
The Usefulness of an Online Simplified Screening Questionnaire (SSQ) in Identifying Work-Related Cancers

 , , , and
, , , and 
Abstract
:1. Introduction
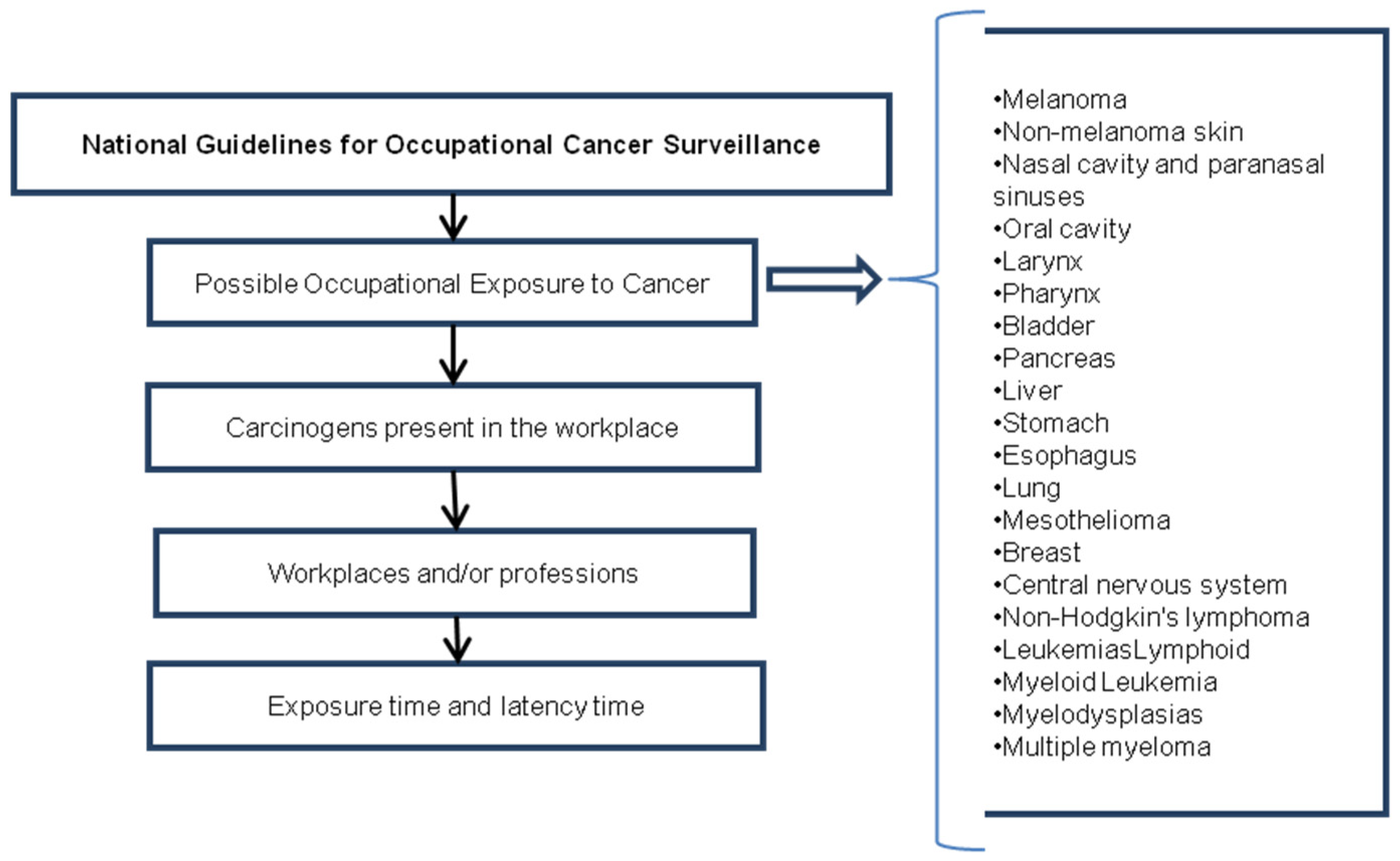
Brazilian Work-Related Cancer Surveillance Guidelines
- i
- In Brazil, there are Work-Related Cancer Guidelines that have been elaborated with clear and notable aims.
