The Impact of the COVID-19 Pandemic on Gastrointestinal Endoscopy Activity in a Tertiary Care Center from Northeastern Romania

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Internal Protocol
2.2. Statistical Analysis
3. Results
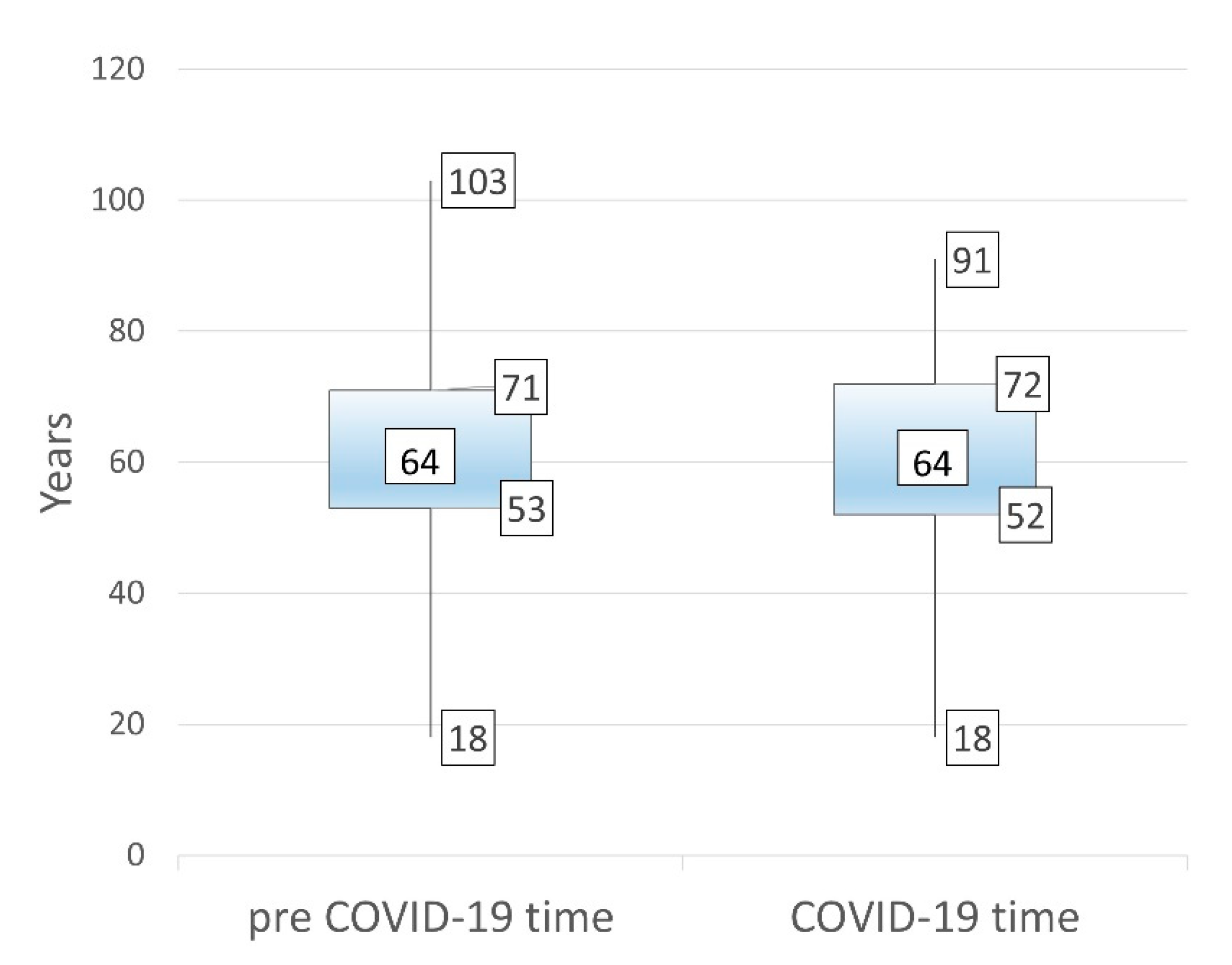
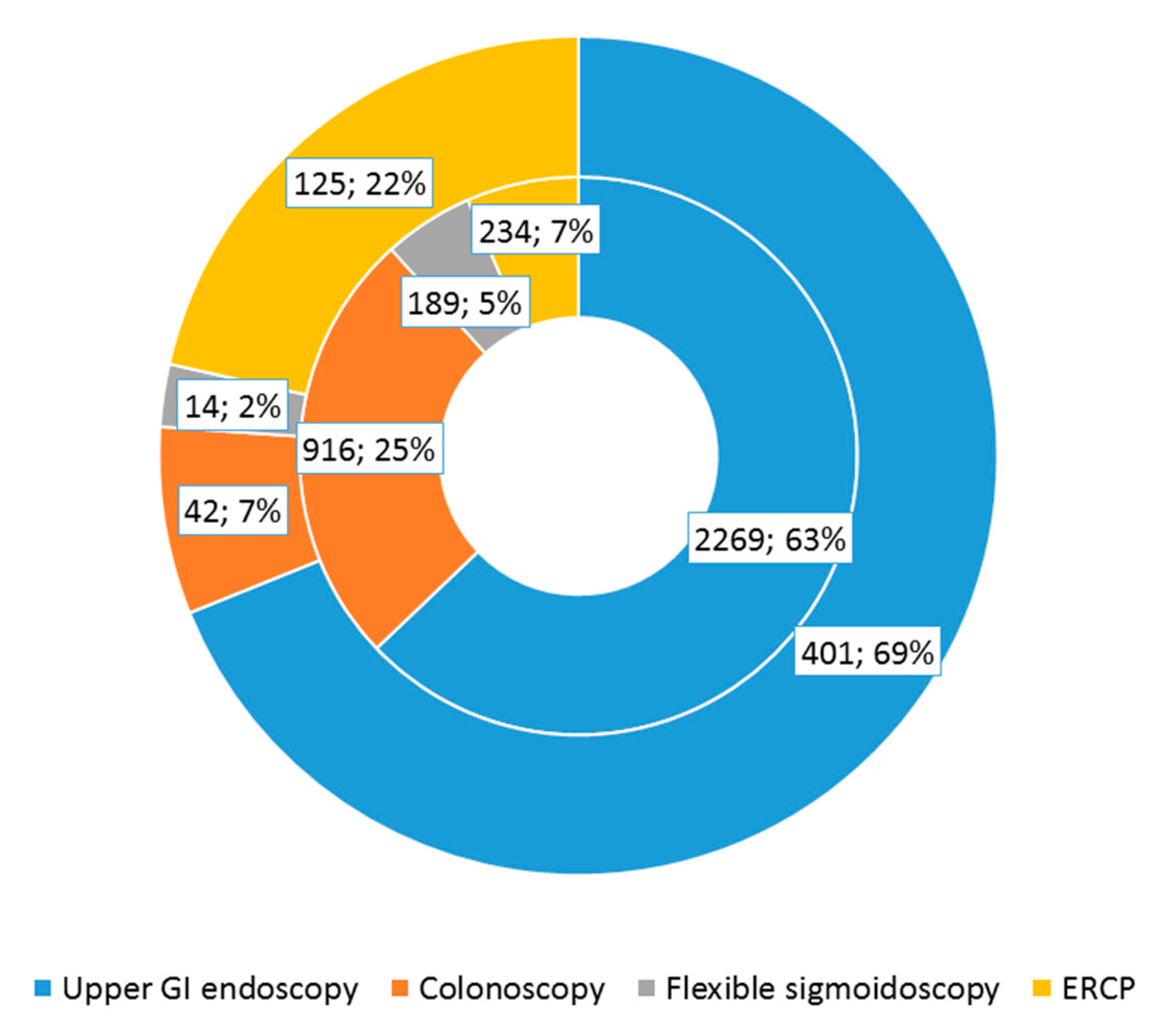
3.1. General Findings
3.2. Training Analysis
3.3. Upper and Lower GI Endoscopy Analysis
3.4. ERCP Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. Infect. Public Health. 2020, 13, 667–673. [Google Scholar] [CrossRef]
- Johns Hopkins University. Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE). Available online: https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 5 October 2020).
