
Real-World Dispensing of Buprenorphine in California during Prepandemic and Pandemic Periods

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCartney, M. The fall of a poisoned empire. Lancet 2022, 399, 135. [Google Scholar] [CrossRef]
- Slavova, S.; Rock, P.; Bush, H.M.; Quesinberry, D.; Walsh, S.L. Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug Alcohol Depend. 2020, 214, 108176. [Google Scholar]
- Rodda, L.N.; West, K.L.; LeSaint, K.T. Opioid overdose–related emergency department visits and accidental deaths during the COVID-19 pandemic. J. Urban Health 2020, 97, 808–813. [Google Scholar]
- National Vital Statistics System. Provisional Drug Overdose Death Counts. Available online: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm (accessed on 1 September 2023).
- California Department of Health Care Services. California Response to the Overdose Crisis. Available online: https://www.californiamat.org/wp-content/uploads/2020/05/MAT_Flyers_DHCS_Opioid_Crisis.pdf (accessed on 1 September 2023).
- Scott, L.C.; Lewis, S. Opioids for chronic pain. JAMA 2016, 315, 1672. [Google Scholar] [CrossRef]
- Comer, S.; Cunningham, C.; Fishman, M.J.; Gordon, F.A.; Kampman, F.K.; Langleben, D.; Nordstrom, B.; Oslin, D.; Woody, G.; Wright, T. National practice guideline for the use of medications in the treatment of addiction involving opioid use. Am. Soc. Addicit. Med. 2015, 66, 39–42. [Google Scholar]
- Morgan, J.R.; Schackman, B.R.; Weinstein, Z.M.; Walley, A.Y.; Linas, B.P. Overdose following initiation of naltrexone and buprenorphine medication treatment for opioid use disorder in a United States commercially insured cohort. Drug Alcohol Depend. 2019, 200, 34–39. [Google Scholar] [CrossRef]
- Roehler, D.R.; Guy, G.P., Jr.; Jones, C.M. Buprenorphine prescription dispensing rates and characteristics following federal changes in prescribing policy, 2017–2018: A cross-sectional study. Drug Alcohol Depend. 2020, 213, 108083. [Google Scholar]
- Krawczyk, N.; Rivera, B.D.; Jent, V.; Keyes, K.M.; Jones, C.M.; Cerdá, M. Has the treatment gap for opioid use disorder narrowed in the US?: A yearly assessment from 2010 to 2019. Int. J. Drug Policy 2022, 110, 103786. [Google Scholar] [CrossRef]
- Lanham, H.J.; Papac, J.; Olmos, D.I.; Heydemann, E.L.; Simonetti, N.; Schmidt, S.; Potter, J.S. Survey of barriers and facilitators to prescribing buprenorphine and clinician perceptions on the Drug Addiction Treatment Act of 2000 waiver. JAMA Netw. Open 2022, 5, e2212419. [Google Scholar] [CrossRef]
- Gordon, A.J.; Kenny, M.; Dungan, M.; Gustavson, A.M.; Kelley, A.T.; Jones, A.L.; Hawkins, E.; Frank, J.W.; Danner, A.; Liberto, J. Are x-waiver trainings enough? Facilitators and barriers to buprenorphine prescribing after x-waiver trainings. Am. J. Addict. 2022, 31, 152–158. [Google Scholar] [CrossRef]
- Andrilla, C.H.A.; Jones, K.C.; Patterson, D.G. Prescribing practices of nurse practitioners and physician assistants waivered to prescribe buprenorphine and the barriers they experience prescribing buprenorphine. J. Rural Health 2020, 36, 187–195. [Google Scholar] [CrossRef]
- Huhn, A.S.; Dunn, K.E. Why aren’t physicians prescribing more buprenorphine? J. Subst. Abus. Treat. 2017, 78, 1–7. [Google Scholar] [CrossRef]
- Herring, A.A.; Kalmin, M.; Speener, M.; Goodman-Meza, D.; Snyder, H.; Campbell, A.; Moulin, A.; Shoptaw, S. Sharp decline in hospital and emergency department initiated buprenorphine for opioid use disorder during COVID-19 state of emergency in California. J. Subst. Abus. Treat. 2021, 123, 108260. [Google Scholar]