- ii
- There is an information system regulating compulsory notification offenses, and Brazil has adopted a form for registering information and notifications, neither of which are being well used or implemented.
- iii
- Although provided by the INCA manual, this form has never been implemented in clinical practice, possibly because of the difficulty in establishing a clear link between disease and occupational risk factors.
2. Materials and Methods
2.1. Development of the Simplified Screening Questionnaire (SSQ) for Work-Related Cancer
2.2. First Step
- i
- List all types of cancer that could be attributed to work-related exposure.
- ii
- For each type of cancer, list the carcinogens that could be present in the workplace and elsewhere.
- iii
- For each carcinogen, list the workplaces and/or professions in which they could be present.
- iv
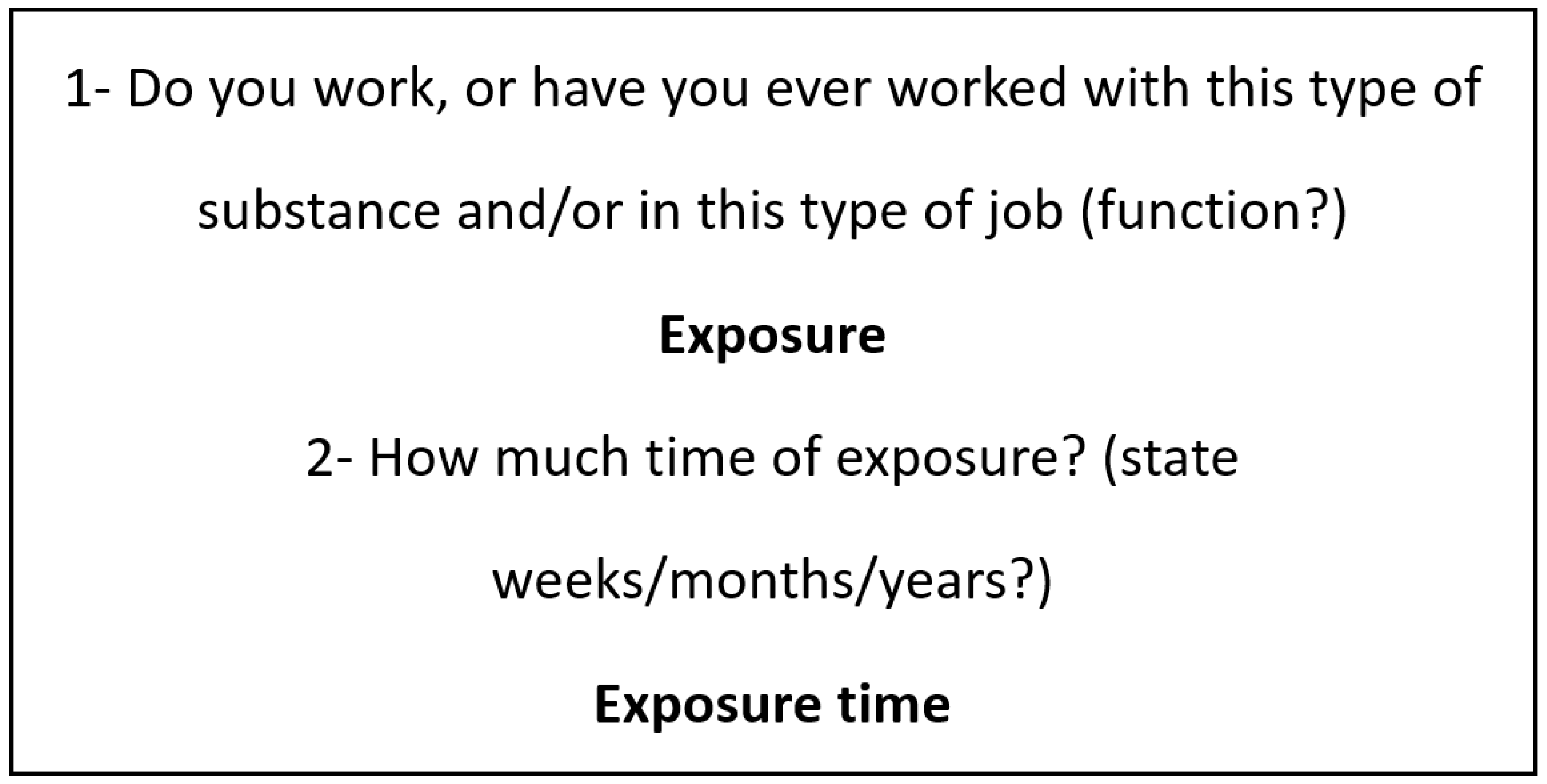
- Calculate the time of exposure.