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Alboraie, M.; Piscoya, A.; Tran, Q.T.; Mendelsohn, R.B.; Butt, A.S.; Lenz, L.; Alavinejad, P.; Emara, M.H.; Samlani, Z.; Altonbary, A.; et al. The global impact of COVID-19 on gastrointestinal endoscopy units: An international survey of endoscopists. Arab. J. Gastroenterol. 2020, 21, 156–161. [Google Scholar] [CrossRef]
- Rutter, M.D.; Brookes, M.; Lee, T.J.; Rogers, P.; Sharp, L. Impact of the COVID-19 pandemic on UK endoscopic activity and cancer detection: A National Endoscopy Database Analysis. Gut 2020, 1–7. [Google Scholar] [CrossRef]
- Arantes, V.N.; Martins, B.C.; Seqatto, R.; Milhomen-Cardoso, D.M.; Franzini, T.P.; Zuccaro, A.M.; Alves, J.S.; Maluf-Filho, F. Impact of coronavirus pandemic crisis in endoscopic clinical practice: Results from a national survey in Brazil. Endosc. Int. Open. 2020, 8, E822–E829. [Google Scholar] [CrossRef]
- Repici, A.; Pace, F.; Gabbiadini, R.; Colombo, M.; Hassan, C.; Dinelli, M.; ITALIAN GI-COVID19 Working Group. Endoscopy Units and the Coronavirus Disease 2019 Outbreak: A Multicenter Experience from Italy. Gastroenterology 2020, 159, 363–366. [Google Scholar] [CrossRef]
- Repici, A.; Maselli, R.; Colombo, M.; Gabbiadini, R.; Spadaccini, M.; Anderloni, A.; Carrara, S.; Fugazza, A.; Di Leo, M.; Galtieri, P.A.; et al. Coronavirus (COVID-19) outbreak: What the department of endoscopy should know. Gastrointest. Endosc. 2020, 92, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Fennelly, K.P. Particle sizes of infectious aerosols: Implications for infection control. Lancet Respir. Med. 2020, 8, 914–924. [Google Scholar] [CrossRef]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal-Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef]
- Guda, N.M.; Emura, F.; Reddy, D.N.; Rey, J.F.; Seo, D.W.; Gyokeres, T.; Tajiri, H.; Faigel, D. Recommendations for the Operation of Endoscopy Centers in the setting of the COVID-19 pandemic—World Endoscopy Organization guidance document. Dig. Endosc. 2020, 32, 844–850. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Hassan, C.; Beilenhoff, U.; Antonelli, G.; Ebigbo, A.; Pellisè, M.; Arvanitakis, M.; Bhandari, P.; Bisschops, R.; Van Hooft, J.E.; et al. ESGE and ESGENA Position Statement on gastrointestinal endoscopy and the COVID-19 pandemic. Endoscopy 2020, 52, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, P.W.Y.; Ng, S.C.; Inoue, H.; Reddy, D.N.; Ling, H.E.; Cho, J.Y.; Ho, L.K.; Hewett, D.G.; Chiu, H.M.; Rerknimitr, R.; et al. Practice of endoscopy during COVID-19 pandemic: Position statements of the Asian Pacific Society for Digestive Endoscopy (APSDE-COVID statements). Gut 2020, 69, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Lim, J.K.; Altayar, O.; Davitkov, P.; Feuerstein, J.D.; Siddique, S.M.; Falck-Ytter, Y.; El-Serag, H.B.; AGA Institute. AGA Rapid Recommendations for Gastrointestinal Procedures During the COVID-19 Pandemic. Gastroenterology 2020, 159, 739–758. [Google Scholar] [CrossRef] [PubMed]
- Das, A. Impact of the COVID-19 pandemic on the workflow of an ambulatory endoscopy center: An assessment by discrete event simulation. Gastrointest. Endosc. 2020, 92, 914–924. [Google Scholar] [CrossRef]
- Pawlak, K.M.; Kral, J.; Khan, R.; Amin, S.; Bilal, M.; Lui, R.N.; Sandhu, D.S.; Hashim, A.; Bollipo, S.; Charabaty, A.; et al. Impact of COVID-19 on endoscopy trainees: An international survey. Gastrointest. Endosc. 2020, 92, 925–935. [Google Scholar] [CrossRef]