- Haddad, M.S.; Zelenev, A.; Altice, F.L. Integrating buprenorphine maintenance therapy into federally qualified health centers: Real-world substance abuse treatment outcomes. Drug Alcohol Depend. 2013, 131, 127–135. [Google Scholar] [CrossRef]
- Tiako, M.J.N. Addressing racial & socioeconomic disparities in access to medications for opioid use disorder amid COVID-19. J. Subst. Abus. Treat. 2021, 122, 108214. [Google Scholar]
- Krawczyk, N.; Williams, A.R.; Saloner, B.; Cerdá, M. Who stays in medication treatment for opioid use disorder? A national study of outpatient specialty treatment settings. J. Subst. Abus. Treat. 2021, 126, 108329. [Google Scholar]
- Hirchak, K.A.; Amiri, S.; Kordas, G.; Oluwoye, O.; Lyons, A.J.; Bajet, K.; Hahn, J.A.; McDonell, M.G.; Campbell, A.N.; Venner, K. Variations in national availability of waivered buprenorphine prescribers by racial and ethnic composition of zip codes. Subst. Abus. Treat. Prev. Policy 2022, 17, 41. [Google Scholar] [CrossRef]
- Ghoshal, M. How Race Affects Access to Opioid Use Disorder Medications. Advances in Addiction & Recovery. Winter 2021. Available online: https://www.naadac.org/assets/2416/aa&r_winter2021_how_race_affects_access_to_opioid_use_disorder_medications.pdf (accessed on 1 September 2023).
- Mauro, P.M.; Gutkind, S.; Annunziato, E.M.; Samples, H. Use of medication for opioid use disorder among US adolescents and adults with need for opioid treatment, 2019. JAMA Netw. Open 2022, 5, e223821. [Google Scholar]
- Neale, K.J.; Weimer, M.B.; Davis, M.P.; Jones, K.F.; Kullgren, J.G.; Kale, S.S.; Childers, J.; Broglio, K.; Merlin, J.S.; Peck, S. Top ten tips palliative care clinicians should know about buprenorphine. J. Palliat. Med. 2023, 26, 120–130. [Google Scholar]
- Huskamp, H.A.; Busch, A.B.; Uscher-Pines, L.; Barnett, M.L.; Riedel, L.; Mehrotra, A. Treatment of opioid use disorder among commercially insured patients in the context of the COVID-19 pandemic. JAMA 2020, 324, 2440–2442. [Google Scholar]
- Nguyen, T.D.; Gupta, S.; Ziedan, E.; Simon, K.I.; Alexander, G.C.; Saloner, B.; Stein, B.D. Assessment of filled buprenorphine prescriptions for opioid use disorder during the coronavirus disease 2019 pandemic. JAMA Intern. Med. 2021, 181, 562–565. [Google Scholar] [CrossRef]
- Cantor, J.; Dick, A.W.; Haffajee, R.; Pera, M.F.; Bravata, D.M.; Stein, B.D.; Whaley, C. Use of buprenorphine for those with employer-sponsored insurance during the initial phase of the COVID-19 pandemic. J. Subst. Abus. Treat. 2021, 129, 108384. [Google Scholar]
- Chalasani, R.; Shinabery, J.M.; Goetz, C.T.; Chang, C.-C.H.; Yang, Q.; Suda, K.J.; Gellad, W.F. Buprenorphine Dispensing in Pennsylvania During the COVID-19 Pandemic, January to October 2020. J. Gen. Intern. Med. 2021, 36, 3915–3917. [Google Scholar]
- Cance, J.D.; Doyle, E. Changes in outpatient buprenorphine dispensing during the COVID-19 pandemic. JAMA 2020, 324, 2442–2444. [Google Scholar]
- Lu, H.; Zheng, J.; Wang, Y. Geospatial Analysis of Opioid Dispensing Patterns in California: A 2021 Real-World Study. Healthcare 2023, 11, 1732. [Google Scholar] [CrossRef]
- Wang, Y.; Zheng, J.; Lam, J.; Gutierrez, M. EPH251 Neighborhood Characteristics of Availability of Buprenorphine-Prescribing Clinicians and X-Waivered Clinicians. Value Health 2023, 26, S208. [Google Scholar] [CrossRef]
- State of California Department of Justice Office of the Attorney General. Controlled Substance Utilization Review and Evaluation System. Available online: https://oag.ca.gov/cures (accessed on 1 September 2023).
