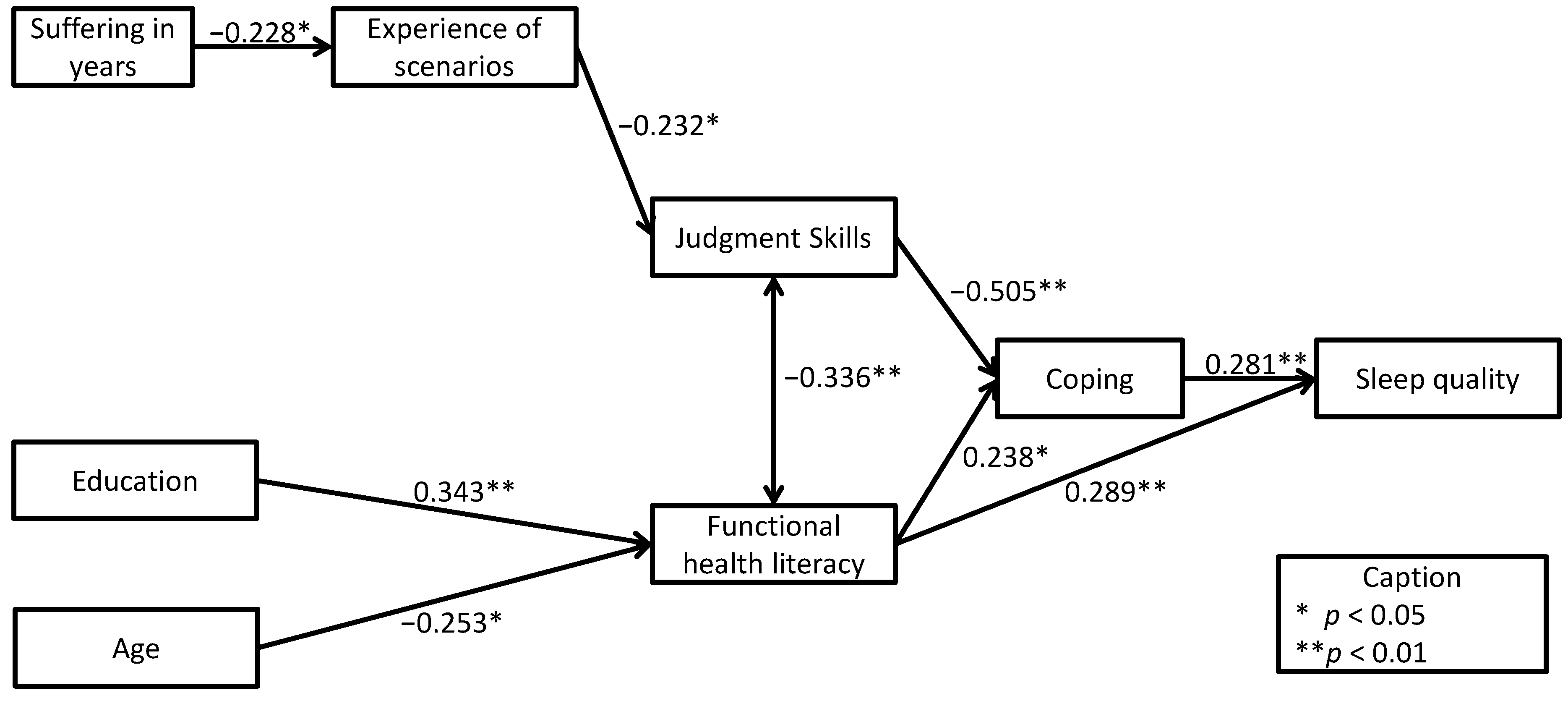
3.4. Scale Correlations in the Path Model
| Scales | Judgment Skills | Experience of Scenarios | Functional Health Literacy | Coping | Sleep Quality | Suffering in Years | Education |
|---|---|---|---|---|---|---|---|
| Experience of scenarios | −0.232 * | ||||||
| Functional health literacy | −0.336 ** | 0.083 | |||||
| Coping | −0.505 ** | 0.238 * | 0.238 * | ||||
| Sleep quality | −0.159 | 0.098 | 0.289 ** | 0.281 ** | |||
| Suffering in years | 0.055 | −0.228 * | −0.012 | 0.128 | 0.017 | ||
| Education | −0.141 | −0.089 | 0.343 ** | 0.116 | 0.045 | 0.154 | |
| Age | 0.004 | 0.074 | −0.253 * | 0.074 | −0.150 | 0.148 | −0.120 |

4. Discussion and Conclusions
4.1. Discussion
4.2. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nutbeam, D. Defining and measuring health literacy: what can we learn from literacy studies. Int. J. Public Health 2009, 54, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Report on the Council of Scientific Affairs, Ad Hoc Committee on health literacy for the Council on Scientific Affairs, American Medical Association. J. Amer. Med. Assoc. 1999, 281, 552–557.