- v
- Calculate the time of latency from exposure to the onset of cancer.
2.3. Second Step
2.4. Third Step
2.5. Study Population
2.6. Ethics
2.7. Privacy, Data Storage and Confidentiality
2.8. Sample Calculation
2.9. Study Conducted in Steps to Enable Use of SSQ
3. Results and Discussion
3.1. Patient Recruitment
The Distribution of Participants by Medical Department
- Head and neck/skin and melanoma: (314, 30.8%): non-melanoma skin (170, 54.1%), melanoma (34, 10.8%), nasal cavity and nasal sinuses (5, 1.6%), oral cavity (45, 14.3%), pharynx (36, 11.5%), larynx (24, 7.6%).
- Upper digestive system: (189, 18.5%): stomach (106, 55.5%), esophagus (43, 23.6%), liver (6, 3.3%), pancreas (32, 17, 6%).
- Thorax: (127, 12.5%): lung (115, 97.5%), mesothelioma (3, 2.5%).
- Hematology: (105, 10.3%): lymphoid leukemia (2, 1.9%), myeloid leukemia (13, 12.4%), myelodysplasias (2, 1.9%), multiple myeloma (18, 17, 1%), non-Hodgkin’s lymphoma (70, 66.7%).
- Breast: (184, 18.0%).
- Urology: (48, 4.7%).
- Neurology: (53, 5.2%).
3.2. Applicability
4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Pearce, N.; Blair, A.; Vineis, P.; Ahrens, W.; Andersen, A.; Anto, J.M.; Armstrong, B.K.; Baccarelli, A.A.; Beland, F.A.; Berrington, A.; et al. Iarc monographs: 40 years of evaluating carcinogenic hazards to humans. Environ. Health Perspect 2015, 123, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Doll, R.; Peto, R. The causes of cancer: Quantitative estimates of avoidable risks of cancer in the united states today. J. Natl. Cancer Inst. 1981, 66, 1191–1308. [Google Scholar] [CrossRef] [PubMed]
- De Vries, H.J. Standardization: A Business Approach to the Role of National Standardization Organizations; Springer Science & Business Media: New York, NY, USA, 2013. [Google Scholar]
- Rushton, L.; Hutchings, S.J.; Straif, K. Occupational Cancer Burden; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar]
- Facina, T. Diretrizes para a vigilância do câncer relacionado ao trabalho. Rev. Bras. Cancerol. 2012, 58, 279–280. [Google Scholar] [CrossRef]
- Lopes, J.N.P. A Relação Entre os Custos Segurado e Não Segurado dos Acidentes do Trabalho. Master’s Thesis, Centro Universitário da FEI, São Bernardo do Campo, Brazil, 2009. [Google Scholar]
- Wright, A. Redcap: A tool for the electronic capture of research data. J. Electron. Resour. Med. Libr. 2016, 13, 197–201. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Department Head and Neck/Skin and Melanoma | n | n Exposed | % Exposed |
|---|---|---|---|
| Non-melanoma skin | 170 | 150 | 88.2 |
| Melanoma | 34 | 23 | 67.6 |
| Nasal cavity and paranasal sinuses | 5 | 4 | 80.0 |
| Oral cavity | 45 | 32 | 71.1 |
| Pharynx | 36 | 28 | 77.8 |
| Larynx | 24 | 20 | 83.3 |
| Total | 314 | 257 | 81.8 |
| Upper Digestive Department | n | n Exposed | % Exposed |
| Stomach | 106 | 59 | 55.7 |
| Esophagus | 44 | 27 | 61.4 |
| Liver | 6 | 5 | 83.3 |
| Pancreas | 33 | 8 | 24.2 |
| Total | 189 | 99 | 52.4 |
| Thorax Department | n | n Exposed | % Exposed |
| Lung | 123 | 61 | 49.6 |
| Mesothelioma | 3 | 2 | 66.7 |
| Total | 126 | 63 | 50.0 |
| Hematology Department | n | n Exposed | % Exposed |
| Lymphoid leukemia | 2 | 1 | 50 |
| Myeloid Leukemia | 13 | 6 | 46.2 |
| Myelodysplasias | 2 | 2 | 100.0 |
| Multiple myeloma | 18 | 10 | 55.6 |
| Non-Hodgkin’s Lymphoma | 70 | 34 | 48.6 |