- Ling, W.; Smith, D. Buprenorphine: Blending practice and research. J. Subst. Abus. Treat. 2002, 23, 87–92. [Google Scholar]
- Ling, W.; Charuvastra, C.; Collins, J.F.; Batki, S.; Brown, L.S., Jr.; Kintaudi, P.; Wesson, D.R.; Mcnicholas, L.; Tusel, D.J.; Malkerneker, U. Buprenorphine maintenance treatment of opiate dependence: A multicenter, randomized clinical trial. Addiction 1998, 93, 475–486. [Google Scholar]
- Penfold, R.B.; Zhang, F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad. Pediatr. 2013, 13, S38–S44. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef]
- Ali, M.M.; Creedon, T.B.; Jacobus-Kantor, L.; Sherry, T.B. National trends in buprenorphine prescribing before and during the COVID-19 pandemic. J. Subst. Abus. Treat. 2023, 144, 108923. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A. Many buprenorphine prescribers don’t take Medicaid or uninsured patients. Alcohol. Drug Abus. Wkly. 2019, 31, 1–3. [Google Scholar]
- Dietz, M.; Lucia, L.; Challenor, T.; Rak, A.; Roby, D.H.; Kominski, G.F.; Kadiyala, S. Undocumented Californians Projected to Remain the Largest Group of Uninsured in the State in 2022; Center for Labor Research and Education: Berkeley, CA, USA, 2021. [Google Scholar]
- Larochelle, M.R.; Jones, C.M.; Zhang, K. Change in opioid and buprenorphine prescribers and prescriptions by specialty, 2016–2021. Drug Alcohol Depend. 2023, 248, 109933. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.S.; Samuels, E.A. Continuing increased access to buprenorphine in the United States via telemedicine after COVID-19. Int. J. Drug Policy 2021, 93, 102905. [Google Scholar] [PubMed]
- Ward, K.M.; Scheim, A.; Wang, J.; Cocchiaro, B.; Singley, K.; Roth, A.M. Impact of reduced restrictions on buprenorphine prescribing during COVID-19 among patients in a community-based treatment program. Drug Alcohol Depend. Rep. 2022, 3, 100055. [Google Scholar] [CrossRef]
- Thornton, J.D.; Varisco, T.J.; Bapat, S.S.; Downs, C.G.; Shen, C. Impact of COVID-19 related policy changes on buprenorphine dispensing in Texas. J. Addict. Med. 2020, 14, e372. [Google Scholar] [CrossRef]
- Stein, B.D.; Landis, R.K.; Sheng, F.; Saloner, B.; Gordon, A.J.; Sorbero, M.; Dick, A.W. Buprenorphine treatment episodes during the first year of COVID: A retrospective examination of treatment initiation and retention. J. Gen. Intern. Med. 2023, 38, 733–737. [Google Scholar]
- US Department of Justice. Informational Documents. Available online: https://www.deadiversion.usdoj.gov/pubs/docs/index.html (accessed on 1 September 2023).