- Repici, A.; Aragona, G.; Cengia, G.; Cantù, P.; Spadaccini, M.; Maselli, R.; Carrara, S.; Anderloni, A.; Fugazza, A.; Pace, F.; et al. Low risk of covid-19 transmission in GI endoscopy. Gut 2020, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Forbes, N.; Smith, Z.L.; Spitzer, R.L.; Keswani, R.N.; Wani, S.B.; Elmunzer, B.J.; North American Alliance for the Study of Digestive Manifestations of COVID-19. Changes in Gastroenterology and Endoscopy Practices in Response to the Coronavirus Disease 2019 Pandemic: Results from a North American Survey. Gastroenterology 2020, 159, 772–774. [Google Scholar] [CrossRef]
- Dinmohamed, A.G.; Visser, O.; Verhoeven, R.H.A.; Louwman, M.W.J.; van Nederveen, F.H.; Willems, S.M.; Merkx, M.A.W.; Lemmens, V.E.P.P.; Nagtegaal, I.D.; Siesling, S. Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands. Lancet Oncol. 2020, 21, 750–751. [Google Scholar] [CrossRef]
- Zhu, L.; Cai, M.Y.; Shi, Q.; Wang, P.; Li, Q.L.; Zhong, Y.S.; Yao, L.Q.; Zhou, P.H. Analysis of selective endoscopy results during the epidemic of coronavirus disease 2019 (COVID-19). Zhonghua Wei Chang. Wai Ke Za Zhi. 2020, 23, 327–331. [Google Scholar]
- Kushnir, V.M.; Berzin, T.M.; Elmunzer, B.J.; Mendelsohn, R.B.; Patel, V.; Pawa, S.; Smith, Z.L.; Keswani, R.N.; North American Alliance for the Study of Digestive Manifestations of COVID-19. Plans to Reactivate Gastroenterology Practices Following the COVID-19 Pandemic: A Survey of North American Centers. Clin. Gastroenterol. Hepatol. 2020, 18, 2287–2294. [Google Scholar] [CrossRef]
- Hennessy, B.; Vicari, J.; Bernstein, B.; Chapman, F.; Khaykis, I.; Littenberg, G.; Robbins, D. Guidance for resuming GI endoscopy and practice operations after the COVID-19 pandemic. Gastrointest. Endosc. 2020, 92, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Hayee, B.; Thoufeeq, M.; Rees, C.J.; Penman, I.; East, J. Safely restarting GI endoscopy in the era of COVID-19. Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- Soetikno, R.; Teoh, A.Y.B.; Kaltenbach, T.; Lau, J.Y.W.; Asokkumar, R.; Cabral-Prodigalidad, P.; Shergill, A. Considerations in performing endoscopy during the COVID-19 pandemic. Gastrointest. Endosc. 2020, 91, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.C.; Shen, L.; Lee, L.S. COVID-19 in endoscopy: Time to do more? Gastrointest Endosc. 2020, 92, 435–439. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Pre COVID-19 Time 3608 | COVID-19 Time 582 | p |
|---|---|---|---|
| Sex, women:men, n (%) | 1620 (44.9):1987 (55.1) | 235 (40.4):347 (59.6) | 0.041 |
| Emergency upper/lower GI endoscopy, n (%) | 947 (26.2) | 226 (38.8) | <0.001 |
| Fellow involvement, n (%) | 3250 (90) | 238 (40.9) | <0.001 |
| Procedure Type/Result | Pre COVID-19 Time 3374 | COVID-19 Time 457 | p |
|---|---|---|---|
| GI Endoscopy Indications, n (%) | |||
| Upper GI bleeding, n (%) | 823 (24.4) | 194 (42.5) | <0.001 |
| Lower GI bleeding, n (%) | 290 (8.6) | 20 (4.4) | 0.002 |
| Anemia, n (%) | 335 (9.9) | 37 (8.1) | 0.148 |
| Chronic abdominal pain, n (%) | 392 (11.6) | 9 (2) | <0.001 |
| Change in frequency of stool/vomiting, n (%) | 245 (7.3) | 34 (7.4) | 0.895 |
| Weight loss, n (%) | 79 (2.3) | 4 (0.9) | 0.032 |
| Control of gastric ulcer/polyps/cancer, n (%) | 175 (5.2) | 6 (1.3) | 0.001 |
| CT/MRI suspicion of neoplasia | 30 (0.9) | 0 | 0.042 |