| Total | 105 | 53 | 50.5 |
| Breast Department | n | n Exposed | % Exposed |
| Breast | 184 | 38 | 20.7 |
| Urology Department | n | n Exposed | % Exposed |
| Bladder | 48 | 20 | 41.7 |
| Neurology Department | n | n Exposed | % Exposed |
| Central Nervous System | 53 | 20 | 37.7 |
| SKIN—NOT MELANOMA | n | % | |
| Exposition | In agriculture, applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) | 59 | 39.3 |
| Exposed to sunlight or exposed to ultraviolet radiation in an outdoor occupation (bricklayer, welder, salesman, farm worker, lifeguard, health worker, fisherman, traffic guard, gardener, mountaineering guide, miner) | 149 | 99.3 | |
| MELANOMA | n | % | |
| Exposed to sunlight or exposed to ultraviolet radiation in an outdoor occupation (bricklayer, welder, salesman, farm worker, lifeguard, health worker, fisherman, traffic guard, gardener, mountaineering guide, miner) | 21 | 91.3 | |
| NASAL SINUS OF PARANASAL SINUSES | n | % | |
| Handling herbicides (Paraquat or Gramoxone) in agriculture | 3 | 75 | |
| Placement or demolition of asbestos products such as in construction; plumbing; laying and remodeling roofs (Eternit tiles); thermal insulation of boilers and pipes | 3 | 75 | |
| ORAL CAVITY | n | % | |
| In direct contact with wood dust, leather dust, cement dust, or cereal dust; in direct contact with textile dust | 17 | 53.1 | |
| applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 16 | 50 | |
| Placement or demolition of asbestos-based products such as construction; plumbing; boiler and piping thermal remodeling (roofing); boiler and piping thermal insulation | 16 | 50 | |
| Animal husbandry | 14 | 43.8 | |
| PHARYNX | n | % | |
| In direct contact with wood dust, leather dust, cement dust or cereal dust; in direct contact with textile dust | 19 | 67.9 | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 13, | 46.4 | |
| Timber, Sawmill and Joinery Industry (creosote) | 12 | 42.9 | |
| LARYNX | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 11 | 57.9 | |
| Animal husbandry | 10 | 52.6 | |
| In direct contact with wood dust, leather dust, cement dust or cereal dust; in direct contact with textile dust | 8 | 42.1 | |
| STOMACH | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 39 | 66.1 | |
| With construction dust (bricklayers, etc.) | 27 | 45.8 | |
| ESOPHAGUS | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 15 | 55.6 | |
| With construction dust (bricklayers, etc.) | 12 | 44.4 | |
| Gas station attendant (or with fuel vapors) | 5 | 18.5 | |
| LIVER | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 3 | 60.0 | |
| Copper production | 1 | 20.0 | |
| Wood industry with creosote used for wood preservation | 1 | 20.0 | |
| The production or manufacture of paints, plastics, rubber products, pigments and papers | 1 | 20.0 | |
| PANCREAS | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 8 | 100 | |
| Wood industry with creosote used for wood preservation | 1 | 12.5 | |
| LUNG | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 30 | 49.2 | |
| Placement or demolition of asbestos products such as in construction; plumbers; laying and remodeling roofs (Eternit tiles); thermal insulation of boilers and pipes | 16 | 26.2 | |
| MESOTHELIOMA | n | % | |
| Placement or demolition of asbestos products such as in construction; plumbers; laying and remodeling roofs (Eternit tiles); thermal insulation of boilers and pipes | 2 | 100 | |