{kind=link}
{kind=link}
| Before Pandemic 19 March 2019–18 March 2020 | During Pandemic 19 March 2020–18 December 2021 | |
|---|---|---|
| Total refills | 640,883 | 983,961 |
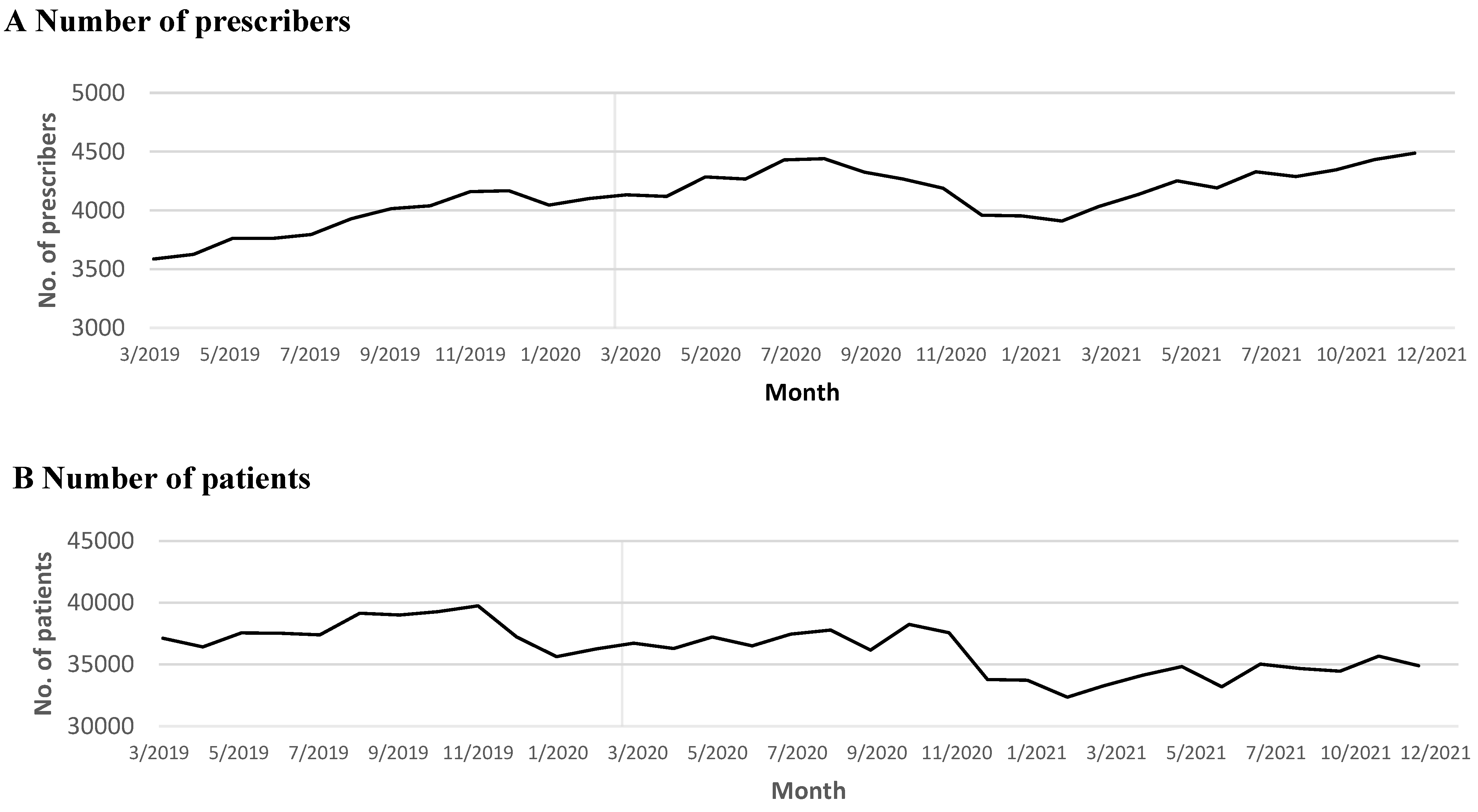
| Average number of prescribers per month | 3916 | 4227 |
| Average number of patients per month | 37,679 | 35,410 |
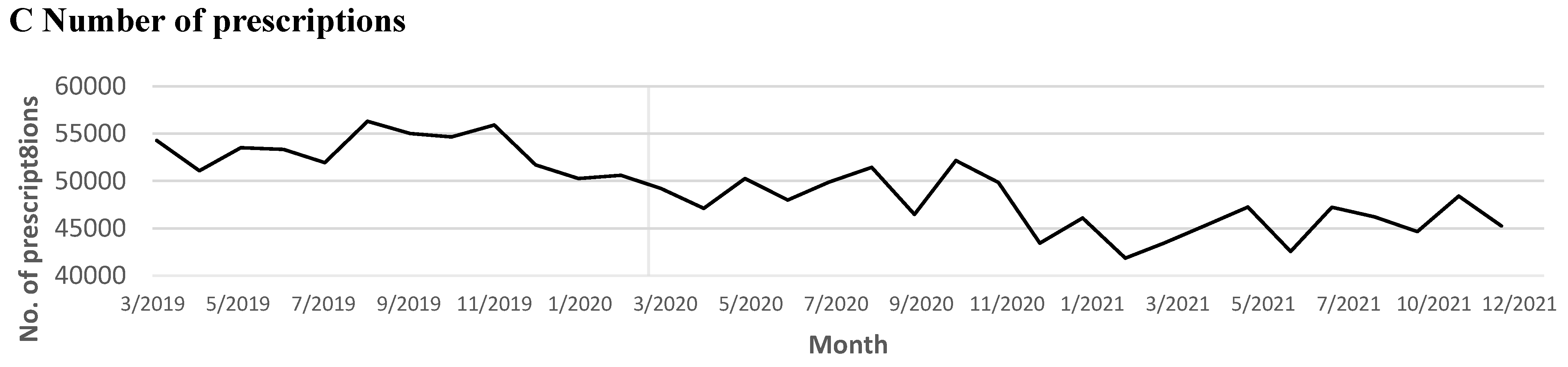
| Prescriptions per month | 53,407 | 46,855 |
| Mean days of supply (day) | 20.67 | 22.10 |
| Mean daily dosage of each filling (mg) | 14.14 | 14.35 |
| Total number of patients | 92,723 | 126,957 |
| Total prescribers | 8166 | 11,590 |
| Outcomes | β Coefficient | p Value | 95% Confidence Interval | |
|---|---|---|---|---|
| Number of prescribers | ||||
| Baseline trend (β1) before COVID-19 | 52.76 | <0.001 | 38.92 | 66.60 |
| Level change (β2) after COVID-19 | −84.87 | 0.328 | −259.35 | 89.60 |
| The change in the trend (β3) after COVID-19 | −47.41 | <0.001 | −64.50 | −30.32 |
| Number of patients | ||||
| Baseline trend (β1) before COVID-19 | −8.60 | 0.939 | −237.42 | 220.21 |
| Level change (β2) after COVID-19 | −600.25 | 0.585 | −2820.80 | 1620.30 |
| The change in the trend (β3) after COVID-19 | −152.65 | 0.204 | −392.99 | 87.69 |
| Number of prescriptions | ||||
| Baseline trend(β1) before COVID-19 | −143.16 | 0.376 | −468.50 | 182.18 |
| Level change (β2) after COVID-19 | −3023.88 | 0.065 | −6248.58 | 200.83 |