- Institute of Medicine. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Baker, D.W. The meaning and the measure of health literacy. J. Gen. Intern. Med. 2006, 21, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.R. The prevalence of limited health literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Kiuchi, T. Health literacy and health communication. BioPsychoSoc. Med. 2010, 4, 4–18. [Google Scholar] [CrossRef]
- Nielsen-Bohlman, L.; Panzer, A.M.; Kindig, D.A. Health Literacy: A Prescription to End Confusion; The National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Parker, R.M.; Baker, D.W.; Williams, M.V.; Nurss, J.R. The test of functional health literacy in adults: A new instrument for measuring patients’ literacy skills. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef]
- Davis, T.C.; Crouch, M.A.; Long, S.W.; Jackson, R.H.; Bates, P.; George, R.B.; Bairnsfather, L.E. Rapid assessment of literacy levels of adult primary care patients. Fam. Med. 1991, 23, 433–435. [Google Scholar] [PubMed]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Andrus, M.R.; Roth, M.T. Health literacy, a review. Pharmacotherapy 2002, 22, 282–302. [Google Scholar] [CrossRef]
- Mancuso, J.M. Assessment and measurement of health literacy: An integrative review of the literature. Nurs. Health Sci. 2009, 11, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.E.; Osborne, R.H.; Buchbinder, R. Critical appraisal of health literacy indices revealed variable underlying constructs, narrow content and psychometric weaknesses. J. Clin. Epidemiol. 2011, 64, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Chinn, D. Critical health literacy: A review and critical analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.J.; Nakamoto, K. Emerging themes in health literacy. Stud. Communic. Sci. 2006, 5, 1–10. [Google Scholar]
- Rubinelli, S.; Schulz, P.J.; Nakamoto, K. Health literacy beyond knowledge and behavior: Letting the patient be a patient. Int. J. Public Health 2009, 54, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Schulz, P.J.; Nakamoto, K. Health literacy and patient empowerment in health communication: The importance of separating conjoined twins. Patient Educ. Couns. 2013, 90, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Frisch, A.L.; Camerini, L.; Diviani, N.; Schulz, P.J. Defining and measuring health literacy: How can we profit from other literacy domains? Health Promot. Int. 2012, 27, 117–126. [Google Scholar]
- Schulz, P.; Nakamoto, K. “Bad” Literacy, the Internet, and the Limits of Patient Empowerment. AAAI Spring Symposium Series: Artificial Intelligence & Health Communication; n.p.: Stanford, CA, USA, 2011. Available online: www.aaai.org/ocs/index.php/SSS/SSS11/paper/view/2430/2853 (accessed on 15 March 2014).
- Dubowicz, A.; Schulz, P.J. Medical assessments of patient decisions and health literacy. A scenario-based measure of judgment skills. Patient Educ. Couns. 2013, 93, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Chew, L.D.; Bradley, K.A.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Fam. Med. 2004, 36, 588–594. [Google Scholar] [PubMed]
- Gazmarariana, J.A.; Williamsb, M.V.; Peelc, J.; Bakerd, D.W. Health literacy and knowledge of chronic disease. Patient Educ. Couns. 2003, 51, 267–275. [Google Scholar] [CrossRef]
- Schillinger, D.; Bindman, A.; Wang, F.; Stewart, A.; Piettec, J. Functional health literacy and the quality of physician-patient communication among diabetes patients. Patient Educ. Couns. 2004, 52, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Chew, L.D.; Griffin, J.M.; Partin, M.R.; Noorbaloochi, S.; Grill, J.P.; Snyder, A.; Bradley, K.A.; Nugent, S.M.; Baines, A.D.; VanRyn, M. Validation of screening questions for limited health literacy in a large VA outpatient population. J. Gen. Intern. Med. 2008, 23, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Franzen, J.; Mantwill, S.; Rapold, R.; Schulz, P.J. The relationship between functional health literacy and the use of the health system by diabetics in Switzerland. Eur. J. Public Health 2013, 1–7. [Google Scholar]
- Becker, P.M. Insomnia: Prevalence, impact, pathogenesis, differential diagnosis, and evaluation. Psychiatr. Clin. North Am. 2006, 29, 855–870. [Google Scholar] [CrossRef] [PubMed]
- Grewal, R.; Doghramji, K. Epistemology of Insomnia. In Clinical Handbook of Insomnia, 2nd ed.; Attarian, H.P., Schuman, C.S., Eds.; Springer: New York, NY, USA, 2010; pp. 13–22. [Google Scholar]
- Lichstein, K.L.; Durrence, H.H.; Taylor, D.J.; Bush, A.J.; Riedel, B.W. Quantitative criteria for insomnia. Behav. Res. Ther. 2003, 41, 427–445. [Google Scholar] [CrossRef] [PubMed]
- Observatoire suisse de la santé et Dipartimento della sanità e della socialità del Can-tone Ticino. La santé dans le Canton du Tessin. Analyse des données de l’Enquête suisse sur la santé 2007 (Obsan rapport 44) (Health Report of the Canton of Ticino); Observatoire suisse de la santé: Neuchâtel, Switzerland, 2010.