| LYMPHOID LEUKEMIA | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 1 | 100 | |
| MYELOID LEUKEMIA | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 3 | 50 | |
| MYELODYSPLASIA | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 2 | 100 | |
| Asbestos extraction mining (asbestos rock extraction processes, drilling, cutting, dismantling, crushing, screening and handling these rocks) | 1 | 50 | |
| MULTIPLE MYELOMA | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 7 | 77.8 | |
| NON-HODGKIN’S LYMPHOMA | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 22 | 64.7 | |
| BREAST | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 17 | 44.7 | |
| Direct contact with formaldehyde (such as hair stylists using permanent brushes and volatile organic compounds, among other occupations that work directly with formaldehyde) | 13 | 34.2 | |
| BLADDER | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 12 | 63.2 | |
| Exposed to diesel flue gases | 7 | 36.8 | |
| CENTRAL NERVOUS SYSTEM | n | % | |
| Applying or handling pesticides (herbicides, pesticides, insecticides, fungicides) in agriculture | 8 | 40 | |
| Wood industry with creosote used for wood preservation | 4 | 20 | |
| Metallurgy and steelmaking (contact with metal waste such as mercury, lead and cadmium); handling heavy metal waste | 4 | 20 |
| Cancer | Carcinogen or Professional Occupation | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agriculture | Sun Exposed | Asbestos | Dust | Breeding | Mason | Gas station Attendant | Diesel | Creosote | Cooper | Formalin | Heavy Metals | |
| Non-melanoma skin | 59 | 149 | ||||||||||
| Melanoma | 21 | |||||||||||
| Paranasal sinuses nasal cavity | 3 | 3 | ||||||||||
| Oral cavity | 16 | 17 | 14 | |||||||||
| Pharynx | 13 | 19 | 12 | |||||||||
| Larynx | 11 | 8 | 10 | |||||||||
| Stomach | 39 | 27 | ||||||||||
| Esophagus | 15 | 12 | 5 | |||||||||
| Liver | 3 | 1 | 1 | |||||||||
| Pancreas | 8 | 1 | ||||||||||
| Lung | 30 | 16 | ||||||||||
| Mesothelioma | 2 | |||||||||||
| Lymphoid leukemia | 1 | |||||||||||
| Myeloid leukemia | 3 | |||||||||||
| Myelodysplasia | 2 | 1 | ||||||||||
| Multiple myeloma | 7 | |||||||||||
| Non-Hodgkin’s lymphoma | 22 | |||||||||||
| Breast | 17 | 13 | ||||||||||
| Bladder | 12 | 7 | ||||||||||
| CNS | 8 | 1 | 4 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vazquez, F.L.; Silveira, H.C.S.; Otero, U.B.; Hosokawa, T.T.; Fregnani, J.H.T.G.; Longatto-Filho, A.; Reis, R.M. The Usefulness of an Online Simplified Screening Questionnaire (SSQ) in Identifying Work-Related Cancers. Healthcare 2023, 11, 1563. https://doi.org/10.3390/healthcare11111563
Vazquez FL, Silveira HCS, Otero UB, Hosokawa TT, Fregnani JHTG, Longatto-Filho A, Reis RM. The Usefulness of an Online Simplified Screening Questionnaire (SSQ) in Identifying Work-Related Cancers. Healthcare. 2023; 11(11):1563. https://doi.org/10.3390/healthcare11111563
Chicago/Turabian StyleVazquez, Fabiana L., Henrique C. S. Silveira, Ubirani B. Otero, Thais T. Hosokawa, José Humberto T. G. Fregnani, Adhemar Longatto-Filho, and Rui M. Reis. 2023. "The Usefulness of an Online Simplified Screening Questionnaire (SSQ) in Identifying Work-Related Cancers" Healthcare 11, no. 11: 1563. https://doi.org/10.3390/healthcare11111563