| The change in the trend (β3) after COVID-19 | −87.05 | 0.621 | −443.13 | 269.03 |
| Daily dosage | ||||
| Baseline trend (β1) before COVID-19 | 0.017 | 0.001 | 0.01 | 0.03 |
| Level change (β2) after COVID-19 | 0.018 | 0.704 | −0.08 | 0.11 |
| The change in the trend (β3) after COVID-19 | −0.009 | 0.063 | −0.02 | 0.00 |
| Days of Supply | ||||
| Baseline trend (β1) before COVID-19 | 0.02 | 0.148 | −0.01 | 0.06 |
| Level change (β2) after COVID-19 | 1.35 | <0.001 | 1.00 | 1.69 |
| The change in the trend (β3) after COVID-19 | −0.03 | 0.083 | −0.07 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Chan, A.; Beuttler, R.; Fleming, M.L.; Schneberk, T.; Nichol, M.; Lu, H. Real-World Dispensing of Buprenorphine in California during Prepandemic and Pandemic Periods. Healthcare 2024, 12, 241. https://doi.org/10.3390/healthcare12020241
Wang Y, Chan A, Beuttler R, Fleming ML, Schneberk T, Nichol M, Lu H. Real-World Dispensing of Buprenorphine in California during Prepandemic and Pandemic Periods. Healthcare. 2024; 12(2):241. https://doi.org/10.3390/healthcare12020241
Chicago/Turabian StyleWang, Yun, Alexandre Chan, Richard Beuttler, Marc L. Fleming, Todd Schneberk, Michael Nichol, and Haibing Lu. 2024. "Real-World Dispensing of Buprenorphine in California during Prepandemic and Pandemic Periods" Healthcare 12, no. 2: 241. https://doi.org/10.3390/healthcare12020241