- Holbrook, A.M.; Crowther, R.; Lotter, A.; Cheng, C.; King, D. Meta-analysis of benzodiazepine use in the treatment of insomnia. CMAJ 2000, 162, 389–390. [Google Scholar]
- Casati, A.; Sedefov, R.; Pfeiffer-Gerschel, T. Misuse of medicines in the European Union: A systematic review of the literature. Eur. Addict. Res. 2012, 18, 228–245. [Google Scholar]
- Finfgeld-Connett, D.L. Treatment of substance misuse in older women: Using a brief intervention model. J. Gerontolo. Nurs. 2004, 30, 30–37. [Google Scholar] [CrossRef]
- Hackney, J.E.; Weaver, T.E.; Pack, A.I. Health literacy and sleep disorders: A review. Sleep Med. Rev. 2008, 12, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.; Sharpley, A.; Ree, M.; Stinson, K.; Clark, D. An open trial of cognitive therapy for chronic insomnia. Behav. Res. Ther. 2003, 45, 2491–501. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [PubMed]
- Vignatelli, L.; Plazzi, G.; Barbato, A.; Ferini-Strambi, L.; Manni, R.; Pompei, F.; D’Alessandro, R.; GINSEN (Gruppo Italiano Narcolessia Studio Epidemiologico Nazionale). Italian version of the Epworth sleepiness scale: External validity. Neurol. Sci. 2003, 23, 295–300. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 21.0; IBM Corp.: Armonk, NY, USA, 2012.
- Roth, T. Insomnia: Definition, prevalence, etiology, and consequences. J. Clin. Sleep Med. 2007, 3, 7–10. [Google Scholar]
- OECD. Educational Attainment. OECD Factbook 2013: Economic, Environmental and Social Statistics; OECD Publishing: Paris, France, 2013. Available online: http://dx.doi.org/10.1787/factbook-2013-77-en (accessed on 5 March 2014).
- Schillinger, D.; Piette, J.; Grumbach, K.; Wang, F.; Wilson, W.; Daher, C.; Leong-Grotz, K.; Castro, C.; Bindman, A.B. Closing the loop. Physician communication with diabetic patients who have low health literacy. Arch. Intern. Med. 2003, 163, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Connor, M.; Mantwill, S.; Schulz, P.J. Functional health literacy in Switzerland—Validation of a German, Italian, and French health literacy test. Patient Educ. Couns. 2013, 90, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.W.; Williams, M.V.; Parker, R.M.; Gazmararian, J.A.; Nurss, J. Development of a brief test to measure functional health literacy. Patient Educ. Couns. 1999, 38, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Nomura, K.; Sato, M.; Yano, E. Developing a measure of communicative and critical health literacy: A pilot study of Japanese office workers. Health Promot. Int. 2008, 23, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubowicz, A.; Schulz, P.J. Functional Validity of a Judgment Skills Measure within the Concept of Health Literacy for Sleeping Disorder Patients. Int. J. Environ. Res. Public Health 2014, 11, 10868-10882. https://doi.org/10.3390/ijerph111010868
Dubowicz A, Schulz PJ. Functional Validity of a Judgment Skills Measure within the Concept of Health Literacy for Sleeping Disorder Patients. International Journal of Environmental Research and Public Health. 2014; 11(10):10868-10882. https://doi.org/10.3390/ijerph111010868
Chicago/Turabian StyleDubowicz, Arthur, and Peter J. Schulz. 2014. "Functional Validity of a Judgment Skills Measure within the Concept of Health Literacy for Sleeping Disorder Patients" International Journal of Environmental Research and Public Health 11, no. 10: 10868-10882. https://doi.org/10.3390/ijerph111010868