| Others (dysphagia, screening for esophageal varices), n (%) | 1005 (29.8) | 153 (33.5) | 0.929 |
| GI Endoscopy Results | |||
| GI neoplasia, n (%) | 249 (7.4) | 57 (12.5) | 0.001 |
| GI polyps, n (%) | 468 (13.9) | 9 (2) | <0.001 |
| Gastric/duodenal ulcer, n (%) | |||
| Forrest 3, n (%) | 185 (5.5) | 40 (8.8) | 0.002 |
| Forrest 1-2, n (%) | 242 (7.2) | 45 (9.8) | 0.69 |
| Esophageal varix, n (%) | 364 (10.8) | 80 (17.5) | <0.001 |
| Others (gastritis, esophagitis, diverticular disease, hemorrhoids), n (%) | 1666 (46.4) | 201 (44) | 0.154 |
| UC/Crohn’s disease, n (%) | 91 (2.7) | 18 (3.9) | 0.134 |
| Normal findings, n (%) | 69 (2) | 1 (0.2) | 0.006 |
| Achalasia, n (%) | 35 (1) | 3 (0.7) | 0.616 |
| Esophageal benign stenosis, n (%) | 5 (0.1) | 3 (0.7) | 0.60 |
| Interventions Performed | |||
| Variceal band ligation, n (%) | 42 (1.24) | 14 (3.06) | 0.715 |
| Ulcer hemostasis, n (%) | 97 (2.87) | 21 (4.59) | 0.039 |
| Bougie dilation of esophageal benign strictures, n (%) | 14 (0.41) | 4 (0.87) | 0.792 |
| Balloon dilation of esophageal benign strictures, n (%) | 24 (0.71) | 7 (1.53) | 0.987 |
| Esophageal cancer stent placement, n (%) | 5 (0.14) | 1 (0.2) | 0.610 |
| Polypectomy/EMR, n (%) | 170 (5.03) | 3 (0.2) | <0.001 |
| PEG, n (%) | 5 (0.14) | 2 (0.43) | 0.752 |
| Pyloric balloon dilation, n (%) | 1 (0.02) | 0 | 0.954 |
| Success, n (%) | 325 (90.7) | 49 (94.2) | 0.01 |
| Early complications (bleeding/perforation), n (%) | 69 (19.2) | 4 (7.6) | <0.001 |
| Delayed complications (bleeding/perforation), n (%) | 7 (1.9) | 0 (0) | 0.395 |
| Procedure Type/Result | Pre COVID-19 Time 233 | COVID-19 Time 124 | p |
|---|---|---|---|
| ERCP indications | |||
| Cholangitis, n (%) | 25 (10.7) | 16 (12.9) | 0.540 |
| CBD stones, n (%) | 164 (70.4) | 81 (65.3) | 0.302 |
| Cholangiocarcinoma, n (%) | 32 (13.7) | 21 (16.9) | 0.700 |
| Pancreatic cancer, n (%) | 22 (9.4) | 15 (12.1) | 0.491 |
| Postoperative biliary lesion, n (%) | 6 (2.6) | 2 (1.6) | 0.171 |
| Others (lymph node metastasis/hepatic metastasis) | 7 (3) | 4 (3.2) | 0.852 |
| ERCP Results | |||
| Complications | |||
| Immediate bleeding Perforation | 27 (11.6) 1 (0.4) | 9 (7.3) 1 (0.8) | 0.196 0.649 |
| Stent placement | 50 (21.4) | 30 (24.1) | 0.378 |
| Therapeutic success | 199 (87.7) | 90 (76.3) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiriac, S.; Stanciu, C.; Cojocariu, C.; Sfarti, C.; Singeap, A.-M.; Girleanu, I.; Cuciureanu, T.; Huiban, L.; David, D.; Zenovia, S.; et al. The Impact of the COVID-19 Pandemic on Gastrointestinal Endoscopy Activity in a Tertiary Care Center from Northeastern Romania. Healthcare 2021, 9, 100. https://doi.org/10.3390/healthcare9010100
Chiriac S, Stanciu C, Cojocariu C, Sfarti C, Singeap A-M, Girleanu I, Cuciureanu T, Huiban L, David D, Zenovia S, et al. The Impact of the COVID-19 Pandemic on Gastrointestinal Endoscopy Activity in a Tertiary Care Center from Northeastern Romania. Healthcare. 2021; 9(1):100. https://doi.org/10.3390/healthcare9010100
Chicago/Turabian StyleChiriac, Stefan, Carol Stanciu, Camelia Cojocariu, Catalin Sfarti, Ana-Maria Singeap, Irina Girleanu, Tudor Cuciureanu, Laura Huiban, Diana David, Sebastian Zenovia, and et al. 2021. "The Impact of the COVID-19 Pandemic on Gastrointestinal Endoscopy Activity in a Tertiary Care Center from Northeastern Romania" Healthcare 9, no. 1: 100. https://doi.org/10.3390/healthcare9010100